
Abstract
Study Design:
Systematic review.
Objectives:
To assess the efficacy of kyphoplasty in controlling pain and improving quality of life in oncologic patients with metastatic spinal disease and pathologic compression fractures of the spine.
Methods:
A literature search through medical database was conducted (using PubMed, EMBASE, Cochrane, and LILACS) for randomized controlled trials comparing balloon kyphoplasty versus the traditional treatment for compression fractures of the spine due to metastatic disease. Two investigators independently assessed all titles and abstracts to select potential articles to be included. Inclusion criteria consisted of randomized controlled trials involving patients with pathologic compression fractures due to spinal metastasis or multiple myeloma treated with balloon kyphoplasty procedure as one of the study interventions, while the control group was any other treatment modality. The risk of bias in individual studies was assessed.
Results:
Two studies, with a combined total of 181 patients, met inclusion criteria. Because of data heterogeneity, the meta-analysis was not possible, and individual analysis of studies was performed. There is moderate evidence that patients treated with balloon kyphoplasty displayed better scores for pain (Numeric Rating Scale), disability (Roland-Morris Disability Questionnaire), quality of life (Short Form–36 Health Survey), and functional status (Karnofsky Performance Status) compared with those undergoing the conventional treatment. Patients treated with kyphoplasty also have better recovery of vertebral height.
Conclusions:
This study concluded that balloon kyphoplasty could be considered as an early treatment option for patients with symptomatic neoplastic spinal disease, although further randomized clinical trials should be performed for improvement of the quality of evidence.
Keywords
Introduction
Spinal fractures caused by bone insufficiency as a consequence of metastatic disease or multiple myeloma are a common cause of morbidity in oncologic patients. 1 This condition may lead to intractable axial pain and neural compression, often accompanied by deteriorating neurologic function. 2,3 With nearly 1.6 million new cases diagnosed in the United States every year, and an estimated 5 million Americans living with cancer, the incidence of symptomatic metastatic spinal tumors is estimated to be around 160 000 new patients per year. 4 Of importance, between 6% and 24% of these patients will have a vertebral compression fracture 5 at some point over the course of their disease.
As cancer treatment improves and life expectancy for patients with metastatic conditions increases, new modalities of palliative treatment for vertebral compression fractures have been developed. 6,7 Among them, minimally invasive approaches such as balloon kyphoplasty are often indicated for patients with pain and debility. 8,9 Despite the popularity of balloon kyphoplasty, its efficacy in treating vertebral compression fractures in patients with spinal metastasis is yet to be accepted due to increased risk of cement and tumor extrusion. 10,11 Overall, the studies available in the literature are not only scarce but also underpowered, of heterogeneous quality, resulting in contradictory results. 8,12
Previous studies evaluating balloon kyphoplasty as a treatment for metastatic vertebral compression fractures demonstrated improved outcomes regarding pain and disability scores. However, these were observational studies and not clinical trials. 6,8 It seems that only one randomized controlled trial (RCT) compared balloon kyphoplasty with standard, nonsurgical management such as analgesic use, bed rest, radiation therapy, and orthoses, 9 reporting improved function and adequate pain control. Previous attempts to conduct systematic reviews resulted in no inclusion of studies, due to the lack of quality of data. 13,14
Given this current gap in the literature, we performed a systematic review of randomized controlled trials assessing the efficacy of balloon kyphoplasty to decrease pain and disability in the treatment of metastatic, pathologic vertebral compression fractures.
Materials and Methods
This systematic review is registered with PROSPERO under the protocol number CRD42015020266. 15
Institutional review board approval (number 154-14) was obtained before the starting of this research.
