
Abstract
Study Design:
Retrospective study.
Objective:
To describe the MRI findings of RNRs in patients with low back pain, and observe the imaging findings and the clinical outcome post decompression surgery.
Methods:
The lumbar spine MRI of 202 patients (122 females) with proven RNRs were retrospectively reviewed. The morphology and the location of the RNRs in relation to the level of stenosis were described. The level(s), grade and cause of lumbar canal stenosis were recorded. The persistence of symptoms and the imaging findings on follow up post decompression surgery were recorded. The imaging findings were correlated among each other and with patients’ demographics.
Results:
Two distinctive morphological appearance of the RNRs were noted: loop (56.4%), and serpentine-shaped. In the majority of the cases the RNRs were located above the level of stenosis (79.7%). Eighteen patients underwent decompression surgery, only 4 patients remained symptomatic post decompression surgery. The RNRs changed in shape and location after decompression surgery. Age was a strong predictor value in the location of the RNRs. There was no correlation between the shape and location of the RNRs, or with the gender of the patients.
Conclusion:
RNRs is not an uncommon finding on lumbar spine MRI with lumbar canal stenosis. Its importance remains a controversy. A common language between the radiologists and the clinicians is mandatory to aid in the management planning.
Introduction
Several previous reports have credited Verbiest (1954) with the description of the redundant nerve roots (RNRs) of the cauda equina.1-6 However, Verbiest described a developmental anomaly that causes spinal canal narrowing resulting in characteristic symptoms, and he suggested that the nerve roots would be affected only if they were deviated from their normal path. 6 On the other hand, in 1967, Cressman and Pawl were the first to introduce the true descriptive term “RNRs of the cauda equina,” as a condition associated with spinal canal narrowing. 7
RNRs is a condition owing to which the nerve roots of the cauda equina become elongated, tortuous, and thickened due to an extradural compression that causes the stenosis of the spinal canal.2,8 The incidence of the occurrence of RNRs was found to be 33.8-42.7%. 9
Lumbar spinal canal stenosis (LCS) is considered to be the primary cause responsible for the development of this condition. The suggested mechanism involves the influence of an external compression force on the nerve roots, which grips them as they squeeze into and out of the narrowed canal, thereby causing them to become tortuous and elongated. 2
Via myelographic studies, this syndrome was initially described as the presence of multiple serpiginous filling defects within the contrast-filled lumbar subarachnoid space, which is associated with a high grade partial or complete extradural block of the transit of contrast. 10
On sagittal T2 images acquired via magnetic resonance imaging (MRI), the RNRs appear as wave-like structures that fill the subarachnoid space in the lumbar spinal canal and that produce a signal intensity similar to that produced by the nerve roots of the cauda equina.
It is a slowly progressive condition that primarily affects elderly individuals who present with more severe symptoms that remain for a longer duration. The damage caused to the nerve roots owing to the long period of exposure to canal narrowing results in the incomplete recovery of the symptoms in most of the patients with RNRs who undergo decompression surgery. 8
Further, this condition is not as uncommon as was previously thought, and its recognition on MR images is important in order to plan surgeries and to predict the clinical outcome post-surgery. 3
The aim of this study was to report on the MRI findings associated with the RNRs of the cauda equina including the morphology of the RNRs and their location with respect to the level of stenosis. The associated degenerative changes of the lumbar spine that contribute to the canal stenosis and the clinical outcomes and imaging findings of the patients post-decompression surgery have also been reported on. To the best of our knowledge, this is the largest study group that has been investigated up to date.
Material and Methods
This study was approved by the Institutional Review Board of our institution. We retrospectively studied the lumbar spine MRI records of 202 patients with evidence of RNRs of the cauda equina associated with LCS between January 2012 to May 2019.
The presence of RNRs was defined as elongated and tortuous nerves of the cauda equina observed within the subarachnoid space on sagittal T2 images. Patients with histories of fractures, previous spinal surgeries, neoplasms, primary lumbar canal stenosis, and inflammatory or infectious diseases were all excluded from our study.
