
Abstract
Study Design:
Systematic review.
Objectives:
Osteoporosis predisposes patients undergoing thoracolumbar (TL) fusion to complications and revision surgery. Cement augmentation (CA) improves fixation of pedicle screws to reduce these complications. The goal of this study was to determine the value and cost-effectiveness of CA in TL fusion surgery.
Methods:
A systematic literature review was performed using an electronic database search to identify articles discussing the cost or value of CA. As limited information was available, the review was expanded to determine the mean cost of primary TL fusion, revision TL fusion, and the prevalence of revision TL fusion to determine the decrease of revision surgery necessary to make CA cost-effective.
Results:
Two studies were identified discussing the cost and value of CA. The mean cost of CA for two vertebral levels was $10 508, while primary TL fusion was $87 346 and revision TL fusion was $76 825. Using a mean revision rate of 15.4%, the use of CA for TL fusion would need to decrease revision rates by 13.7% to be cost-effective. Comparison studies showed a decreased revision rate of 11.3% with CA, which approaches this value.
Conclusion:
CA for TL fusion surgery improves biomechanical fixation of pedicle screws and decreases complications and revision surgery in patients with diminished bone quality. The costs of CA are substantial and reported decreases in revision rates approach but do not reach the calculated value to be a cost-effective technique. Future studies will need to focus on the optimal CA technique to decrease complications, revisions, and costs.
Keywords
Introduction
Osteoporosis remains the most prevalent bone disorder in the world and estimates have shown up to 20% of men and 50% of women will have an osteoporosis-related fracture. 1 Although there have been major advances in the diagnosis and treatment of this disease, osteoporosis and bone health care remains suboptimal. 2 As such, osteoporosis and bone quality are important factors for all spine surgeons to consider when planning thoracolumbar (TL) fusion surgery. 3
Previous studies have shown 41% to 59% of patients undergoing spinal surgery have osteopenia and 10% to 51% have osteoporosis. 4,5 Diminished bone mineral density (BMD) has been shown to be a risk factor for a variety of complications in spine surgery, including vertebral body compression fractures (VBCF), proximal junctional kyphosis (PJK), proximal junctional failure (PJF), hardware failure (broken or dissociated arthrodesis components, screw pull-out, or screw loosening), pseudoarthrosis, and catastrophic failure. 5,6 This has led to a variety of treatment options to help reduce these complications, including preoperative optimization with treatment of osteoporosis with bisphosphonates and other anabolic medications and vitamin D deficiency with supplementation. 3,7 Similarly, improved surgical techniques such as the use of nontraditional screw trajectory, undertapping of screws, new hardware designs, the use of anterior column support, and cement augmentation (CA) have been described to reduce complications in these patients. 3,8
A variety of techniques have been described for CA of pedicle screws. These include (1) transpedicular vertebroplasty augmentation, where cement is injected into the vertebral body through the pedicle and screws are inserted after cement injection 9 -11 ; (2) kyphoplasty augmentation, where a cavity is created in the vertebral body using the inflatable bone tamp, cement is then injected down the pedicle path and screws are inserted after cementing 12 ; (3) coating of pedicle screws with cement prior to insertion rather than injection of cement down the pedicle tract 13 ; (4) use of cannulated screws with injection of cement through the cannulation after screw insertion 14 -16 ; and (5) vertebroplasty completed at a second stage after TL fusion. The best technique remains controversial as comparative studies have been conflicting. 12,15,17,18 Therefore, the technique is often based on surgeon preference and availability of resources. Similarly, the levels to augment are often patient specific based on surgeon experience and size of the planned fusion construct.
