
Abstract
Study Design:
Retrospective cohort study.
Objective:
The present study analyzes complication rates and episode-based costs for patients with and without diabetes mellitus (DM) following posterior lumbar fusion (PLF).
Methods:
PLF cases at a single institution from 2008 to 2016 were queried (n = 3226), and demographic and perioperative data were analyzed. Patients with and without the diagnosis of DM were compared using chi-square, Student’s t test, and multivariable regression modeling.
Results:
Patients with diabetes were older (63.10 vs 56.48 years, P < .001) and possessed a greater number of preoperative comorbidities (47.84% of patients had Elixhauser Comorbidity Index >0 vs 42.24%, P < .001) than did patients without diabetes. When controlling for preexisting differences, diabetes remained a significant risk factor for prolonged length of stay (OR = 1.59, 95% CI 1.26-2.01, P < .001), intensive care unit stay (OR = 1.52, 95% CI 1.07-2.17, P = .021), nonhome discharge (OR = 1.86, 95% CI 1.46-2.37, P < .001), 30-day readmission (OR = 2.15, 95% CI 1.28-3.60, P = .004), 90-day readmission (OR = 1.65, 95% CI 1.05-2.59, P = .031), 30-day emergency room visit (OR = 2.15, 95% CI 1.27-3.63, P = .004), and 90-day emergency room visit (OR = 2.27, 95% CI 1.41-3.65, P < .001). Cost modeling controlling for overall comorbidity burden demonstrated that diabetes was associated with a $1709 increase in PLF costs (CI $344-$3074, P = .014).
Conclusions:
The present findings indicate a correlation between diabetes and a multitude of postoperative adverse outcomes and increased costs, thus illustrating the substantial medical and financial burdens of diabetes for PLF patients. Future studies should explore preventive measures that may mitigate these downstream effects.
Introduction
Posterior lumbar fusion (PLF) is one of the most common spinal surgeries performed, and has been demonstrated to be highly effective at managing a myriad of spinal deformities and degenerative pathologies.1,2 Shifting demographics are leading to a progressively more aged population, which has served to increase the demand for effective degenerative spine disease treatment. 3 This aging population is burdened by significantly higher rates of comorbidities, thus escalating the complexity of their medical and surgical management.4-6 Furthermore, PLF costs continue to rise without a corresponding improvement in functional outcomes. 7 A more comprehensive understanding of how preexisting comorbidities impact PLF outcomes would better allow health care professionals to anticipate risks, streamline patient care, and target areas for improvement.
Diabetes mellitus (DM) is a highly prevalent disease with the capacity to adversely affect nearly every major organ system. 8 In 2015, 9.4% of the US population (or 30.3 million Americans) had a diagnosis of DM, and 1.5 million new Americans are predicted to be diagnosed each year. 9 DM has been demonstrated as a risk factor for a variety of complications within medical and surgical spheres. Specifically for spine surgery, DM has been implicated in changes in bone metabolism, leading to increased fracture risks, 10 and has additionally been associated with an elevated risk of surgical site infection (SSI), one of the leading causes of postoperative readmissions.11,12 The literature exploring the effect of DM on outcomes in spine surgery, however, yields conflicting results. Prior studies have illustrated that diabetes is associated with higher rates of 30-day unplanned readmissions, 13 longer lengths of stay (LOS), 14 and increased 2-year SSI-related reoperation rates. 15 Whether these effects are due to diabetes alone or its numerous associated comorbidities, however, is yet to be elucidated.
The present study employs an institutional database to provide additional evidence regarding the effects of diabetes on PLF outcomes and costs. The present analysis compares the rates of postoperative complications, readmissions, and emergency room (ER) visits between patients with and without DM, and explores whether, in a controlled multivariate model, diabetes is an independent risk factor for a variety of adverse postoperative events. Finally, the present study provides a cost modeling analysis of the effects of a DM diagnosis on PLF-associated expenditures.
Materials and Methods
Institutional review board approval was obtained for the present study, and informed consent was waived. Patients undergoing elective inpatient PLF at a single institution from January 1, 2008 to November 30, 2016 were queried for perioperative and postoperative data. Patients undergoing PLF were identified using the Current Procedural Terminology (CPT) codes 22 630, 22 633, and 22 612. Patients undergoing outpatient PLF and PLF for tumors, trauma, and infections were excluded.
