
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare outcomes of percutaneous pedicle screw fixation (PPSF) to open posterior stabilization (OPS) in spinal instability patients and minimal access separation surgery (MASS) to open posterior stabilization and decompression (OPSD) in metastatic spinal cord compression (MSCC) patients.
Methods
We analysed patients who underwent surgery for thoracolumbar metastatic spine disease (MSD) from Jan 2011 to Oct 2017. Patients were divided into minimally invasive spine surgery (MISS) and open spine surgery (OSS) groups. Spinal instability patients were treated with PPSF/OPS with pedicle screws. MSCC patients were treated with MASS/OPSD. Outcomes measured included intraoperative blood loss, operative time, duration of hospital stay and ASIA-score improvement. Time to initiate radiotherapy and perioperative surgical/non-surgical complications was recorded. Propensity scoring adjustment analysis was utilised to address heterogenicity of histological tumour subtypes.
Results
Of 200 eligible patients, 61 underwent MISS and 139 underwent OSS for MSD. There was no significant difference in baseline characteristics between MISS and OSS groups. In the MISS group, 28 (45.9%) patients were treated for spinal instability and 33 (54.1%) patients were treated for MSCC. In the OSS group, 15 (10.8%) patients were treated for spinal instability alone and 124 (89.2%) were treated for MSCC. Patients who underwent PPSF had significantly lower blood loss (95 mL vs 564 mL; P < .001) and surgical complication rates(P < .05) with shorter length of stay approaching significance (6 vs 19 days; P = .100) when compared to the OPS group. Patients who underwent MASS had significantly lower blood loss (602 mL vs 1008 mL) and shorter length of stay (10 vs 18 days; P = .098) vs the OPSD group.
Conclusion
This study demonstrates the benefits of PPSF and MASS over OPS and OPSD for the treatment of MSD with spinal instability and MSCC, respectively.
Keywords
Introduction
Metastatic spine disease (MSD) is associated with a decrease in quality of life with complications including cord compression, pathological fractures and spinal instability. 1 Symptomatic spinal cord compression may be present in 10–20% of patients with MSD. 2
In the past, radiotherapy was the standard of care for symptomatic spinal metastases. 3 In 2005, Patchell et al. 4 demonstrated the superiority of surgery with adjuvant radiotherapy over radiotherapy alone in patients with metastatic spinal cord compression (MSCC), which led to an increase in metastatic spine tumour surgery (MSTS). 5 The decision for surgical treatment of MSD is based on the presence of neural compression, instability, tumour histology and the patient’s prognosis.1,6 The goals of surgery include improvement in neurological function; achievement of spinal stability and pain relief; separation of tumour from neural elements to allow safe adjuvant radiotherapy and local tumour control and acquiring tumour tissue for histological subtyping. 7
Open spine surgery (OSS) with stabilization and decompression is the current gold standard of surgical treatment in MSD. However, OSS is associated with extensive soft tissue dissection leading to excessive blood loss, 8 increased hospital stay and complication rates. 9 This is undesirable in MSD patients with limited life expectancies and multiple comorbidities.10,11 In recent years, advancements in surgical techniques and technology have led to the advent of minimally invasive spine surgery (MISS). The aim of MISS is to achieve the same surgical goals as OSS, with the minimisation of approach-related morbidity.12,13 Percutaneous pedicle screw fixation (PPSF) has now become a common MISS modality of spinal stabilization in MSD, associated with lower blood loss, good pain relief, faster initiation time to radiation therapy and reduced complication rates.12-15 Its main advantage is the ability to stabilize the spine without excessive dissection of the posterior skeletal musculature.
There is still debate about the best surgical approach and extent of resection needed to treat MSCC. While anterior approaches may be effective in achieving ventral decompression, they are associated with significant approach related morbidity. 16 In recent years, the transpedicular approach as described by Bilsky et al. 17 has increased in popularity as circumferential decompression can be achieved via a posterior approach without the morbidity of an anterior approach. Minimal access approaches have been described to perform both separation surgery and anterior reconstruction. 18
In this study, we describe our experience and outcomes in using MISS techniques of PPSF and minimal access separation surgery (MASS) compared to conventional open surgical decompression and stabilization in patients with spinal instability and MSCC.
Materials and Methods
We retrospectively analysed all patients aged >21 years who underwent surgery for thoracolumbar MSD at our tertiary referral centre, during January 2011–October 2017. Institutional review board (IRB) approval (DSRB ref., 2014/00050) was sought prior to study commencement. Informed consent was not required as a waiver of consent was granted by the IRB due to anonymisation and retrospective nature of the data. Surgical indications included spinal instability, and MSCC qualified by clinical neurological deficit with evidence of radiological cord compression. Spinal instability was considered as ‘present’ if Spinal Instability Neoplastic Score (SINS) was ≥13 and ‘indeterminate’ if SINS was between 7 and 12. 19 MSCC was classified as Bilsky grade 2 or 3 epidural spinal cord compression 20 and/or the presence of motor weakness and sensory impairment. Exclusion criteria included cervical MSD, revision cases, combined anterior and posterior surgery and patients who underwent combined open and MISS techniques. En bloc spondylectomy and vertebroplasty/kyphoplasty were also excluded.
