
Abstract
Study Design
Retrospective cohort study.
Objective
To build a predictive model for risk factors for failure of radiation therapy, hypothesizing a higher SINS would correlate with failure.
Methods
Patients with spinal metastasis being treated with radiation at a tertiary care academic center between September 2014 and October 2018 were identified. The primary outcome measure was radiation therapy failure as defined by persistent pain, need for re-irradiation, or surgical intervention. Risk factors were primary tumor type, Karnofsky and ECOG scores, time to treatment, biologically effective dose (BED) calculations using α/β ratio = 10, and radiation modality. A logistic regression was used to construct a prediction model for radiation therapy failure.
Results
One hundred and seventy patients were included. Median follow up was 91.5 days. Forty-three patients failed radiation therapy. Of those patients, 10 required repeat radiation and 7 underwent surgery. Thirty-six patients reported no pain relief, including some that required re-irradiation and surgery. Total SINS score for those who failed reduction therapy was <7 for 27 patients (62.8%), between 7-12 for 14 patients (32.6%), and >12 for 2 patients (4.6%). In the final prediction model, BED (OR .451 for BED > 43 compared to BED ≤ 43; P = .174), Karnofksy score (OR .736 for every 10 unit increase in Karnofksy score; P = .008), and gender (OR 2.147 for male compared to female; P = .053) are associated with risk of radiation failure (AUC .695). A statistically significant association between SINS score and radiation therapy failure was not found.
Conclusions
In the multivariable model, BED ≤ 43, lower Karnofksy score, and male gender are predictive for radiotherapy failure. SINS score was among the candidate risk factors included in multivariable model building procedure, but it was not selected in the final model.
Level of Evidence:
Prognostic level III
Keywords
Introduction
Fifty to eighty-five percent of patients with cancer will develop bony metastases; the most common location of bony metastatic disease is the spine.1,2 Spinal metastases can cause severe pain, disability, pathologic fracture, and neurological compromise with significant impact on patients’ remaining quality of life. 3
Treatment options for spinal metastases include radiation therapy, chemotherapy, surgical decompression, and stabilization. The goals of treatment are to provide durable local disease control, alleviate pain, restore spinal stability, and decompress the neural elements to address or prevent neurological compromise. The literature has established the therapeutic role of surgical decompression and stabilization prior to radiotherapy in the setting of cord compression secondary to metastatic cancer. 4 Spinal stability, or the ability of the spine to tolerate physiological loading without pain or compromise, is a significant consideration in surgical decision-making for this patient population.
In the absence of an evidence-based clinical definition of spinal instability, the Spine Oncology Study Group (SOSG) used consensus expert opinion to develop the Spine Instability Neoplastic Score (SINS), a classification system to quantify instability. 5 The goal of the SINS is to guide communication between providers, streamline referrals, and potentially aid surgical decision-making. Patients with a low SINS (<6) are at low risk for instability and are treated with radiation therapy; conversely, a high SINS (>12) is suggestive of spinal instability and evaluation by a spine surgeon is recommended. A moderate SINS (6-12) represents an indeterminant or potentially unstable lesion. This classification system has since been shown to have high inter- and intra-observer reliability (.846 and .886 respectively). 6 It should be noted that limited research into the benefits of surgery in the indeterminant stability category has been undertaken.
Radiation therapy has a well-documented role in the management of this patient population. Conventional external beam radiation therapy (EBRT) has been shown to alleviate pain in up to 70% of patients. 7 Stereotactic body radiotherapy (SBRT) allows for higher radiation dosages to be concentrated at the lesion with the goal of durable tumor control, while sparing the spinal cord.7,8 Despite these benefits, radiation therapy has been shown to increase the risk of vertebral compression fractures (VCFs), particularly when SBRT is performed.7-15 Risk factors for the development of VCFs after treatment with SBRT include VCF prior to the initiation of treatment, lytic lesions, and spinal misalignment.7,8,10,11,13,14,16 While fewer studies have examined VCFs following treatment with EBRT, VCFs prior to initiation of treatment and the presence of lytic lesions were demonstrated to be risk factors.11,12,17
While SINS is widely accepted as a tool for evaluating spinal instability, there is limited research studying how SINS correlates with the rate of skeletal related events (SRE) or failure after radiation therapy. The purpose of the present study is to identify risk factors that predict failure of radiation therapy. Failure was defined as persistent pain, the need for re-irradiation, or surgical intervention after radiation therapy. We hypothesized that a higher SINS score would predict failure of radiation therapy.