The MR images were obtained using two 1.5 T scanners (Toshiba, Japan and Philips, USA) and a 3 T scanner (Philips, USA). Sagittal T1 and T2 and axial T2 spin echo sequences were obtained for all the patients using a phase array coil.
The images were individually analyzed by 2 radiologists to detect the presence of spinal canal stenosis, to determine whether the stenosis was single or multilevel, and to assess the degree of the stenosis. The degree of LCS was assessed based on the grading system proposed by Lee et al, 11 according to which LCS was defined as the obliteration of the cerebrospinal fluid (CSF) space anterior to the cauda equina in the dural sac as observed on T2 axial images, and it was categorized into the following 3 grades: grade 1/mild stenosis: mild obliteration of the anterior CSF space with clear separation among each of the cauda equina nerves; grade 2/moderate stenosis: moderate obliteration of the anterior CSF space with some aggregation of the cauda equina making it impossible to visually separate the nerves; and grade 3/severe stenosis: severe obliteration of the anterior CSF space with the cauda equina appearing as 1 bundle, thereby resulting in none of the nerves appearing visually separated from each other. Only the levels of stenosis involving the presence of RNRs were taken into consideration.
In addition, the images were assessed for the following causes of LCS: degenerative disc bulges (DDB), spondylolisthesis, facet joint degeneration (FJD), and ligamentum flavum hypertrophy (LFH). The thickness of the ligamentum flavum responsible for focal spinal canal stenosis was measured at the facet joint level on T2 axial images. If the thickness was asymmetrical at that particular level, the measurement of the thickest side was used. The measurements that we obtained were compared with those corresponding to the thickness of the ligamentum flavum at various levels for specific age groups that are recorded in a table created by Sakamaki et al. 12
The RNRs were assessed based on their morphology, i.e. whether they were loop-shaped or serpentine-shaped and based on their location in relation to the level of stenosis, i.e. whether they were located above, below, or above and below the level of stenosis.
The patients were categorized as having persistent or non-persistent symptoms post-surgery. The available images and surgical records were analyzed to determine the type of surgery performed (microdiscectomy vs. laminectomy with transpedicular fixation screws), and the level and morphology of the RNRs following surgery.
Intravenous contrast material was administered to only 1 patient who was highly suspected of being affected by a dural arteriovenous malformation owing to the extensive tortuosity of the RNRs.
The pre and post operative clinical data, and the operation notes were obtained through the hospital’s electronic data base.
All the statistical analyses for the dependent and independent variables were performed using the SAS statistical software (version 9.2; SAS institute, Cary, NC, USA). Frequencies and percentages were used for categorical variables. The statistical associations between variables, such as RNRs shapes and locations, were tested using the Pearson’s X2 Chi-test and Fisher’s Exact test for low counts. The analysis was performed both for the overall sample and for each sex. A p-value of <0.05 was considered significant.
Results
On sagittal T2 MR images, the RNRs appeared as wave-like structures filling the subarachnoid space in the lumbar spinal canal, and they produced a signal intensity similar to that produced by the nerve roots of the cauda equina in relation to a focal stenosis.
The majority of the study group was females (60.4%) with an age range between 42-85 years. The age range of the males was 36-88 years.
Two distinctive morphological configurations of the RNRs were noted: in the majority of patients, they (56.4%) appeared to be loop-shaped while in the rest, they were observed to be serpentine-shaped (Figure 1).

Morphological configuration of the RNRs demonstrated on sagittal T2 images. (a) Loop-shaped RNRs above L3 level in a patient with moderate spinal canal stenosis at L3-L4 level. (b) Serpentine-shaped RNRs above L3 level in a patient with severe spinal canal stenosis at L3-L4 level.
In 79.7% of the patients, the RNRs were located above the level of the canal stenosis, and in 14.3% of them, the RNRs were located above and below the level of stenosis. Further, in only 12 patients, the RNRs were located below the level of the stenosis (Figure 2).