Patient data collected included demographic characteristics, tumour histology and clinical findings in relationship to the primary tumour and skeletal metastases. Clinical findings recorded at the time of surgery included Karnofsky performance scale; number of vertebral/extraspinal bone and visceral metastases and neurologic assessment. Preoperative Tokuhashi score, 21 Eastern Cooperative Oncology Group (ECOG) score, Charlson comorbidity index (CCI) and ASIA score were also recorded. Preoperative radiological investigations such as magnetic resonance imaging (MRI), computed tomography (CT) spine and/or bone scan provided the data on pathological fracture and MSCC.
Patients were treated with either MISS or OSS. Minimally invasive surgery was introduced at our institution by the first author in 2010. However, the choice of open surgery vs MISS was guided by the overarching principles of MSTS. The final treatment decision was made based on inputs from a multidisciplinary team comprising of surgical colleagues, and radiation/medical oncologists, keeping in view, the patients’ prognosis and suitability for surgery or other alternative forms of treatment. Patients with extensive visceral metastasis (>3 areas of solid organ involvement) were preferentially done via a minimally invasive approach if permitted. Patients with clinical spinal instability alone guided by SINS (pathological fractures requiring fixation with no clinical and/or radiological compression) were treated with PPSF or open posterior stabilization (OPS) with pedicle screws. Patients with MSCC guided by Bilsky score (clinical and/or radiological cord compression with or without a fracture) were treated with MASS or open posterior stabilization and decompression (OPSD). Standard spinal instrumentation constructs were utilized; no cemented screws were used.
The surgical procedure (MISS or open) was conducted with great care to avoid tumour contamination, even though all our patients had stage 4 malignancy. During the surgical procedure, care was taken to find the proper plane between the neural elements and the offending tumour tissue. Near total resection of the tumour tissue was carried out with a view to relieve the compression on the neural elements while creating a 3–5 mm gap between the residual tumour and neural elements. After resection of the tumour, the surgical site was irrigated with adequate amounts of normal saline and sterile water in accordance with the established protocols.
Primary outcomes included intraoperative blood loss, operative time, duration of hospital stay and improvement in ASIA score. While secondary outcomes included time to initiate radiotherapy and presence of perioperative complications. Perioperative complications were divided into surgical and non-surgical. A delay in initiating oncological treatment was defined as time to initiation of radiotherapy >3 week. Overall survival and disease-free survival are guided by tumour type, tumour burden at the time of presentation and response to radiotherapy and chemotherapy.10,12 While survival outcomes were calculated, the primary focus of our study was on evaluating surgical outcomes of MISS vs open surgery.
Open Spine Surgery Technique
In patients undergoing OSS for spinal instability alone, OPS was performed through a posterior single midline incision, which spanned at least 2 vertebrae above and below the involved pathological vertebra. Pedicle screws were inserted using free hand techniques. In patients with MSCC, in addition to the above, laminectomy and pedicle resection, followed by partial corpectomy, if required was performed to achieve circumferential decompression.
Minimally Invasive Spine Surgery Technique
Percutaneous Pedicle Screw Fixation
A posterolateral stab incision was made over the vertebra to be instrumented in line with the pedicle under radiographic guidance, followed by blunt dissection of the deep fascia and muscles. The pedicle entry point was identified under radiographic guidance and a cannulated pedicle screw was inserted as per the standard surgical technique. In patients with multiple levels of involvement with spinal instability as defined by the SINS score, the involved vertebrae were spanned by pedicle screws with a minimum of 2 vertebrae instrumented above and below the involved level.
Minimal Access Separation Surgery
In patients undergoing MASS, screw insertions were made through stab incisions dictated by standard MIS techniques. The lamina of the involved vertebra was approached by a muscle-splitting technique by joining the 2 stab incisions adjacent to the pathological vertebra. This minimal access approach allowed enough visualization to perform laminectomy, over the top decompression, pediculectomy and partial corpectomy to achieve a circumferential decompression and separation of the neural elements from the residual tumour. The side of approach was decided by the clinical and radiological assessment of the compression of neural elements. Muscle splitting was the primary modality of deeper dissection in most cases.
All our circumferential decompressions (MISS or open) were done by the posterior approach, with appropriate sacrifice of the thoracic nerve roots, if needed, to achieve the surgical outcome. The amount of tumour resection was attempted to be similar in both groups (MASS and OPSD). It is evident from the literature that approach-related complications will be theoretically less in MIS due to the length of skin incision and amount of muscle dissection. Length of skin incision in OPSD was variable and was dependent on the number of levels being treated and the body girth (which in turn is dependent on patient characteristics such as body mass index and obesity).
Statistical Analysis
Statistical analysis was performed with the use of SPSS statistical software (IBM SPSS Statistics Version 22). The surgical outcomes by indications, namely, MSCC and/or instability, were compared by using Mann–Whitney U test for numerical variables, and chi-square test or Fisher exact test for categorical variables. As our data cover 7 years of MSTS with a wide array of various histological tumour subtypes, a propensity score was calculated utilising the following key variables, age, type of the tumour, modified Tokuhashi score and extent of visceral metastasis, within each group defined by the surgical indications. Linear regression was used to adjust the propensity score when comparing the numerical outcomes between MIS and open surgery, while logistic regression was used when comparing the binary outcomes. The propensity score adjusted P-value is reported. A P-value of < .05 was considered to be significant. Overall survival was presented with Kaplein–Meir analysis.