Patients with DM were characterized utilizing the International Classification of Diseases Ninth and Tenth Revision (ICD-9, ICD-10) codes 250.xx, E10.xxxx, E11.xxxx, and E13.xxxx. Demographic variables studied included age, gender, number of segments fused, and revision status. Preoperative diagnosis was characterized, and comorbidity burden was described utilizing the Elixhauser Comorbidity Index (ECI).16,17 The ECI was created using administrative records of ICD-9 and ICD-10 codes, as has been described previously, 18 and comorbidities were weighted utilizing the van Walraven weighting system, as this has been shown to have a high degree of accuracy for predicting orthopedic complications.19,20 Although DM is an included comorbidity in the original ECI, the van Walraven weighting system multiplies DM status by zero, leading to its noninclusion in this modified ECI, and thereby preventing it from causing issues of collinearity. Complicated and uncomplicated diabetes were separated on the basis of microvascular complications, as defined in the calculation of the ECI.
Other perioperative and postoperative complications were identified using a similar coding structure based on ICD-9 and ICD-10. These postoperative complications included airway complications, bleeding, anemia, acute kidney injury, acute myocardial infarction, cardiac arrest, sepsis, septic shock, superficial surgical site infection, urinary tract infection (UTI), deep vein thrombosis (DVT), pulmonary embolism (PE), pneumonia, cerebrovascular accident (CVA), wound dehiscence, durotomy, and death. Other outcomes, including delayed extubation (defined as extubation not occurring in the operating room), required ICU stay, nonhome discharge, prolonged LOS (defined as ≥75th percentile of the cohort), and 30- and 90-day readmissions and ER visits were also studied.
All statistical analyses were performed on Statistical Analysis Software version 9.4 (SASv9.4). Categorical variables were analyzed using chi-square and Fisher’s Exact test, and continuous variables were analyzed utilizing the Mann-Whitney U test (for nonparametric distributions) or Student’s t test. For display purposes, the weighted ECI is grouped into 4 groups (<0, 0, 1-4, ≥5), but it was left as a continuous variable in all models. After these univariate analyses, multivariable logistic regression models were created for various outcomes, controlling for age, gender, ECI score, number of segments fused, revision status, preoperative diagnosis, and complications from diabetes. Cost modeling was performed with sequentially built linear regression models, such that each of the four models added variables to the previous model’s covariates. The first model included only diabetes, while the second model added patient age, gender, ECI score, number of segments fused, revision status, preoperative diagnosis, and complications from diabetes. The third model added intraoperative fluids, blood products, and time to the second model, while the final model added number of days in the ICU and LOS to the third model. Furthermore, a sensitivity analysis was performed comparing patients with complicated and uncomplicated diabetes to understand the differing demographic factors and postoperative outcomes of these two patient cohorts, with the ultimate goal of comparing patients with differing severities of diabetes.
Results
During the time period studied, 3226 patients were identified within a single institution as having undergone elective posterior lumbar fusion. Of this cohort, 508 patients had a diagnosis of DM (Table 1). PLF patients with DM were significantly older (63.10 vs 56.48 years, P < .001) and possessed higher comorbidity burdens than did patients without diabetes, as characterized by ECI score (47.84% of patients had ECI > 0 vs 42.24%, P < .001). A total of 14.57% of PLF patients with diabetes suffered preoperatively from one or more diabetic complications (vs 0% of patients without diabetes, P < .001). The number of segments fused did not differ substantially between patients with and without diabetes (medians of 3 and 2, respectively, P = .188). Similarly, rates of revision surgery between patients with and without diabetes (19.29% vs 16.81%, P = .174) did not differ.
Characteristics of PLF Patients With and Without Diabetes.