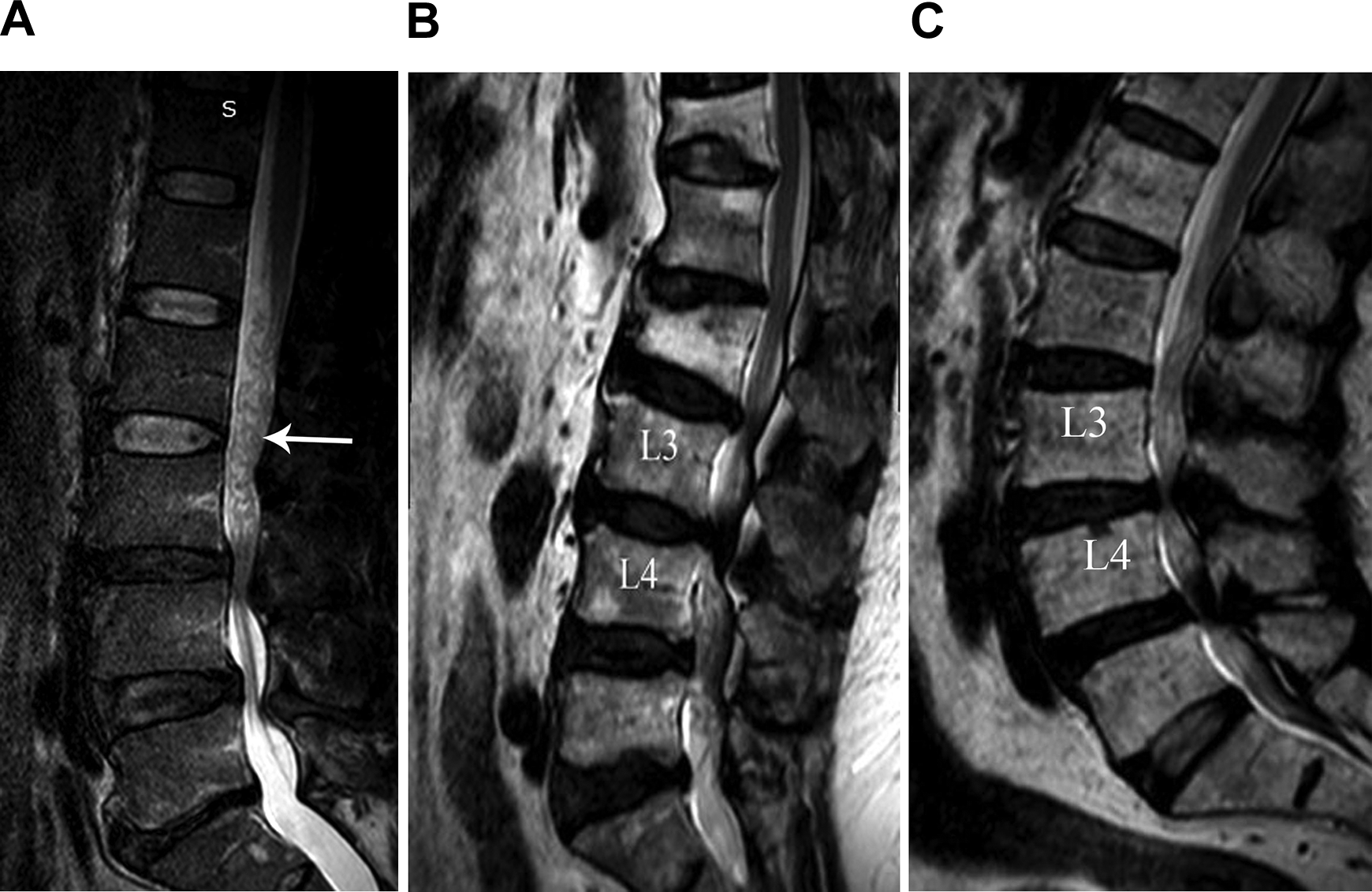
Locations of the RNRs in relation to the focal spinal canal stenosis. (a) Above the level of moderate spinal canal stenosis at L3-L4 level (arrow). (b) Below the level of severe spinal canal stenosis at L3-L4 level. (c) Above and below the level of severe spinal canal stenosis at L3-L4.