Results
Demographic Data
Baseline Characteristics of the Study Participants.
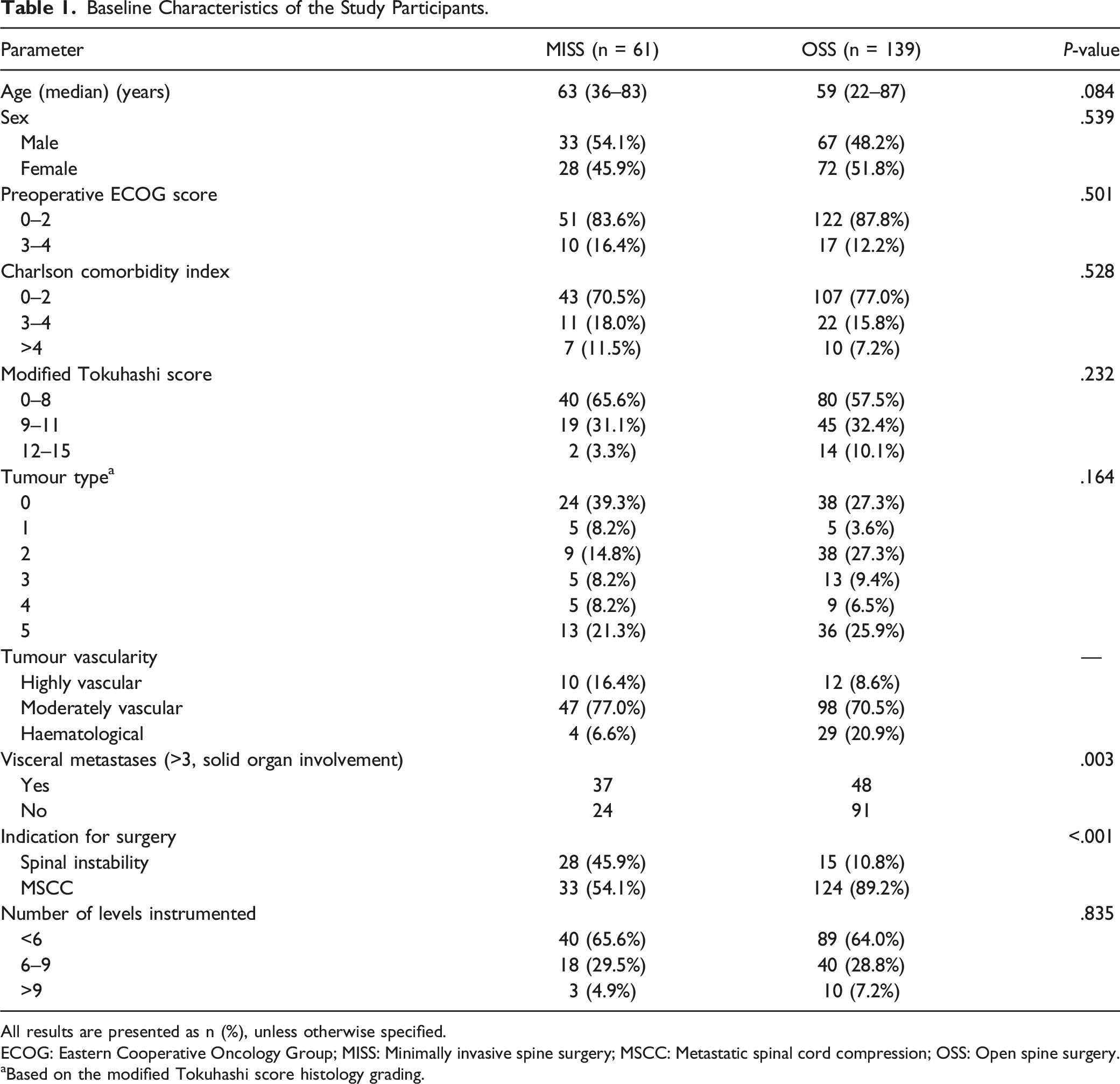
All results are presented as n (%), unless otherwise specified.
ECOG: Eastern Cooperative Oncology Group; MISS: Minimally invasive spine surgery; MSCC: Metastatic spinal cord compression; OSS: Open spine surgery.
aBased on the modified Tokuhashi score histology grading.
We performed an analysis comparing the outcomes in patients who underwent spinal surgery for instability alone (PPSF vs OPS) and patients who underwent surgery for MSCC (MASS vs OPSD).
Percutaneous Pedicle Screw Fixation vs Open Posterior Stabilization
Comparison of Outcomes Between PPSF and OPS Patients.