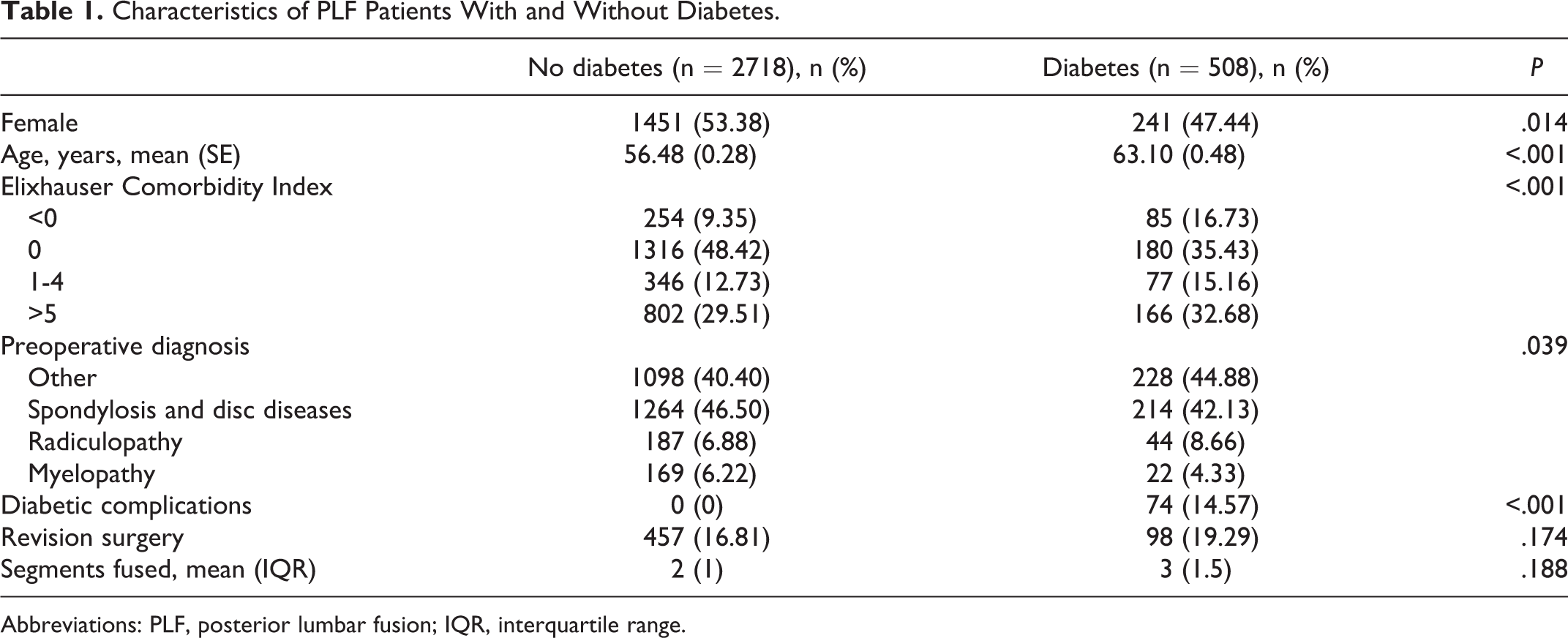
Abbreviations: PLF, posterior lumbar fusion; IQR, interquartile range.
As can be seen in Table 2, patients with DM were significantly more likely to experience postoperative acute kidney injury (3.35% vs 1.14%, P < .001), myocardial infarction (2.56% vs 1.14%, P = .011), cardiac arrest (2.76% vs 1.18%, P = .006), and pneumonia (3.54% vs 1.55%, P = .002). Patients with diabetes were not more likely to experience an airway complication (0.20% vs 0.11%, P = .496), cerebrovascular accident (0.15% vs 0.20%, P = .576), DVT (0.20% vs 0.15%, P = .576), superficial skin infection (0.79% vs 0.37%, P = .257), sepsis (0.59% vs 0.18%, P = .118), septic shock (0.39% vs 0.15%, P = .241), durotomy (3.35% vs 3.13%, P = .796), or death (0.39% vs 0.07%, P = .119).
Comparison of Adverse Events in PLF Patients With and Without Diabetes.