In addition to its association with postoperative complications, BMD has been shown to correlate with pedicle screw stability. 19 -21 Many authors have determined CA can increase screw pull-out strength (POS) by 80-1031% in osteoporotic spines. 15,17,22 Biomechanical studies have demonstrated improved POS with a kyphoplasty technique, 12 vertebroplasty-augmented solid screws, 17 cement prefilling compared with cannulated screws, 15 solid-core screws with cement prefilling, 18 and partially cannulated fenestrated screws. 23 Additionally, cadaveric biomechanical testing has shown the use of prophylactic vertebroplasty at the upper instrumented vertebra (UIV) and cranial-adjacent vertebra (UIV+1) can help reduce the incidence of junctional fractures after long segment fusion. 24
Along with improved biomechanical fixation, CA has shown promising clinical benefits. These include improvements in walking distance, back pain, ability to perform activities of daily living, and Oswestry Disability Index scores, 9,11 low incidence of osteoporosis-related complications (ORC) requiring revision surgery, 9,11,25 sustained correction, 11 with no significant complications from cement leakage. 25 Clinical studies have also shown benefit when combining CA of pedicle screws with CA of the UIV+1 or the level caudal to instrumentation (LIV-1). These benefits include improvements in patient-reported outcomes, 26 a low incidence of complications from cement, 27 and low early incidence of ORC and revision surgery. 26,27 However, studies with longer follow-up revealed moderate rates of ORC and revision surgery. 28 A recent meta-analysis reviewing screw-related complications in patients with osteoporosis found screw loosening was lower in CA screws (23% vs 2%) while fusion rates were higher (98% vs 88%) but this did not necessarily lead to an decreased risk of vertebral fracture (7% vs 8%) or reoperation (4% vs 5%) compared with nonaugmented screws. 21
A variety of techniques for CA of pedicle screws have been described to improve fixation in patients with poor bone quality with excellent results. Unfortunately, there is limited data examining the cost and value of this treatment method. The purpose of this review was to review the currently available literature on the value of CA, TL fusion, revision TL surgery, and the prevalence of revision surgery to perform a cost analysis of the use of CA in TL fusion surgery.
