
Abstract
Study Design:
Retrospective cohort study.
Objective:
The purpose of this study was to compare outcomes between different treatment modalities for metastatic disease with indeterminate instability (Spinal Instability Neoplastic Score [SINS] 7-12).
Methods:
We retrospectively reviewed neurologically intact patients treated for spinal metastatic disease with a SINS of 7 to 12. The cohort was stratified by treatment approach: external beam radiation therapy alone (EBRT), surgery + EBRT (S+E), and cement augmentation + EBRT (K+E). Kaplan-Meier analysis was used to assess differences in length of survival (LOS) and ability to ambulate at time of death. Multivariate analysis was performed to assess adjusted LOS and ability to ambulate at time of death.
Results:
The cohort included 211 patients, S+E (n = 57), EBRT (n = 128), and K+E (n = 27). In the S+E group, the median LOS was 430 days, which was statistically longer than the median LOS for the EBRT group (121 days) and the K+E group (169 days). In the S+E group, 52 patients (91.2%) and in the K+E group 24 patients (92.3%) retained the ability to ambulate at their time of death compared to 99 patients (77.3%) of the EBRT patients (P = .01). The overall rate of revision treatment at the spinal level initially treated was 17.5%, S+E (15.8%), EBRT (20.3%), and K+E (7.7%).
Conclusions:
The length of survival, ability to maintain ambulatory ability, and revision treatment rates were all improved following surgical management and radiation therapy compared to radiation therapy alone. The authors’ conclusion from these results are that patients with indeterminate spinal instability should be discussed in a multidisciplinary setting for the need of spinal stabilization in addition to radiation therapy.
Keywords
Introduction
Metastatic spinal disease (MSD) occurs in 30% to 70% of cancer patients, and 50% of patients with MSD require local control. 1 The vertebral column is the most common location of osseous metastatic disease, and the third most common site of metastatic disease following lung and liver metastases. 1 The most common tumors to metastasize to the spine include breast, non–small cell lung cancer (NSCLC), renal cell carcinoma (RCC), prostate, melanoma, and hematologic tumors.
The treatment for spinal metastatic disease is palliative; however, with the life expectancy of cancer patients increasing, the treatment of MSD is gaining greater attention for its ability to prolong quality of life. The treatment goals when managing patients with MSD include alleviating pain, maintaining functional status, preserving neurologic function, restoring spinal stability, and providing local tumor control. 2 Treatment algorithms for the management of spinal metastatic disease have been previously described: The NOMS Framework, The Algorithm for Spinal Metastases, and The Metastatic Spine Disease Multidisciplinary Working Group.2-4 These treatment algorithms incorporate a multidisciplinary approach to spinal metastatic care and aim to identify patients that would benefit from surgical intervention. Based on these algorithms, the decision to proceed with surgical management is based on the degree of spinal cord compression, the tumor histology, the mechanical stability of the spine, and the patient’s medical fitness. In these algorithms spinal instability is an indication for surgical stabilization; however, in actual practice it can be difficult to determine if a metastatic lesion has resulted in spinal instability. The Spinal Oncology Study Group (SOSG) has defined tumor-related spinal instability as, “loss of spinal integrity as a result of a neoplastic process that is associated with movement-related pain, symptomatic or progressive deformity, or neural compromise under physiologic loads.” In 2010, the SOSG developed the Spinal Instability Neoplastic Score (SINS) as a classification system to assist in identifying patients with spinal instability.
The SINS is used to classify metastatic spinal lesions as stable, unstable, or “indeterminate stability.” 5 The classification system was designed to provide guidance for medical and radiation oncologists to refer patients for possible surgical stabilization with indeterminate or unstable spinal lesions. In general, stable lesions (SINS 0-6) do not require surgical stabilization, and unstable lesions (SINS >12) require surgical stabilization. Currently, the ideal treatment for patients with indeterminate stability (SINS 7-12) and no evidence of neurologic involvement remains a matter of debate.
Despite the above-mentioned algorithms and classification systems, the complexity of these patients makes the ideal treatment controversial, and the ultimate decision needs to be made by a multidisciplinary team. Various treatment modalities exist with 3 common techniques including surgical stabilization followed by radiation, percutaneous cement augmentation followed by radiation, and conventionally fractionated external beam radiation therapy (EBRT). These 3 treatment modalities have all been shown to reduce pain levels, improve quality of life, reduce disability, and improve functional status in patients with metastatic spinal lesions.6-19 Previous studies investigating treatment options have included patients with heterogeneous spinal lesions with varying degrees of spinal cord compression and spinal column instability making it difficult to generalize study results to all patients. Specifically, no studies have been able to parse out treatment superiority for neurologically intact patients with indeterminate spinal stability.
The purpose of this study was to examine a single tertiary cancer center’s experience in treating neurologically intact patients with indeterminate spinal stability. The purpose of the study was to identify which patient characteristics were guiding our treatment selection, and second to compare overall treatment outcomes between surgical stabilization and EBRT, EBRT alone, and cement augmentation and EBRT for this commonly encountered group of patients. The study outcomes include length of survival (LOS), ability to ambulate at time of death, and revision treatment rates.
Methods
We retrospectively reviewed patients treated for spinal metastatic disease at a single academic institution between January 2009 and December 2016. Three groups of patients were identified based on the primary treatment of the metastatic spinal lesion: (1) surgical stabilization and EBRT (S+E), (2) EBRT alone (EBRT), and (3) cement augmentation and EBRT (K+E).