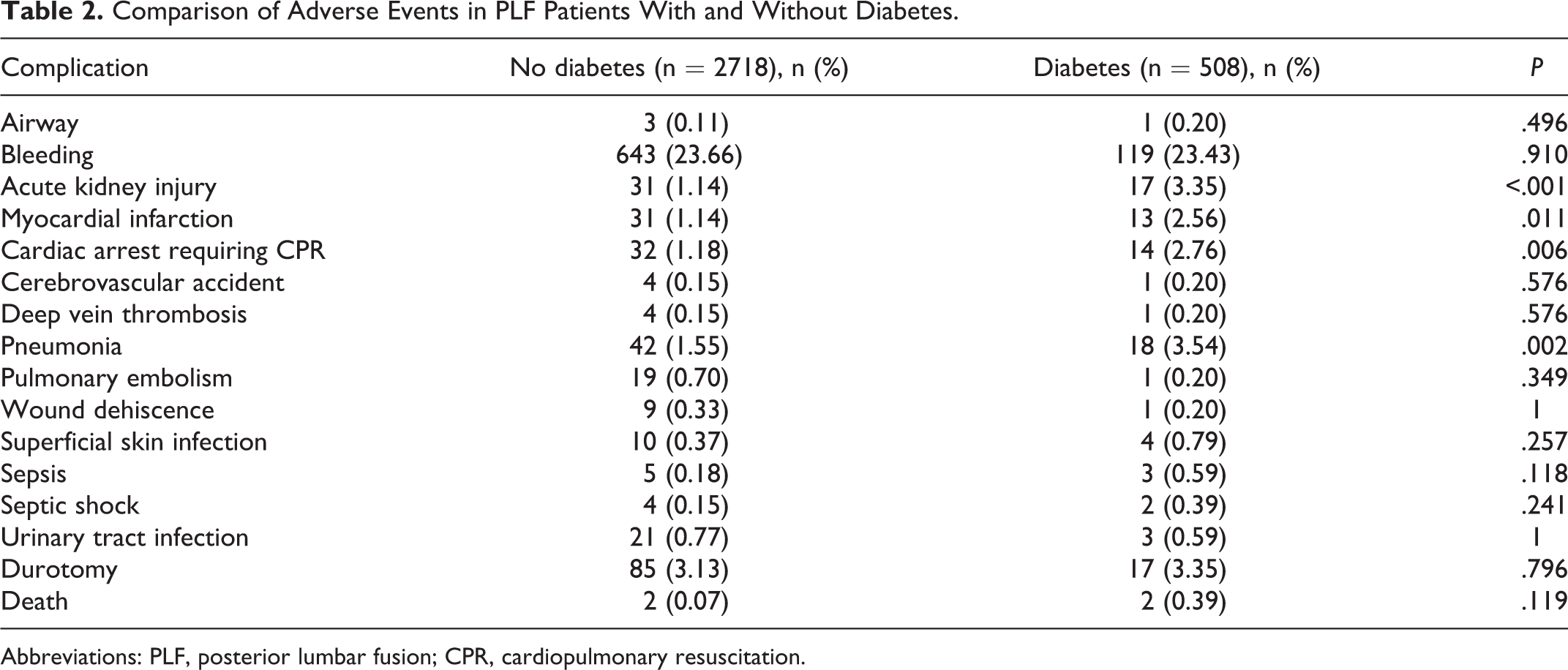
Abbreviations: PLF, posterior lumbar fusion; CPR, cardiopulmonary resuscitation.
In multivariable modeling, a diagnosis of DM proved to be an independent risk factor for postoperative ICU stay (OR = 1.52, 95% CI 1.07-2.17, P = .021), nonhome discharge (OR = 1.86, 95% CI 1.46-2.37, P < .001), prolonged LOS (OR = 1.59, 95% CI 1.26-2.01, P < .001), 30-day readmission (OR = 2.15, 95% CI 1.28-3.60, P = .004), 90-day readmission (OR = 1.65, 95% CI 1.05-2.59, P = .031), 30-day ER visit (OR = 2.15, 95% CI 1.27-3.63, P = .004), and 90-day ER visit (OR = 2.27, 95% CI 1.41-3.65, P < .001). A detailed report of individual postoperative complications and their rates amongst patients with and without diabetes can be found in Table 3.
Episode-Based Outcomes of PLF Patients With and Without Diabetes.