Search Strategy
A literature search for studies involving balloon kyphoplasty in the treatment of metastatic, pathologic spine fractures was conducted up to May 2015 through the following medical databases: Medline (PubMed); EMBASE (Ovid); Cochrane database of systematic reviews (CDSR); the Database of Abstracts of Reviews of Effectiveness (DARE); and Latin American and Caribbean Health Science Literature (LILACS). No restriction to language or date was applied. To minimize risk of missing relevant reviews, a hand-search of the reference lists of studies captured by the initial search was performed as well. The search strategy used for Medline is shown in the appendix. Other databases followed the same search strategy with minor adjustments. Two investigators (NA and OA) independently assessed all titles and abstracts to exclude duplicate articles and select potential articles to include while inconsistencies were resolved through discussion. When more than one study with the same or similar interventions from the same author were found, only the most current one was included and was considered an update of previous work.
Study Eligibility and Selection Criteria
After a list of studies was gathered from all database searches, only RCTs were included. Inclusion criteria consisted of trials involving patients with a vertebral fracture secondary to spinal metastasis or multiple myeloma submitted to the balloon kyphoplasty procedure as one of the interventions. Control group would be any non-surgical or surgical treatment. Studies looking at vertebral fractures due to osteoporosis or other etiology were excluded. No requirement for clinical follow-up was set due to potential short-term survival of this population. Study quality was assessed through the CONSORT statement for randomized trials. 16
Data Extraction
Data was extracted independently by 2 reviewers (NA and OA) who are board certified in spine surgery. Any disagreement that might have arisen was discussed and resolved by consensus. The following items were included in our form and collected for every RCT: study design, number of patients assigned and assessed at the end of the study, age of participants, funding sources, diagnoses enrolled, and study intervention. Primary outcomes assessed were pain relief, improvement in disability and quality-of-life scores. Secondary outcomes were vertebral height restoration, effect on neurologic deficits, thromboembolic events, performance status, cost, and complications.