The patient’s medical record and previous imaging studies were reviewed to calculate the SINS, rTokuhashi score, and epidural spinal cord compression (ESCC) score.5,20,21 The specific variables obtained for each patient included tumor histology, number of spinal lesions, location of spinal lesions, degree of spinal cord compression, extent of nonspinal systemic disease, Karnofsky performance score, ambulatory status prior to intervention, length of survival following intervention, documented ability to ambulate at time of death, and requirement of revision treatment. 21
Exclusion criteria included neurologic deficit at time of treatment, SINS score <7 or >12, nonambulatory patients at time of treatment, intradural metastatic disease, insufficient clinical or radiographic data to accurately classify SINS and rTokuhashi score, and deceased patients without a date of death recorded (Figure 1). In patients with multilevel disease, the level with the most instability (greatest SINS) was investigated. The ability to ambulate was defined as being able to walk with or without an assistive device. Survival and ambulation status were monitored until patient death or last follow-up with a minimum 2-year follow-up for all living patients.
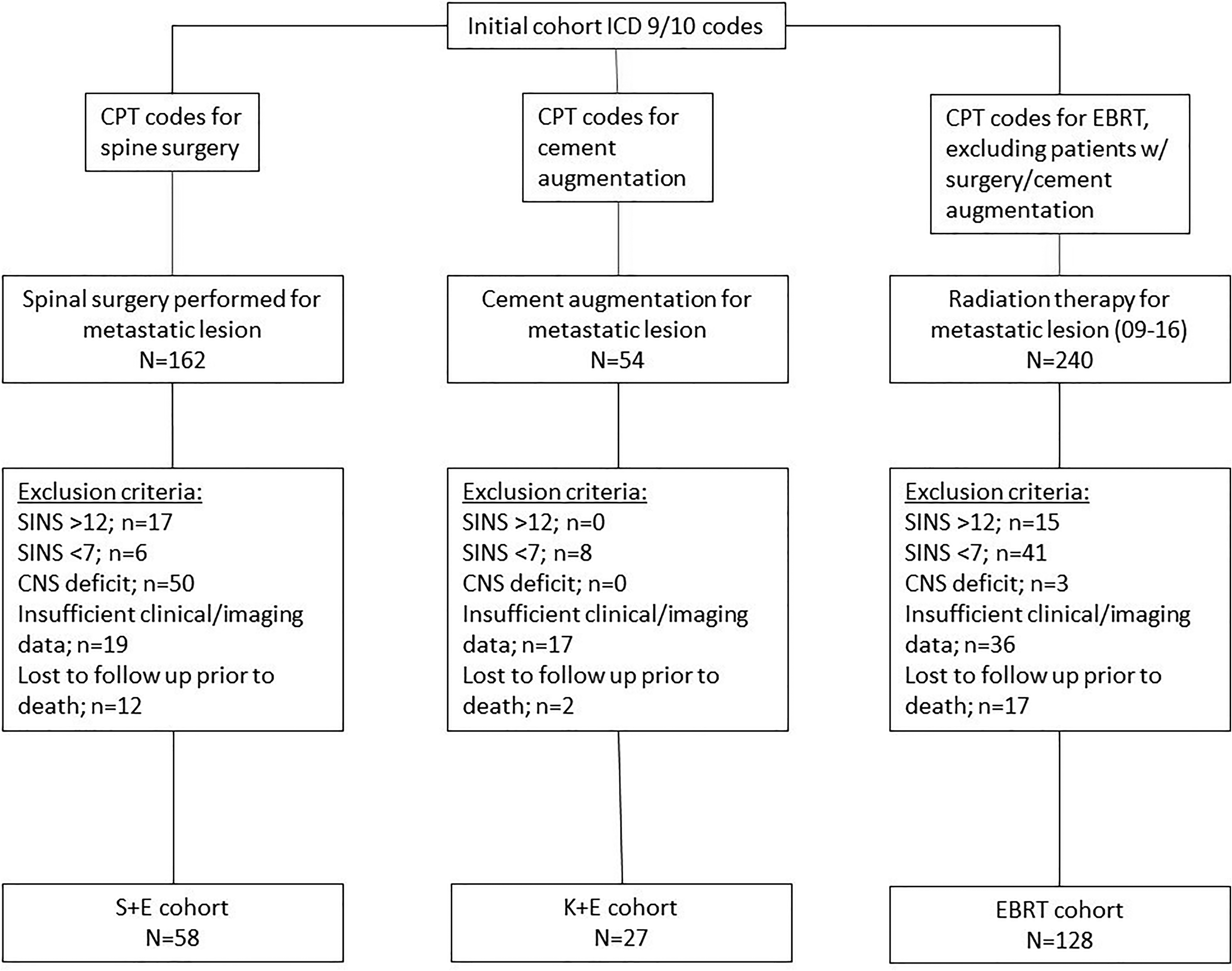
CONSORT diagram demonstrating the inclusion of patients within each cohort.
The SINS was calculated for each patient in the cohort. The SINS was calculated by a senior resident, and calculations were confirmed by the senior author (SML). Patients with a SINS 7 to 12 were included in the study. The rTokuhashi score and ESCC score were then determined for each patient included in the study. In this study, the rTokuhashi score was used as a surrogate for each patient’s overall medical fitness and predicted length of survival. Calculating this score took into account the patient’s Karnofsky performance score or Eastern Cooperative Oncology Group performance score, the primary cancer type, extent of metastatic disease, and presence of spinal cord palsy. 20 The LOS was calculated for each patient as the number of days following treatment until the patient died or until the end of the observation period. Survival analysis was used to compare LOS between treatment arms. The patient’s ability to ambulate at their time of death was then determined from the patient’s medical record. Last, the need for revision treatment at the level of the lesion for persistent pain, new neurologic deficits, progressive disease, or wound complications was recorded.
A subgroup analysis of the data was then performed that only included patients with an rTokuhashi score greater than 8. The purpose of this analysis was to investigate patients with a life expectancy of greater than 6 months. Analyzing this group theoretically helped minimize selection bias by excluding patients that received radiation therapy alone because they were not surgical candidates. In this analysis, only the S+E and EBRT groups were compared due to the limited number of cement augmentation patients with a rTokuhashi score >8. Survival analysis was used to compare LOS between S+E and EBRT, and a multivariate model was used to determine independent predictors for LOS in this subgroup.
