
Abstract
Study Design
Retrospective Cohort.
Objective
We investigate whether duration of symptoms a patient experiences prior to lumbar microdiscectomy affects pain, lifestyle, and return to work metrics after surgery.
Methods
A retrospective review of patients with a diagnosis of lumbar radiculopathy undergoing microdiscectomy was conducted using a statewide registry. Patients were grouped based on self-reported duration of symptoms prior to surgical intervention (Group 1: symptoms less than 3 months; Group 2: symptoms between 3 months and 1 year; and Group 3: symptoms greater than 1 year). Radicular pain scores, PROMIS PF Physical Function measure (PROMIS PF), EQ-5D scores, and return to work rates at 90 days, 1 year, and 2 years after surgery were compared using univariate and multivariate analysis.
Results
There were 2408 patients who underwent microdiscectomy for lumbar disc herniation for radiculopathy with 532, 910, and 955 in Groups 1, 2, and 3, respectively. Postoperative leg pain was lower for Group 1 at 90 days, 1 year, and 2 years compared to Groups 2 and 3 (P < .05). Postoperative PROMIS PF and EQ-5D scores were higher for Group 1 at 90 days, 1 year, and 2 years compared to Groups 2 and 3 (P < .05).
Conclusion
Patients with prolonged symptoms prior to surgical intervention experience smaller improvements in postoperative leg pain, PROMIS PF, and EQ-5D than those who undergo surgery earlier. Patients undergoing surgery within 3 months of symptom onset have the highest rates of return to work at 1 year after surgery.
Introduction
Background
Intervertebral disc herniations represent one of the most common spinal pathologies requiring surgery. Lumbar disc herniations can cause severe debilitating pain which places a great burden on patients and the health care system alike. 1 The radiculopathy associated with lumbar disc herniation results in reduced patient quality-of-life across multiple metrics including the Patient-Reported Outcomes Measurement Information System PROMIS PF, and Euroqol (EQ-5D).2,3
Initial management of intervertebral disc herniation involves conservative measures with physical therapy, anti-inflammatory medications, and epidural spinal injections. 4 Most patients experience relief of symptoms within 6 weeks; however, some have progression of symptoms. 5 In these cases, surgical treatment has been shown to provide effective relief of symptoms from lumbar disc herniation.6,7 Despite the high success ranging from 78-95% for microdiscectomies, some authors argue that poor outcomes may occur due to the duration of pre-operative symptoms (i.e., motor deficits, sensory changes, persistent low back pain, or persistent radiculopathy).6,8–10
Earlier surgical intervention has been shown to result in faster pain relief and better functional and clinical outcomes relative to conservative management, while delay in surgery may result in significantly worse outcomes.2,10,11 Multiple studies have evaluated the effects of the duration of symptoms on outcomes following microdiscectomy, suggesting that increased symptom duration caused by lumbar disc herniation may result in poorer outcomes following treatment.12,13 However, other studies have suggested that there is limited or inconclusive evidence to suggest a relationship between the duration of symptoms and post-operative success. 14 Movassaghi et al 15 (n = 210) assessed patient-reported outcomes and reported that the duration of symptoms prior to surgery did not notably influence postoperative clinical outcomes, the frequency of subsequent operations, or the level of patient satisfaction. The polarized differences in the literature have emphasized the indeed for large multi-institutional studies assessing whether there truly is a relationship between symptom chronicity and postoperative outcomes.
Large multi-center research registries are increasing in popularity. The Michigan Spine Surgery Improvement Collaborative (MSSIC) is a collaborative quality initiative with the goal of improving spine surgery outcomes throughout the state of Michigan.16,17 MSSIC maintains a comprehensive data registry from across 29 hospital sites that includes demographic and pre-surgical clinical data, as well as individual patient surgical procedure information including complications and/or adverse events. MSSIC quality initiatives have led to a 15.1% reduction in readmissions from 2017 to 2018, allowing the organization to expand its agenda on patient-reported outcomes pre- and post-spine surgery. 17
The purpose of this study was to use the MSSIC database to examine the effect of the duration of symptoms on outcomes following lumbar microdiscectomy. We hypothesized that patients with a longer duration of pre-operative symptoms have less favorable clinical outcomes compared to those with a shorter duration of symptoms. This information may help spine surgeons and their patients to understand the optimal time for surgical intervention of lumbar disc herniations.
Patients/Methods
A retrospective review was conducted by examining prospectively compiled data from the MSSIC registry. The MSSIC is a quality improvement initiative that involves a diverse range of orthopedic surgeons and neurosurgeons from private, academic, rural, and urban contexts. The registry includes data from elective spine surgeries for degenerative diseases, excluding non-degenerative and/or complex pathologies.
This study protocol was approved by our institutional review board. A retrospective cohort study was performed using the MSSIC registry between June 1, 2016 to December 4, 2020. Informed consent was waived since data collection was part of routine care in a de-identified fashion. Patients who underwent a standard primary single-level lumbar microdiscectomy for radiculopathy were identified based on International Classification of Diseases 10 th revision code (ICD-10). Patients who were under 18 years of age at the time of surgery and patients who had undergone fusion were excluded. 2408 patients were identified who met inclusion criteria. Patients were excluded if they had any previous lumbar surgery, were pregnant, or had more than 1 level operated on.