Statistical Analysis and Synthesis of Results
Statistical analysis consisted of descriptive statistics including mean, range, and standard deviation. In a random-effects model (due to the heterogeneity of the disease studied), odds ratio, 95% confidence interval, and probability values were calculated for dichotomous variables, and mean difference, 95% confidence interval, and probability values were calculated for continuous variables when outcomes in all included trials were considered uniform. Such estimates were calculated considering intention-to-treat (ITT) analysis. The Q- and I2-statistics were used to test for statistical heterogeneity. An I2 value less than 40% was considered homogeneous. An additional analysis of outcomes and subgroups was performed if applicable to determine if there were different results for different diseases. When possible, meta-analysis was performed on the extracted data with RevMan 5.3 software (Cochrane IMS).
Risk of Bias
Risk of bias in individual studies was assessed for selection bias (patient selection criteria, allocation and randomization), detection bias (blinding), and transfer bias (lost-to-follow-up of patients). Furthermore, the quality of evidence was evaluated using a rating system with 4 levels recommended by the Grading of Recommendations Assessment, Development and Evaluation Working Group (GRADE). 17,18
Results
After a full electronic search, a total of 1053 references were identified (Figure 1), composed of 514 studies in Medline, 525 in EMBASE, 10 in Cochrane/DARE, 6 in Cochrane/CENTRAL, and 8 in LILACS. Duplicates were excluded, 957 titles were excluded after title analysis and 60 abstracts were included in the eligibility analysis. After the full-text of remaining 17 studies were assessed, 2 studies 9,19 were included for data analysis and 15 were excluded (Figure 1). 20 -34
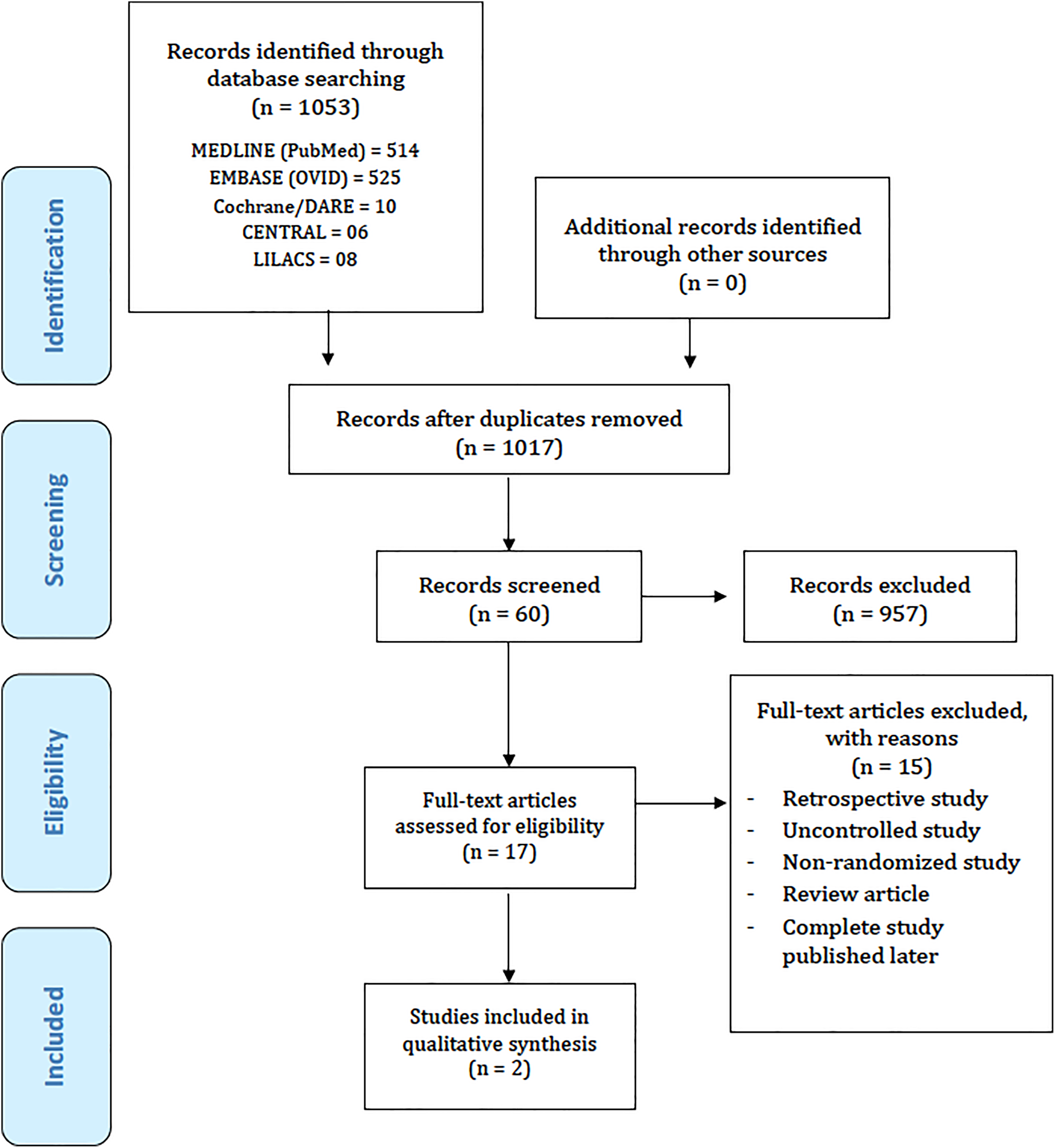
Flowchart of the literature for eligible articles.
Description of the Studies Included
The characteristics of the 2 included studies are summarized in Table 1. All participants had a history of painful neoplastic vertebra due to metastasis or multiple myeloma and all of them were randomized into groups. Both articles reported on RCTs.
Characteristics of the Included Studies.

Abbreviations: RCT, randomized controlled trial; NRS, Numeric Rating Scale; RDQ, Roland-Morris Disability Score; SF-36, Short Form–36 Health Survey; KPS, Karnofsky Performance Status; VAS, visual analogue scale; ODI, Oswestry Disability Index.