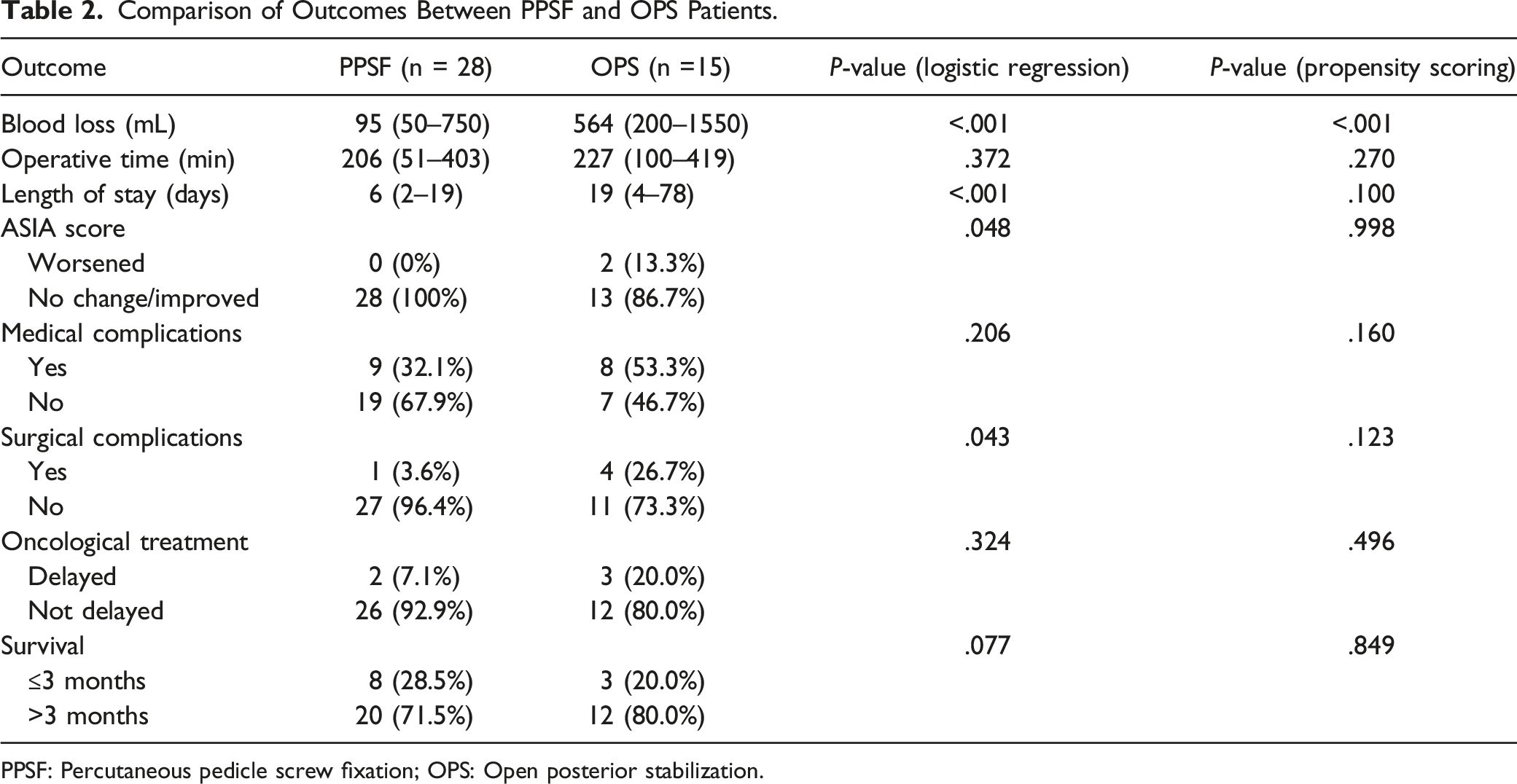
PPSF: Percutaneous pedicle screw fixation; OPS: Open posterior stabilization.
Minimal Access Separation Surgery vs Open Posterior Stabilization and Decompression
Comparison of Outcomes Between MASS and OPSD Patients.
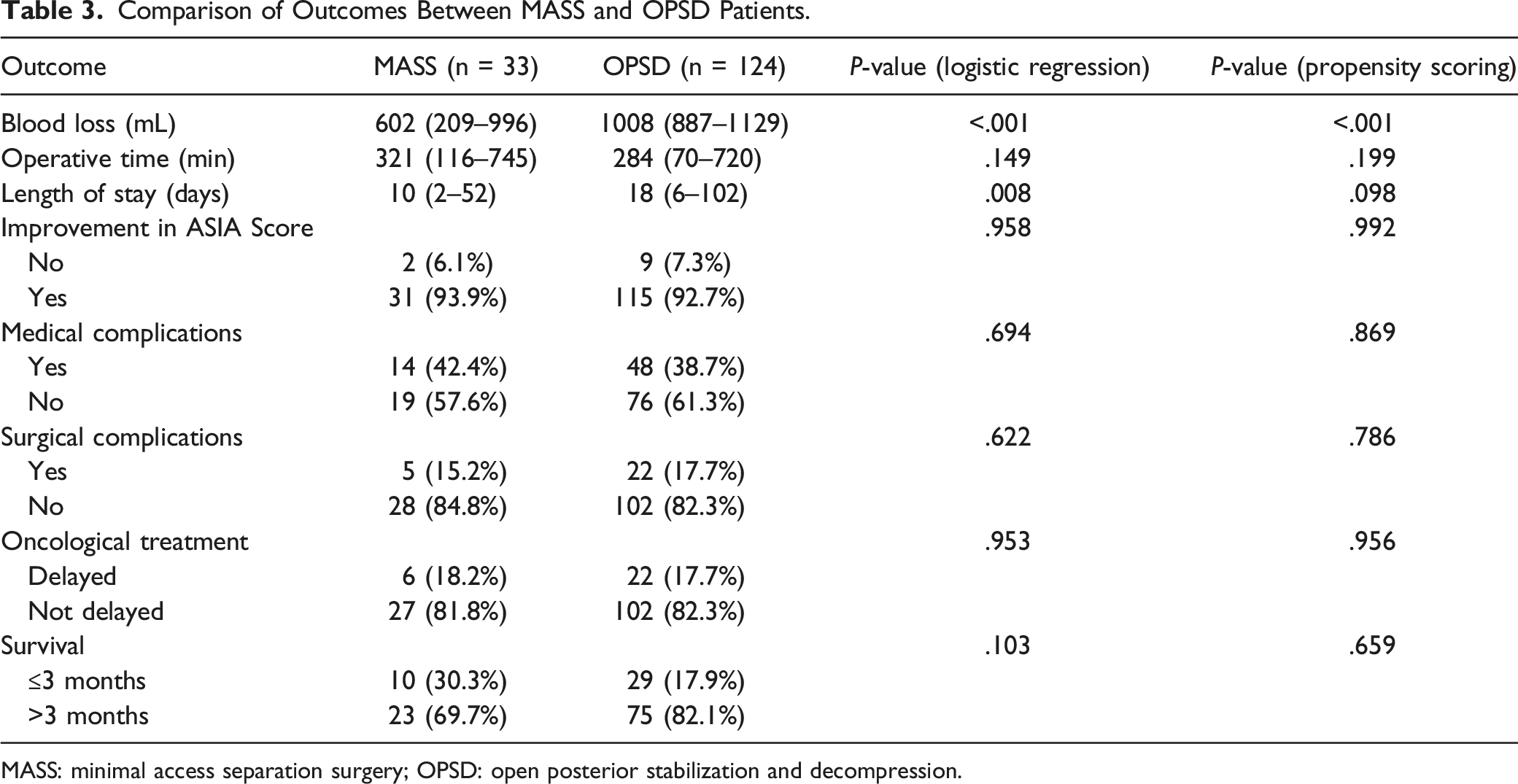
MASS: minimal access separation surgery; OPSD: open posterior stabilization and decompression.
Perioperative Complications