Patients were separated into three groups based on self-reported duration of symptoms prior to surgical intervention. Prior to surgery, Group 1 had symptoms for <3 months; Group 2 had symptoms >3 months but <1 year; and Group 3 had symptoms for 1 year or greater (Figure 1). Baseline patient characteristics include age, gender, race, body mass index (BMI), education, diabetes, deep vein thrombosis (DVT), coronary artery disease (CAD), depression, anxiety, osteoporosis, ambulation status, private insurance, previous spine surgery, hypertension, current smoking status, current work status, and ASA scores were collected. Pre- and post-operative 0-10 radicular pain rating scores, PROMIS PF Physical Function four-item Short Form (PROMIS PF), EQ-5D scores, as well as self-reported return to work rates at 90 days, 1 year, and 2 years after surgery were collected on all patients and compared among groups. For PROMIS PF, EQ-5D, and 0-10 pain ratings, patients were classified as “yes” or “no” in terms of whether they had achieved at least a “Minimum Clinically Important Difference” (MCID) degree of improvement from baseline to follow-up point. Patient distribution based on symptom duration.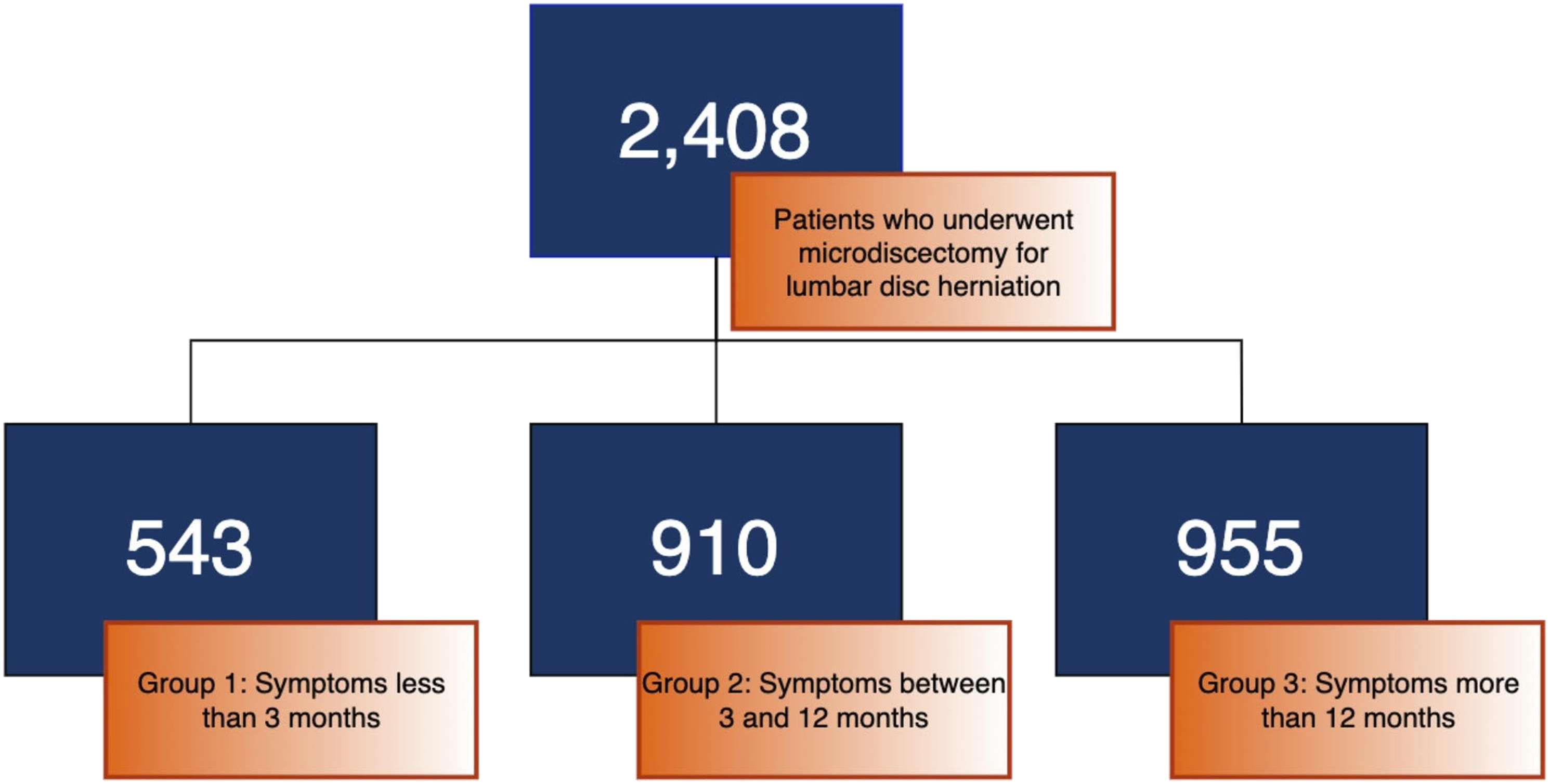
Ethical Approval
This study was reviewed by Beaumont Hospital IRB committee and was determined to be exempt from institutional review board approval (IRB number # 2019-379).
Statistical Analysis
Univariate comparisons were performed for demographic, medical history, and complication variables between patient symptom duration groups of <3 months, >3 months but <1 year, and 1 year or more. T-tests were used for normally distributed continuous variables, while Wilcoxon Rank Sum tests were used for continuous skewed variables, and Chi-square tests were performed for categorical variables. Poisson generalized estimating equation (GEE) models were used for multivariate analysis to determine patient and operative characteristics associated with PROMIS PF minimum clinically important difference (MCID), EQ-5D MCID, Leg pain MCID, and complications at 90 days, 1 year, and 2 years. For continuous EQ-5D at 90 days, 1 year, and 2 years, normal GEE models were used for multivariate analysis. Variables adjusted for during multivariate analysis include age, gender, race, education, BMI, diabetes, DVT, CAD, depression, anxiety, osteoporosis, ASA >2, independent ambulation pre-op, private insurance, previous spine surgery, hypertension, current smoking status, and appropriate baseline score. All analyses are performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) with statistical significance set at P < .05.