Berenson et al 9 randomized 134 patients into either a kyphoplasty surgical treatment group or nonsurgical control group with conventional treatment for metastasis, such as radiotherapy. Primary measured outcomes were disability (Roland-Morris Disability Questionnaire [RDQ]), quality of life (Short Form–36 Health Survey [SF-36]), and pain (Numeric Rating Scale [NRS]). They also assessed Karnofsky Performance Status (KPS) and vertebral height restoration. Follow-up assessment was at 1 month due to the nature of this condition and early-expected outcomes. No crossovers were allowed until the 1-month follow-up was reached. Analysis was made as ITT.
Korovessis et al 19 allocated 47 patients into 2 groups: kyphoplasty treatment (n = 24), and Kiva (Benvenue Medical, Santa Clara, CA) treatment (n = 23). Kiva is an alternative percutaneous transpedicular vertebral augmentation technique based on a coil-guided polyetheretherketone (PEEK) intravertebral implant filled with high temperature polymethylmethacrylate (PMMA). Primary outcomes were pain (analyzed with the visual analogue scale, VAS) and disability (using the Oswestry Disability Score, ODI). Secondary outcome was vertebral height restoration. Follow-up assessment was of 1 month.
Methodological Quality Assessment and Risk of Bias of the Studies Included
The fulfillment of the CONSORT (Consolidated Standards of Reporting Trials) guideline checklist items was 24 items for the study by Korovessis et al 19 and 33 for the study by Berenson et al. 9 Both studies failed to report blinding, while Korovessis et al 19 did not report the randomization method, how sample size was determined, and a protocol registration.
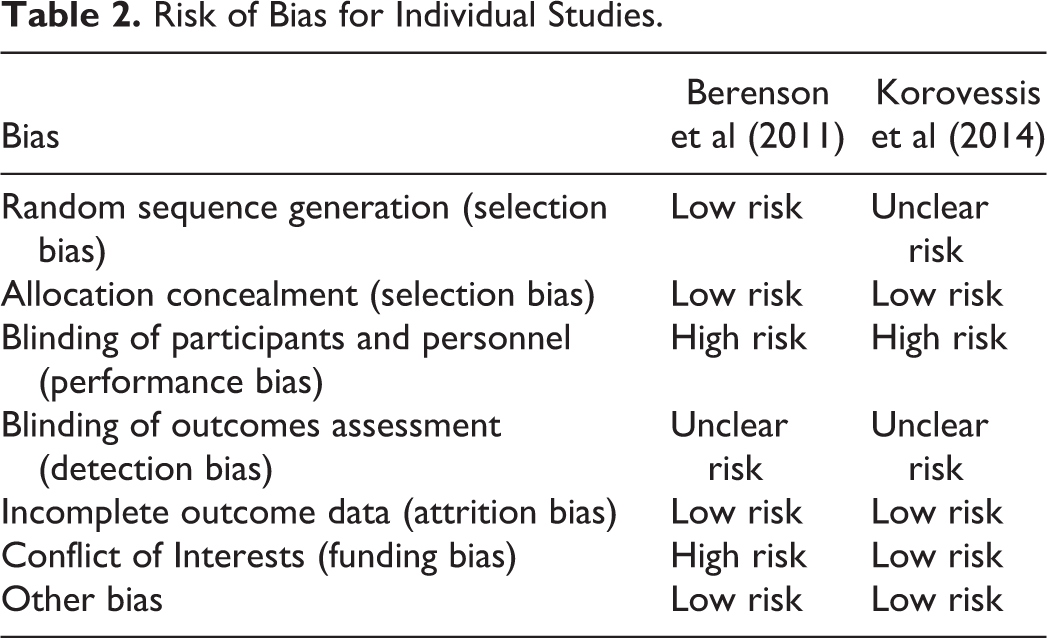
Quality of evidence for each outcome in individual studies was assessed through the GRADE system and moderate quality was defined for both of them. Moderate quality means that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Reasons for classifying as moderate quality in the study by Berensons et al 9 were lack of blinding, early stoppage of trial, and possible funding bias. The study by Korovessis et al 9 had its outcomes evidence rated as moderate due to unknown randomization method and lack of blinding. Risk of bias within studies is summarized in Table 2.
