
Abstract
Study design
Retrospective cohort study.
Objectives
To compare Hounsfield unit (HU), vertebral bone quality (VBQ), and dual-energy X-ray absorptiometry (DEXA) T-score in predicting cage subsidence (CS) after posterior lumbar interbody fusion.
Methods
We retrospectively reviewed patients undergoing PLIF and measured L4 HU and VBQ. Baseline characteristics between CS and non-CS groups were compared. Multiple logistic regression analysis was used to identify risk factors for CS. Receiver operating characteristic (ROC) curves were used to explore the predictive value of variables for CS. Subgroup analysis was conducted for patients with available DEXA results.
Results
Eighty-four patients were analyzed. The subsidence group was older, with lower L4 HU (92.6 (35.4) vs 130.8 (47.8), P < 0.001) and higher VBQ (3.30 (0.64) vs 2.99 (0.63), P = 0.041) compared to the non-CS group. Low L4 HU (OR 0.979, P = 0.022) was an independent risk factor for subsidence, while VBQ was not. ROC analysis indicated that L4 HU (AUC = 0.733, P < 0.001) exhibited superior predictive performance compared to VBQ (AUC = 0.643, P = 0.032). Subgroup analysis in patients with DEXA showed that the femoral neck T-score (AUC = 0.67, P = 0.037) could differentiate CS, with L4 HU exhibiting the highest predictive ability (AUC = 0.778, P < 0.001), both outperforming VBQ (AUC = 0.645, P = 0.075).
Conclusions
Among the three BMD parameters, only low L4 HU could be an independent risk factor for CS. Preoperative HU is mandatory in patients at risk for osteoporosis when undergoing spine surgery.
Introduction
The posterior lumbar interbody fusion (PLIF) procedure is widely recognized as the established surgical approach for treating lumbar degenerative diseases, and it has become the gold standard for lumbar fusion surgeries. 1 Its extensive and direct neural decompression contributes to achieving satisfactory therapeutic outcomes in patients. However, excising the posterior column structure during the procedure leads to the interbody fusion device experiencing a significantly increased vertical load under both static and dynamic loading conditions, compared to transforaminal lumbar interbody fusion (TLIF) surgery.2,3 As a result, this contributes to a higher cage subsidence rate than TLIF surgery. 4 Cage subsidence, accompanied by a loss of intervertebral height, leads to suboptimal clinical outcomes and can necessitate revision surgery. 5 However, studies on this topic predominantly focus on TLIF, 6 oblique lumbar interbody fusion, 7 anterior lumbar interbody fusion, 8 and lateral lumbar interbody fusion. 9 Factors predicting cage subsidence in PLIF are less studied than in TLIF or other approaches.
Osteoporosis is a significant factor contributing to cage subsidence. While dual-energy X-ray absorptiometry (DEXA) remains the gold standard for bone density assessment, it is susceptible to the influence of degenerative factors such as vertebral osteophyte formation and aortic calcification, leading to falsely elevated results in bone density assessments. 10 However, the Hounsfield unit (HU), as a method for evaluating local vertebral bone density, has demonstrated superior predictive capabilities in various postoperative complications, such as predicting screw loosening and cage subsidence, compared to traditional DEXA.11,12
The recently proposed novel MRI-based vertebral bone quality (VBQ) scores assess bone density indirectly by evaluating intra-vertebral fat content. 13 It can independently predict vertebral compression fractures in patients with spinal metastasis, demonstrating unique advantages14, such as its correlation with bone trabecular microstructure measured by micro-computed tomography. 15 Additionally, due to the correlation between paravertebral muscle fat infiltration and intra-vertebral fat content, VBQ has recently been discovered as a comprehensive indicator for assessing bone and muscle quality. 16 However, limitations of this simplified scoring system have been identified, with MRI machine parameters affecting its results. 17 Recent conflicting conclusions have emerged regarding VBQ’s role in assessing bone density, predicting fractures after spinal metastasis, and predicting proximal junctional failure in adult spinal deformity patients.18-20
Previous studies have often evaluated the predictive value of a single bone density assessment method for cage subsidence without proper controls. There is a limited amount of comparative research in different ways. This study aims to compare the predictive abilities of these three methods and explore the optimal approach.
Method
Patient Cohort
A retrospective analysis was conducted on patients who underwent PLIF surgery for lumbar degenerative diseases between January 2020 and June 2022, after obtaining approval from the Institutional Review Board of our hospital. As this study was retrospective, written and signed informed consent was waived. Demographic, clinical, and radiological data were reviewed. Inclusion criteria: 1. Patients aged 18 years and older; 2. Patients with available preoperative CT, MRI, and postoperative CT scans; 3. Patients who underwent preoperative examinations within one month before surgery; 4. Patients with a follow-up period exceeding five months. Exclusion criteria: 1. Patients undergoing lumbar fusion at more than two levels (> 2); 2. Patients with conditions such as ankylosing spondylitis, spinal tuberculosis, or metastatic tumors; 3. Patients who had undergone previous lumbar fusion surgery.
Surgical Information
In this study, all patients underwent open PLIF. In our clinical practice, after preparing the intervertebral space, we routinely apply BMP and then fill the space with bone grafts, taking care to avoid BMP-induced nerve irritation. A PEEK cage was then implanted, with the size of the cage selected according to the dimensions of the vertebral body. No cement-augmented screws were used in any of the cases.