Results
Demographics
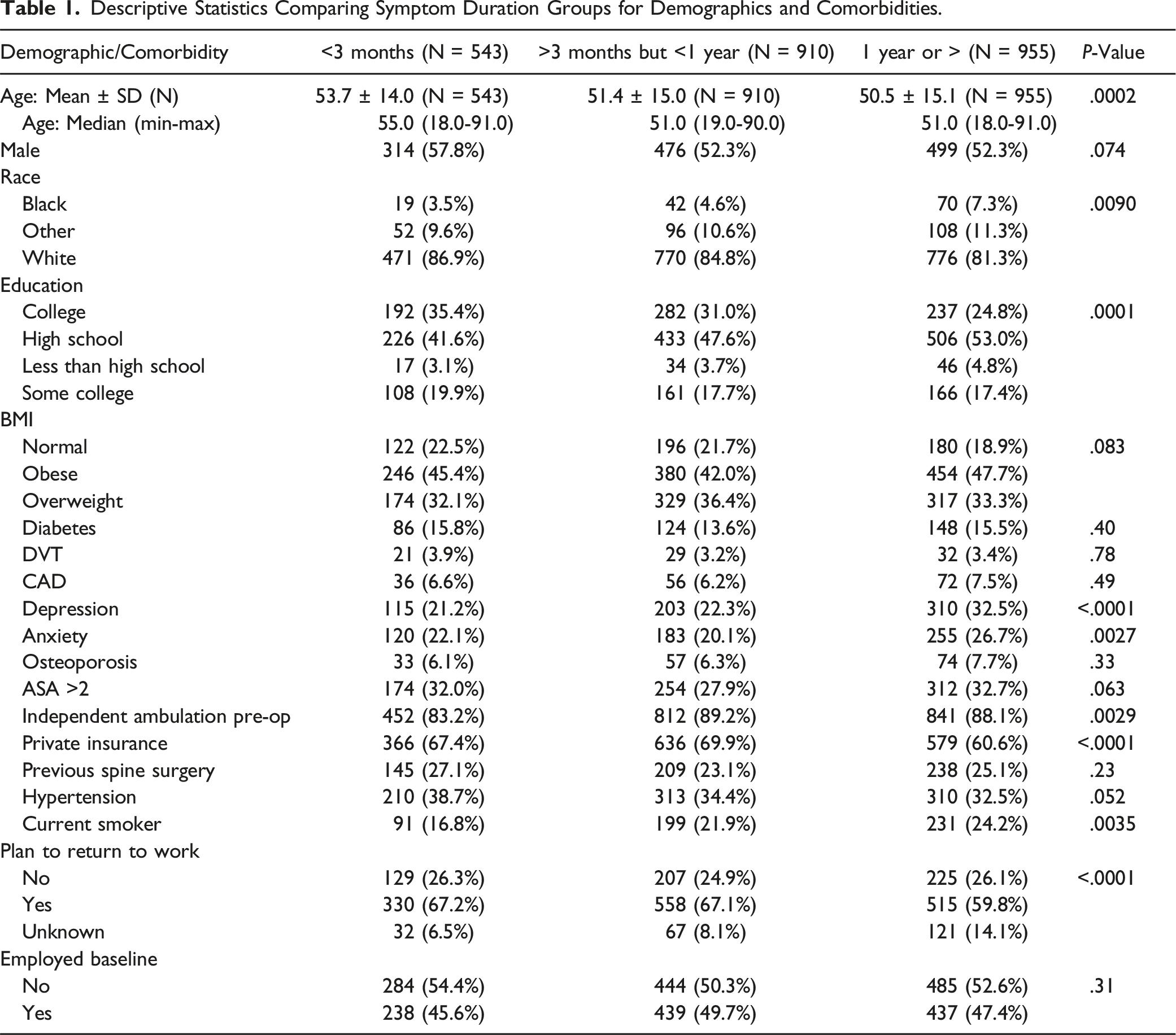
Descriptive Statistics Comparing Symptom Duration Groups for Demographics and Comorbidities.
Comparison of Metrics Pre-Operatively
Descriptive Statistics Comparing Symptom Duration Groups for Baseline Values.

Analysis of Leg Pain Scores & Lifestyle Metrics
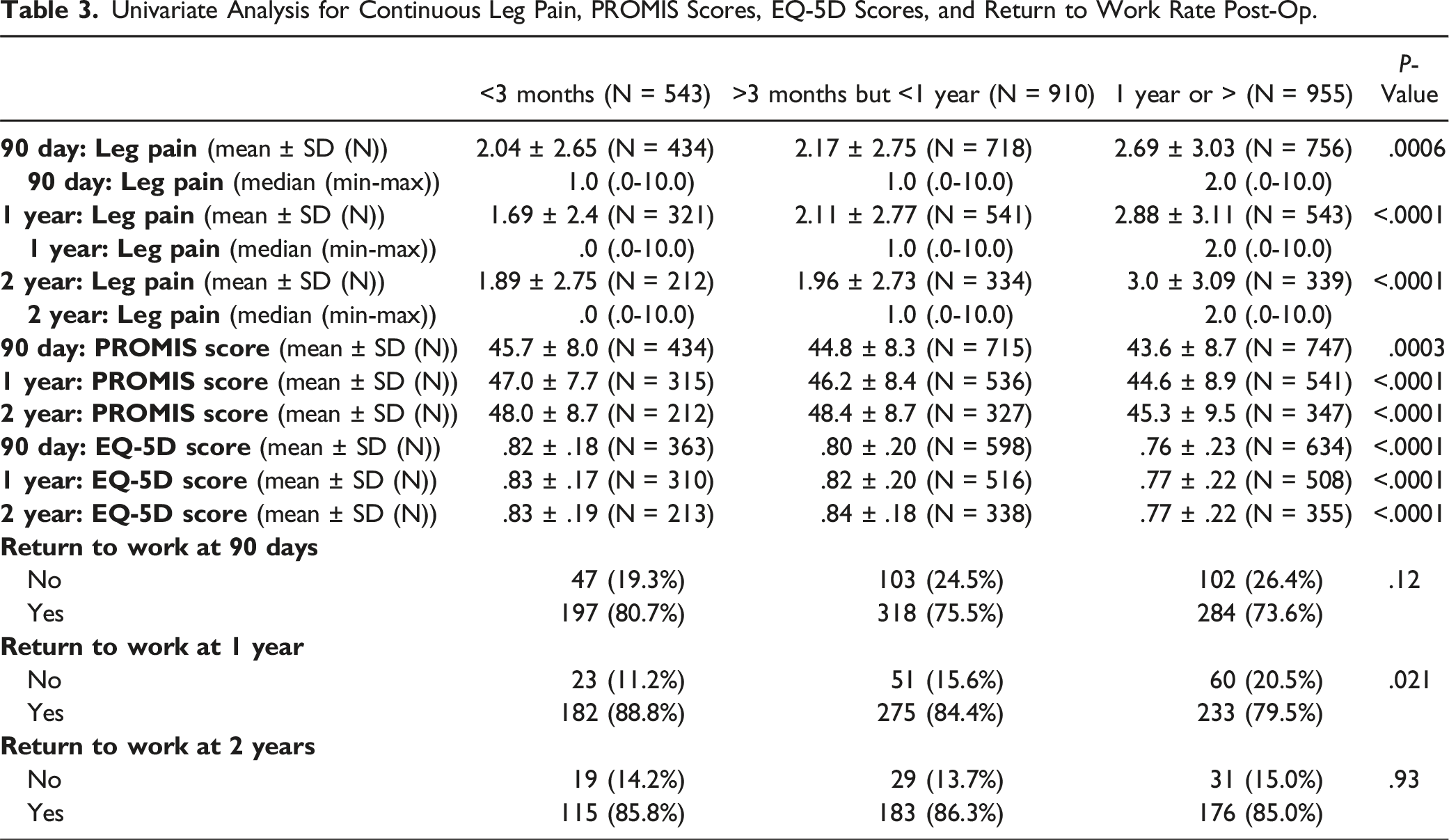
Univariate Analysis for Continuous Leg Pain, PROMIS Scores, EQ-5D Scores, and Return to Work Rate Post-Op.