Methods
An electronic literature search was completed in March of 2020 including the PubMed, Cochrane, MedLine, and Google Scholar databases (Figure 1A). Search keywords included a combination of “cost,” “value,” “augmentation,” “spine,” and “pedicle.” Only literatures with abstract in the English language were included for review. These searches resulted in 138 articles of which the title and abstract were examined to ensure the study was relevant to our clinical question. “Is cement augmentation of pedicle screws a cost-effective technique to prevent revision surgery in patients with diminished bone density undergoing thoracolumbar spine surgery?” Full manuscripts of all relevant articles were then reviewed and only studies that included the cost or a cost analysis were included. Only two studies evaluated the cost of CA in patients undergoing TL fusions. 29,30 One of these studies used CA of the vertebral bodies above the fusion construct rather than CA of pedicle screws, but was included given the low number of studies examining the value and cost of this technique. 30
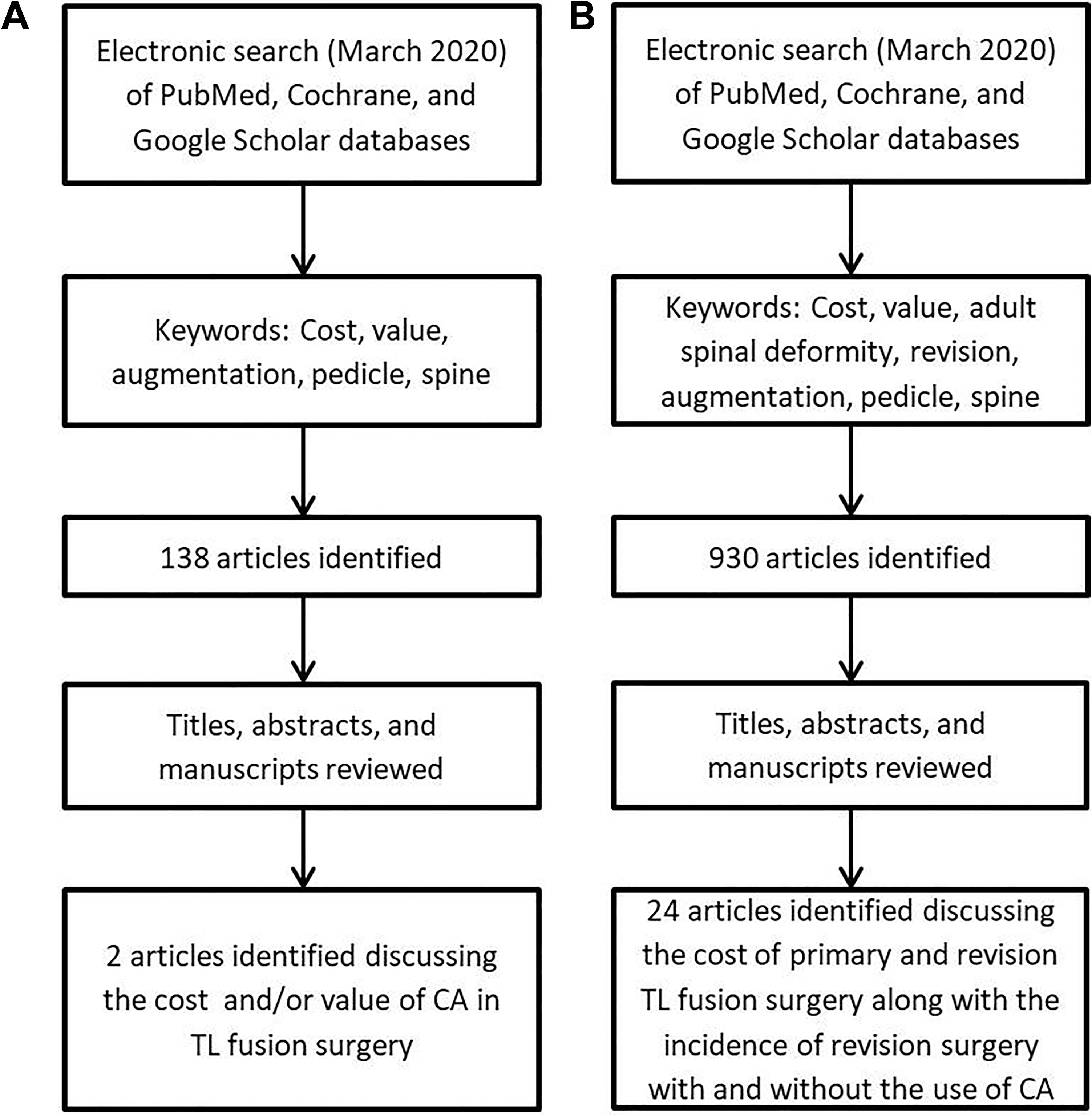
Flowchart of database search and article selection algorithm. Original literature search to evaluate the cost and value of cement augmentation (CA) (A) and the expanded literature search to determine the cost of thoracolumbar (TL) fusion, revision TL fusion, and the incidence of revision surgery for patients undergoing TL fusion with and without CA.
As the primary literature was insufficient to complete a thorough value analysis of CA of pedicle screws, a review of the literature to examine cost of TL surgery, TL revision surgery, and the need for revision after TL surgery with and without CA of pedicle screws was completed. Search keywords included a combination of “cost,” “value,” “adult spinal deformity,” “revision,” “augmentation,” “spine,” and “pedicle” (Figure 1B). The mean cost of TL surgery and TL revision surgery reported in the literature was calculated. Similarly, the mean need for revision after long construct TL fusion was calculated.