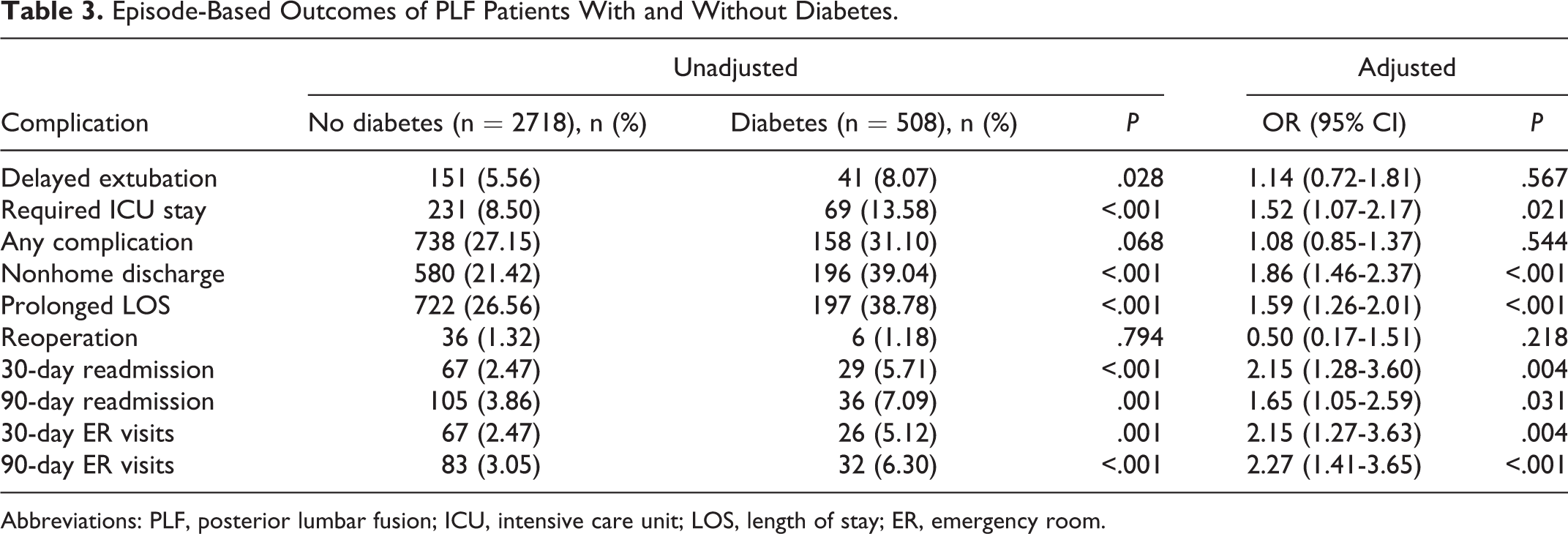
Abbreviations: PLF, posterior lumbar fusion; ICU, intensive care unit; LOS, length of stay; ER, emergency room.
Table 4 shows a sequence of cost models that controlled for a multitude of patient demographics and intraoperative features. Cost modeling indicated that PLF in patients with diabetes was associated with a $2834 increase in costs (95% CI $1184-$4483, P < .001) when compared with PLF in patients without DM. When controlling for age, gender, preoperative diagnosis, diabetic complications, ECI score, revision status, and number of segments fused, DM was significantly associated with a $1709 increase in costs (95% CI $344-$3074, P = .014). A third model controlling for operative time and colloid and crystalloid utilization, in addition to the aforementioned variables, demonstrated that DM was associated with $882 more in overall costs (95% CI −$340 to $2105, P = .157). Last, when controlling for the above variables and length of hospital and ICU stays, a diagnosis of DM was associated with a $349 increase in costs (95% CI −$760 to $1458, P = .537).
Sequential Cost Modeling for PLF Patients With Diabetes.