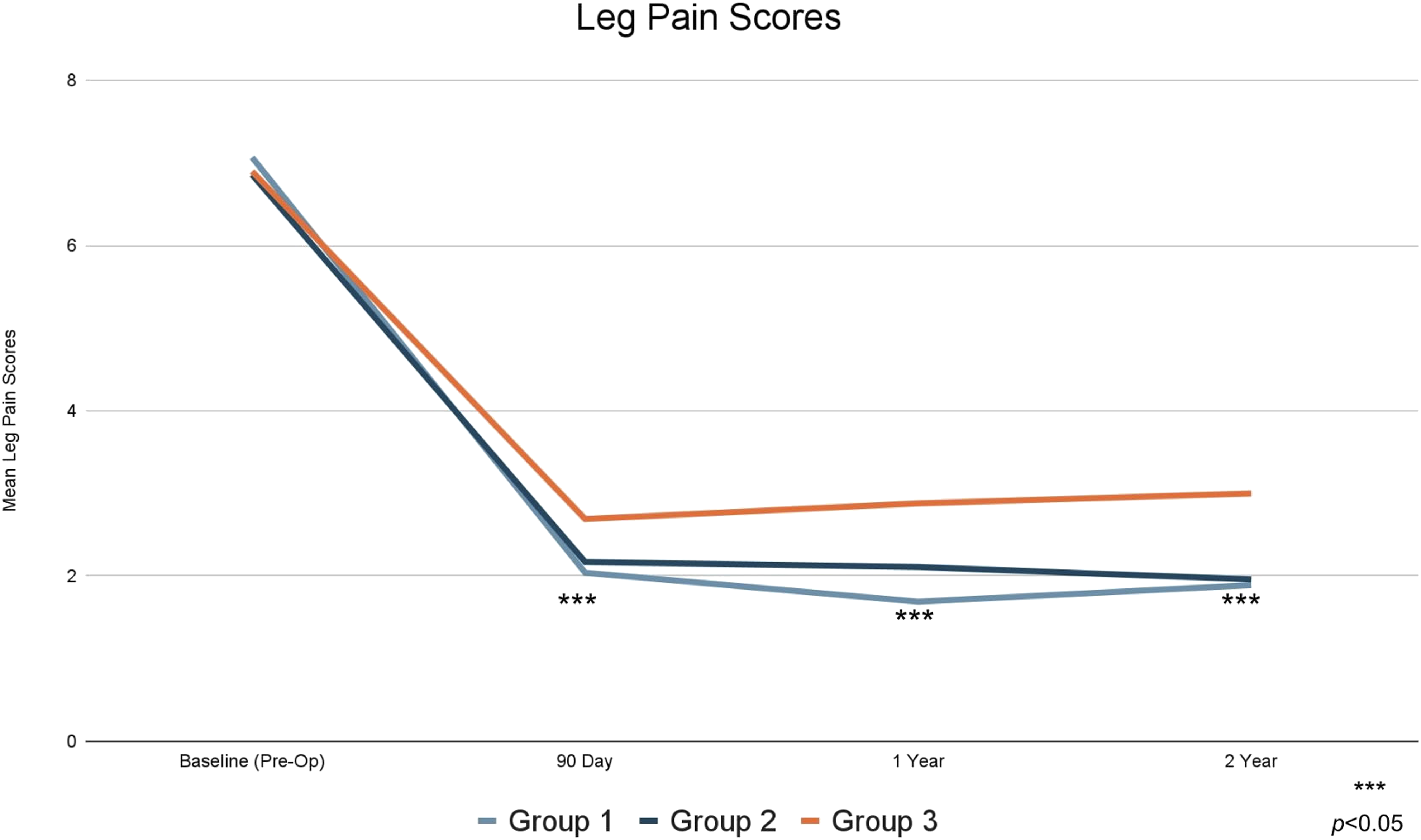
Mean leg pain scores.
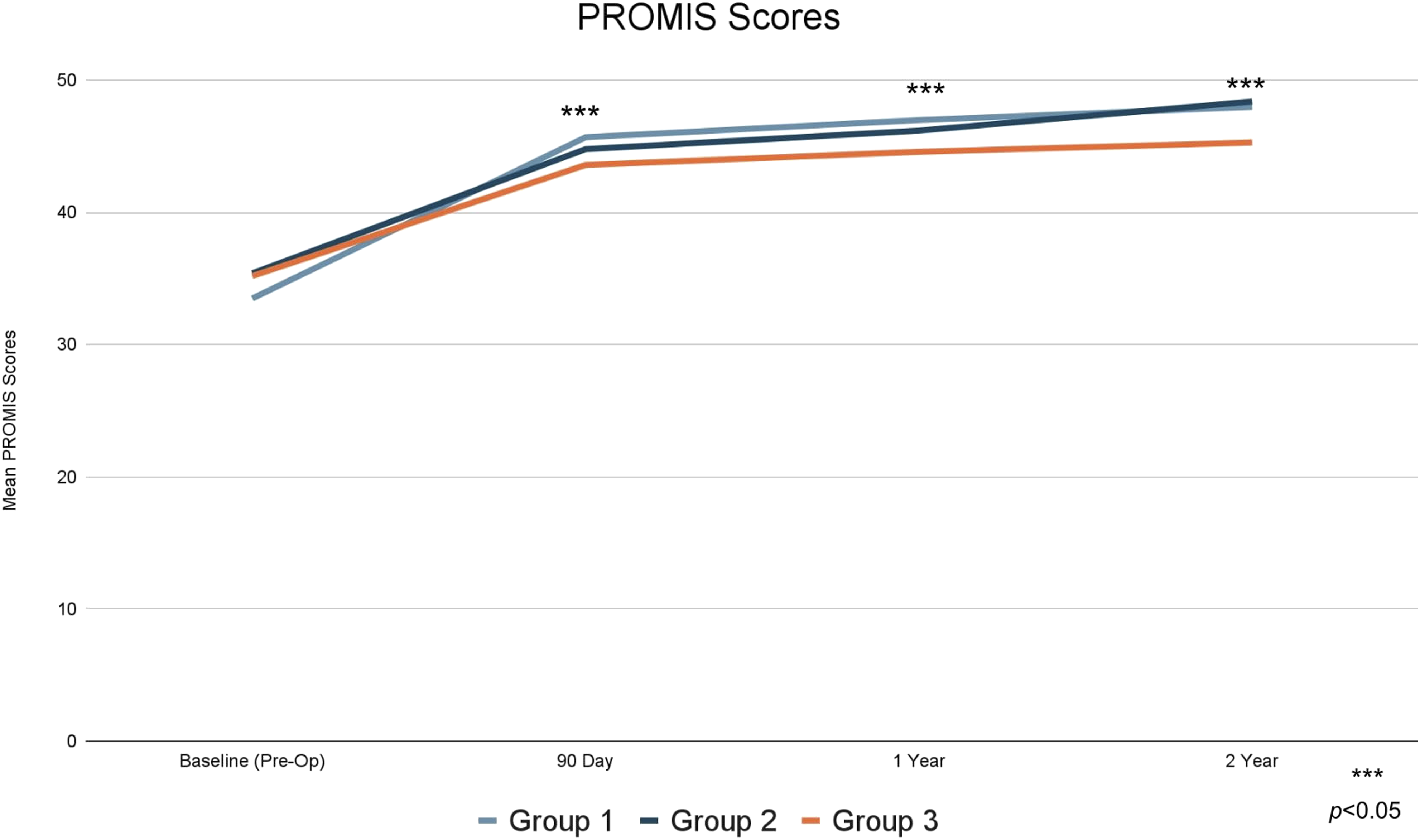
Mean PROMIS PF scores.