We then used the following equation to determine the decrease in revisions necessary to make CA of pedicle screws cost-effective, $TLF + $RTLF(%R) = $TLFCA + $RTLF(x), ($TLF, mean cost for TL fusion; $RTLF, mean cost of revision TL fusion; %R, mean percentage of need for revision; $TLFCA, mean cost of TL fusion with CA; x, variable to solve for to determine the revision percentage in patients undergoing CA to make CA cost-effective). For this analysis we used the cost per vertebral level of CA from our literature review for 2 vertebral levels as many studies have shown good results with CA of only the UIV and level proximal to the fusion construct (UIV+1). 26,28,31,32
Results
The use of CA in spine surgery is becoming increasingly more common with 80% of German surgeons utilizing this technique routinely. 33 Surgeons are aware of the increased costs, but the value of this technique remains unknown. While the true cost for this technique and cost-effectiveness remains unknown, 2 studies have discussed the cost of CA. 29,30
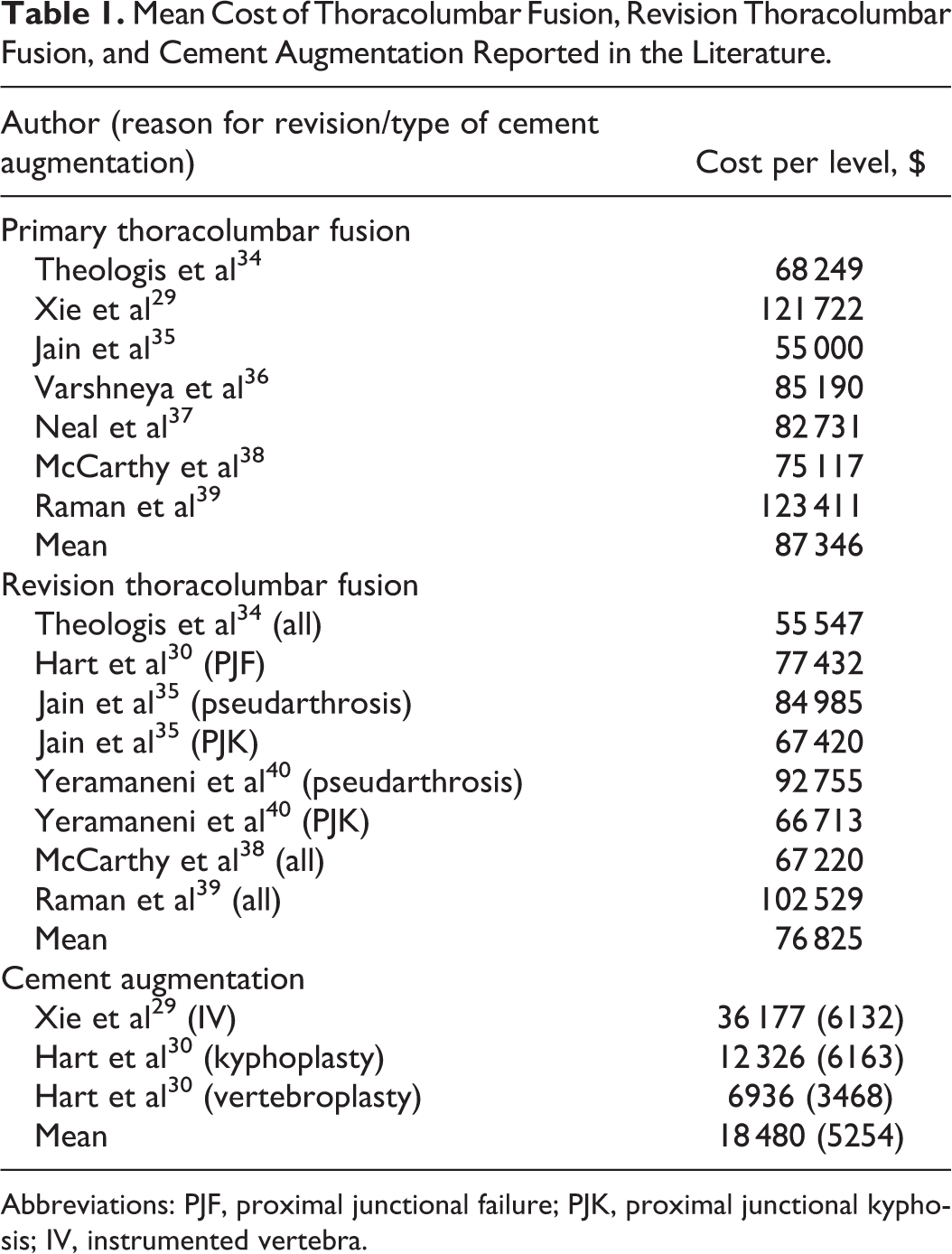
Xie et al 29 examined the cost of CA of pedicle screws with polymethylmethacrylate (PMMA) (14 patients) compared with pedicle screws augmented with autograft bone (17 patients). They found the total treatment cost of CA with PMMA was $157 899 while autograft augmentation cost $121 722 (Table 1), a difference of $36 177. This increased cost was attributed to the CA technique and PMMA as there was no difference in the number of level fused (n = 6), hospital length of stay or surgical time. No patients underwent revision at a mean 3.8 years. There was no difference in preoperative patient characteristics, complications, coronal or sagittal parameters, Oswestry Disability Index, surgical times, or blood loss; however patients with PMMA augmentation did take opioid pain medications for a shorter period of time (6 vs 13 days, P = .001). 29 Due to the low numbers compared and lack of revision surgeries it is difficult to determine the value of CA from this study alone.