Surgical and Non-Surgical Complications in MISS Vs OSS Groups.
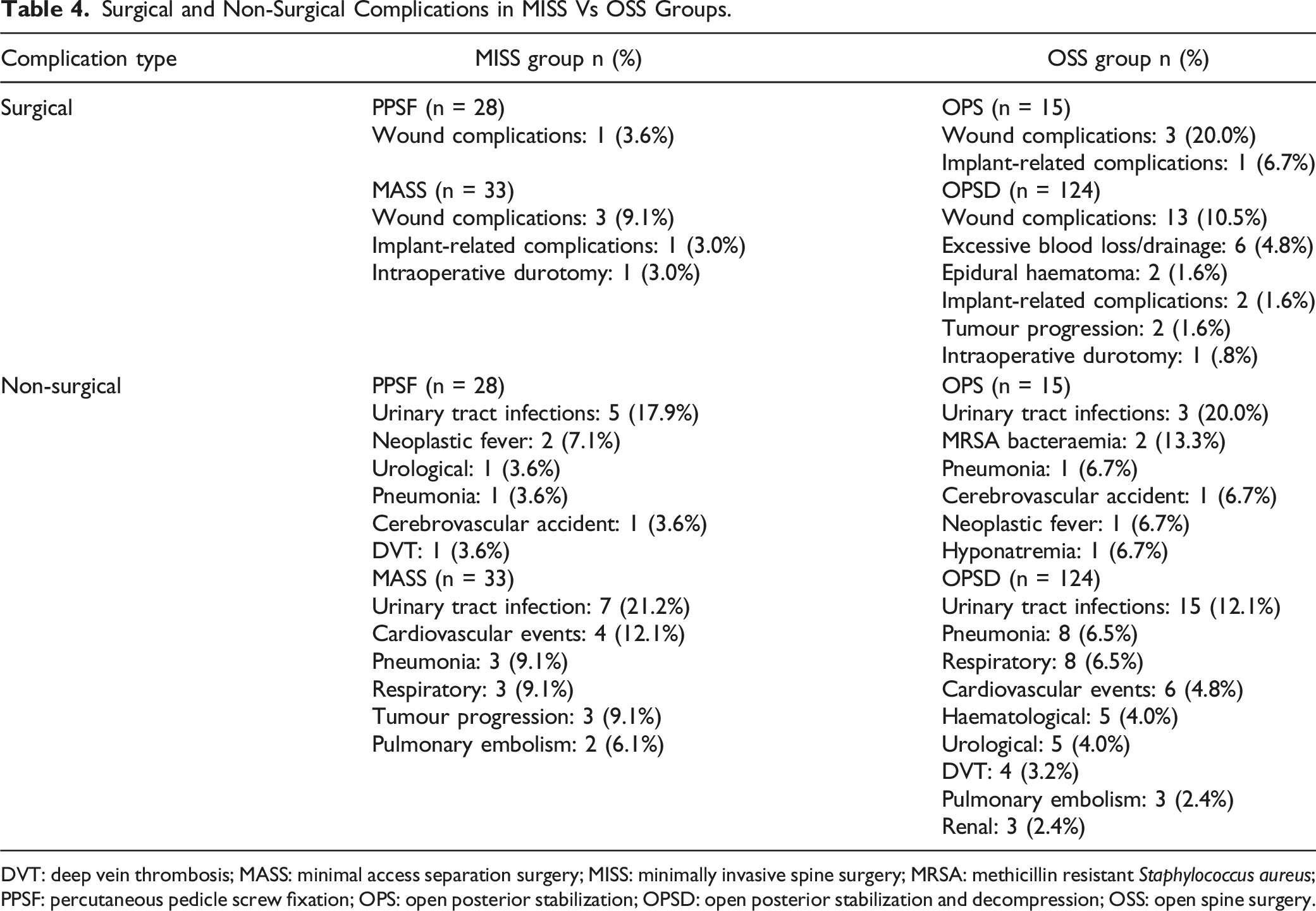
DVT: deep vein thrombosis; MASS: minimal access separation surgery; MISS: minimally invasive spine surgery; MRSA: methicillin resistant Staphylococcus aureus; PPSF: percutaneous pedicle screw fixation; OPS: open posterior stabilization; OPSD: open posterior stabilization and decompression; OSS: open spine surgery.