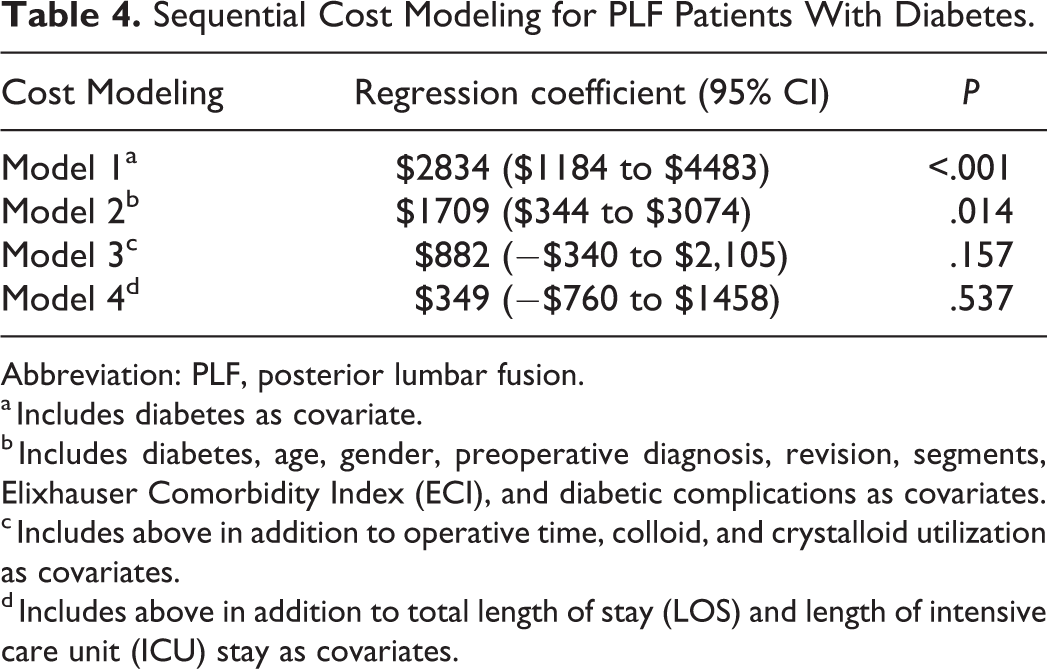
Abbreviation: PLF, posterior lumbar fusion.
a Includes diabetes as covariate.
b Includes diabetes, age, gender, preoperative diagnosis, revision, segments, Elixhauser Comorbidity Index (ECI), and diabetic complications as covariates.
c Includes above in addition to operative time, colloid, and crystalloid utilization as covariates.
d Includes above in addition to total length of stay (LOS) and length of intensive care unit (ICU) stay as covariates.
Supplementary Table 1 provides the results of a sensitivity analysis performed on patients with complicated and uncomplicated diabetes. Though these 2 subgroups experienced comparable rates of most complications included in the analysis, patients with complicated diabetes experienced significantly higher rates of delayed extubation (14.86% vs 6.91%, P = .020), nonhome discharge (52.70% vs 36.68%, P = .009), and 30- and 90-day readmissions (10.81% vs 4.84%, P = .041 and 13.51% vs 5.99%, P = .020, respectively).
Discussion
The results of the present study indicate that a diagnosis of DM in PLF patients is associated with a plethora of adverse postoperative outcomes, higher likelihood of readmission, and higher overall episodic costs. These findings illustrate the tremendous medical and financial burdens of diabetes for PLF patients and add an important voice to the existing body of literature studying the role that diabetes plays in a myriad of adverse outcomes.
Table 2 illustrates the substantial divergence in postoperative complications between patients with and without DM. This data is supported by numerous other studies within spine surgery and PLF specifically, which have found DM to be a risk factor for a range of adverse postoperative events, such as wound infection, pneumonia, sepsis, and UTI.13-15,21,22 At the univariate level, patients with diabetes experienced a higher prevalence of delayed extubation. This effect did not endure in an adjusted model (Table 3), suggesting that this complication is likely due to demographic differences or additional afflictions often found to be comorbid with diabetes (eg, hypertension, hyperlipidemia, chronic kidney disease, cardiovascular disease, sleep apnea, etc). 23 Corroborating these findings are several additional studies, conducted within spine surgery overall, which illustrate diabetes as being associated with, but not an independent risk factor for, common postoperative complications such as the aforementioned.21,22,24
The present study illustrates a significant increase in both 30- and 90- day readmissions and ER visits, required ICU stays, prolonged LOS, and non-home discharges. These findings retained their significance in a multivariate model accounting for preexisting differences, suggesting that DM is an independent risk factor for a variety of episode-based outcomes. Though many sources utilizing multivariate analysis espouse diabetes as a significant risk factor for a variety of episode-based adverse outcomes,13,22 this perspective is not universal. One dissenting study, Katz et al, 25 identified diabetes as an independent risk factor for increased mortality, but not for 30-day readmissions or reoperation rates. However, Katz et al 25 included only interbody fusions, whereas the present findings are based on all posterior lumbar fusion techniques. Two additional studies of ACDF patients found diabetes to be a nonsignificant predictor of readmission when accounting for patient demographics and comorbidities. 24 The variation in procedure types and follow-up periods (30 vs 90 days) may have contributed to this divergence in findings; however, the factors accounted for within analyses likely also play a role.