Evaluating Cage Subsidence through Sagittal and Coronal CT Scans
CS was defined as an interbody cage sinking of more than 2 mm into the adjacent endplate.7,21 In patients undergoing two-level fusion, if subsidence occurred in either of the intervertebral spaces, they were categorized into the subsidence group. Two independent observers, blinded to patient data, assessed CS. In cases of disagreement between the two observers, a third observer reassessed to achieve consensus.
L4 HU Calculation
Sagittal CT has been confirmed to be consistent with axial CT regarding HU values and represents a more rapid and reproducible measurement method.
22
As in previous studies, we selected the L4 vertebral body for measurements.23-25 The region of interest (ROI) was placed in the mid-sagittal plane of the vertebral body, avoiding areas such as cortical bone and venous plexuses. The average L4 HU value was then measured (Figure 1). Representative image measuring preoperative L4 Hounsfield Units (HU) through CT.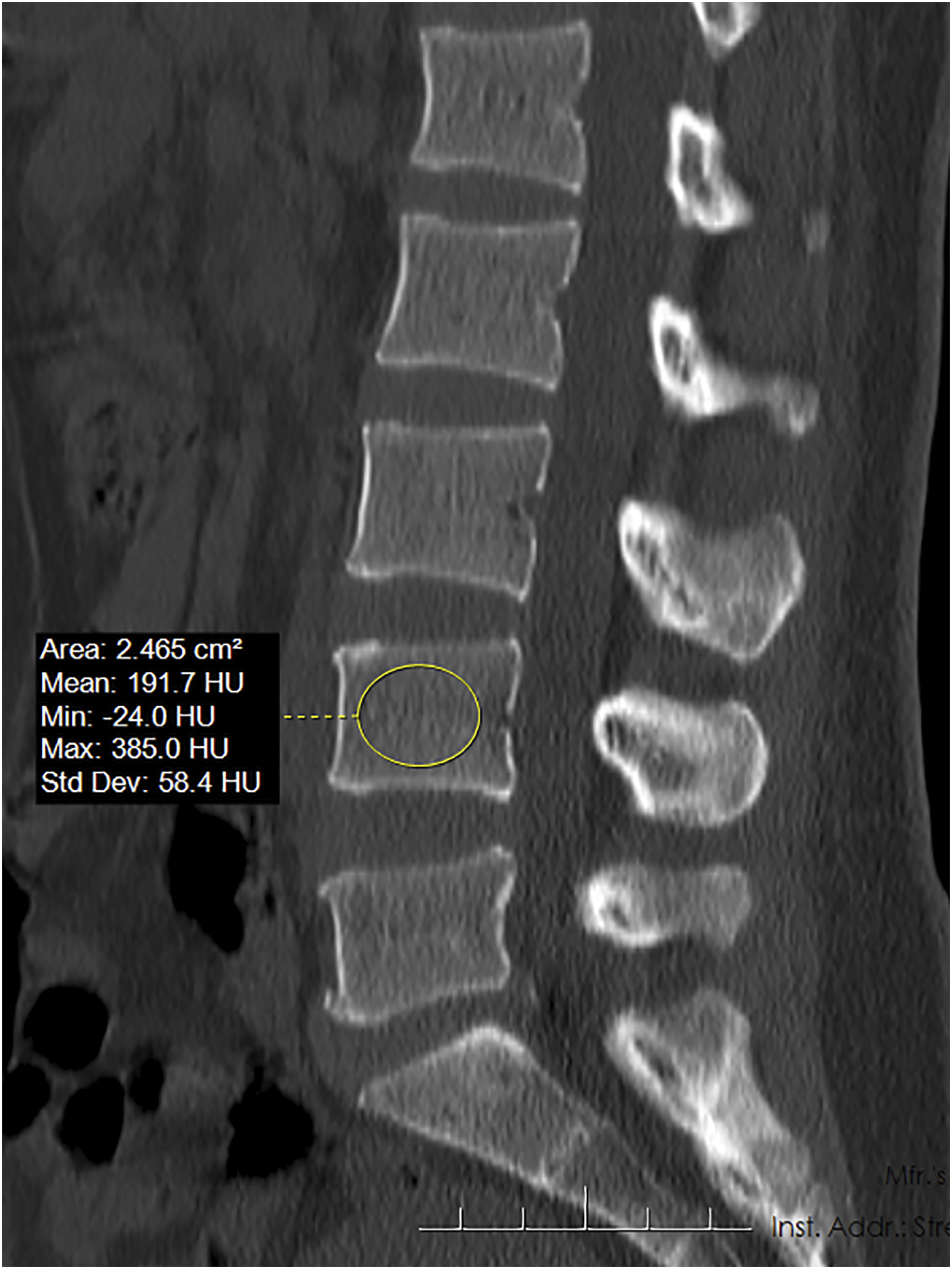
VBQ Calculation
Following the previously described method,
13
non-contract, T1-weighted MR images of the lumbar spine were used for measurements. ROIs were placed in the mid-sagittal plane at the L1-L4 vertebral levels to measure vertebral signal intensity (SI). Posterior to the L3 vertebra, the SI of cerebrospinal fluid (CSF) was measured (Figure 2). An adjacent level was selected for analysis if narrowing was observed at L3 CSF. Representative image measuring preoperative Vertebral Bone Quality (VBQ) through MRI.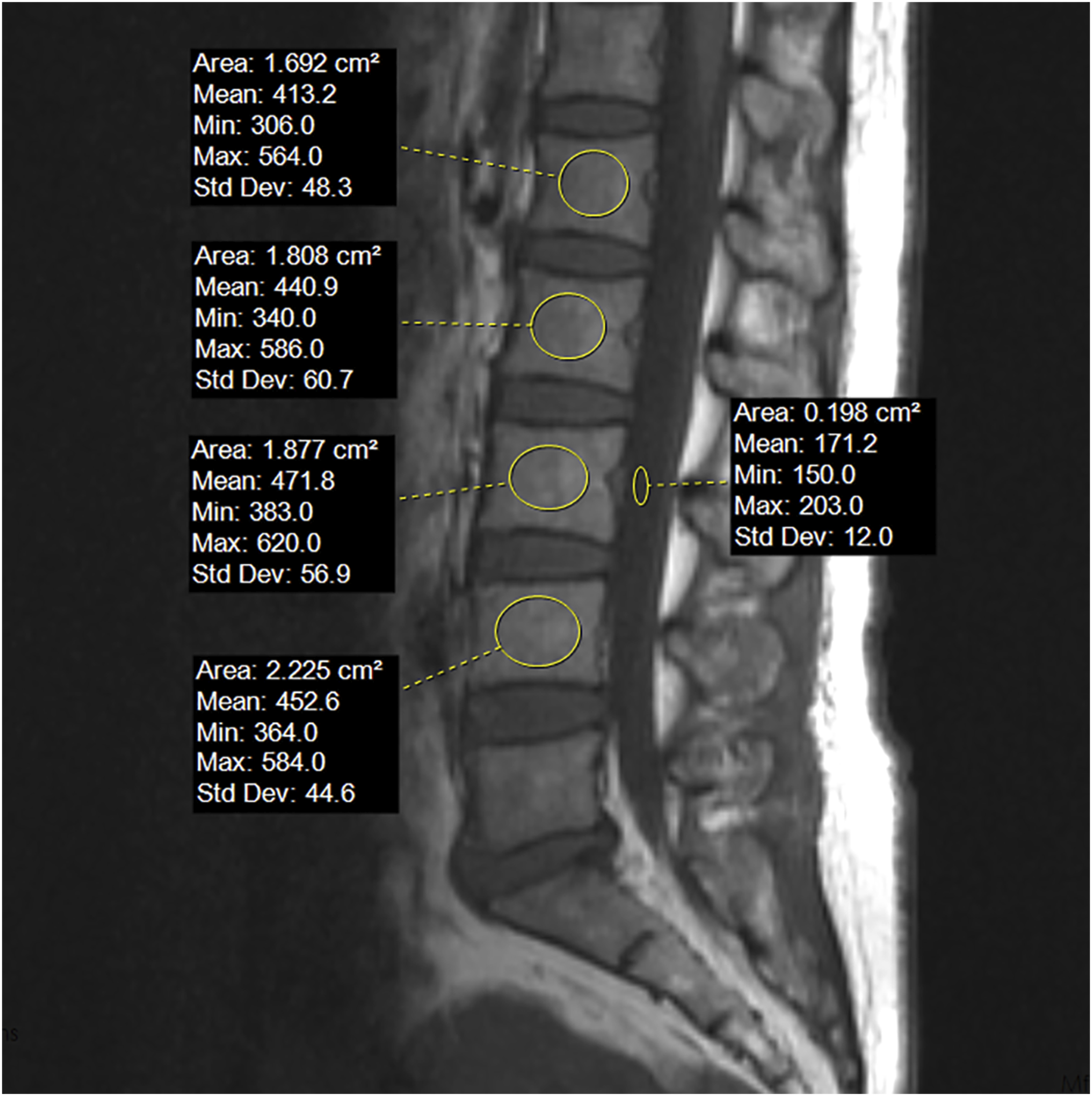