Materials and Methods
We conducted an IRB approved retrospective cohort study (Oregon Health & Science University Institutional Review Board, #16170). Given the retrospective nature, this study was deemed exempt from obtained informed consent. Consecutive patients with spinal metastases being treated with radiation therapy to the spine at a tertiary academic center between 9/2014 and 10/2018 were identified. Patients over the age of 18 with metastatic cancer to the spine and a computed tomography (CT) scan or magnetic resonance imaging (MRI) study of the lesion were eligible for inclusion in the study. Patients with multiple lesions, treated either simultaneously or subsequently, were eligible as long as there was documentation sufficient to localize the pain and evaluate for pain resolution after therapy. Individual treatment fields were considered as two separate courses of radiation therapy. Patients with myeloma, leukemia, lymphoma, primary bone tumors or metastatic sarcoma were excluded. Patients presenting with cord compression and those with a history of prior radiation or surgical intervention to the area being treated were excluded. Patients who had inadequate follow up or documentation to evaluate the outcomes were excluded. Follow up time was calculated as days since initial radiation oncology evaluation. In patients who died, timing of death was calculated as days since final radiation treatment.
The SINS for each lesion was calculated as described by the SOSG. 5 Other potential risk factors were collected through chart review. The variables included were primary tumor origin, sensitivity to radiation, age, gender, Karnofsky and ECOG score, Tomita score, time between diagnosis and initiation of treatment, radiation technique and dose (conventional external beam or stereotactic radiation), and number of vertebrae involved in the treatment area. Similarly, pain was assessed through chart review; no standardized scoring system was utilized. Tumor histology was grouped into breast, prostate, lung, renal, and other. Breast and prostate cancer were defined as radiosensitive as skeletal breast and prostate metastases have been shown to be more responsive to radiation therapy than other solid tumors. Radiation dose was standardized using the biologically effective dose (BED) assuming an α/β ratio = 10, and BED was categorized as more or less than 43. The biologically effective dose is routinely used in radiation oncology research to standardize different dosing regimens in different tumor types and accounts for the cell kill-rate of various tissues. 18 The cut off of 43 was selected based on expert opinion after discussion with our radiation oncology department, as it represents the common dose of 24 Gy in 3 fractions utilized at our institution.
The primary outcome for this study was radiation therapy failure as defined as persistent severe pain, need for re-irradiation, or surgical intervention after radiation therapy. Re-irradiation was specifically indicated for local tumor progression or persistent pain.
Statistical Analysis
Descriptive statistical analysis was conducted for patient characteristics and outcome variables. Univariate analysis was performed using Chi-squared or Fischer’s exact test for categorical variables and two-sample t-test for continuous variables. Variables with a P-value < .2 in the univariate analysis were used to build the initial multivariable logistic regression model. For the continuous variables (total SINS, age, Tomita, ECOG and Karnofsky), we examined their relationship with outcome variable graphically to assess whether it is appropriate to assume linearity in logit of the outcome. Categorical forms of age (≥66; <66), total SINS (<7; 7-12; >12) and Tomita score (0-4; 5-7; 8-10) were used. Due to the high collinearity between Karnofsky and ECOG scores, the ECOG was dropped because it had a weaker association with radiation failure than the Karnofsky score. From the initial multivariable model, an automated stepwise (backwards) model selection procedure by AIC (Akaike information criterion) was used to select a parsimonious main effect only model that accomplishes a desired level of prediction without over-fitting the current data. Youden’s 19 index was used to select the optimal cut-point on the receiver operating characteristic curve (ROC).