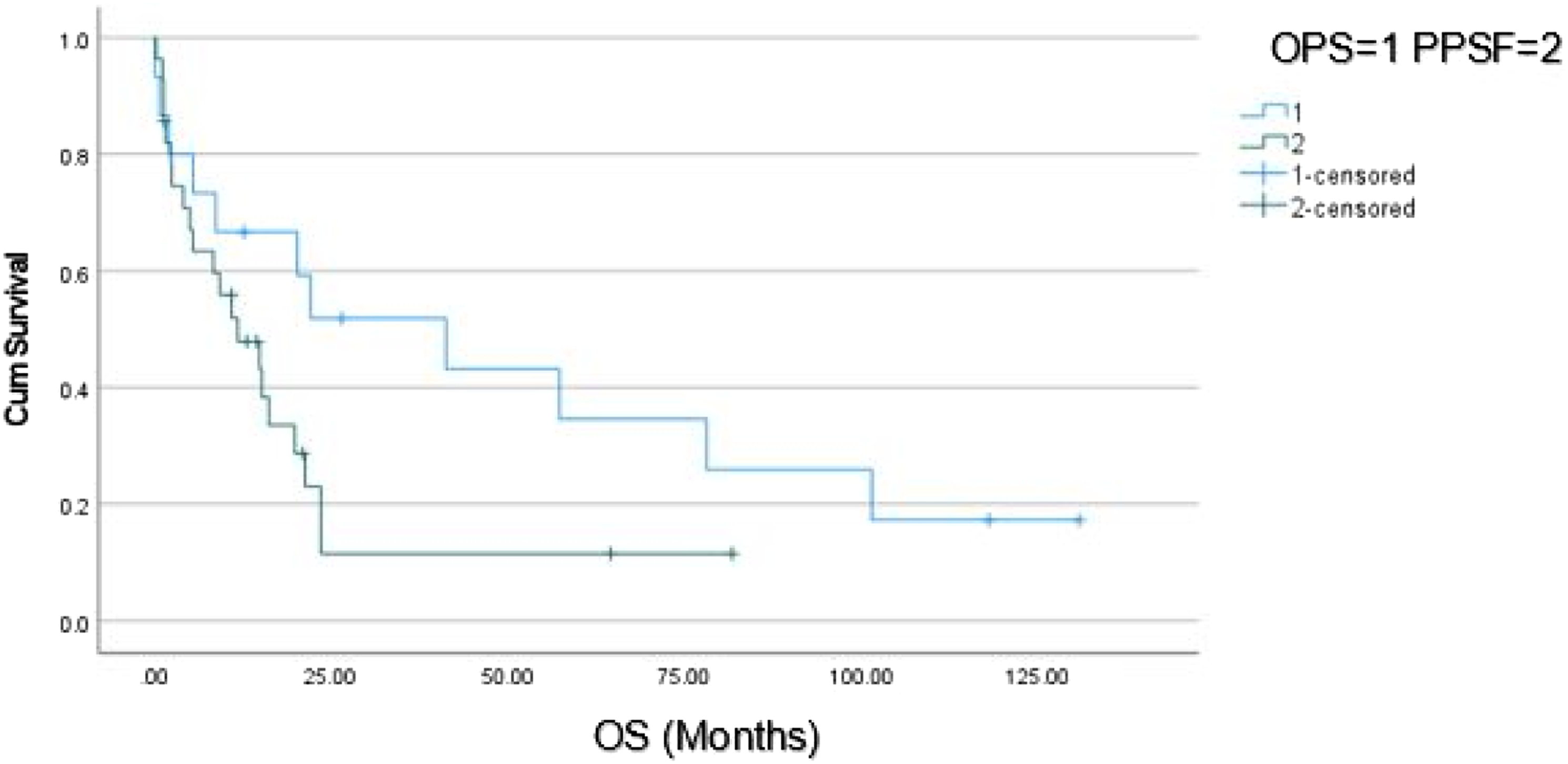
Kaplein–Meier survival curve of PPSF vs OPS. OPS: open posterior stabilization; OS: overall survival; PPSF: percutaneous pedicle screw fixation.