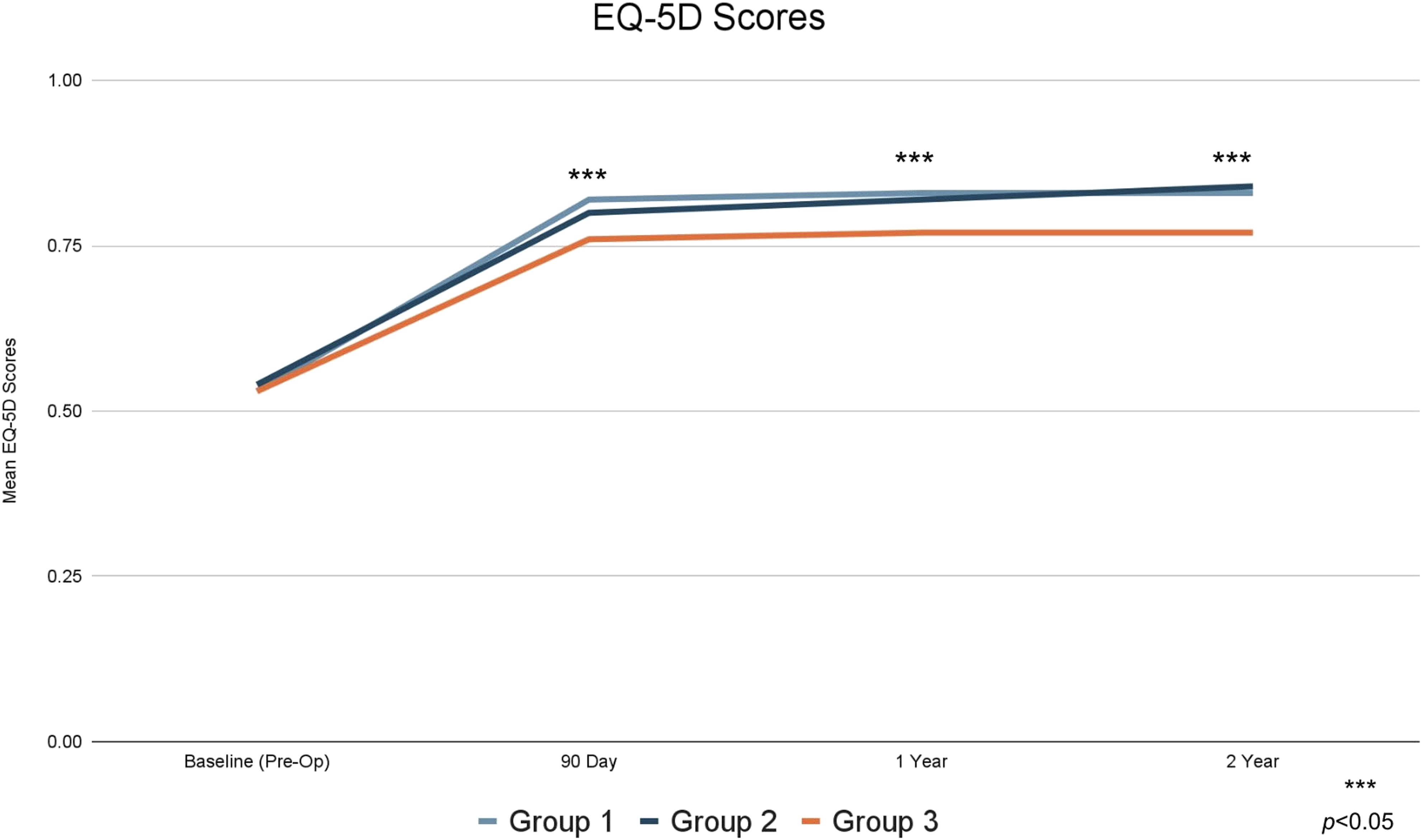
Mean EQ-5D scores.