Results
A total of 547 adult patients were treated with radiation for spinal metastases between 9/2014 and 10/2018. Patients were then excluded who had cord compression (n = 26), primary bone disease (n = 23), myeloma, lymphoma, leukemia or metastatic sarcoma (n = 84), prior radiation to the area (n = 19), prior surgical intervention to the treatment area (n = 45), multiple simultaneous indistinguishable areas of treatment (n = 67), and no demonstrated lesion on CT or MRI (n = 17). There were 19 that died prior to follow up and 32 that were lost to follow up. One hundred and seventy patients met criteria and were included in the review (Figure 1). Median follow up was 91.5 days. Participant eligibility flow diagram.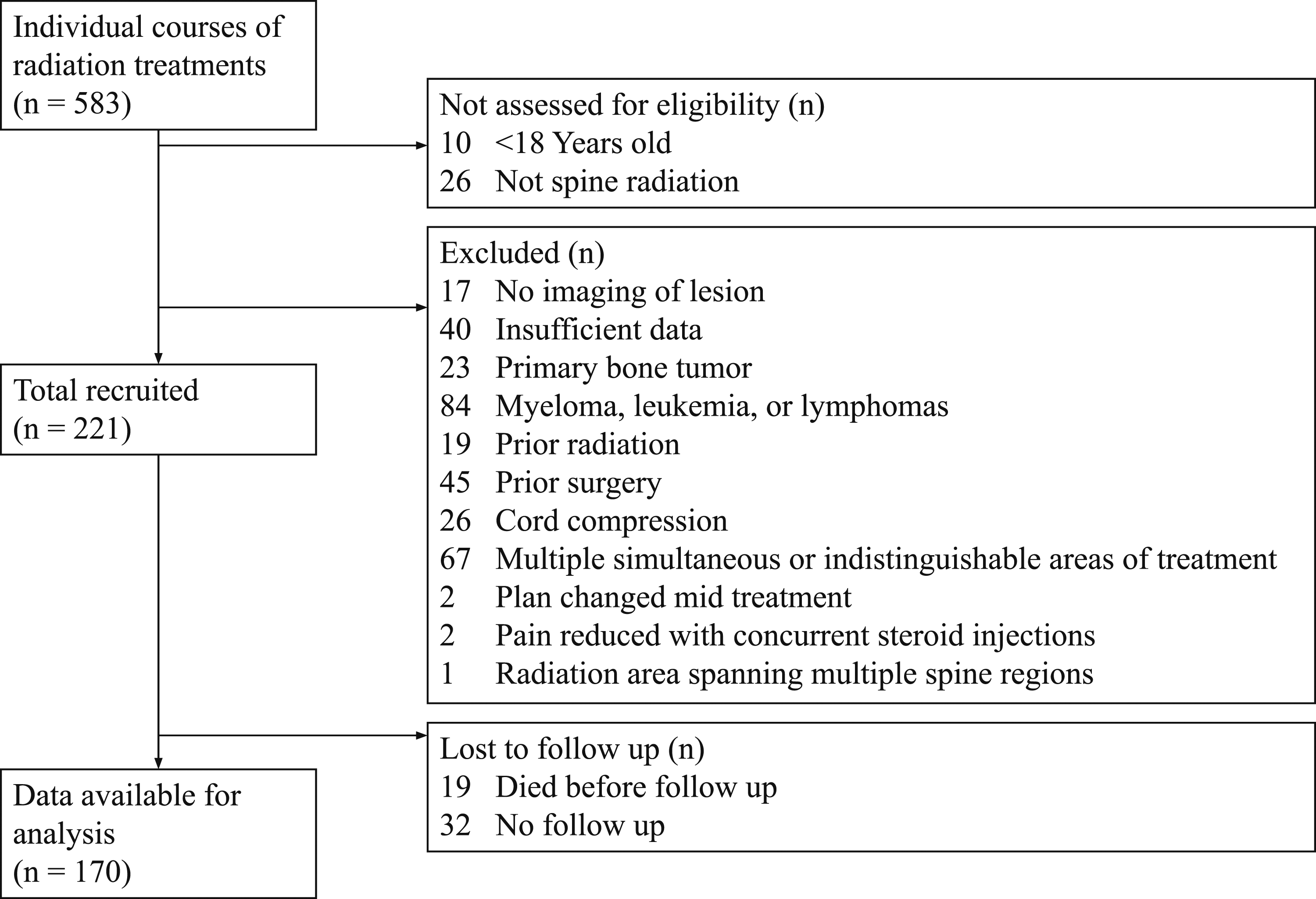
Radiation failure occurred in 43 treatment courses. Ten patients required re-irradiation to the area, 7 required surgery, and a total of 36 reported no pain relief. Some patients failed radiation therapy in more than one way, such as not having pain relief and needing surgery. Ultimately, 71 patients died. Median time to death was 138 days.