Statistical Analysis
Descriptive statistics were utilized to define the entire cohort. Demographics, clinical, and outcomes data was compared between the treatment groups using χ2 tests for categorical variables and analysis of variance (ANOVA) tests for continuous variables. The Kaplan-Meier method with the log rank test was used to compare LOS between the treatment groups. A multivariate statistical analysis was performed utilizing Cox proportional hazard models to assess independent factors for adjusted LOS. All statistical analyses were performed using SAS/JMP (SAS Institute Inc).
Results
The final patient cohort included 211 patients. The inclusion of patients into each treatment arm of the study is demonstrated in Figure 1. The average age in the S+E group was 59 years, which was statistically younger than the EBRT group (64 years) and the K+E group (66 years; P = .004). The median length of follow-up for the cohort was 174 days ranging from 4 to 2793 days. The patient with a length of follow-up of 4 days received palliative radiotherapy, and died 4 days following treatment in hospice. The 3 most commonly encountered tumor diagnoses were NSCLC (28%), breast cancer (19.9%), and prostate cancer (14.7%.). The percentages of radioresistant and radiosensitive tumors were similar in the 3 groups (Table 1). The S+E group had a greater rate of ESCC high-grade lesions compared to the EBRT and K+E groups (77.2% vs 38.3% vs 11.5%, P < .001). The mean SINS in the S+E group, EBRT group, and K+E groups, respectively, were 9.4, 9.1, and 8.5 (P = .02). The mean rTokuhashi score in the S+E group was statistically greater than in the EBRT and K+E groups (10.4 vs 8.6 vs 8.6, P < .001; Table 1). For the subgroup analysis of S+E and EBRT patients with rTokuhashi scores greater than 8, the cohort included 119 patients; 45 S+E patients and 74 EBRT patients.
Demographic and Tumor Characteristics Between Groups.
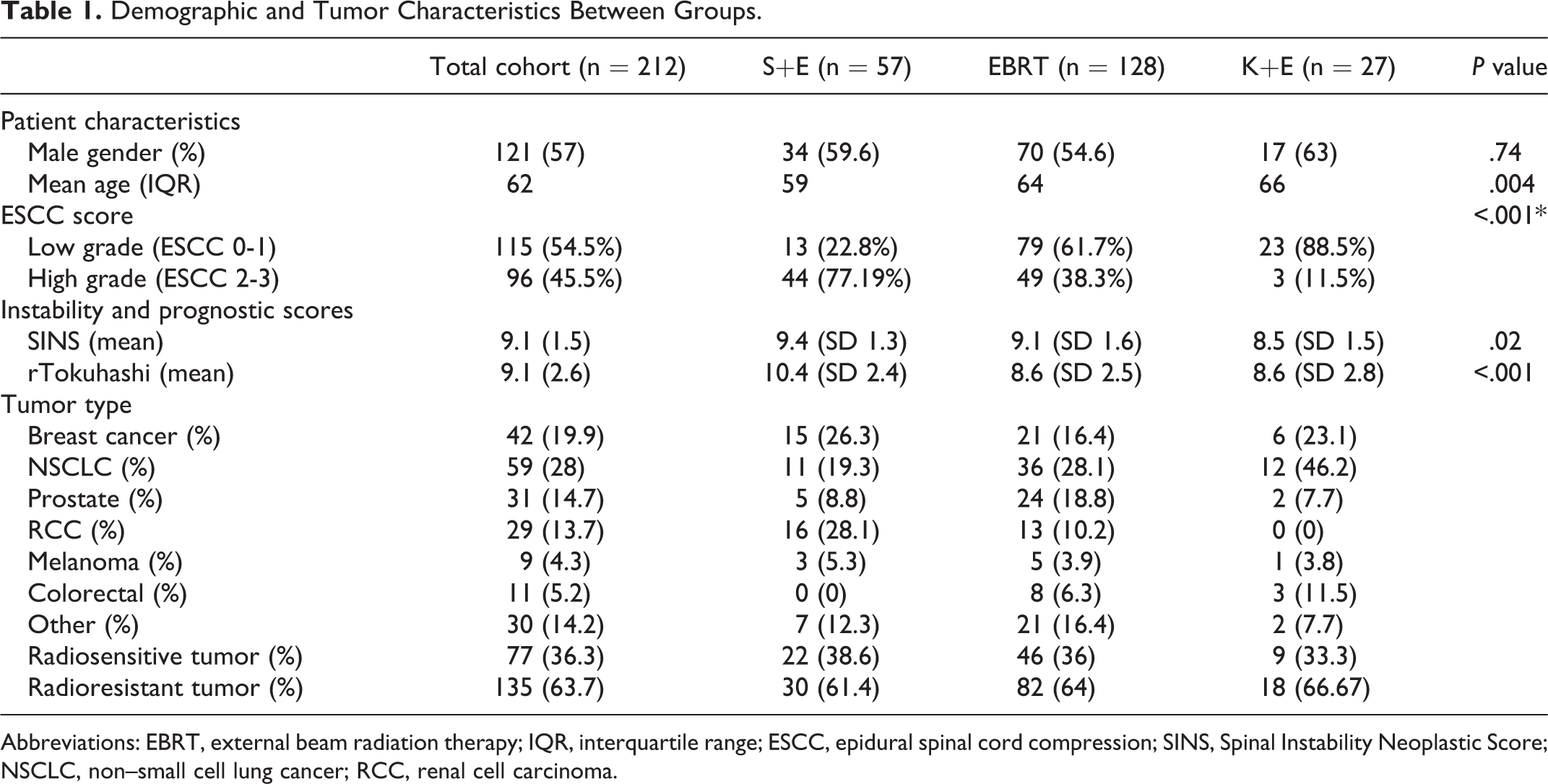
Abbreviations: EBRT, external beam radiation therapy; IQR, interquartile range; ESCC, epidural spinal cord compression; SINS, Spinal Instability Neoplastic Score; NSCLC, non–small cell lung cancer; RCC, renal cell carcinoma.