DEXA T-scores
T-scores for DEXA were obtained from the lumbar spine and femoral neck. DEXA T-scores were available for 64.3% of the study population.
Statistical Analysis
Statistical analysis was performed using SPSS26. Figures were created using GraphPad Prism 8. Continuous variables were shown as mean (standard deviation), and categorical variables were shown as frequency (percentage). Comparisons between the two groups were made using Student's t-tests for continuous variables. The chi-square test or Fisher’s exact test was used for categorical variables. Independent risk factors for CS were analyzed using multiple logistic regression. Clinical factors associated with CS,26,27 including sex, age, BMI, fusion level, and the follow-up period, were included as covariates. L4 HU, VBQ, and DEXA T-scores were included as predictors in separate models due to the correlation among these three BMD assessment parameters. Receiver operating characteristic (ROC) analysis, including area under the curve (AUC) calculations, was used to assess the diagnostic efficacy of predictors. The optimal cutoff values, sensitivity, and specificity were determined by the Youden index.
Results
Demographic Information
A total of 84 patients (30 male and 54 female patients) were included in the study, with a mean age of 60.06 (10.96) years. The mean follow-up period was 8.57 (3.20) months, and the subsidence rate was 34.5%. Single-level fusion was performed in 63 patients, while 21 underwent two-level fusion.
Comparison between Subsidence and Non-subsidence Groups
Characteristics of the Study Population.