Univariate Analysis of Risk Factors. P-values < .2 Included in Multivariate Analysis; Shown in Bold.
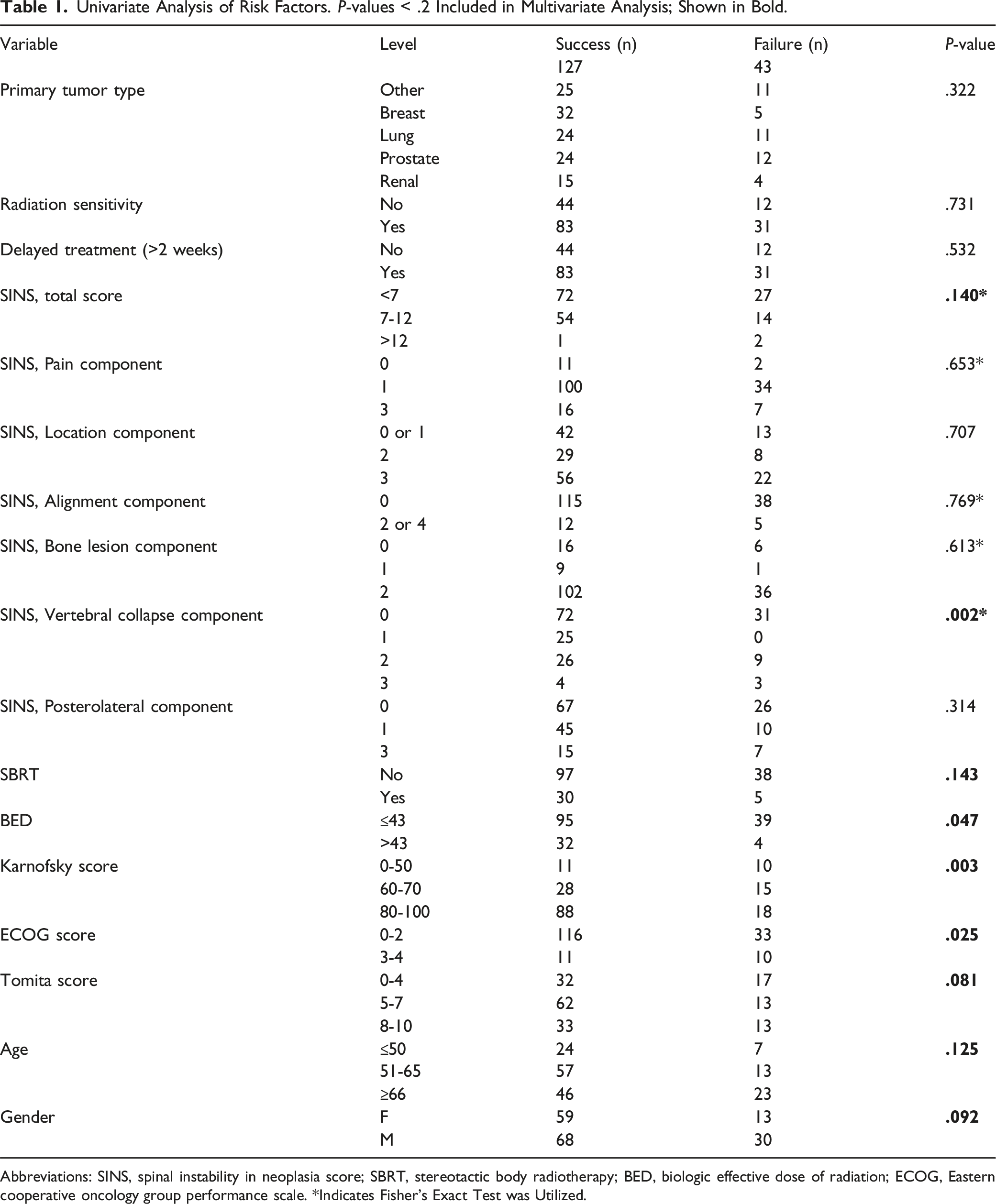
Abbreviations: SINS, spinal instability in neoplasia score; SBRT, stereotactic body radiotherapy; BED, biologic effective dose of radiation; ECOG, Eastern cooperative oncology group performance scale. *Indicates Fisher’s Exact Test was Utilized.