The median LOS for the entire cohort was 174 days (5.8 months), and the 1-year survivorship was 35.5%. A total of 175 patients (82.9%) retained the ability to ambulate at their time of death. In the S+E group, the median LOS was 430 days (1 year and 2 months), which was statistically longer than the median LOS for the EBRT group (121 days) and the K+E group (169 days; Table 2 and Figure 2). In addition, the 1-year survivorship was statistically greater in the S+E group compared to the EBRT and K+E groups (59.6% vs 25.8% vs 30.8%, P < .001; Table 2). In the S+E group, 52 patients (91.2%) and in the K+E group 24 patients (92.3%) retained the ability to ambulate at their time of death compared to 99 patients (77.3%) of the EBRT patients (P = .01; Table 2). In the multivariate analysis, the patient’s age (hazard ratio [HR] 1.01, 95% confidence interval [CI] 1.0-1.03, P = .04), the rTokuhashi score (HR 3.14, 95% CI 2.05-4.82, P < .001), and surgical treatment (HR 0.51, 95% CI 0.29-0.87, P = .01) were independently predictive for LOS (Table 3).
Length of Survival and Ambulatory Status.
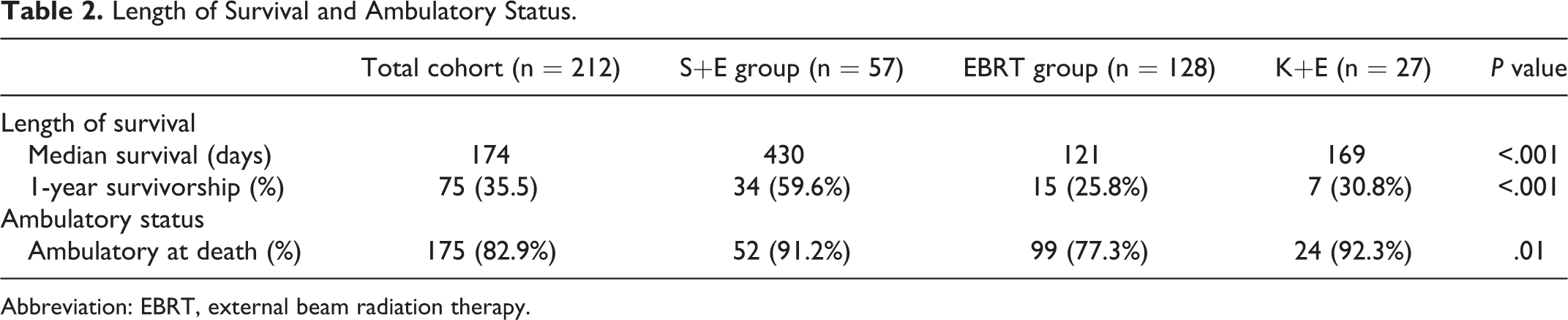
Abbreviation: EBRT, external beam radiation therapy.
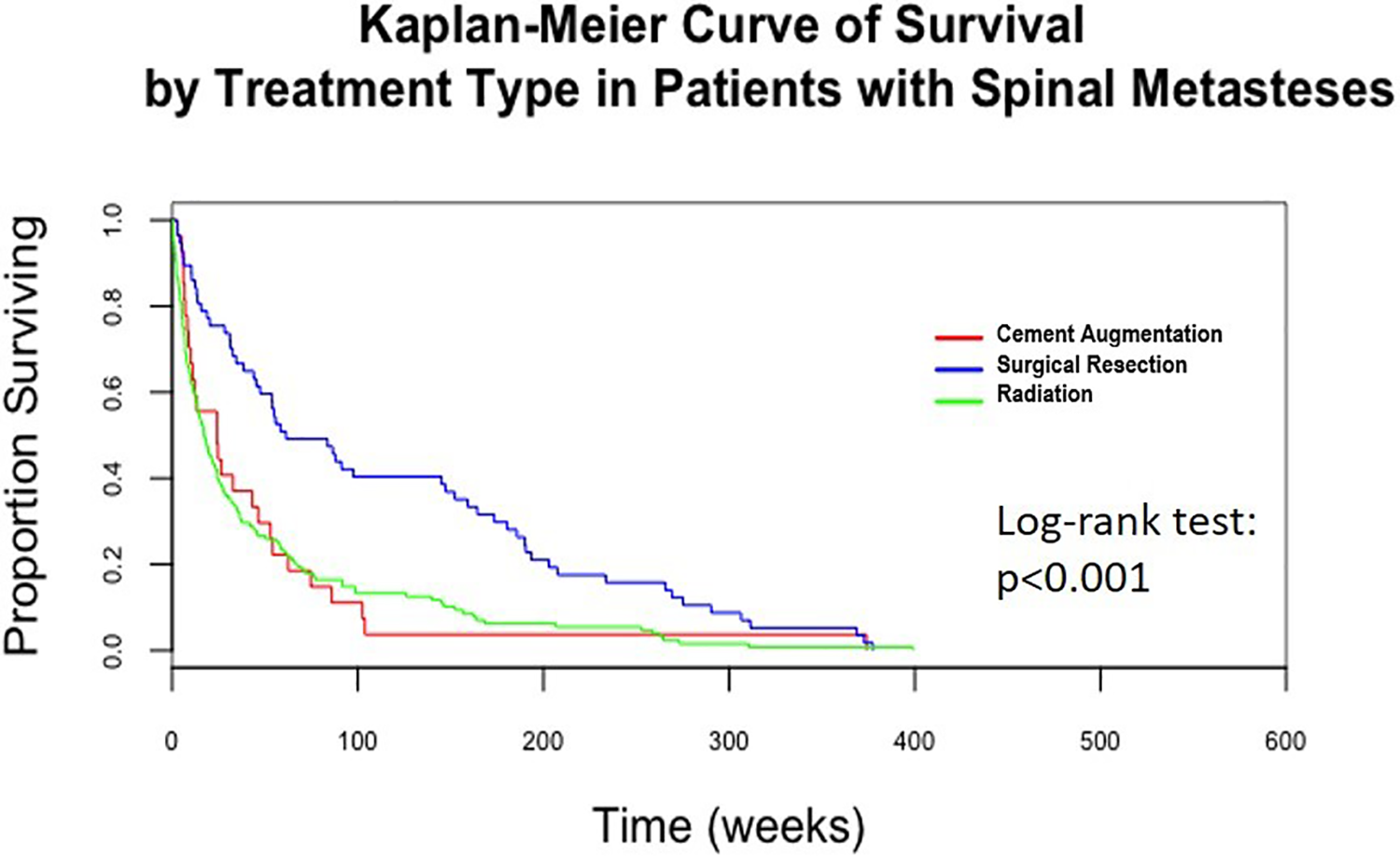
Survival curve for the length of survival following treatment.