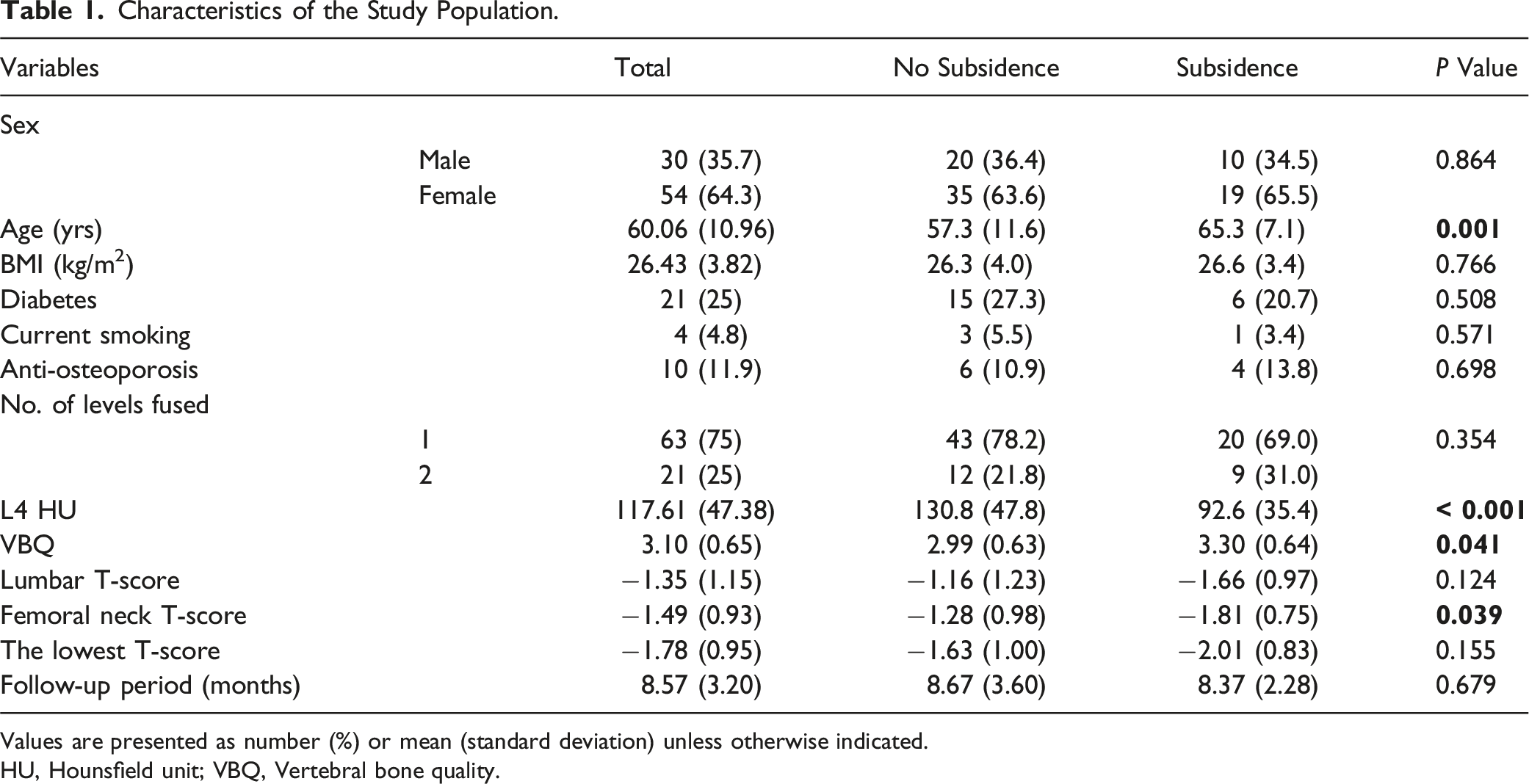
Values are presented as number (%) or mean (standard deviation) unless otherwise indicated.
HU, Hounsfield unit; VBQ, Vertebral bone quality.
Multiple Logistic Regression Analysis for Risk Factors of Subsidence after PLIF
Multiple Logistic Regression Analysis for Risk Factors of Cage Subsidence After PLIF.
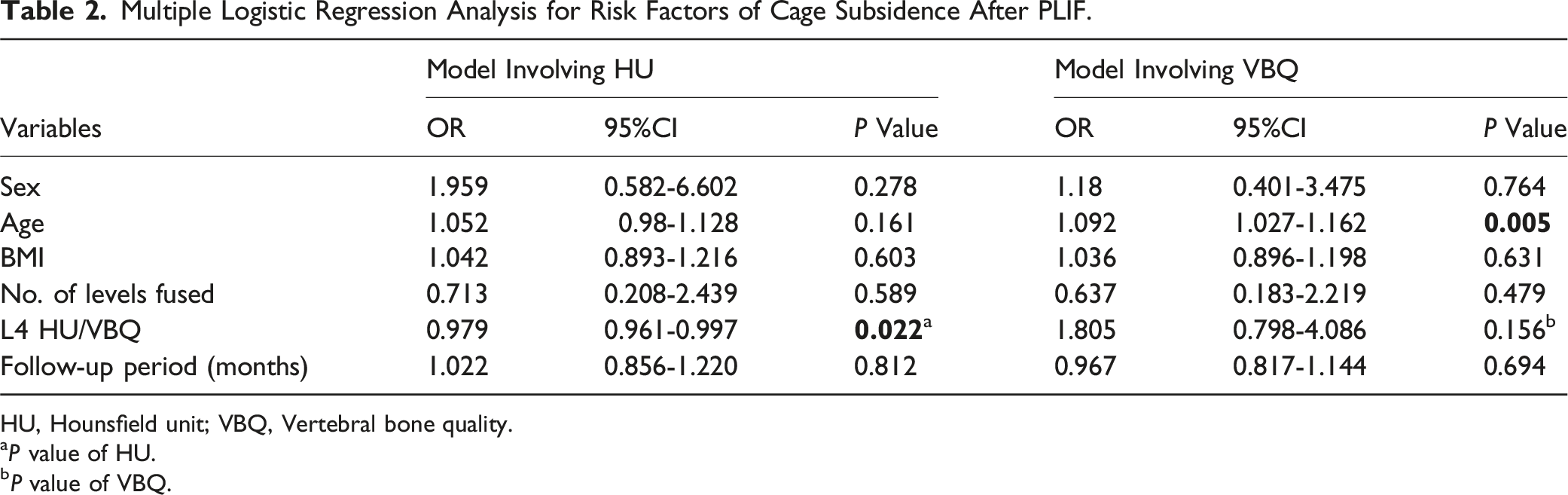
HU, Hounsfield unit; VBQ, Vertebral bone quality.
aP value of HU.
bP value of VBQ.