Univariate analysis was performed using Chi-squared or Fischer’s exact test for categorical variables and two-sample t-test for continuous variables (Table 1). Variables with a P-value < .2 in the univariate analysis were used to build the initial multivariable logistic regression model.
Risk Factors and Odds Ratios in Multivariate Model. BED – Biological Effective Dose.

Abbreviation: BED, biologic effective dose of radiation.
Discussion
Spinal metastases are common in patients with cancer and represent a significant burden of disease. Metastases can cause spinal instability, fracture, and deformity, resulting in pain, disability, neurological compromise, and mortality.5,6 The mainstay of treatment is radiation; however, the indication and timing of surgical intervention remains a challenge for clinicians. The benefits of surgical intervention must be weighed against the risks and invasiveness of the procedure and the medical fitness and life expectancy of the patient. This decision is made in conjunction with a multi-disciplinary team consisting of spine surgeons, medical oncologists, and radiation oncologists. Patchell et al 4 demonstrated that patients with neurological compromise have improved outcomes with surgical decompression and stabilization. However, the treatment of patients with painful spinal metastases without neurological deficits remains a challenge. 20 While it is well accepted that patients with spinal instability require surgical stabilization, many patients fall into the category of indeterminate stability (SINS 7 – 12). It is unclear which of these patients would benefit from surgical intervention.
In order to understand how to best surgically manage these patients it is imperative to understand which patients are at increased risk of failing radiation therapy. Our study sought to analyze risk factors for failure of radiation therapy as it relates to the SINS as well as performance scores. In regard to our hypothesis, we did not find that increased SINS was associated with radiation failure in our multivariate model.
Lam et al 11 studied risk factors for failure of radiation treatment in uncomplicated spine metastases and found a SINS >11 and a single fraction of radiation therapy to be predictive of a skeletal adverse event. Similarly, Huisman et al 21 found that an increased SINS was significantly and independently associated with radiotherapy failure. However, we did not identify a significant association between SINS score and radiation failure. One potential factor is the small number of radiation failures found in our cohort. Additionally, few patients with SINS scores > 12 were included, largely attributable to the exclusion criteria specified for this study. This limited the variation in SINS scores and thus may have obscured a more nuanced relationship between SINS score and radiation therapy failure. The prognostic value of the SINS score in predicting radiation failure requires further investigation with a well-done prospective study.
The benefits of surgical stabilization also require further study; however, there is recent data demonstrating the value of surgical intervention in patients with indeterminate and high SINS (>7). Versteeg et al 22 and the SOSG found that patients with indeterminate SINS (7 – 12) had early and lasting increases to health related quality of life scores, starting at 6 weeks and sustained out to 1 year post-operatively. Patients treated with radiotherapy alone had improvements in pain scores although these were not sustained past 3 months.