Multivariate Hazard Analysis: Length of Survival.
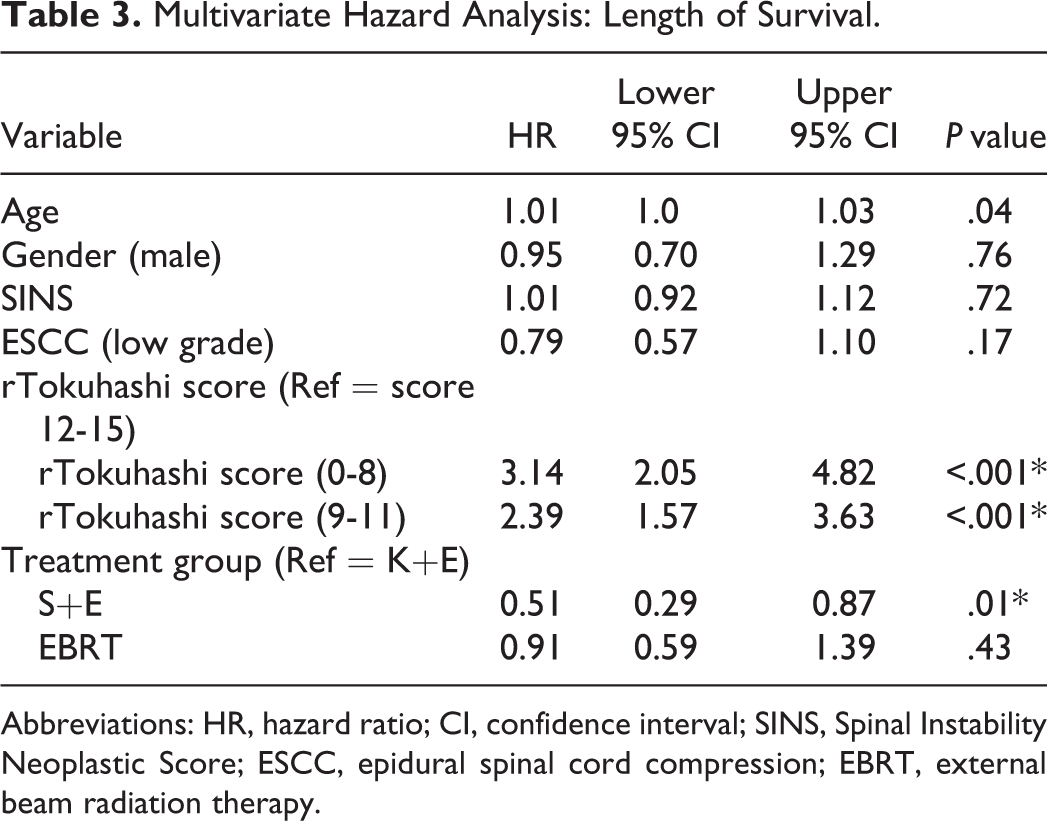
Abbreviations: HR, hazard ratio; CI, confidence interval; SINS, Spinal Instability Neoplastic Score; ESCC, epidural spinal cord compression; EBRT, external beam radiation therapy.
The subgroup analysis of S+E and EBRT patients with rTokuhashi scores greater than 8 included 45 S+E patients and 74 EBRT patients. The median LOS for the entire subgroup was 307 days (10 months), and 100 patients (84%) retained the ability to ambulate at their time of death (Table 4). In the S+E group, the median LOS was 639 days (1 year and 9 months), which was statistically longer than the median LOS of 172 days in the EBRT group (P < .001; Table 4 and Figure 3). In the S+E group, 91.1% of patients retained the ability to ambulate compared to 82.4% of patients in the EBRT group (P = .01). In the hazard analysis for this subgroup ESCC low-grade compression (HR 0.46, 95% CI 0.27-0.80, P = .005) and EBRT treatment (HR 2.79, 95% CI 1.49-5.25, P = .001) were independently predictive for LOS (Table 4).
Subgroup Analysis (rTokuhashi >8): Length of Survival, Ambulatory Status, and Multivariate Analysis.