Mean Cost of Thoracolumbar Fusion, Revision Thoracolumbar Fusion, and Cement Augmentation Reported in the Literature.
Abbreviations: PJF, proximal junctional failure; PJK, proximal junctional kyphosis; IV, instrumented vertebra.
Hart et al 30 reviewed the cost of prophylactic vertebral augmentation of the 2 or 3 vertebral levels above a long-segment TL fusion construct. They reviewed 28 patients of which 15 underwent vertebroplasty or kyphoplasty cranial to the fused segment. They found the cost for an intraoperative 2-level vertebroplasty was $6936 and kyphoplasty was $12 326 while the cost for revision surgery for proximal junctional collapse was $77 432. They reported a revision rate of 0% in patients receiving prophylactic CA and 15% in those without. Their analysis determined the cost to prevent a single proximal junctional acute collapse was $46 240 using vertebroplasty (must decrease incidence by 9%) and $82 172 using kyphoplasty (must reduce incidence by 16%). 30 This would appear to favor vertebroplasty in this scenario.
Neither of the above articles completely answers the question of what is the cost and value of CA of pedicle screws. Therefore, a combination of the above data and published data regarding the cost of primary TL fusion, revision TL fusion, and revision rates (Table 2) was used to perform a value analysis. The average cost for primary TL fusion found in the literature was $87 346, cost of revision TL fusion was $76 825, and cost for CA of 2 vertebral levels was $10 508. There was a wide range of revision rates reported for long TL fusions (9%-21%), with an average rate of 15.4%. 13,30 -32,34,41 -45 Value analysis determined, the use of CA for TL fusion would need to decrease revision rates by 13.7% bringing the total revision rate to 1.7% in order to be cost-effective.
Complications and Need for Revision in Patients Undergoing Cement Augmentation for Thoracolumbar Fusion Surgery.a
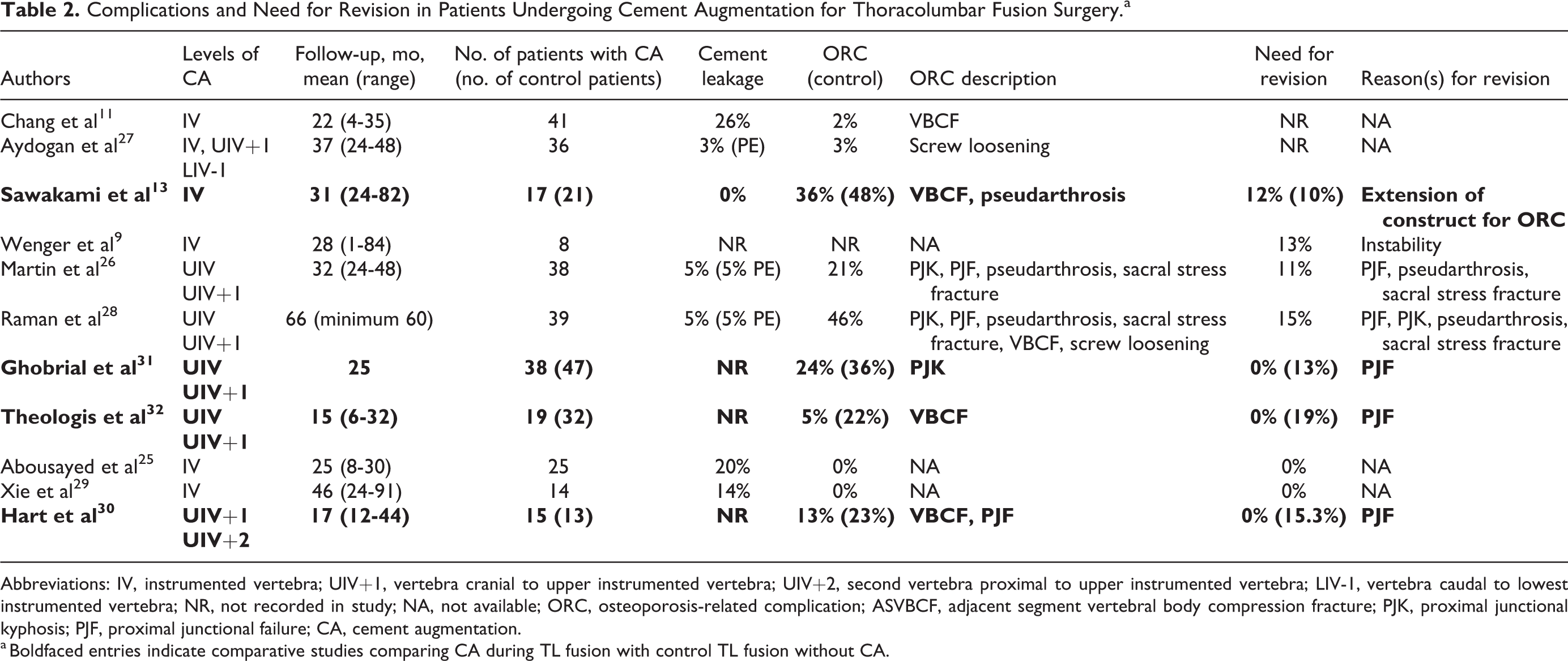