Risk of Bias for Individual Studies.
Results of Individual Studies
There was heterogeneity between both included studies due to the use of different control groups and outcome measures. The control groups consisted of patients with nonsurgical treatment (Berenson et al 9 ) and surgical treatment with a different augmentation technique (Kiva, Korovessis et al 19 ). Therefore, comparison and meta-analysis between study outcomes was not possible; otherwise, results would be inaccurate and meaningless. Thus, individual analysis of studies was performed.
Berenson et al 9 measured disability with the RDQ questionnaire and noted a 1-month kyphoplasty treatment effect of −8.4 points (95% CI −9.2 to −7.6; P < .0001) compared with conventional nonsurgical treatment (Figure 2). Quality of life was assessed with the SF-36 questionnaire and showed an improvement of 8.4 points (95% CI 10.7-11.5; P < .0001) when kyphoplasty was compared with nonsurgical treatment (Figure 3). The difference in the change from baseline to the end of treatment between the control group and the kyphoplasty group for NRS pain was −3.3 points (95% CI −3.6 to −3.0; P < .0001) at 1 month (Figure 4) (negative values meaning improvement of pain). Secondary outcomes consisted of KPS score and vertebral height restoration. The kyphoplasty group had a mean improvement in KPS of 15.3 points (95% CI 13.5-17.1; P < .0001) compared with the nonsurgical treatment group. Vertebral height restoration improved 2.4 mm in the kyphoplasty group compared with 0.7 mm worsening in the control group, a treatment effect of 3.1 mm (95% CI 2.1-4.1; P < .0001) (Figure 5).

Disability—Roland Morris Questionnaire (RDQ). Kyphoplasty versus nonsurgical treatment.

Quality of Life—Short-Form 36 (SF-36). Kyphoplasty versus nonsurgical treatment.

Pain—Numeric Rating Scale (NRS). Kyphoplasty versus nonsurgical treatment.

Vertebral height restoration. Kyphoplasty versus nonsurgical treatment.
Korovessis et al 19 assessed 2 primary outcomes: disability (Oswestry Disability Index [ODI]) and pain (visual analogue scale [VAS]). Both groups had significant improvement at 1-month ODI scores of 42 and 43 points to kyphoplasty and Kiva, respectively (Figure 6). Pain scores went from baseline 8.1 and 8.3 to 1-month 3.0 and 3.2 points for kyphoplasty and Kiva, respectively. No significant difference was observed between groups (Figure 7). Vertebral height restoration at 1-month postprocedure had a mean improvement of 7.2% with kyphoplasty and 5.1% with Kiva. No statistical difference was observed.

Disability—Oswestry Disability Index (ODI). Kyphoplasty versus Kiva.

Pain—Visual Analogue Scale (VAS). Kyphoplasty versus Kiva.
Complications increased from 5.7% to 16% for the kyphoplasty procedure. Berenson et al 9 reported 1 adjacent fracture 1 day after the index procedure, 1 superficial wound infection, 1 asymptomatic balloon rupture, and 1 asymptomatic extravasation into the vertebral disc. Korovessis et al 19 reported 4 asymptomatic cement leakages.
Discussion
As advances in cancer treatment prolong the life expectancy for patients with metastatic disease, the rate of pathologic spinal compression fracture will likely increase. With no hope of cure in many of these cases, palliative care becomes of paramount importance. Cancer patients with no hope of cure require extensive palliative treatment. Back and extremity pain in these patients is related to extensive neoplastic spread into the vertebral bodies, collapse, and, at times, neural compression. Kyphoplasty became a well-accepted percutaneous treatment for this population due to its approved use for the very similar pathologic vertebral compression fracture from osteoporosis.