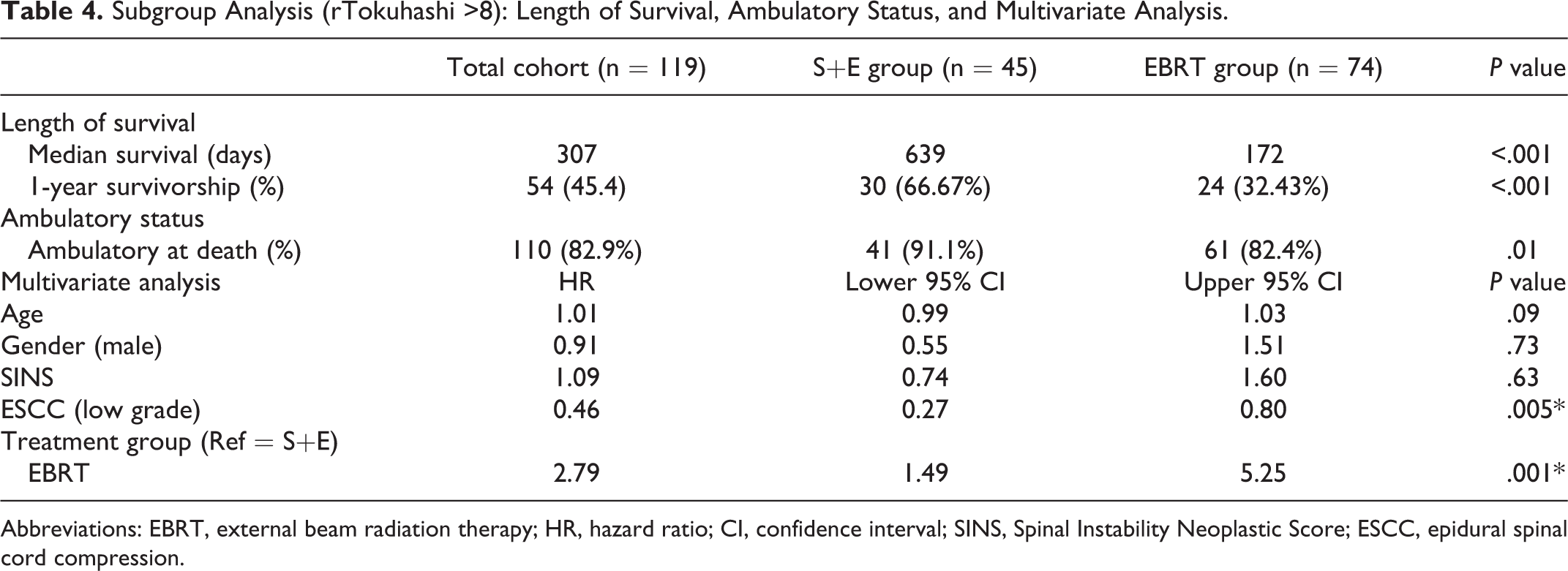
Abbreviations: EBRT, external beam radiation therapy; HR, hazard ratio; CI, confidence interval; SINS, Spinal Instability Neoplastic Score; ESCC, epidural spinal cord compression.
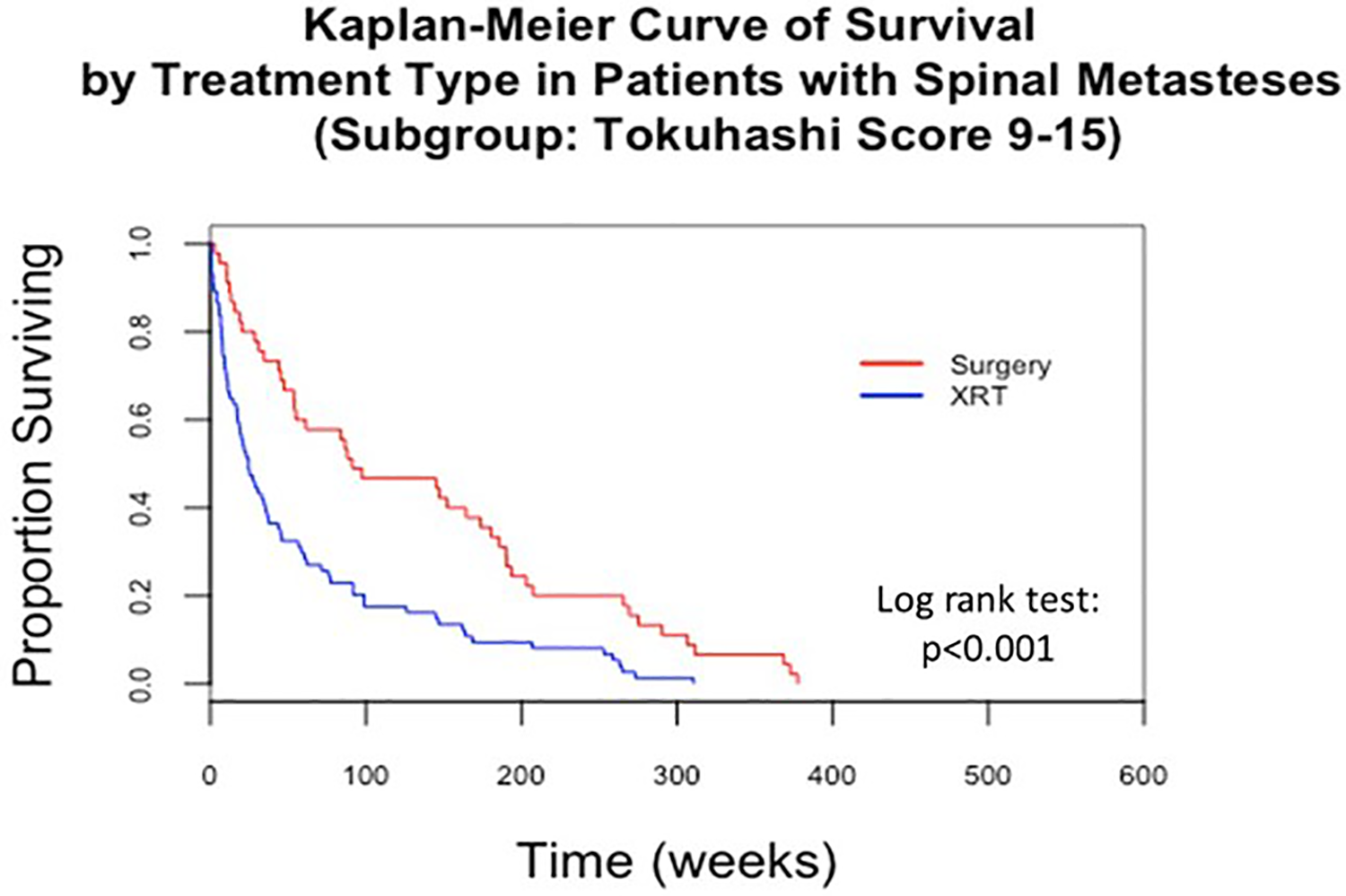
Survival curve for rTokuhashi scores greater than 8.