Analysis of Return to Work
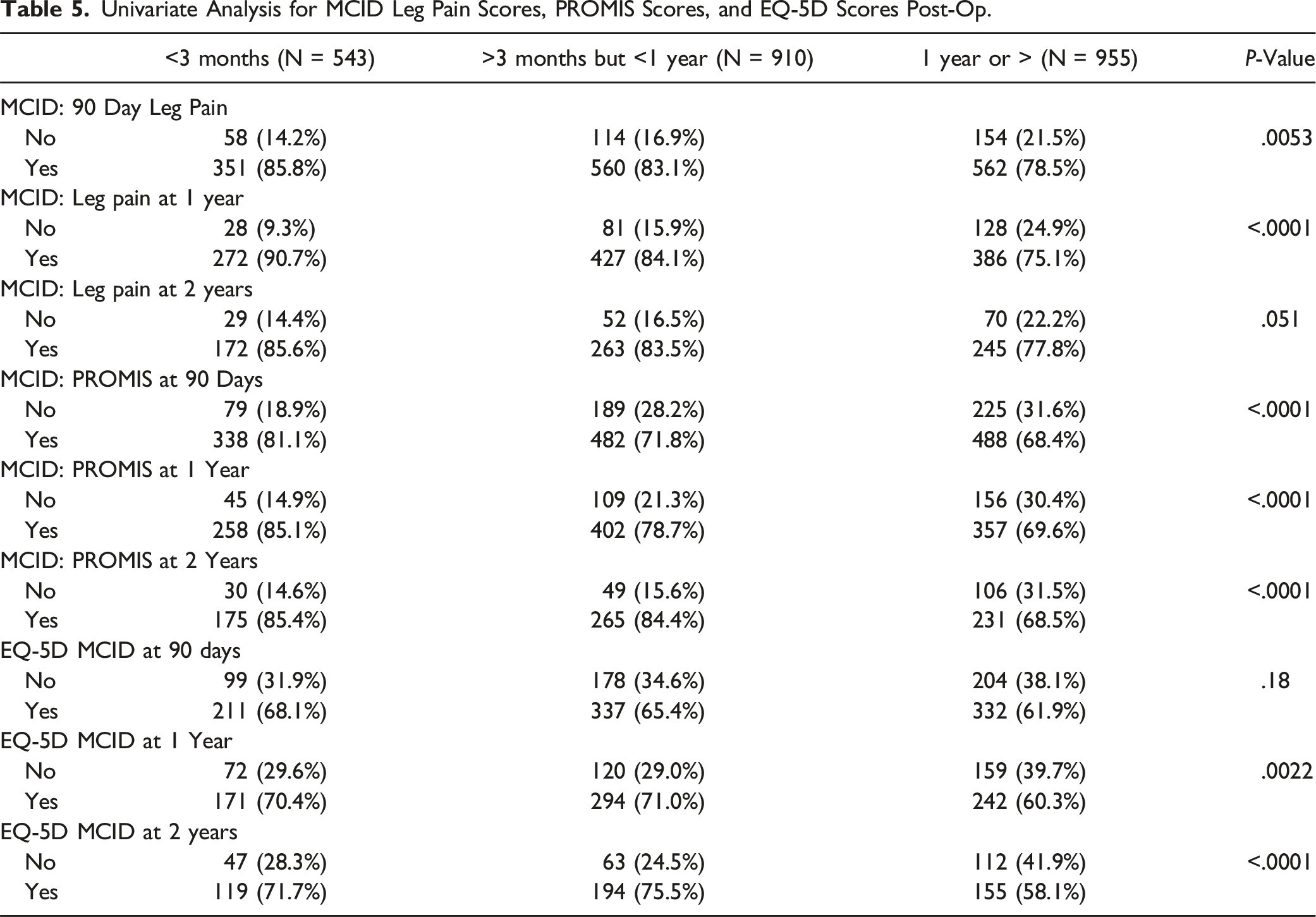
Patients who had symptoms less than 3 months prior to surgery were more likely to return to work (P < .05) at 1 year after surgery (return to work rate = 88.8% vs 84.4% vs 79.5% for Group 1, Group 2, and Group 3, respectively) (Figure 5). When comparing Group 1 to both Group 2 and Group 3, minimal clinically improved differences (MCID) were achieved by a higher proportion of patients after surgery for PROMIS PF at all time points (P < .05), EQ-5D at 1 year and 2 years (P < .05), and leg pain at 90 days and 1 year (P < .05). Return to work rates.
Multivariate Analysis of Metrics
Multivariate Analysis for Continuous Leg Pain, PROMIS Scores, EQ-5D Scores, and Return to Work Rate Post-Op.
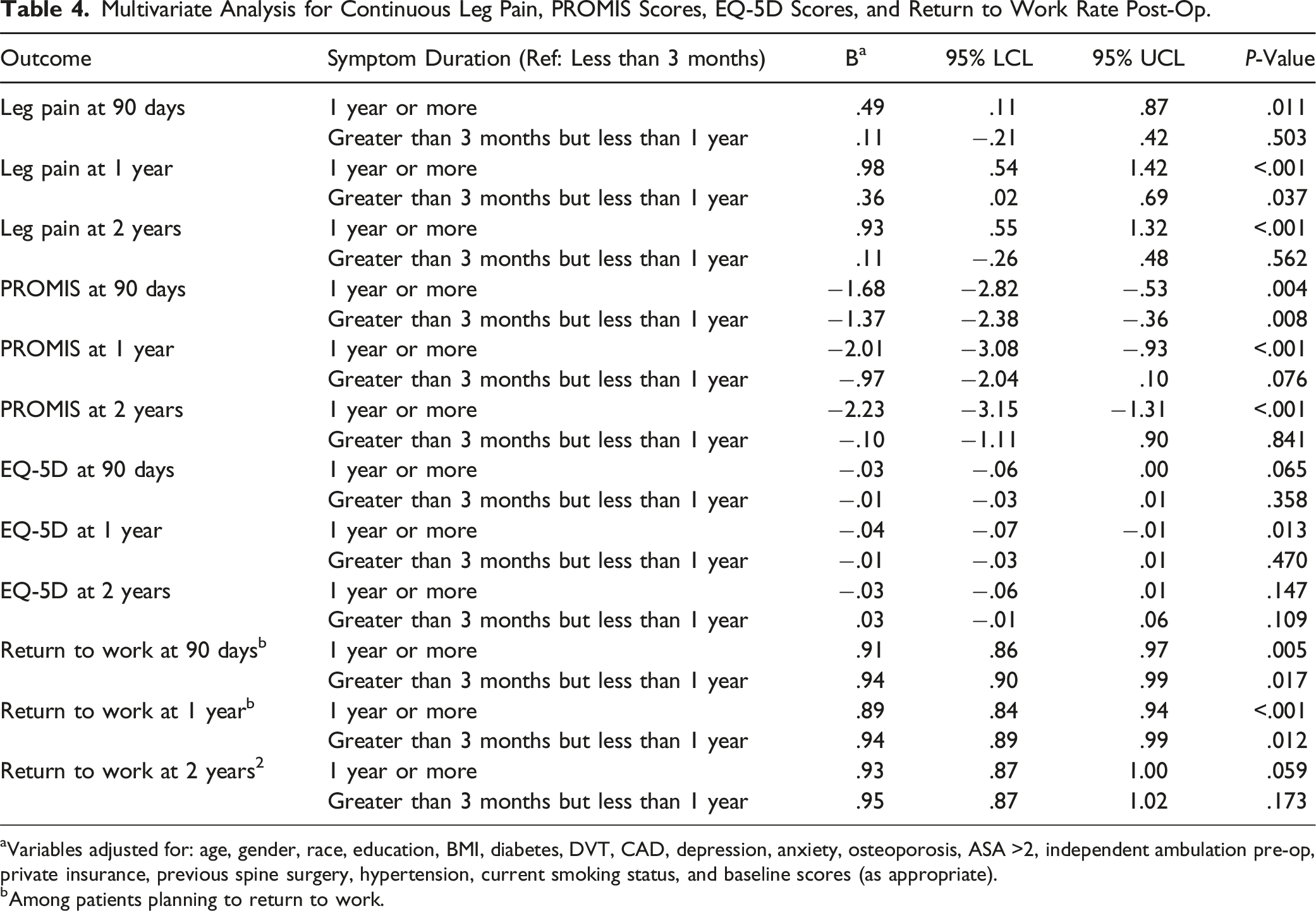
aVariables adjusted for: age, gender, race, education, BMI, diabetes, DVT, CAD, depression, anxiety, osteoporosis, ASA >2, independent ambulation pre-op, private insurance, previous spine surgery, hypertension, current smoking status, and baseline scores (as appropriate).