Abbreviations: IV, instrumented vertebra; UIV+1, vertebra cranial to upper instrumented vertebra; UIV+2, second vertebra proximal to upper instrumented vertebra; LIV-1, vertebra caudal to lowest instrumented vertebra; NR, not recorded in study; NA, not available; ORC, osteoporosis-related complication; ASVBCF, adjacent segment vertebral body compression fracture; PJK, proximal junctional kyphosis; PJF, proximal junctional failure; CA, cement augmentation.
a Boldfaced entries indicate comparative studies comparing CA during TL fusion with control TL fusion without CA.
Four studies have directly compared revision surgery for those undergoing CA and those without augmentation (Table 2). As previously discussed, Hart et al 30 found a revision rate of 15% in those not receiving CA and 0% in those undergoing prophylactic CA. Sawakami et al 13 compared patients receiving CA and those without CA undergoing pedicle screw fixation for vertebral pseudarthrosis after an osteoporotic VBCF. They demonstrated a decreased incidence of clear zones around the screws in those receiving CA (29% vs 71%, P < .05) along with decreased loss of correction (3° vs 7°, P < .05) and increased fusion rates (94% vs 76%, P < .05). There were no perioperative complications related to CA or cases of screw pull out. However, the rate of subsequent VBCF at an adjacent level was 30% with 12% requiring extension of the construct in the CA cohort compared to a VBCF rate of 24% and revision rate of 10% in the control group. 13 Ghobrial et al 31 showed vertebroplasty at the UIV and UIV+1 levels decreases PJK (24% vs 36%, P = .02), UIV+1 angle (6.8° vs 10°, P = .02) and PJF requiring revision (0% vs 13%, P = .03). Similarly, Theologis et al 32 demonstrated that CA of the UIV and UIV+1 decreased adjacent fracture rate (5% vs 22%, odds ratio [OR] 3.7, P = .19) and need for revision (0% vs 19%, P = .02, OR 9.2, P = .18). The combined revision rate of these comparative studies was 3% for CA and 14.3% without CA. 13,30 -32 This indicates a decreased revision rate of 11.3%, which approaches the 13.7% calculated to make CA a cost-effective technique.