Diagnostic Efficacy Assessed by ROC Analysis of L4 HU and VBQ
ROC curve analysis indicated that the AUC for L4 HU was 0.733 (P < 0.001). The optimal cutoff for cage subsidence was 98.05 (sensitivity: 62.1%, specificity: 76.4%). After excluding 9 patients whose fusion levels did not involve L4, the sensitivity analysis showed an AUC of 0.721, which was not significantly different from the primary analysis. VBQ demonstrated inferior predictive performance with an AUC of 0.643 (P = 0.032). The optimal cutoff for VBQ was 2.94 (sensitivity: 82.8%, specificity: 54.5%) (Figure 3). The ROC curves of cage subsidence predicted by L4 HU and VBQ.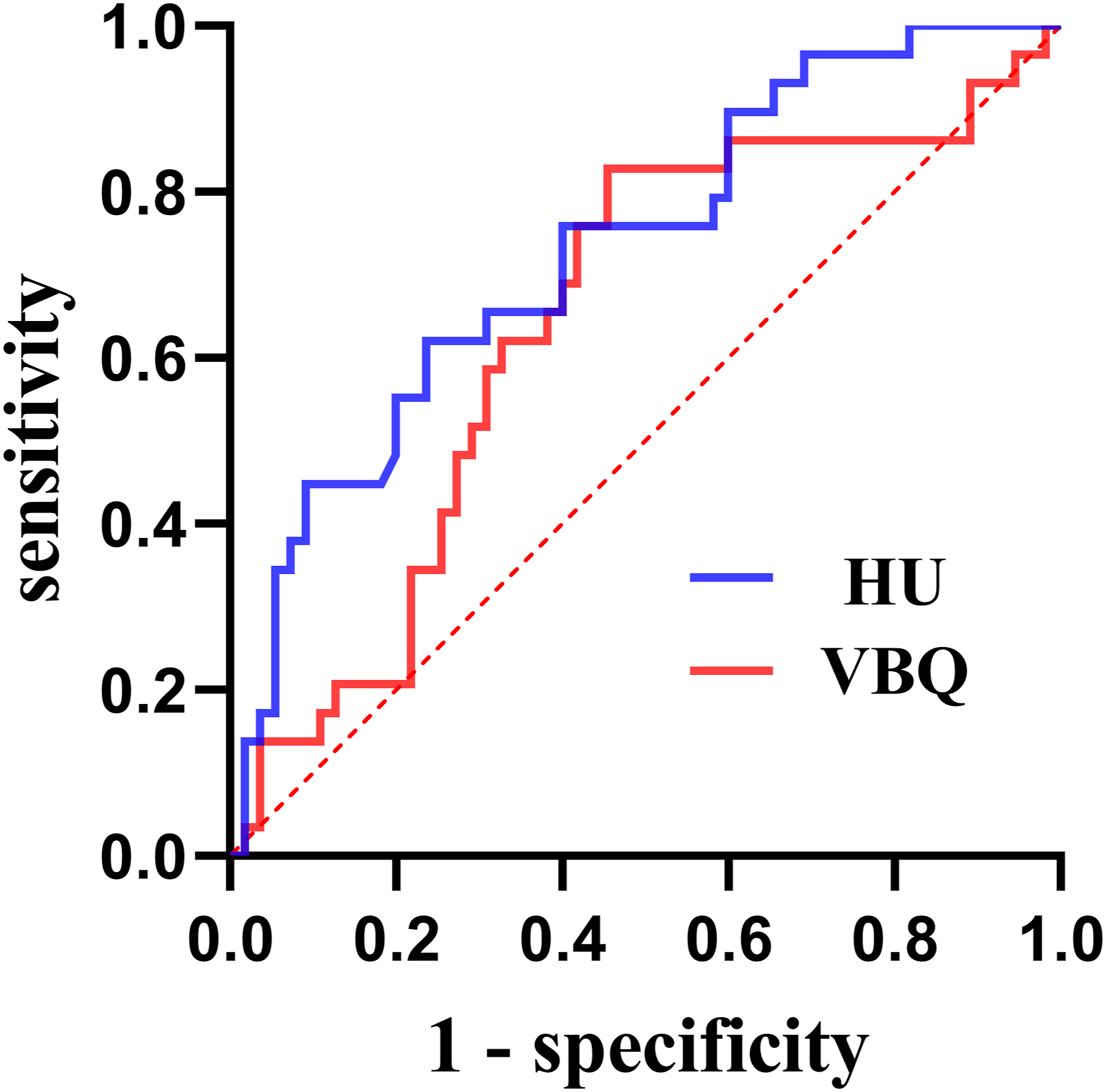
Subset Analysis of Patients with Preoperative CT, MRI, and DEXA Results
We first compared the predictive value of T-scores at different sites. ROC analysis indicated that the femoral neck T-score (AUC = 0.67, P = 0.037) could differentiate patients with subsidence. However, lumbar spine T-score (P = 0.134) and the lowest value T-score (P = 0.183) were not predictive factors.