bAmong patients planning to return to work.
Univariate & Multivariate Analysis of MCID
Univariate Analysis for MCID Leg Pain Scores, PROMIS Scores, and EQ-5D Scores Post-Op.
Multivariate Analysis for MCID Leg Pain Scores, PROMIS Scores, and EQ-5D Scores Post-op.
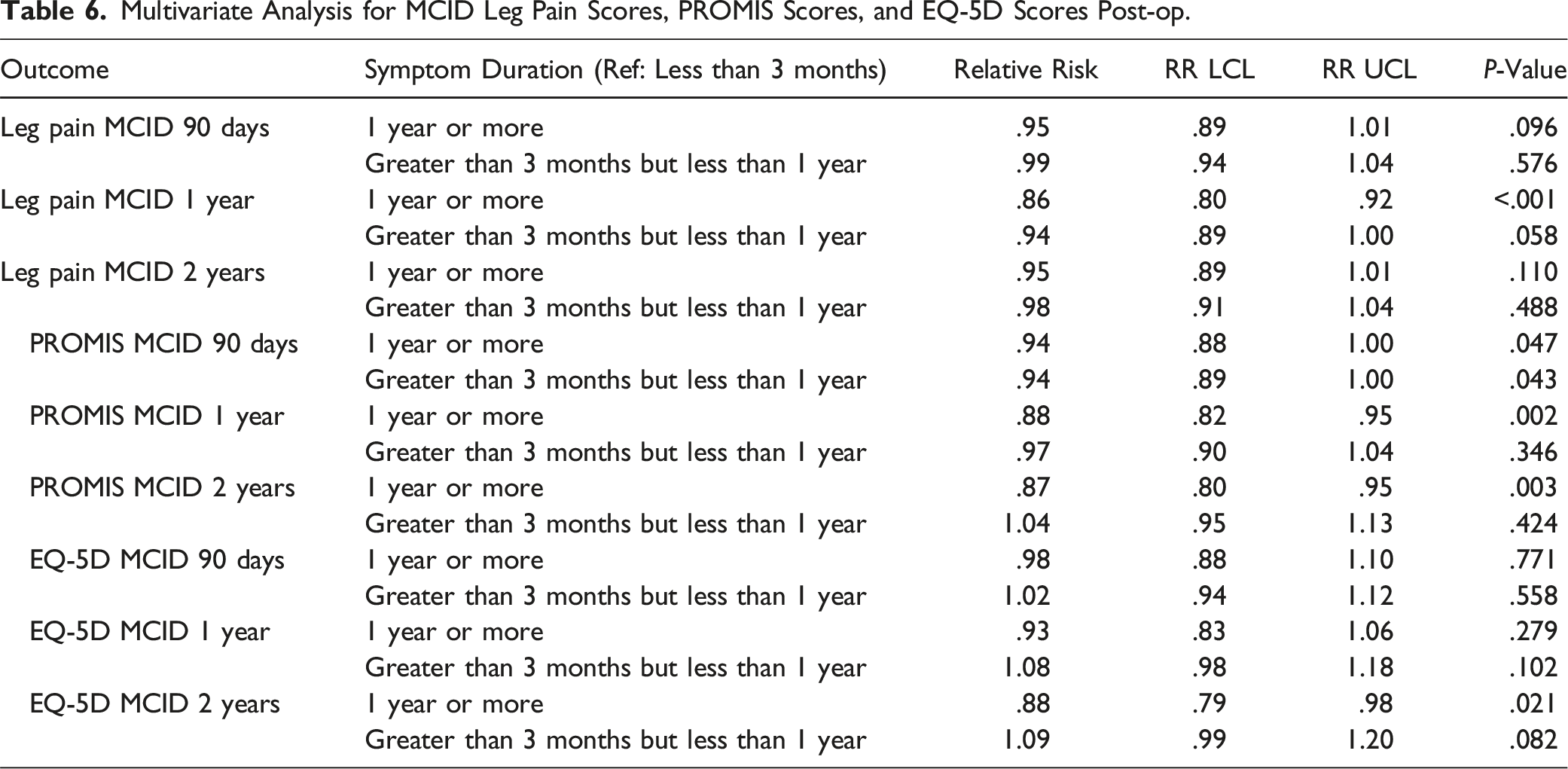
However, other comparisons did not show statistically significant results. Specifically, there was no significant difference in achieving MCID for leg pain scores at 90 days (RR: .95, 95% CI: [.89, 1.01], P = .096), EQ-5D scores at 90 days (RR: .98, 95% CI: [.88, 1.10], P = .771) and 1 year (RR: .93, 95% CI: [.83, 1.06], P = .279) for Group 3.