When examining the postoperative effect of a disease, utilization of multivariate analysis becomes increasingly imperative if the disease is chronic and manifests within a constellation of comorbidities. Up to 75% of patients with diabetes are hypertensive, 26 and up to 40% of patients with diabetes are found to possess at least three other comorbidities, the most common of which are hyperlipidemia, cardiovascular disease, renal disease, and nonalcoholic fatty liver disease. 27 Table 1 evidences the significant preexisting differences between patients with and without DM. A greater proportion of patients with diabetes possessing an elevated ECI is unsurprising given that diabetes is often comorbid with other illnesses, and that lack of disease control may serve to raise the ECI score. 17 The ECI score has been found to be predictive of extended LOS in posterior spinal fusion, and consistently outperforms the Charlson Comorbidity Index in predicting adverse events, LOS, discharge disposition, and mortality in orthopedic surgery.19,28-30 The ECI score and other relevant preoperative differences were selected as covariates in our multivariate analysis, providing a more accurate representation of DM as an independent risk factor for a multitude of postoperative events.
Though sources largely agree that diabetes is associated, either indirectly or independently, with poorer outcomes, there is some discordance in the literature around whether the extent of disease control affects the likelihood of adverse outcomes. Some sources argue that the mere presence of a DM diagnosis, regardless of associated end-organ complications, predicts these adverse outcomes. Rubel et al 31 found that both uncomplicated diabetes and diabetes with chronic complications were independent risk factors for 90-day readmissions in patients undergoing elective primary lumbar spine surgery. In contrast, a separate study reported that patients with adequately controlled DM without comorbidities were found to have outcomes comparable to those of patients without diabetes altogether. 32 Similarly, the supplemental analysis provided here suggests that patients with complicated diabetes, and therefore implicitly poorly controlled diabetes, differ in a few key postoperative outcomes. With higher rates of delayed extubation, nonhome discharge, and 30- and 90-day readmissions despite few differences in preoperative characteristics, patients with complicated diabetes were at higher risk for poor outcomes (Supplemental Table 1). This would suggest that, though they represent just a small portion of the present study’s diabetic cohort, patients with complicated diabetes require more robust preoperative optimization and postoperative monitoring to safely undergo spine surgery. More extensive stratification by complexity of disease in future studies may further clarify this issue.
Several studies within total joint arthroplasty literature have emphasized the role that glycemic control plays in postoperative complications. Specifically, perioperative hyperglycemia, but not solely the diagnosis of DM, is associated with an increased incidence of venous thromboembolism, stroke, postoperative hemorrhage, extended length of stay, and mortality, among others.33-38 Numerous other studies have suggested that stress-induced postoperative hyperglycemia may serve as an independent risk factor for surgical site infections, even in those without DM altogether.39-42 Clinical trials and metanalyses examining surgical specialties overall have failed to show that perioperative glycemic control improves patient outcomes. In fact, one such trial found a higher rate of stroke and morbidity in the glycemic control cohort.43-45 The equivocal nature of this point may stem from subtle differences in the type of surgery, as well as the style of approach. Though stratification for glycemic control and insulin dependence is beyond the scope of the present analysis, a structured analysis of these factors specifically within PLF is warranted.