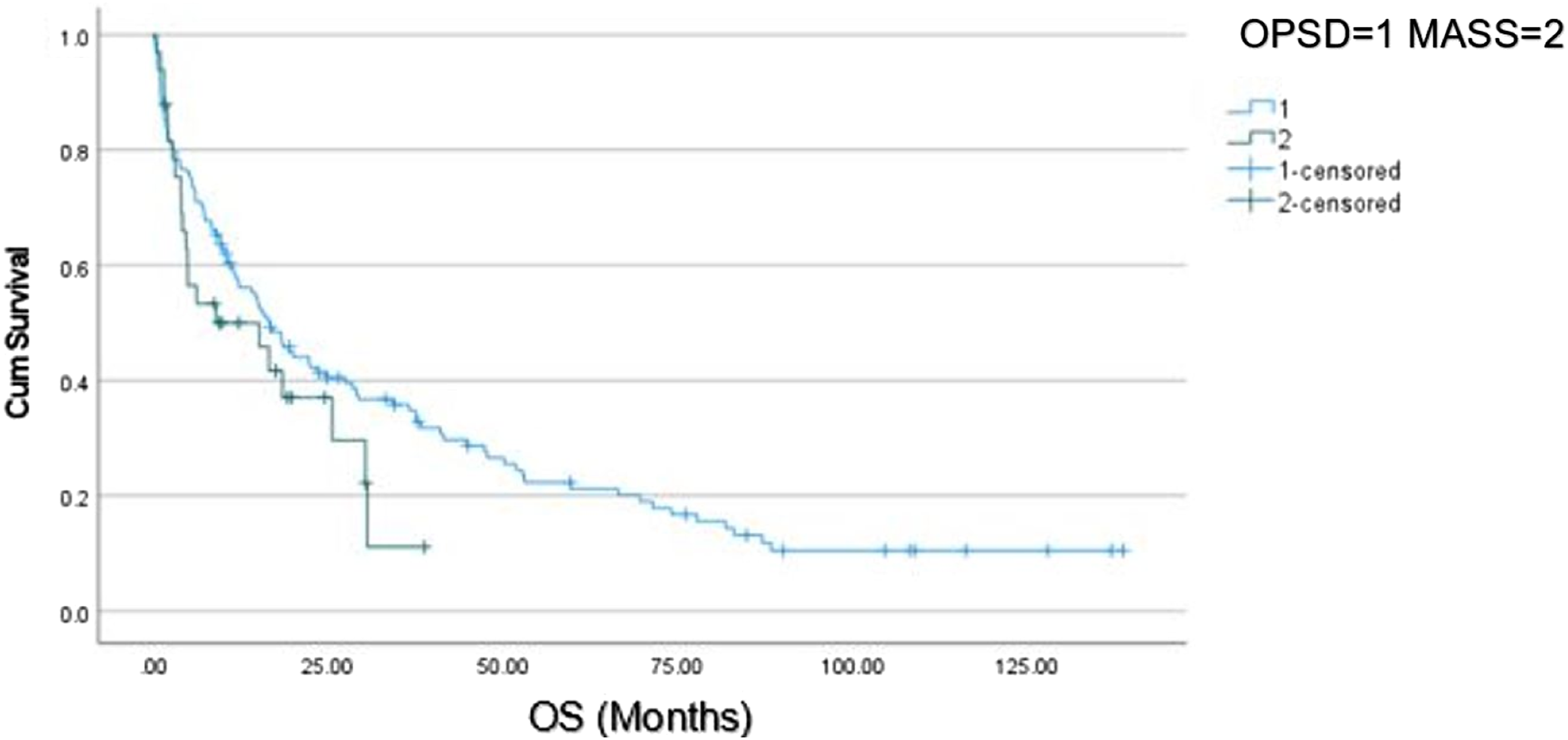
Kaplein–Meier survival curve of MASS vs OPSD. MASS: minimal access separation surgery; OPSD: open posterior stabilization and decompression.
Discussion
Metastatic spine disease patients often have multiple systemic comorbidities and are at an increased risk for complications post-surgery. Complication rates have been reported to range from 10 to 52%. 22 OSS with stabilization and decompression is associated with significant blood loss. In a study by Kumar et al., 8 the estimated mean perioperative blood loss was 870 mL in patients undergoing surgery for MSD. MISS aims to reduce soft tissue dissection, blood loss and approach-related morbidity associated with OSS. In a systematic review by Pennington et al., 23 MISS was found to be associated with a significant reduction in blood loss, length of hospital stay and complication rate when compared to traditional OSS for MSD.
Spinal instability secondary to MSD refers to mechanical pain or neurologic compromise under physiological loads and surgical stabilization is the recommended treatment.6,7 SINS is used to assess tumour-related instability in the vertebral column, and surgical stabilization has been shown to improve patient reported outcomes in cases with unstable or potentially unstable spine as defined by SINS.19,24 PPSF is a versatile surgical procedure for spinal stabilization; it can be used to treat patients with multiple levels of vertebral involvement by the use of long constructs, skip instrumentation and percutaneous iliac screw fixation. 25 The inclusion of decompression and partial corpectomy in MSTS is associated with increased blood loss, operative time and hospital stay. 25 Therefore, there is a need to separately analyse patients undergoing stabilization surgery alone for spinal instability secondary to MSD and patients undergoing separation surgery and spinal stabilization.