Subset Analysis of Those Patients in Whom Preoperative DEXA was Available.
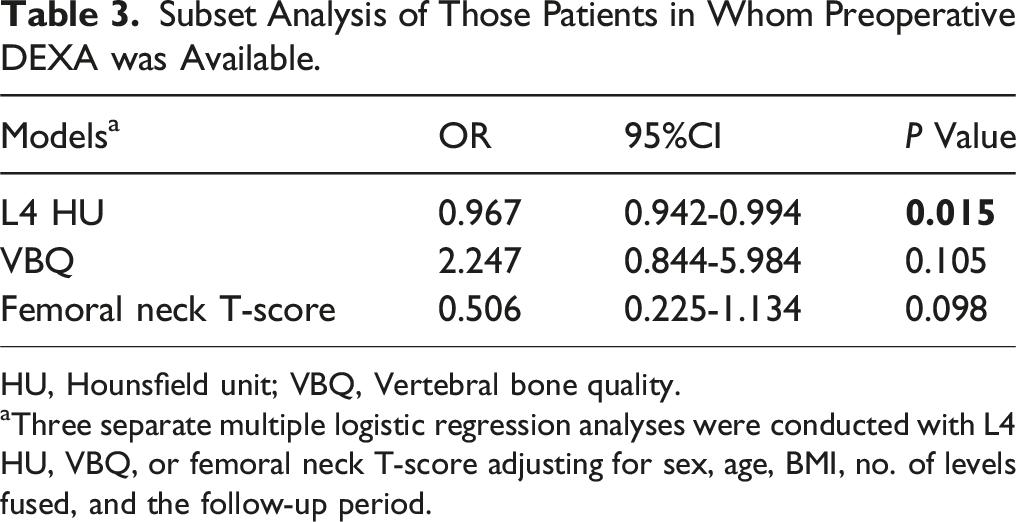
HU, Hounsfield unit; VBQ, Vertebral bone quality.
aThree separate multiple logistic regression analyses were conducted with L4 HU, VBQ, or femoral neck T-score adjusting for sex, age, BMI, no. of levels fused, and the follow-up period.
ROC analysis for this subset demonstrated that the AUC for L4 HU was 0.778 (P < 0.001). The optimal cutoff for cage subsidence was 98.6 (sensitivity: 81%, specificity: 66.7%). The AUC of the femoral neck T-score was 0.67 (P = 0.037), with an optimal cutoff of −1.15 (sensitivity: 90.5%, specificity: 51.5%). VBQ could not predict subsidence (AUC = 0.645, P = 0.075) (Figure 4). The ROC curves of cage subsidence predicted by L4 HU, VBQ, and DEXA T-value of those patients in whom preoperative DEXA was available.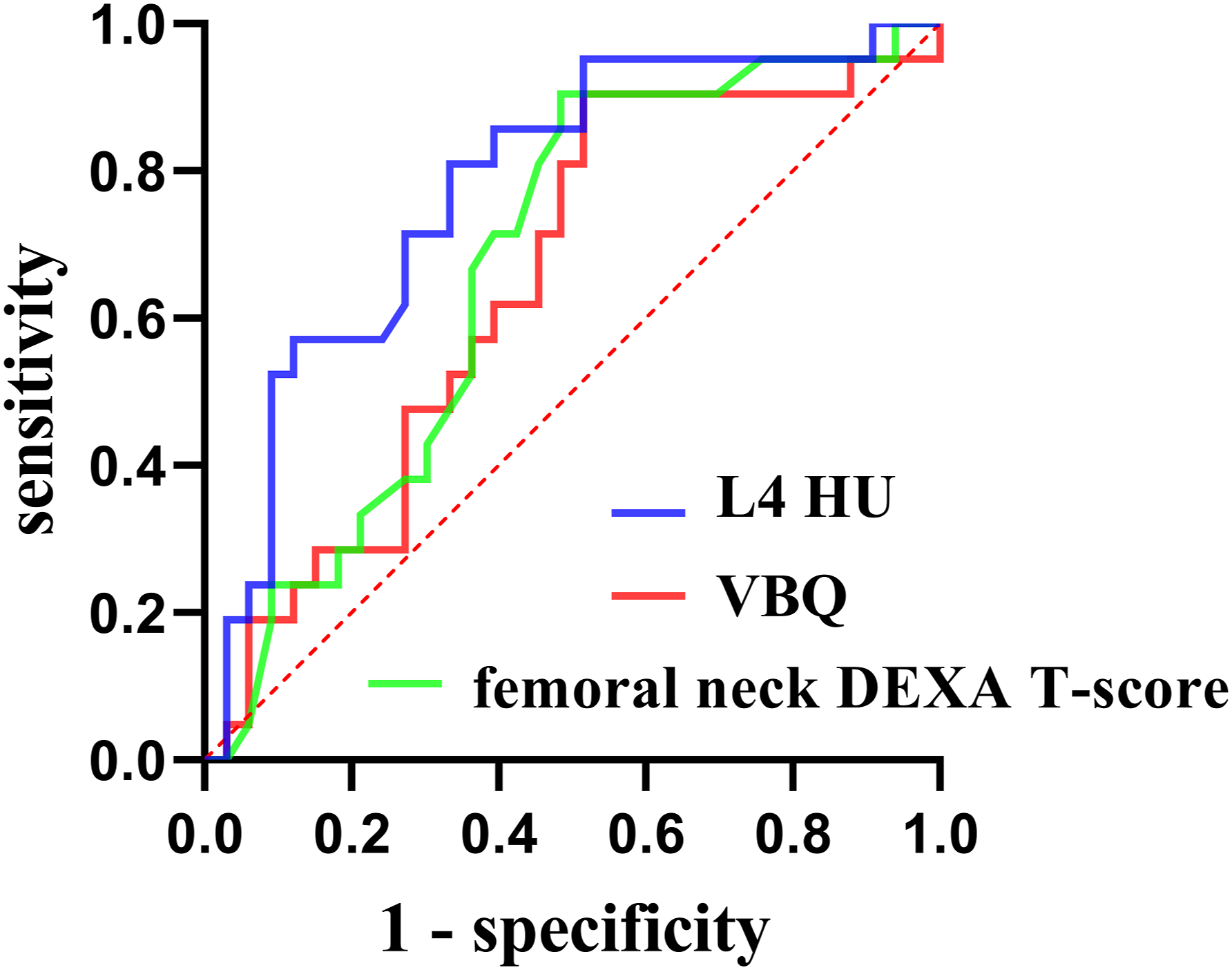
Discussion
We compared the predictive value of three bone mineral density assessment methods for cage subsidence after PLIF. Our findings indicate that L4 HU is currently the optimal prediction method. The femoral neck T-score can identify patients with subsidence, but the lumbar spine T-score cannot. In general, DEXA has limited predictive value for subsidence, and VBQ is not currently recommended for predicting subsidence, necessitating further multicenter studies to validate its performance.