In this systematic review, we searched for available evidence in the literature to support such therapeutic benefits related to kyphoplasty in treating the neoplastic spine. Up to now, as far as we know, 2 systematic reviews on this topic were made, 13,14 but neither presented strict selection of randomized controlled studies. In 2009, Bouza et al 14 included 7 studies in their systematic review, however, none of those were RCTs. Retrospective and observational studies were included since no RCTs were available at that point. Still, meta-analysis of included papers resulted in evidence level III of recommendation of kyphoplasty as a method to control pain and improve function in patients with painful vertebral fracture due to metastasis. Two years later, in 2011, Schroeder at al 13 performed another systematic review including 2 retrospective studies 6,35 comparing kyphoplasty with vertebroplasty in patients with spinal tumor. In their study, although recommending kyphoplasty and vertebroplasty to treat patients with back pain and vertebral metastasis without neural compression or vertebral instability, authors declared that there is weak evidence on this benefit. Mendel et al 36 also performed a systematic review, but they included percutaneous vertebral embolization of spinal tumors as a comparative intervention as well. Following the same limitations as previous reviews, no quality RCT was found or included and no evidence-based conclusion was reported.
Although it is easy to criticize lack of evidence and weak level of recommendation, clinical trials and systematic reviews of surgical interventions are difficult to perform when gold-standard methodological patterns are followed. While it is almost impossible to blind participant surgeons and patients, obstacles frequently include heterogeneity of patients and diseases, surgeon technique, and implants used. Furthermore, clinical trials of surgical intervention are extremely costly and time consuming. Some of the most well-designed and well-executed randomized trials are industry funded, which became of paramount importance to sponsor and turn possible wide proportion studies with evidence-based and quality conclusions. Recently, an overview of systematic reviews 37 of the surgical treatment of low back pain assessed quality of all reviews according to established and validated scoring tools and concluded that most reviews do not achieve acceptable methodological quality and reported that conclusions are frequently scientifically unsupported. To perform a systematic review is not an easy task since rigid criteria are applied in the review protocol. Insufficient data to perform a meta-analysis are often the complicating matter. To conclude their study and generate results, authors usually include observational or nonrandomized studies, even retrospective ones, which results in the decrease of quality of evidence.
This review also found insufficient data for a meta-analysis, although 2 good-quality trials were included. This happened for 2 reasons: We strictly followed Cochrane established methodology 38 and kept analysis of quality, 16 -18 which limited our number of included studies, and, our 2 included studies had considerable heterogeneity of control groups and outcome measures. The lack of sufficient clinical trials available in the literature for this group of patients and intervention is explained due to the newness of kyphoplasty, with the first report of the technique being published in less than 20 years ago. 39 In this period, the technique was widely used to treat vertebral compression fractures in patients with osteoporosis. For this population, enough RCTs and systematic reviews have been published to evidence the benefits of kyphoplasty. 40,41 The first series of cases of patients with spinal metastasis treated with kyphoplasty are reported within the past 14 years, 6,42 and the first well-designed RCT was published 7 years ago by Berenson et al 9 in 2011.
According to the GRADE 17,18 and CONSORT 16 statements, moderate grade of evidence was found for the outcomes presented. Lack of blinding was the main bias of trials, which is almost inherent to trials of surgical interventions. In the analysis of kyphoplasty effect on disability and pain, Berenson et al 9 reported superior results for all outcome measures for this intervention over conventional, nonsurgical treatment. This beneficial effect had already been reported in previous large-scale prospective and retrospective studies. 32,43 In 2012, Pflugmacher 32 prospectively evaluated 768 patients with metastasis or multiple myeloma in the spine that underwent kyphoplasty collecting results on 409 patients at the end of the study. There was significant improvement in pain and disability scores. They also presented evidence of fracture stabilization and no further loss of vertebral height was observed 36 months postprocedure. Although the main objective of kyphoplasty for cancer patients is to treat pain, maintaining vertebral height is also an important benefit that might avoid vertebral body collapse and neural impingement, which would be catastrophic in this population that already carries severe comorbidities. Analysis of both included studies revealed an increase or maintenance of vertebral height after kyphoplasty. The structural effect of cement, as well as the stability it imparts may be related to pain and functional improvement.