Though the present study primarily examined patient outcomes, a financially overburdened medical system requires an investigation into how diabetes affects the overall cost of PLF. The increased incidence of DM has been accompanied by staggering surges in diabetes-associated costs. One in 4 health care dollars in the United States is spent on care for people with diagnosed diabetes, and greater than 50% of that amount is directly spent on diabetes alone. 9 The International Diabetes Federation estimated that global health expenditures related to diabetes and its numerous complications reached 376 billion US dollars in 2010; that number is projected to surpass $490 billion by 2030. 32 Furthermore, when compared to those without diabetes, surgical patients with diabetes have been found to utilize 45% excess bed days. 32 These figures indicate an urgent need to both optimize outcomes for patients with diabetes and abate the rapidly growing associated costs.
Our multivariate cost model, controlling for age, gender, preoperative diagnosis, segments fused, revision status, ECI score, and presence of diabetic complications, indicates that a diagnosis of diabetes is associated with substantially increased costs of PLF. This effect disappears when controlling for intraoperative resource utilization, suggesting that these resources may govern cost differences between PLF for patients with and without diabetes. These findings land within a veritable dearth of literature speaking to the effect of diabetes on costs specifically for PLF. Within primary joint arthroplasty, one study found diabetes to be associated with a $5074 increase in 90-day charges. However, this study neglected to account for preexisting demographics or potentially confounding factors as mentioned above. 46 Browne et al 21 found that the risk- and inflation-adjusted charges of hospitalization were nearly $1300 greater in patients with diabetes than in those without when undergoing PLF specifically. When examining patients undergoing surgery for lumbar spinal stenosis, Lee et al 47 found that medical expenses were $290 higher in patients with DM. The study, however, did not account for concomitant comorbidities and demographic factors such as ECI score, age, or diabetic complications, perhaps leading to the different magnitudes of cost augmentation. When controlling for measures of comorbidity, our data indicate that these differences in cost are likely due to increased intraoperative resource use secondary to a diagnosis of diabetes, but not the medical conditions that routinely accompany diabetes.
The present study is not without its limitations. This investigation was conducted within a single institution, therefore somewhat reducing the generalizability of its findings. Though the vast majority of studies, including the present one, categorize diabetes as a binary (presence or absence of DM), the differing pathophysiology of type 1 and type 2 may merit individual analyses not included in this analysis. DM is also a spectrum of disease; although a sensitivity analysis was performed comparing patients on different ends of this spectrum, the lack of more precise measures of diabetic control also constitutes a significant limitation. Because of low rates of several complications in patients with diabetes overall, the sensitivity analysis is underpowered to recognize some differences between complicated and uncomplicated patients with diabetes. Furthermore, recent estimates suggest that the prevalence of DM is approximately 10%. As the prevalence in the present study was 16%, this likely indicates a degree of Berkson’s bias. 48 Retrospective studies such as ours are limited both by their associational, rather than causational conclusions, and the inability to control for unknown confounders. Last, the retrospective and administrative coding-based nature of the present study could lead to unintended biases that would partially confound portions of the results.
Conclusions
The present results indicate a compelling need for more comprehensive risk stratification of patients prior to posterior lumbar fusion. When used in the context of risk-benefit discussions, these findings may better equip patients to establish realistic expectations and make informed decisions regarding their care. Stratification based on A1c levels or the precise number of diabetic sequelae (eg, retinopathy, neuropathy) may provide further insight into the relationship between diabetes and postoperative outcomes. Future studies would also do well to explore the preoperative interventions most effective in optimizing the surgical candidacy of patients with DM. This study illustrates a strong correlation between DM and adverse outcomes in patients undergoing PLF, though prospective studies are required to establish a causal relationship. Nonetheless, glycemic control should not be discounted in the perioperative period.
Supplemental Material
sj-docx-1-gsj-10.1177_2192568220948480 - Diabetes Is Predictive of Postoperative Outcomes and Readmission Following Posterior Lumbar Fusion
sj-docx-1-gsj-10.1177_2192568220948480 for Diabetes Is Predictive of Postoperative Outcomes and Readmission Following Posterior Lumbar Fusion by Annie E. Arrighi-Allisan, Sean N. Neifert, Jonathan S. Gal, Lawrence Zeldin, Jeffrey H. Zimering, Jeffrey T. Gilligan, Brian C. Deutsch, Daniel J. Snyder, Dominic A. Nistal and John M. Caridi in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr John M. Caridi is a consultant for Zimmer Biomet. The remaining authors have no disclosures or conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.