The US Preventive Services Task Force (USPSTF) recommends osteoporosis screening using central DEXA to prevent osteoporotic fractures in women aged 65 and older, as well as in postmenopausal women under 65 who are identified as high-risk based on clinical risk assessment. Risk factors include a parental history of hip fracture, smoking, excessive alcohol consumption, and low body weight. However, there is currently insufficient evidence to evaluate the balance of benefits and risks of screening for osteoporosis to prevent osteoporotic fractures in men. 28 Lumbar CT, a routine examination method in spine surgery, provides an opportunistic screening for bone density and prediction of postoperative mechanical complications. HU is widely recognized for assessing bone density and predicting complications following lumbar spine surgery. Previous literature suggests that sagittal and axial plane HU measurements are in agreement, with sagittal view assessments providing a more rapid measurement. 29 Koichi Murata’s study found that sagittal plane HU measurements were associated with short-term vertebral fractures after lumbar fusion surgery, whereas axial plane HU measurements were not. 30 We believe that subsidence, similar to fractures, results from sagittal plane loading, and sagittal measurements have comparable predictive value. Supporting literature indicates that predictions of subsidence using sagittal and axial HU measurements are roughly equivalent (0.891 vs 0.909). 31
VBQ, as a novel local bone density assessment method, has been controversial. Previous research has produced significant discrepancies, particularly regarding its ability to assess bone density and predict complications such as postoperative proximal junctional failure (PJF) in adult spinal deformity patients. Emily C. Courtois et al. conducted a study involving 238 patients and concluded that the diagnostic capability of VBQ for osteopenia/osteoporosis is limited (AUC = 0.557). 18 Akihiko Hiyama, et al's research indicated lower upper instrumented vertebra or L4 HU values were associated with PJF after lateral lumbar interbody fusion in female adult spinal deformity patients, but there was no significant difference in VBQ scores between the PJF and non-PJF groups. 20 As research advances, VBQ is recognized for its unique advantages in reflecting trabecular bone structure or simultaneously assessing muscle conditions,15,16 but limitations in its cross-machine application have been identified. 17 Whether VBQ can predict postoperative subsidence in PLIF is still under exploration.
Our initial comparison of L4 HU and VBQ for subsidence in patients with available preoperative MRI and CT data revealed that L4 HU was an independent risk factor for subsidence, whereas VBQ was not. Previous studies have found that HU varied among vertebral levels, with disc degeneration associated with reduced vertebral bone density.32,33 Considering that we measured HU at explicit L4 level, we conducted a sensitivity analysis by excluding 9 patients whose fused levels did not involve L4. The predictive performance did not significantly change. Additionally, two-level fusion did not increase the subsidence rate, consistent with Tien V. Le et al's findings on XLIF, which showed similar subsidence rates for single-level and two-level fusion (10.3% vs 9.4%), with a significant increase only in three or more segment fusions. 34
Diabetes, associated with decreased bone turnover, accumulation of advanced glycation endproducts (AGEs), and increased bone fragility, 35 has a controversial impact on bone density, with some studies showing an increase in bone density due to diabetes, while others indicate a decrease.36,37 Studies examining the relationship between diabetes and cage subsidence have not found a significant association.
Two meta-analyses showed that bisphosphonate use does not significantly improve fusion rates but does reduce mechanical complications such as subsidence and screw loosening.38,39 However, the study by Seungjun Ryu et al. indicated that while denosumab reduced postoperative osteolysis but did not significantly decrease the rate of subsidence. 40 Existing evidence supports the role of bisphosphonates in preventing mechanical complications.
Gengyu Han et al. identified that the Paraspinal Muscle Endurance and Morphology (PMEM) Score as an independent indicator of mechanical complications. 41 Manuel Moser and colleagues hypothesized that a smaller psoas and/or paraspinal FCSA could be a risk factor for severe cage subsidence following standalone lateral lumbar interbody fusion. Interestingly, they did not find that patients with sarcopenia were at increased risk of severe cage subsidence. Instead, they observed that a larger psoas muscle cross-sectional area in male patients was associated with severe subsidence, possibly due to the higher compressive forces borne by the lumbar spine. 42 Further research is needed to validate the role of sarcopenia in mechanical complications.