The main presenting symptom was lower back pain which was present in all of the patients. The symptoms overlapped with more than 1 symptom presenting in the same patient. Sciatica was the most common associated symptom (65%). Numbness and parasthesia was seen in 18% of the patients. 8% of the patients presented with associated neurogenic claudication. The least associated symptoms were weakness and foot drop (2.4% and 1% respectively).
The RNRs in patients with sciatica were most commonly seen above the level of stenosis and were serpentine-shaped. In patients with numbness and paresthesia and foot drop, the RNRs were most commonly located above the level of stenosis. Equal frequency of the shape of the RNRs in the former and loop-shaped was common in the latter. In patients with neurogenic claudication the RNRs were most commonly noted above and below the level of stenosis and were loop-shaped. RNRs were serpentine-shaped in patients with associated weakness with equal frequency regarding their location. There were no significant statistical correlations among the location and morphology of the RNRs and the presenting symptoms.
There were no significant statistical correlations among the location and morphology of the RNRs and patient sex, and there were no significant statistical correlations between the location and the morphology of the RNRs (Table 1).
Correlation Between Gender and the Location and Shape of the RNRs. A p-value of <0.05 Was Considered Significant.
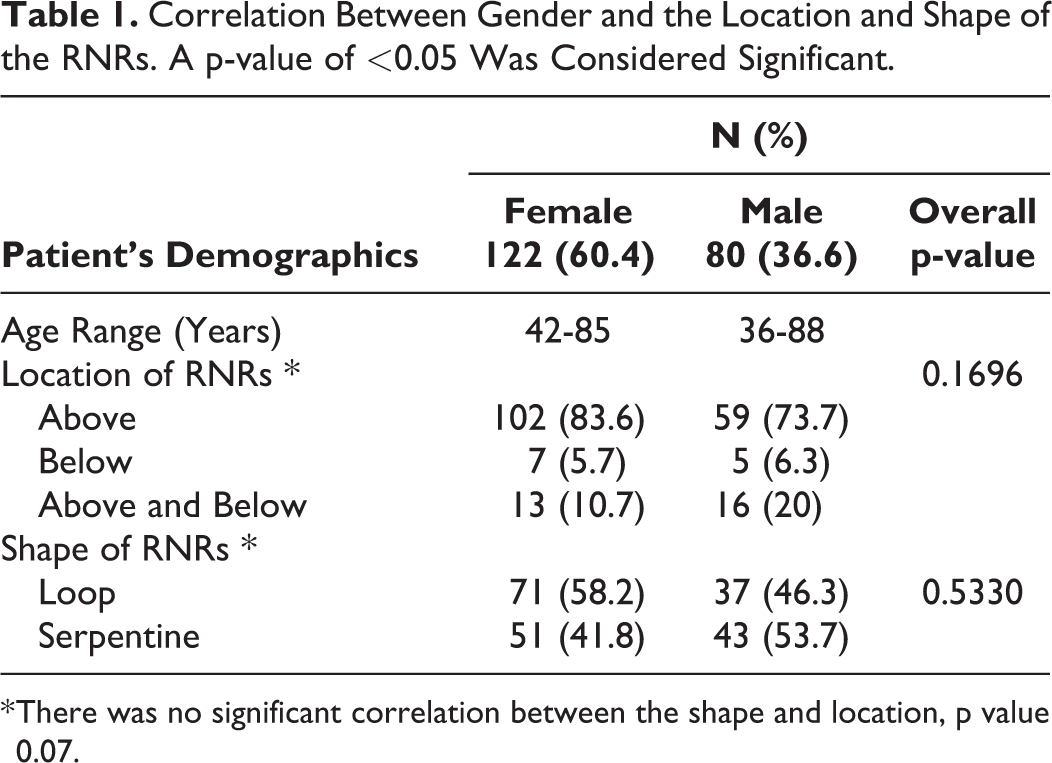
* There was no significant correlation between the shape and location, p value 0.07.