For patients who had symptoms for more than 3 months but less than 1 year (Group 2), none of the comparisons reached statistical significance, including PROMIS PF scores at 1 year (RR: .97, 95% CI: [.90, 1.04], P = .346) and 2 years (RR: 1.04, 95% CI: [.95, 1.13], P = .424), EQ-5D scores at 90 days (RR: 1.02, 95% CI: [.94, 1.12], P = .558), 1 year (RR: 1.08, 95% CI: [.98, 1.18], P = .102), and 2 years (RR: 1.09, 95% CI: [.99, 1.20], P = .082).
Discussion
While conservative management is often the first line of treatment for symptomatic lumbar disc herniation, surgery is ultimately required in about 10% of cases. 18 Despite the high success with standard open lumbar discectomy, less than ideal outcomes may occur in patients with prolonged duration of pre-operative symptoms. Prior Spine Patient Outcomes Research Trial (SPORT) and observational studies have associated worse post-operative pain and quality-of-life outcomes with longer duration of pre-operative symptoms. 19 In their SPORT study (n = 1192), Rihn et al 19 reported that patients who had symptoms for more than six months reported lower increases on Short Form-36 and higher scores in the Oswestry Disability Index score when compared to patients who had symptoms for less than six months following both operative and conservative measures. 19 Kerr et al also conducted a SPORT study (n = 1244) which found that patients exhibiting symptoms less than or equal to six months had significantly better outcomes with both surgical and nonoperative treatment cohort. 20 However, the authors note that patients who had symptoms longer than six months benefitted relatively more from surgery than other patient groups. Ng and Sell 18 reported in their prospective cohort study (n = 113) that patients who had sciatica for more than 12 months had an overall less favorable outcome. Peul et al 21 noted in their multi-center prospective study (n = 283) that patients who had early surgery reported faster relief of leg pain and faster rate of perceived recovery compared to those who underwent conservative management and eventual surgery. The purpose of this study was to examine whether the duration of symptoms a patient experiences prior to lumbar microdiscectomy affects their outcomes after surgery.
The principal findings of our study showed that even with similar baseline scores, patients who undergo surgery following a reported symptom duration of longer than 3 months had significantly worse outcomes (increased leg pain and lower PROMIS PF and EQ-5D scores) at 90 days, 1 year, and 2 years post-operative compared to those patients with symptom duration of less than 3 months. Patients who had symptoms for over a year before undergoing surgery (Group 3) were observed to have lower average post-operative PROMIS PF scores at various time points (90 days, 1 year, and 2 years) compared to patients with symptoms that persisted for less than 3 months (Group 1). Furthermore, patients from Group 3 experienced higher average post-operative leg pain scores at these same time intervals relative to Group 1, as evidenced by our multivariate analysis. Univariate analysis revealed that a greater proportion of patients with symptom duration for less than 3 months achieved MCID as well as attained higher return to work rates at 1-year follow-up compared to other groups. Specifically, 88.8% of subjects in group 1 were able to return to work within a year following their surgery, in contrast to the 84.4% in Group 2 and 79.5% in Group 3 (P < .05). This information can help guide physicians when counseling patients on a timeline of treatment or possible treatment options when treating their lumbar disc herniation. While there is no optimal duration of conservative treatment before the consideration of surgery, our findings suggest that early intervention offers the best outcomes after surgery.
MCID is a valuable metric for interpreting the clinical relevance of statistical differences, particularly in patient-reported outcomes. It provides a benchmark for the smallest difference in scores that patients perceive as beneficial, thus bridging the gap between statistical significance and clinical relevance. Despite the observed 2.23 points lower post-operative PROMIS PF score in Group 3 compared to Group 1 at 2 years, our multivariate MCID results give a deeper perspective. For instance, when considering MCID in PROMIS PF scores, we found that Group 3 was significantly less likely to achieve MCID at 90 days (RR = .94, P < .05), 1 year (RR = .88, P < .05), and 2 years (RR = .87, P < .05) compared to Group 1.
Importantly, all groups displayed significant improvements in leg pain and lifestyle metrics compared to baseline, suggesting that patients can be assured that they may have relative improvement post-operation regardless of the duration of their symptoms. Thus, consistent with the findings of Siccoli et al as well as other prior studies, earlier surgical intervention can lead to better postoperative clinical and functional outcomes.2,21–24
Limitations
The present study is not without limitations. Differences in baseline data including the location of lumbar disc herniation and operative time between groups may have altered the results as our study also showed significant differences between patient groups at baseline in relation to factors like education level, diagnoses of depression and anxiety, pre-operative independent ambulation, private insurance status, smoking habits, and return to work plans. One important consideration is that nearly 33% of patients with symptoms greater than 12 months presented with concurrent depression which was significantly higher compared to other patient groups. Physicians may bias against patients with a psychiatric diagnosis and understate the severity of their reported statements. These findings are consistent with epidemiological studies which have revealed that nearly 1 in 5 patients with symptomatic lumbar stenosis report depression.19,22 Additionally, higher preoperative mental health scores have been shown to produce better patient satisfaction and outcome scores, suggesting that depression may skew reported patient data.25,26 Nevertheless, our study suggests that patients with longer duration of symptoms have higher rates of depression and the avoidance of this bias may be unavoidable. The retrospective nature is a limitation in its own, but we believe the large number of patients provides a signal that duration of symptoms may influence outcomes after microdiscectomy.
Conclusion
Microdiscectomy for lumbar disc herniation within 3 months of symptom onset leads to greater improvements in postoperative leg pain, PROMIS PF, and EQ-5D than if surgery is performed after 3 months of symptom onset. Furthermore, patients undergoing surgery within 3 months of symptom onset have the highest rates of return to work at 1 year after surgery. These results suggest that the swift treatment of lumbar disc herniations within 3 months gives patients the best outcomes after surgery. While our study does suggest a potential influence of symptom duration on certain surgical outcomes, this relationship is likely complex and may be influenced by various patient-specific factors. The direct causal relationship between symptom duration and surgical outcomes warrants further exploration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have no relationships related to this study specifically. Although BCBSM and MSSIC work collaboratively, the opinions, beliefs, and viewpoints expressed by the authors do not necessarily reflect the opinions, beliefs, and viewpoints of BCBSM or any of its employees. Support for MSSIC is provided by BCBSM and Blue Care Network as part of the BCBSM Value Partnerships program. Although BCBSM and MSSIC work collaboratively, the opinions, beliefs, and viewpoints expressed by the authors do not necessarily reflect the opinions, beliefs, and viewpoints of BCBSM or any of its employees. Support for MSSIC is provided by BCBSM and Blue Care Network as part of the BCBSM Value Partnerships program.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.