Complications were reported by the included studies. Most frequent and yet feared was cement extravasation through the vertebral body. Although those were asymptomatic leakages, it was reported as 2.8% to 9.3% for kyphoplasty cases. Other studies reported extravasation rates for neoplastic vertebras from 0% 13 to 6%. 14 No adjacent fractures were reported in this review although follow-up period is considerably short to detect this type of complication. Bouza et al 14 reported a chance of approximately 10% that patients with neoplastic spine will present with a new vertebral collapse 2 years after treatment. This complication seems to be more frequent in multiple myeloma patients.
Patients with cancer and painful spine metastases will benefit from interventions that will decrease the need for pain medication and bed rest. Improvement of physical function means a hopeful decrease in comorbidities related to long periods of immobility such as thromboembolic events, pneumonia, and pressure sores. Thus, a procedure resulting in pain control would be expected to increase life expectancy. Furthermore, it is a minimally aggressive technique, with the possibility of hospital discharge in less than 24 hours that will not delay eventual chemo- or radiotherapy.
Limitations of this study are primarily related to the fact that there are no homogeneous RCTs to make a complete meta-analysis of results. We chose to follow quality patterns of a systematic review instead of including observational or uncontrolled prospective studies as an alternative to add data. We hope that this article encourages further work with kyphoplasty in oncologic patients; thus, meta-analysis could be performed bringing better strength of evidence.
Conclusions