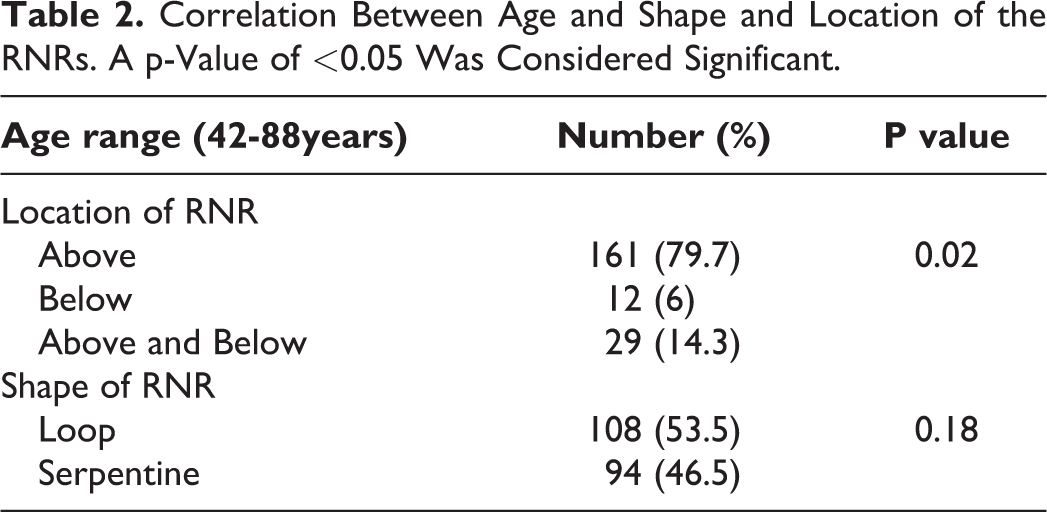
There was significant statistical correlation among the location of the RNRs and the age of the patients. The patients with RNRs present above and below the level of the canal stenosis were much older than the rest. The age differences between the patients with RNRs above and below the level of stenosis were 2-12 years and 3-19 years older than those with RNRs above the level of stenosis and below the level of stenosis respectively. No significant age difference was noted between RNRs above the level of stenosis and those below the level of stenosis. However, no statistical correlation was observed among the shape of the RNRs and the age (Table 2).
Correlation Between Age and Shape and Location of the RNRs. A p-Value of <0.05 Was Considered Significant.
LCS was secondary to DDB in association with LFH in the largest proportion of patients (94%), in association with FJH in 41.1% of the patients, and in association with spondylolisthesis in 6.4% of them (Table 3). None of the degenerative changes resulting in LCS showed significant statistical correlations with either the shape or location of the RNRs.
The Distribution of the Cause of LCS Among Both Genders. The Causes of the LCS Overlapped in Most of the Patients.
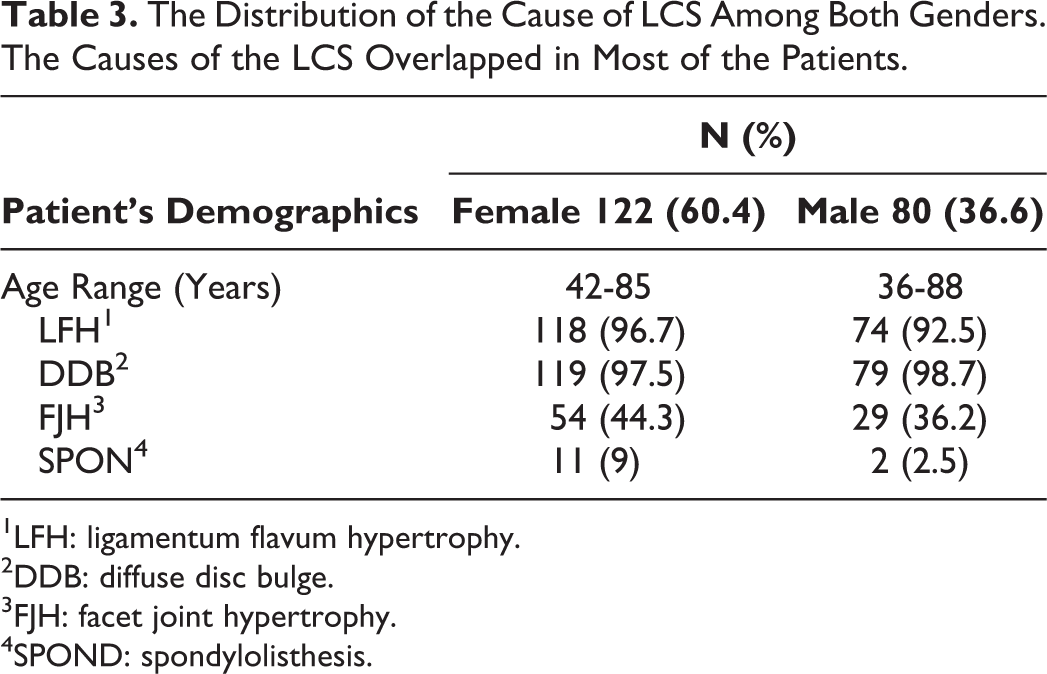
1LFH: ligamentum flavum hypertrophy.