The overall rate of revision treatment at the spinal level initially treated was 17.5%. In the S+E group, 9 patients (15.8%) required revision surgery within the follow-up period. The revision surgeries were performed for wound complications or infection (n = 7) and new-onset neurologic symptoms (n = 2). In the EBRT group, 26 patients (20.3%) required revision treatment within the follow-up period: subsequent cement augmentation was performed in 6 patients for persistent back pain or pathologic compression fracture. Surgical stabilization was performed in 10 patients for persistent back pain or new-onset neurologic deficit. Repeat radiation therapy was performed in 10 patients for persistent back pain. In the K+E group, 2 patient (7.4%) required revision surgery for new onset neurologic symptoms (Table 5).
Need for Revision Treatment.
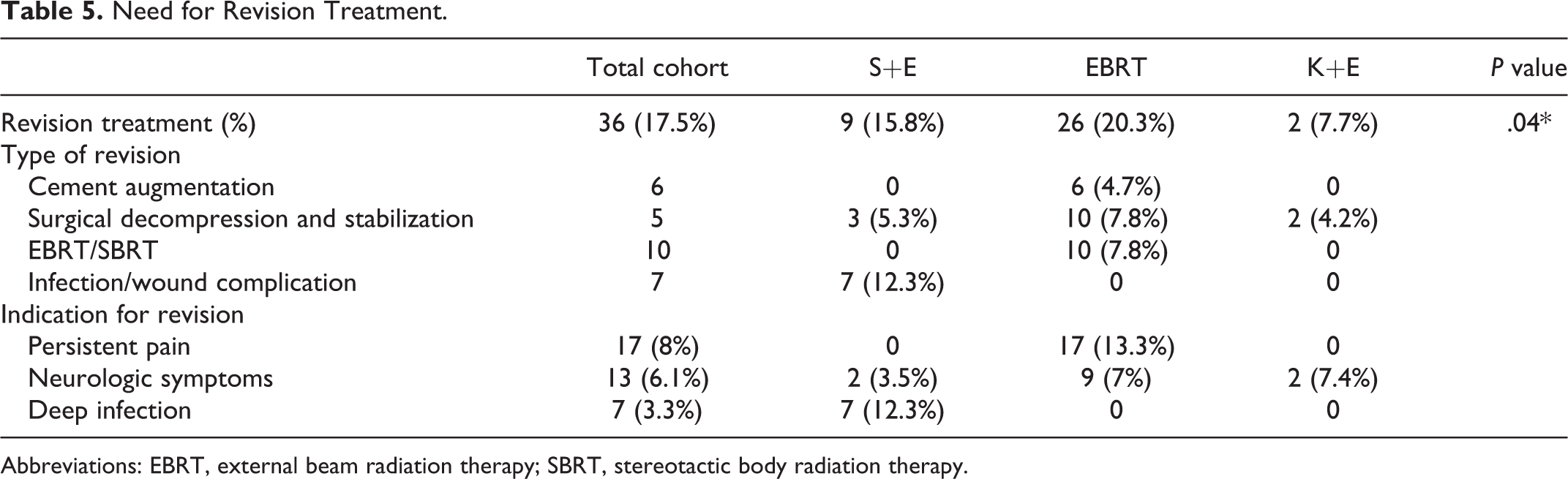
Abbreviations: EBRT, external beam radiation therapy; SBRT, stereotactic body radiation therapy.
Discussion
The decision on how to best manage patients with MSD is complex, and a multidisciplinary team should be involved in determining the ultimate treatment modality. In this study, we controlled for the neurologic status of the patient and the spinal stability, but still individual patients varied significantly. In general, patients that received surgical stabilization prior to radiation therapy were younger and had a better predicted length of survival based on the rTokuhashi score. Additionally, 61% of patients that were managed with surgical stabilization had tumor histology that has been historically considered radioresistant. Interestingly, of the 29 cases of RCC, which is known to respond poorly to radiation therapy, 16 cases were surgically stabilized, but 13 patients were treated with EBRT alone. The patients that were managed with cement augmentation and radiation had a similar age profile and rTokuhashi profile as patients that were treated with EBRT alone, but almost all of the patients that underwent cement augmentation had ESCC low grade compressive lesions.
The study outcomes of LOS, ability to ambulate at time of death, and revision treatment rates were selected based on these being clinically important patient outcomes that could be obtained in a retrospective manner. Other outcome variables such as health-related quality of life (HRQOL), patient satisfaction with treatment choice, and family satisfaction with treatment choice are necessary to consider when selecting the preferred treatment modality for an individual patient. Unfortunately, these and other critical outcome measures could be not obtained in a retrospective manner, and future prospective studies are indicated. The goal of this retrospective review was to provide the first data on survival outcomes, percent chance of retaining the ability to ambulate, and percent chance of requiring an additional treatment following 3 common treatment modalities for this specific patient presentation, indeterminate spinal instability without neurologic deficit.
Survival and ability to ambulate were significantly longer in patients managed with surgery and radiation therapy compared with patients managed with radiation alone. In the multivariate analysis we controlled for ESCC grade, rTokuhashi score, and patient’s age; and surgical stabilization remained an independent predictor for improved survival. A limitation of this analysis, which was inherent to the retrospective design of the study, is selection bias. The concern was that patients in the EBRT alone group or K+E group were medically less fit than patients in the S+E group. In an attempt to control for this, a subgroup analysis compared surgical stabilization and radiation therapy to radiation therapy alone in patients with rTokuhashi scores greater than 8 (anticipated survival >6 months). In the subgroup analysis surgical stabilization continued to be associated with prolonged survival and improved ability to ambulate compared to EBRT alone.