Previous studies have found an association between BMP use and endplate resorption and subsidence. 43 However, other studies have reported that BMP use is not an independent risk factor for subsidence,21,44,45 leaving this topic still open for further investigation. Moreover, since all patients in our study received BMP, the sample was homogeneous, so BMP use did not affect the results.
We also assessed the predictive abilities of DEXA T-scores at different sites for CS and found that only the femoral neck T-score exhibited satisfactory performance. Degenerative changes such as sclerosis, osteophyte formation at the vertebral margins, facet joint hypertrophy, or aortic calcification can lead to falsely elevated lumbar spine T-scores. However, the femoral neck is less affected by degenerative factors. Fang Xie et al investigated the predictive performance of DEXA for CS following TLIF and found that femoral BMD was superior to lumbar spine BMD, 25 similar to our results. Additionally, Kyeong Hwan Kim et al's study on screw loosening did not find a significant difference in lumbar spine DEXA between the loosening and non-loosening groups, 46 suggesting lumbar spine DEXA may not be essential for preoperative planning in cases of severe lumbar degeneration.
Subset analysis of patients with complete preoperative MRI, CT, and DEXA data indicated that L4 HU and femoral neck T-score could differentiate subsidence patients, while VBQ could not. Consistent with the primary analysis, multiple analyses showed that only L4 HU was an independent risk factor. HU directly reflects local cancellous bone density, displaying superior predictive capabilities for osteoporosis-related complications. DEXA scans are constrained by their two-dimensional scanning nature, affected by degenerative factors in the lumbar region, such as osteophyte formation, sclerotic Modic changes, and aortic calcification, leading to relatively suboptimal results. The femoral neck T-score outperforms the lumbar spine T-score, further affirming the limitations of DEXA, as the femoral neck is less susceptible to age-related degeneration. VBQ, as a novel local bone density assessment method, indirectly reflects bone density through vertebral body fat content, resulting in poor predictive performance. Simultaneously, the confounding effects of MRI parameters, such as relaxation times and echo times, cannot be ruled out. 17 Hyperlipidemia may cause a false elevation in VBQ measurements, reducing its precision in assessing bone density. 47 The inverse relationship between bone marrow fat and bone density varies between genders. 48 Differences in gender distribution and the prevalence of hyperlipidemia across studies may lead to disparate conclusions. Xingxiao Pu et al. found comparable performance for mean global L1-L5 HU (0.802) and VBQ (0.814) for postoperative subsidence in OLIF. 49 Variations in sample size, study design, and surgical procedures may account for differences in findings. Bo Zhang et al 's study was similar in design to ours and compared the predictive performance of L1-L4 HU, VBQ, and DEXA T-scores for thoracolumbar fragility fractures. Consistent with our findings, all three methods demonstrated the ability to predict fractures, with HU exhibiting the highest predictive performance, followed by DEXA and VBQ performing the lowest effectively. 50
Based on the above, we recommend that L4 HU represent the optimal method for predicting CS after PLIF. The femoral neck T-score demonstrates the ability to differentiate CS patients but is secondary to L4 HU. VBQ should be used with caution for predicting subsidence, pending validation with larger datasets.
Limitations: Not all study populations underwent DEXA, which may introduce bias in analysis related to DEXA T- scores. The sample size is relatively limited, and further confirmatory studies are needed for validation. Although the follow-up period is relatively short, Luis Marchi’s study found that 90.2% of stand-alone lateral interbody fusion subsidence occurred within six weeks postoperatively, so we believe a 5-month follow-up still accurately reflects the actual situation. 51
Our study has strengths: Our study used comprehensive CT analysis in sagittal and coronal planes to assess subsidence, which may provide more accurate results compared to traditional X-ray methods. During clinical follow-up, we observed cases where X-rays indicated subsidence or gap collapse in some patients, but further CT examination revealed no apparent subsidence. Therefore, the patient’s positioning and X-ray projection angle during anteroposterior and lateral X-ray imaging may produce false-positive results.
Conclusion
Among HU, VBQ, and DEXA T-scores, only low L4 HU was identified as an independent risk factor for CS after PLIF, with L4 HU demonstrating the best predictive performance. Femoral neck DEXA is a secondary choice and the predictive capability of VBQ is limited. Thus, when CT is available, HU should be prioritized to predict subsidence in all pre-operative patients undergoing a PLIF procedure.
Supplemental Material
Supplemental Material - Comparison of Hounsfield Unit, Vertebral Bone Quality, and Dual-Energy X-Ray Absorptiometry T-Score for Predicting Cage Subsidence After Posterior Lumbar Interbody Fusion
Supplemental Material for Comparison of Hounsfield Unit, Vertebral Bone Quality, and Dual-Energy X-Ray Absorptiometry T-Score for Predicting Cage Subsidence After Posterior Lumbar Interbody Fusion by Yunsheng Wang, Jiali Zhang, Tong Tong, Dechao Miao, Feng Wang and Linfeng Wang in Global Spine Journal.
Footnotes
Author Contributions
Conceptualization: Y.S.W., J.L.Z., T.T., L.F.W., Formal Analysis: Y.S.W., J.L.Z., T.T., Investigation: Y.S.W., J.L.Z., T.T., D.C.M., F.W., Methodology: Y.S.W., J.L.Z., T.T., Project Administration: L.F.W., Writing – Original Draft: Y.S.W., J.L.Z. and Writing – Review & Editing: T.T., D.C.M., F.W., L.F.W..
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.