Surprisingly, radiosensitivity of the tumor, and radiation modality (SBRT vs EBRT) were not found to be significantly associated with radiotherapy failure in our univariate model (Table 1). Increased BED was included in the multivariate model (OR .451) and was associated with a lower risk of radiation failure but was not statistically significant (P = .174) (Table 2). The BED is the cumulative radiation dose standardized across tissues using an alpha/beta ratio. The alpha/beta ratio for rapidly growing tissues such as tumors is generally set at 10, while the ratio for neural tissues is 2. This is an area that requires more research, as optimal dosing for radiotherapy in spinal metastatic disease is controversial. Low dose therapy runs the risk of recurrence while high dose therapy puts the patient at risk of radiation related complications, including vertebral compression fracture and radiation induced myelitis.23-25 Many radiation oncologists are concerned about applying high dose fractions of radiation (8 Gy) to the spinal cord due to the risk of late toxicity. However, studies have found cumulative BED to the spinal cord to be safe at doses as high as 120 Gy, assuming an alpha/beta ratio of 2.26,27 This is important as the cut off of 43 for BED assumes an alpha/beta ratio of 10 but coincides with the most commonly deployed regimen of 24 Gy in 3 fractions in our cohort-this yields a cumulative BED of 120 Gy when the alpha/beta ratio is two. Other studies have found that escalating radiation doses is effective at increasing local control in patients with favorable prognoses but did not find the same dose related effect when treating patients with radioresistant tumors to the spine.28,29 One study described the effects of BED > 50 in renal cell metastases at different anatomic sites and found that it was associated with increased response to treatment. 30 Total BED appears to be associated with response of spinal metastases to radiation treatment, however the optimal dosing in the setting of potential spinal instability is not known.
Male gender was included in the multivariate model (OR 2.147) as a predictive factor for radiation failure but only approached significance (P = .053) (Table 2). There is limited data on the effect to gender in the treatment of bony metastasis with radiotherapy. Several prior studies have described worse outcomes in males with radiotherapy for various cancer types, including brain metastases, retroperitoneal sarcomas, and head and neck cancer.31-34 The reasons for this have not been delineated. It should be noted that the most common site of metastasis of prostate cancer is to the spine, with approximately one third of these lesions becoming symptomatic due to mechanical instability or neurological deficit.35,36 While this may be one contributing factor influencing the efficacy of treatment, further research is warranted on the role of gender in the treatment of spinal metastases.
Finally, we found that a higher Karnofsky performance score was associated with a decreased risk of radiotherapy failure. The Karnofsky score is on a scale from 0 – 100 and is widely used to report the functional status. Each 10 point increase in Karnofsky was associated with a decreased odds of radiotherapy failure (OR .736; P-value = .008). Prior studies corroborate this and have found that a Karnofsky greater than 70 was associated with response to radiation treatment in renal cell carcinoma metastases. 30 Intuitively this makes sense, as a lower performance score may be a surrogate for the pain and morbidity of spinal instability. However, we cannot make any determinations as to why performance score is associated with failure given the retrospective nature of the study. This is, however, a very important area for further research, and prospective studies should be conducted to delineate the role that the performance score plays in response to treatment, be it radiotherapy or surgical intervention.
The strength of this study is that it was conducted on a relatively large cohort of patients. We looked at a wide variety of risk factors for failure, including gender, Karnofsky score, and BED. This is an important area of research as there is limited available data on the risk factors for failure of radiation therapy in spine metastases. The limitations of this study are several and are related to its retrospective nature. The evaluation of pain relief was subjective due to documentation. It would have been preferable to have objective data with VAS scores before and after radiotherapy. Despite our large patient cohort there was a relatively small number of failures (n = 43). This inherently limits statistical analysis. More numbers would allow us to better analyze risk factors for different modes of failure. Finally, we cannot determine causation from this study as it is retrospective. Our multivariate analysis shows associations, but we can only conjecture as to why each risk factor affects treatment outcome. It is important to note that this study does not provide information on which patients would do better with surgical management of spinal metastasis. It does serves as a basis for more robust prospective studies on the effects of risks factors on outcomes of radiotherapy and surgical management.
In conclusion, a lower Karnofsky performance score predicted an increased risk of radiotherapy failure. SINS group was not a significant risk factor after controlling for all other important variables in the model.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.