Discussion
ORCs remain a global concern for spine surgeons when considering TL fusion surgery. A variety of strategies have been used to improve pedicle screw fixation in patients with diminished bone density, including CA. Biomechanical studies have clearly demonstrated improved fixation of pedicle screws with CA. 12,15,17,18,22,24 Similarly, many clinical reviews have shown lower complication rates and/or revision rates using CA. 13,30 -32 These studies demonstrate the importance of this technique to help limit ORC, unfortunately, the value and cost analysis of using this technique remains unknown. The goal of this review was to determine the value of CA in TL fusion surgery.
Many authors have previously evaluated the value of spine surgery. The surgical treatment of spinal stenosis, 46 adult spinal deformity surgery, 47 -49 and the use of rhBMP-2 (recombinant human bone morphogenetic protein–2) 35 have all been found to be cost-effective options. However, only 2 studies have discussed cost of CA in TL fusion surgery. Xie et al 29 found CA cost $36 177 more than autograft augmentation of pedicle screws without changing the prevalence of revision surgery. Meanwhile, prophylactic CA of 2 segments above a fusion construct would need to decrease revision rates by 9% to 16% to be cost-effective. 30 Using our value analysis algorithm, we determined CA (of 2 vertebral segments) would need to decrease revision rates by 13.7% or more to be a cost-effective strategy. Review of comparative studies in the literature showed the use of CA decreases revision rates by 11.3%, which approaches but does not reach our calculated value needed to be cost-effective.
This value analysis has multiple limitations. There was limited primary data evaluating the cost-effectiveness of CA. Therefore, we expanded the review and used a cost-effectiveness formula to determine if CA was cost-effective based on available literature. This type of analysis is therefore restricted by the limitations of the studies included. While reviewing the cost of TL fusion and revision surgery there was a wide range of values. This is likely due to different payers being included in the cost analysis and differences in cost between hospitals and regions. 50 Similarly, the revision rates reported varied significantly. This may be due to differences in the size of fusion constructs and baseline characteristics of the patient populations. Using the mean of multiple cost values and revision values helps limit these biases. Additionally, the technique used for CA will significantly affect final costs as the different instruments and hardware used vary significantly in cost. As there is no literature comparing the costs of the different techniques, this could not be taken into account in our value analysis. Finally, this cost analysis did not consider improvements in patient quality of life or compare TL fusion with CA to nonoperative management, which may increase the tolerable revision rate to make CA cost-effective. Future studies should focus on determining the value of CA using both revision data along with quality-adjusted life years (QALYs) based on patient-reported outcomes.
There are many questions which need to be addressed to fully determine the value of CA of pedicle screws. The technique resulting in the best biomechanics and clinical outcomes remains controversial. 12,15,17,18 CA after PJK has also been shown to be beneficial and has the potential to be more cost-effective than prophylactic CA. 51 Similarly, augmentation with calcium phosphate 52 -55 and calcium sulfate 56 have been used as alternatives to PMMA cement. Many have also discussed the risk of epidural leakage of cement and subsequent neurologic deficits 11,17,25,26,28,29 and pulmonary embolism 27,57 as complications of CA. All these factors change the cost and ultimately value of CA. For this reason, we recommend the surgeon to take cost into consideration along with the likely clinical benefits when deciding on which CA technique to use and levels to augment. Additionally, all surgeons should recommend starting osteoporosis treatment prior to an instrumented fusion in hopes to decrease ORC and revision operations in these patients whether CA is used or not. 7
CA of pedicle screws for TL fusion surgery may be an effective strategy to decrease ORC and revision surgery. Cost analysis showed a decrease in revision surgery of 13.7% is required to make prophylactic CA a cost-effective strategy. This is close to the mean decrease in revision surgeries reported in comparative studies in the literature. Future studies should focus on the optimal CA technique to reduce cost and revision surgeries and use QALY data to help determine the true value of CA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by a grant from AO Spine North America.