To our knowledge, there is a paucity of studies in the literature directly comparing patients undergoing PPSF and OPS. In our study, patients undergoing PPSF had a significantly lower blood loss (95 mL vs 564 mL), surgical complication rate (3.6% vs 26.7%) and shorter length of hospital stay (6 days vs 19 days) with no incidence of worsening neurology. Our estimated surgical blood loss and length of hospital stay with PPSF are comparable to the 100 mL estimated blood loss and 7 days median length of stay reported by Versteeg et al 26 Our surgical site wound dehiscence and infection rate was lower than that reported in a series of 297 surgically treated MSD patients by Sebaaly et al 27 (3.6% vs 5.1%). Furthermore, a trend towards faster initiation of adjuvant radiotherapy was seen in the PPSF subgroup. The advantage of PPSF is its ability to span a longer portion of the spinal column with minimal soft tissue dissection, resulting in reduced blood loss and surgical complications. Our study demonstrates the potential benefits in treating spinal instability with PPSF in MSD.
Numerous approaches have been described to achieve decompression in the setting of MSCC. The anterior transcavitary approach, costotransversectomy and the lateral extracavitary approach have been described to provide direct access to the vertebral body for resection and reconstruction. However, these approaches are associated with significant cardiorespiratory complications which are poorly tolerated in patients with significant comorbidities. ‘Separation surgery’ is an established promising alternative, which is a posterior transpedicular approach and is able to achieve circumferential tumour debulking and decompression in addition to placement of pedicle screws without the approach-related complications associated with anterior or lateral approaches. 17 Anterior column reconstruction is not always a part of separation surgery, and hence. there is a theoretical risk of construct failure or progression of deformity. 28 Amankulor et al. 29 reported a 2.8% rate of implant failure requiring revision surgery in a cohort of 318 patients undergoing separation surgeries for MSD.
Minimal access approaches in all surgical disciplines are associated with a significant decrease in blood loss and postoperative pain leading to a shorter length of hospital stay. In a meta-analysis by Saadeh et al. 30 mini-OSP was associated with a significant decrease in blood loss compared to OSP (805 mL vs 1732 mL) and a significant decrease in postoperative pain scores. Similarly, we reported significantly lower perioperative blood loss (602 mL vs 1008 mL) (P < .001), resulting in a trend towards a shorter length of hospital stay (10 days vs 18 days) (P = .098) when comparing patients treated with MASS vs OPSD. We highlight that due to the wide heterogenicity of our histological tumour subtypes, length of hospital stay in our study was shorter in the MISS group with propensity scoring adjustments approaching statistical significance. We believe with a larger study cohort analysing histological subtypes, this value is likely to be statistically significant. Furthermore, we noted that there were no surgical complications associated with an increased blood loss in the MASS group such as an epidural haematoma requiring re-exploration or excessive postoperative drainage requiring a blood transfusion. Allogeneic blood transfusions are associated with complications such as infections, immune-mediated complications, haemolytic transfusion reactions, transfusion-related acute lung injury and an overall poorer prognosis.31,32 MASS may also be performed with autologous blood transfusion such as the use of intraoperative cell salvage to reduce the dependence on allogeneic blood transfusions and their inherent risks. 32
There was no increased incidence of revision surgery for tumour progression or implant-related complications (loosening/breakage) despite the smaller incision size for the operative procedure in MASS subgroup.33,34 There was also no significant difference in the time to starting chemotherapy agents between the 2 groups. We attribute this to the prevailing oncological practice in our institution for prompt and early initiation of oncological treatments at less than 3 weeks, where applicable. 14
We chose to focus on early clinical outcomes as our primary endpoints as factors such as blood loss and shorter length of stay are tangible outcomes that surgeons can easily address. Outcomes such as local recurrence rate and overall survival are heavily influenced by the primary tumour type, histological and receptor subtype and the tumour load at time of index surgery which is unlikely to be affected by the type or invasiveness of surgery. Additionally, we found no significant difference in survival between patients undergoing MISS and OSS, as the preoperative modified Tokuhashi, ECOG scores and CCI in both the groups were comparable (Table 1). It is well-established that survival in patients undergoing MSTS is primarily influenced by the primary tumour type and the tumour load at the time of index surgery, with the underlying tumours’ sensitivity to chemotherapy/radiotherapy. 12
Conclusion
This study demonstrates the significant benefit of minimally invasive techniques such as PPSF and MASS in decreasing perioperative blood loss over open techniques such as OPS and OPSD. It is one of the first studies to directly compare PPSF vs OPS in treating patients with spinal instability secondary to MSD and show significantly lower blood loss, surgical complication rates and length of hospital stay in favour of the PPSF group. We highlighted a tendency towards reduction in time interval between surgery and initiation of radiotherapy in the MISS group. Our study suggests that MISS is a safe and effective technique both for treatment of spinal instability and MSCC. Awareness of these findings can help oncologists/surgeons individualize treatment approaches, and provide appropriate patient counselling/surveillance, which may in turn improve quality of life and patient outcomes after MSTS, alongside optimizing resource allocation/utilization.
Footnotes
Acknowledgements
We would like to acknowledge A/Prof Joseph Thambiah and Asst. Prof Leok Lim Lau for their contribution of their cases. We also acknowledge Ms Laranya Kumar and Ms Deyvapriya S for data curation and manuscript editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.