There is moderate evidence that kyphoplasty improves pain, function, and quality of life in cancer patients with pain and disability from pathologic compression fracture of the spine. For this reason, kyphoplasty could be recommended as an early treatment for this population. There are still insufficient RCTs and future studies are needed for better evidence of treatment effects.
Footnotes
Appendix
Medline Search Strategy.
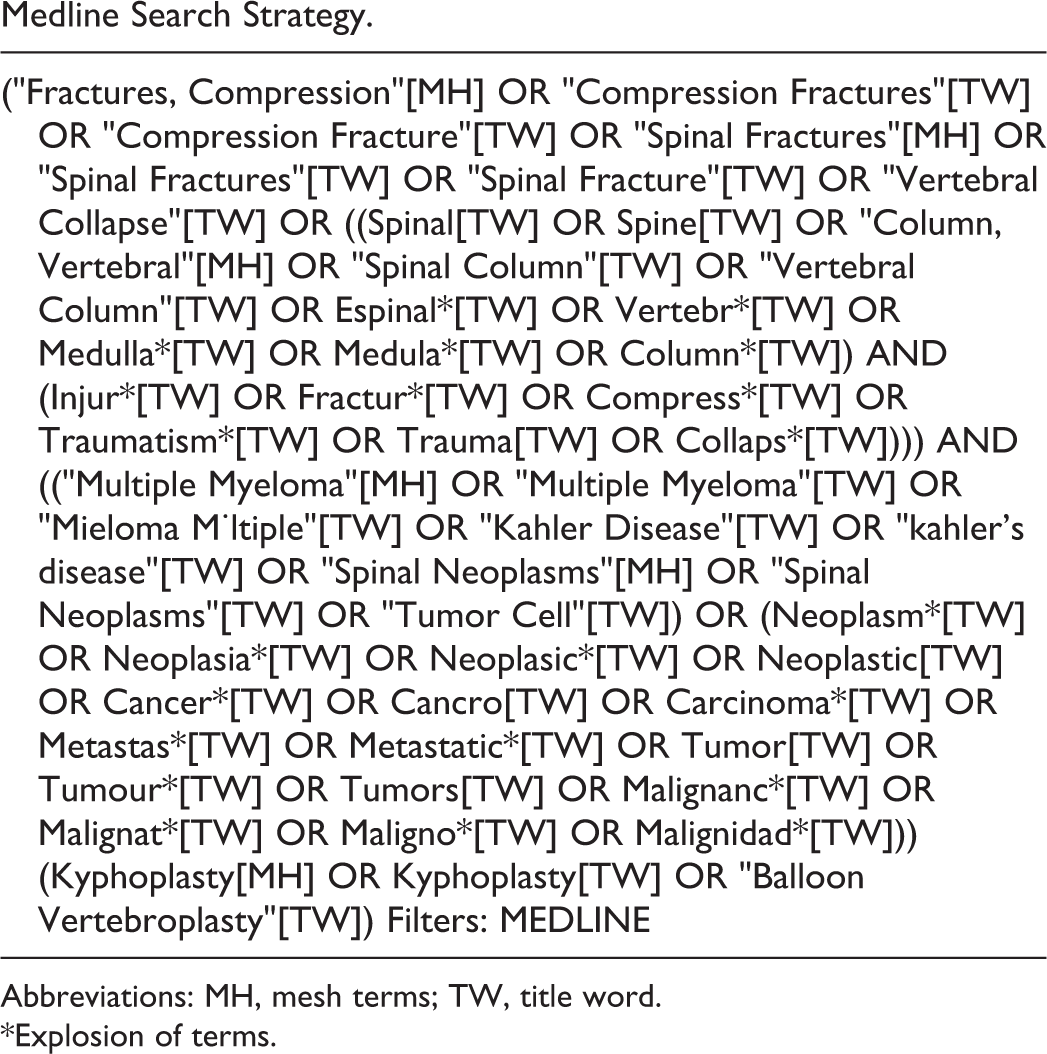
| ("Fractures, Compression"[MH] OR "Compression Fractures"[TW] OR "Compression Fracture"[TW] OR "Spinal Fractures"[MH] OR "Spinal Fractures"[TW] OR "Spinal Fracture"[TW] OR "Vertebral Collapse"[TW] OR ((Spinal[TW] OR Spine[TW] OR "Column, Vertebral"[MH] OR "Spinal Column"[TW] OR "Vertebral Column"[TW] OR Espinal*[TW] OR Vertebr*[TW] OR Medulla*[TW] OR Medula*[TW] OR Column*[TW]) AND (Injur*[TW] OR Fractur*[TW] OR Compress*[TW] OR Traumatism*[TW] OR Trauma[TW] OR Collaps*[TW]))) AND (("Multiple Myeloma"[MH] OR "Multiple Myeloma"[TW] OR "Mieloma M·ltiple"[TW] OR "Kahler Disease"[TW] OR "kahler’s disease"[TW] OR "Spinal Neoplasms"[MH] OR "Spinal Neoplasms"[TW] OR "Tumor Cell"[TW]) OR (Neoplasm*[TW] OR Neoplasia*[TW] OR Neoplasic*[TW] OR Neoplastic[TW] OR Cancer*[TW] OR Cancro[TW] OR Carcinoma*[TW] OR Metastas*[TW] OR Metastatic*[TW] OR Tumor[TW] OR Tumour*[TW] OR Tumors[TW] OR Malignanc*[TW] OR Malignat*[TW] OR Maligno*[TW] OR Malignidad*[TW])) (Kyphoplasty[MH] OR Kyphoplasty[TW] OR "Balloon Vertebroplasty"[TW]) Filters: MEDLINE |
Abbreviations: MH, mesh terms; TW, title word.
*Explosion of terms.
Acknowledgments
The authors would like to thank Aaron T. Creek, MD, for his support in reviewing the English in the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) (BR).