Surgical management for MSD should improve patients’ quality of life, but is not intended to alter the LOS. However, recent evidence has begun to demonstrate the importance of posttreatment performance status, and how performance status can influence LOS.9,10,22-25 In a study of 133 NSCLC patients treated with surgical stabilization or conservative management, the surgically treated group had better functional outcome scores and longer survivorship compared to the nonsurgical group. 8 Similarly, the results of our study demonstrated that a greater percentage of patients treated surgically retained the ability to ambulate compared to those treated with radiation alone. Similar to surgical stabilization, the patients treated with cement augmentation and radiation therapy retained the ability to ambulate at the time of death at a greater rate compared to radiation therapy alone. It is important to reiterate that in our cohort patients managed with cement augmentation had low-grade compressive lesions, which may place them at a lower risk of losing the ability to ambulate at baseline compared to those that were treated with surgical stabilization or radiation alone. In this cohort the patients treated with cement augmentation and radiation therapy had poorer survival compared to the surgically stabilized patients, and this finding can be explained by that the K+E group had lower rTokuhashi scores prior to treatment compared to the S+E group.
Spinal instability can result in mechanical pain, progressive deformity, neurologic injury, and pathologic fracture, all of which can be debilitating to a patient’s quality of life. The management of metastatic spinal lesions parallels the management of metastatic disease in long bones, and by providing stability through load sharing constructs one can prevent pathologic fracture and/or improve the patient’s quality of life. Radiation therapy reliably alleviates patient’s pain, but does not provide additional stability to the spine.13,14 A concern with radiation therapy alone for the treatment of patients with indeterminate spinal stability is persistent spinal instability and persistent instability related pain or neurologic injury following treatment.
In the current literature, 4 single-arm studies have investigated treatment success rates with radiation therapy alone with increasing spinal instability neoplastic scores.26-29 A retrospective review of 110 patients treated with radiation therapy alone found no correlation between SINS and adverse events. 26 A retrospective review of 299 patients with low-grade ESCC lesions treated with radiation therapy alone found that spinal instability scores greater than or equal to 11 were predictive of a spinal adverse event. 27 In a study of 124 MSD patients treated with radiation therapy, complete resolution of pain was achieved in patients with a SINS 0 to 6, and only partial resolution of pain was achieved in patients with a SINS >6, leading the authors to recommend stabilization for patients with indeterminate or unstable lesions. 28 The last study compared 2 groups of patients that required repeat radiation for persistent pain for MSD to those patients that had complete resolution of pain following the first treatment of radiation and found a higher average SINS in the group that required repeat radiation treatment. 29 These 4 studies largely evaluated patients with SINS ranging from 0 to 11, and the revision treatment rates ranged from 10.2% to 15%.26-29 In the current study the revision treatment rate for the EBRT alone group was 20.3%. The most common indication for revision treatment was persistent pain. The higher revision treatment rate observed in our cohort compared to previous studies could be because we included patients with a SINS from 7 to 12, and excluding patients with SINS 0 to 6, which made up many of the patients in the previous published studies. An additional factor that could be contributing to the high revision treatment rate in our cohort was the number of radioresistant tumors managed with EBRT alone. Nineteen of the 26 patients (73.1%) requiring additional treatment following radiation therapy had a radioresistant tumor (RCC n = 7, NSCLC n = 5, colorectal n = 3, cholangiocarcinoma n = 1, adrenal cancer n = 1, and adenoid carcinoma n = 1).
In the S+E group the reoperation rate was 15.8%. Six patients required reoperation for a deep surgical site infection or wound complication, and 2 patients required reoperation for new-onset neurologic symptoms. The surgical revision rate in this study was consistent with previous reports in the literature ranging from 10.7% to 22%.30,31 In the K+E group, only 2 patients were revised with surgical decompression and stabilization due to progressive neurologic deficits related to tumor progression. No patients in the S+E or K+E underwent repeat treatment for persistent pain alone.
As previously noted, the greatest limitations of this study are the presence of selection bias, and the omission of key outcome variables such as HRQOL and patient satisfaction with treatment choice. To account for selection bias we incorporated the rTokuhashi score in order to be able to compare the fitness of patients regardless of type of treatment received. The subgroup analysis of patients with rTokuhashi scores >8 was also an attempt to minimize selection bias by only comparing patients with a minimum of 6 months of predicted survival. In addition, we had a single reviewer determining the SINS and rTokuhashi scores, which did not allow for interobserver or intraobserver analysis. This can introduce measurement bias to the data set. For patients with controversial scores the senior author of this article determined the SINS or rTokuhashi. Last, the multivariable statistical outcomes for this study needs to be interpreted in the setting of a relatively small sample size. The small sample size can lead to less precise associations. An example being the S+E group was associated with greater survival (HR 0.51) in the multivariate analysis, but due to the smaller sample size the confidence interval ranged from 0.29 to 0.87. Therefore, the associated survival benefit of surgical resection could realistically only be 0.87.
The results of this study demonstrate that the choice of treatment for neurologically intact patients with indeterminate spinal stability has an impact on the patient’s outcome, and the risks and benefits of each treatment need to be discussed in detail prior to making a treatment decision. Surgical stabilization was independently associated with prolonged survival and prolonged ability to ambulate compared to those who were treated with EBRT alone. This association needs to be interpreted in the setting of potential selection bias and a relatively small sample size. Cement augmentation plus radiation had excellent outcomes with 93% of patients remaining ambulatory at their time of death and this treatment arm had the lowest revision treatment rate. The patients that received cement augmentation had low-grade compressive lesions, and from this data it cannot be determined if cement augmentation would have equivocal outcomes with high-grade compressive lesions. One important takeaway was that patients with indeterminate spinal instability and radioresistant tumors should not be treated with EBRT alone. Nineteen of the 26 patients with radioresistant tumors managed with EBRT alone required revision treatment. In summary, the results of this study demonstrate variability in treatment outcomes between surgical stabilization, cement augmentation, and radiation alone for the treatment of neurologically intact patients with indeterminate stability, and provide further clinical equipoise for future randomized controlled trials evaluating these treatment modalities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.