2DDB: diffuse disc bulge.
3FJH: facet joint hypertrophy.
4SPOND: spondylolisthesis.
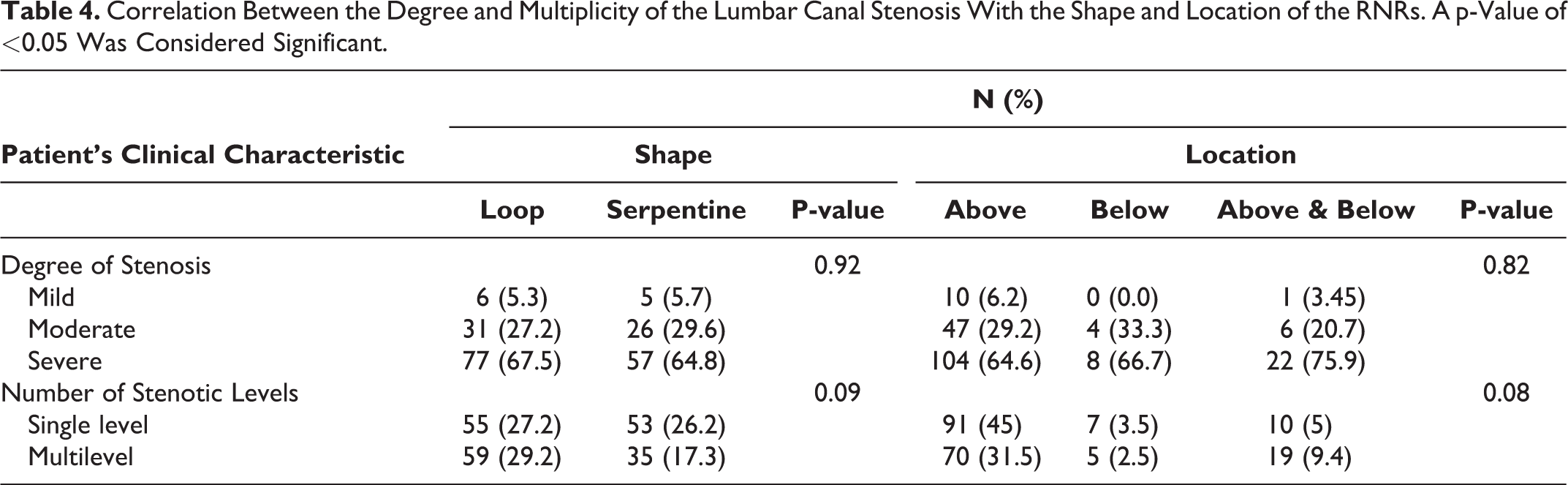
The degree of stenosis was estimated using the Lee et al. grading system 11 and only the level at which the RNRs were present was taken into consideration. Further, 65.8% of the patients had severe spinal canal stenosis, 28.7% had moderate stenosis, and the remaining 5.5% had only mild canal stenosis.
In this study, 46.5% of the patients had multilevel stenosis, and it was noted that the most cranial stenotic level was closely related to the development of RNRs. Stenosis was most commonly present at the L3-L4 and L4-L5 levels, and it was least commonly observed at the L5-S1 level.
Neither the multiplicity nor the degree of stenosis exhibited significant statistical correlations with either the shape or location of the RNRs (Table 4).
Correlation Between the Degree and Multiplicity of the Lumbar Canal Stenosis With the Shape and Location of the RNRs. A p-Value of <0.05 Was Considered Significant.
The patients’ follow-up revealed that 18 of them had undergone decompression surgery, only 7 of the patients had post-surgical imaging records, most of the other patients were lost for follow up or refused surgery. Six patients underwent laminectomy with transpedicular screws and 1 patient underwent microdiscectomy. Four patients remained symptomatic post surgery, in 2 of them; the RNRs disappeared on MRI, in 1 patient the location changed, and in another patient the shape of the RNRs changed. The remaining 3 patients who became symptom free post surgery, the RNRs were still observed on their post operative MRI, in 1 patient only the shape of the RNRs changed. Due to small sample size no statistical correlation could be withdrawn.
Discussion
In our study, the following 2 distinctive morphological configurations of RNRs were noted: loop-shaped and serpentine-shaped. The former was the most common and appeared in 56.4% of the patients, and the latter, in 43.6% of the patients. Although the Yokoyama et al. study reported the serpentine-shape to be the most common morphology, 3 our findings are in concordance with those of Poureisa et al. 13
On the studied images, 3 locations of the RNRs were noted in relation to the level of stenosis: above the level of stenosis (79.7%), below the level of stenosis (6%), and below and above the level of stenosis (14.3%). In previously published data, the RNRs located above the level of stenosis were also found to be the most commonly occurring.3-5,10,13-15 When redundancy was solely noted above the level of stenosis, the nerve roots appeared normal in morphology below the stenotic level.
In our study, we found that age was a strong predictor factor for the location of the RNRs which is in concordance with other studies.2,4,13,16,17 The oldest age groups was found among patients with RNRs present above and below the level of stenosis with severe secondary LSC and multilevel stenosis which is expected in older age groups due to increased likelihood of degenerative diseases.
Ehni et al. suggested that the reason behind the occurrence of RNRs below the level of stenosis is that the nerve root bundle below the level of stenosis is gripped by the spondylotic pathology that tightly holds the nerve roots located above the stenotic level, thereby allowing the nerve roots below to be more loosely arranged. 18 We believe that the presence of nerve roots below and above the level of stenosis, mainly in the elderly, is attributed to the excessive elongation of the nerve roots within a tight spinal canal owing to a longer duration of stenosis and to the occurrence of more severe degenerative changes that allow for the nerve roots to be loose on both sides of the stenosis.
In patients with multilevel canal stenosis, the redundancy was noted to be above the most cranial stenotic level, this might be explained by the fact that the nerve roots are fixed between 2 points: the conus medullaris and intraforaminal ganglia and by the stensois caudally causing them to move within a tight container and thus causing them to become redundant. In our study, there was no significant statistical correlation between the multiplicity and degree of stenosis and the occurrence of RNRs opposed to the study conducted by Papavero et al. 19
In our study, the presence of degenerative changes was attributed as being the cause of LCS; these changes were observed to be mainly DDB with LFH in 94% of our patients while 41.1% of them suffered from an additional change, FJH, and 6.4% had associated spondylolisthesis. Our findings support the proposition of Hur et al. that suggests that LFH rather than isolated intervertebral disc bulges is the major contributing factor to spinal canal stenosis that causes mechanical stress on the nerve roots, eventually leading to their redundancy. 20
Long term repeated lumbar movements cause the nerve roots that are forced out through the tight narrowing canal to become elongated and thickened, eventually leading to tissue damage and the severe impairment of the affected nerve roots with a reduction in the number of nerve fibers associated with demyelination, endoneurial fibrosis, and the proliferation of Schwann cells as observed via histopathological studies.2,21 The results of electrophysiological studies revealed that there was temporal dispersion of the action potentials and a delay in sensory nerve conduction velocities indicating various degrees of irreversible neuronal loss.2,22 The pathological changes associated with the affected nerve roots are thought to be irreversible, thereby contributing to a low level of clinical improvement in the patients following decompression surgery regardless of the fact that the RNRs disappear on imaging following surgery.2,3,10,17,21
In our study, only 18 patients underwent decompression surgery, only 7 of the patients had post surgery MRI, in 5 of them the RNRs remained present (2 of whom remained symptomatic and 3 who became symptom free). Our findings are consistent with other studies stating the persistence of RNRs in patients’ post surgery MRI.3,23
Four of the patients who had surgery remained symptomatic. In the 2 patients who underwent laminectomies with transpedicular fixation screws, the RNRs disappeared on imaging despite the fact that the patients remained symptomatic. We speculate that the disappearance of the RNRs is due to the alleviation of the severe canal stenosis that frees the nerve roots, thereby allowing them to regain their normal morphology. However, the persistence of symptoms is mostly attributed to the irreversible damage to the nerve roots. Both these patients were elderly individuals who suffered from a longer duration of symptoms.
The RNRs of 1 patient whose symptoms subsided post-microdiscectomy changed in morphology from serpentine- to loop-shaped. In 1 patient who underwent the same procedure, the location of the RNRs changed although the symptoms persisted. These observations may be the result of a change in the intensity of the gripping force applied on the tight nerve roots within the narrowed canal, which alters their morphology and location. A larger number of patients with post surgery MRI scans is essential to test any significant statistical correlation.
The results of the Yokoyama et al. study revealed that in patients with loop-shaped RNRs, there was a statistically significant correlation among the loop-shaped RNRs on MRI, the persistence of the RNRs, and a relatively poorer post-surgical clinical outcome. 3 Most of the previous studies revealed no significant statistical correlation in the post-surgical outcome between patients with and without RNRs.1,4,24 In a study conducted by Hacker et al., the total relief of symptoms were observed postoperatively. 10 However, none of the patients exhibited complete recovery in a relatively long follow-up study conducted by Pau et al. 25 One patient was reported to exhibit some level of recovery after receiving chiropractic treatment. 26
To date, the clinical significance of this condition remains a controversy; some studies have observed a worst clinical outcome in patients with RNRs post-surgery,1,2,20,21 and others found no significant statistical correlations.4,22 Despite this fact, we believe it is important to recognize this condition on imaging because it alerts the surgeon to the possibility of the nerve roots extruding out of the dura if a dural tear occurs at the time of surgery in which case the surgeon must be prepared to perform a potential duraplasty.15,24 In addition, the presence of RNRs and their various morphologies and locations may be considered as prognostication factors in patients who undergo medical and surgical treatments. Further studies with larger numbers of patients is required.
We emphasize the importance of establishing a classification system for RNRs to facilitate communication between the radiologists and clinicians such as the ASED classification system proposed by Papavero et al describing the allocation, shape, extension, and direction of the RNRs. 27
The limitations of our study are the small number of patients who underwent decompression surgery and whose images were available for evaluation. Additionally, it was a retrospective study, and the pain scores of the patients evaluated before and after decompression surgery were not clinically recorded by the authors.
In conclusion, RNRs are not an uncommon observation on MRI. This condition is associated with variable degrees of degenerative LCS, and the RNRs have distinctive morphological configurations and locations in relation to the level of stenosis. The effect of RNRs on the post-surgical clinical outcome remains a debate. Therefore, further larger studies regarding the contribution of the presence of RNRs on post-surgical outcome is recommended to assess their importance. Nevertheless, RNRs should be recognized on MRI, and radiologists should report on the associated details. We emphasize the importance of development of a classification system and a common language that can be used among the radiologists and treating surgeons and that place the emphasis on the shapes and locations of the RNRs in order to facilitate adequate surgical planning and to aid in determining the prognosis of the clinical outcome in the future.
Footnotes
Author Contribution
LA Rousan: Conceptualization, original draft writing, review and editing. Methodology, project administration. MH Al-Omari: draft review and editing. RM Musleh: data curation. MI Amir: data curation. H Al-Kortobi: data curation. NAbdo: formal data analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.