
Abstract
Study Design
Retrospective cohort study.
Objective
Physicians may be deterred from operating on elderly patients due to fears of poorer outcomes and complications. We aimed to compare the outcomes of surgical treatment of spinal metastases patients aged ≥70-yrs and <70-yrs
Materials and Methods
This is a retrospective study of patients surgically treated for metastatic epidural spinal cord compression and spinal instability between January-2005 to December-2021. Follow-up was till death or minimum 1-year post-surgery. Outcomes included post-operative neurological status, ambulatory status, medical and surgical complications. Two Sample t-test/Mann Whitney U test were used for numerical variables and Pearson Chi-Squared or Fishers Exact test for categorical variables. Survival was presented with a Kaplan-Meier curve. P < .05 was significant.
Results
We identified 412 patients of which 29 (7.1%) patients were excluded due to loss to follow-up and previous surgical treatment. 79 (20.6%) were ≥70-yrs. Age ≥70-yrs patients had poorer ECOG scores (P = .0017) and Charlson Comorbidity Index (P < .001). No significant difference in modified Tokuhashi score (P = .393) was observed with significantly more ≥ prostate (P < .001) and liver (P = .029) cancer in ≥70-yrs. Improved or maintained normal neurological function (P = .934), independent ambulatory status (P = .171), and survival at 6 months (P = .119) and 12 months (P = .659) was not significantly different between both groups. Medical (P = .528) or surgical (P = .466) complication rates and readmission rates (P = .800) were similar.
Conclusion
≥70-yrs patients have comparable outcomes to <70-yr old patients with no significant increase in complication rates. Age should not be a determining factor in deciding surgical management of spinal metastases.
Introduction
Advances in oncological treatment have resulted in increased life expectancies for cancer patients, 1 this combined with an aging population has led to more elderly patients presenting with spinal metastases. Approximately 10%–20% of cancer patients develop symptomatic spinal metastases. 2 These can present as symptomatic cord compression, pathological fractures, spinal instability and intractable pain. 3
Patchell et al., 4 demonstrated the superiority of surgery followed by radiotherapy in treating patients with metastatic epidural spinal cord compression (MESCC) leading to an increase in surgical treatment of patients with metastatic spine disease (MSD 5 However, the perceived increased risk of complications and decreased benefits of operating on elderly patients may deter surgeons from operating on patients ≥70-yrs. The effect of spinal surgery in elderly patients is controversial. Chen et al, 6 and Yagi et al, 7 reported poorer clinical outcomes in patients ≥70-yrs for cervical myelopathy and spinal deformity respectively. Similarly, Chi et al, 8 in a retrospective analysis of patients participating in Patchell’s 4 RCT found that decompressive surgery was not superior to radiotherapy alone in patients aged ≥70 yrs. In contrast, others have shown that elderly patients treated surgically for spinal metastases had significant improvements in ambulatory, neurological and performance status.9-11
The concern about increased mortality and morbidity in elderly patients may lead to suboptimal surgical treatment. 12 In this study we aim to compare the outcomes of surgical treatment of spinal metastases in patients ≥70-yrs and <70-yrs. We compared the post-operative neurological & ambulatory status, perioperative complication and survival rates between these two groups.
Materials and Methods
Ours is a retrospective study of prospectively collected data of patients who underwent surgical treatment for MSD at a tertiary referral centre between January-2005 to December-2021. Institutional review board (IRB) approval was obtained prior to the commencement of this study namely IRB No: 2020/00495 and 2022/00866 approved by Domain Specific Review Board (DSRB) under the purview of National Healthcare Group (NHG). Both the approvals were waived off informed consent. Data was collected from operating theatre records and hospital electronic medical records by a member of the research team not involved in data analysis and anonymised prior to analysis.
Inclusion criteria comprised of surgical treatment for spinal metastases with metastatic spinal cord compression or spinal instability. Patients <18-yrs, with intradural tumors, primary spinal tumors, previous spine surgery or radiotherapy procedures or who had undergone en-bloc spondylectomy or vertebroplasty/kyphoplasty only were excluded. Patients were operated for spinal instability if the SINS score was 7-18. Patients were followed up till death or minimum 1-year post surgery. Follow up was till death or a minimum 1-year post surgery. Data was collected from operative records and patient electronic medical records.
The cohort was divided into two groups ≥70-yrs and <70-yrs. This stratification was similar to other studies comparing outcomes in patients with advanced and non-advanced age undergoing surgery for spinal metastases.9,11
Demographic data namely age at time of surgery, race, gender, pre-operative ECOG-score and Charlson Comorbidity Index (CCI) were collected. Oncological data included tumour histology, subtype, number of vertebral and skeletal metastases, presence of visceral metastases, Karnofsky Performance scale (KPS) and Frankel score were collected. The Frankel score was categorised into 3 categories, Frankel A+B, Frankel C+D and Frankel E. The modified Tokuhashi score 13 was calculated.
Tumour location was recorded and classified as cervical (C1-C6), cervicothoracic (C7-T2), thoracic (T3-T10), thoracolumbar (T11-L1), lumbar (L2-L4), lumbosacral (L5-S1) and sacral (S2-S5). This location was allocated based on the most symptomatic level in patients with polymetastatic disease. Type of surgery was classified into stabilisation only, posterior decompression & stabilisation, separation surgery, partial and complete corpectomy. Stabilisation is defined as posterior instrumentation with no decompression. Posterior decompression and stabilisation are defined as posterior instrumentation and laminectomy with no circumferential decompression. Separation surgery was performed as described by Laufer et al, 11 and popularised by Kumar et al 14 in our region, namely a laminectomy followed by anterior decompression via a transpedicular approach for circumferential tumour decompression, with no anterior reconstruction. Partial corpectomy was described as piecemeal intralesional excision of up to 50% of vertebral body with or without anterior reconstruction and corpectomy was piecemeal intralesional excision of ≥50% to ≤90% followed by anterior reconstruction
Surgical approach was classified into posterior, anterior and combined. The surgical technique of instrumentation was recorded as open, minimally invasive where pedicle screws were placed percutaneously and hybrid where both minimally invasive and open techniques were used. Anterior cervical procedures were classified as open procedures. The number of levels decompressed and instrumented was also recorded. Intra-operative blood loss, amount of blood transfused and type of transfusion were recorded. Duration of hospital stay with HD/SICU stay, post-operative neurological outcome and ambulatory status were recorded. We defined a complication as ≥ Grade 2 as per Zaw et al, 15 classification. Complications were divided into medical or surgical. Complications occurring up to 1-month post-discharge requiring readmission were recorded.
Finally, length of survival, which was defined as time from surgery to demise was recorded. In patients lost to follow-up, we recorded time from surgery to last follow-up. We recorded 1, 3, 6 and 12-month survival in both groups. The actual survival of each patient was then compared to predicted survival by the modified Tokuhashi score. We recorded how actual survival compared to prognosticated survival.
Statistical Analysis
SPSS Version 28 was used. Two Sample t-test/Mann Whitney U test were used to compare the differences for numerical variables between the two groups. Pearson Chi-Squared or Fishers Exact test were used for categorical variables. Overall survival between the two groups was presented with a Kaplan-Meier analysis. P value <.05 was taken to be significant.
Results
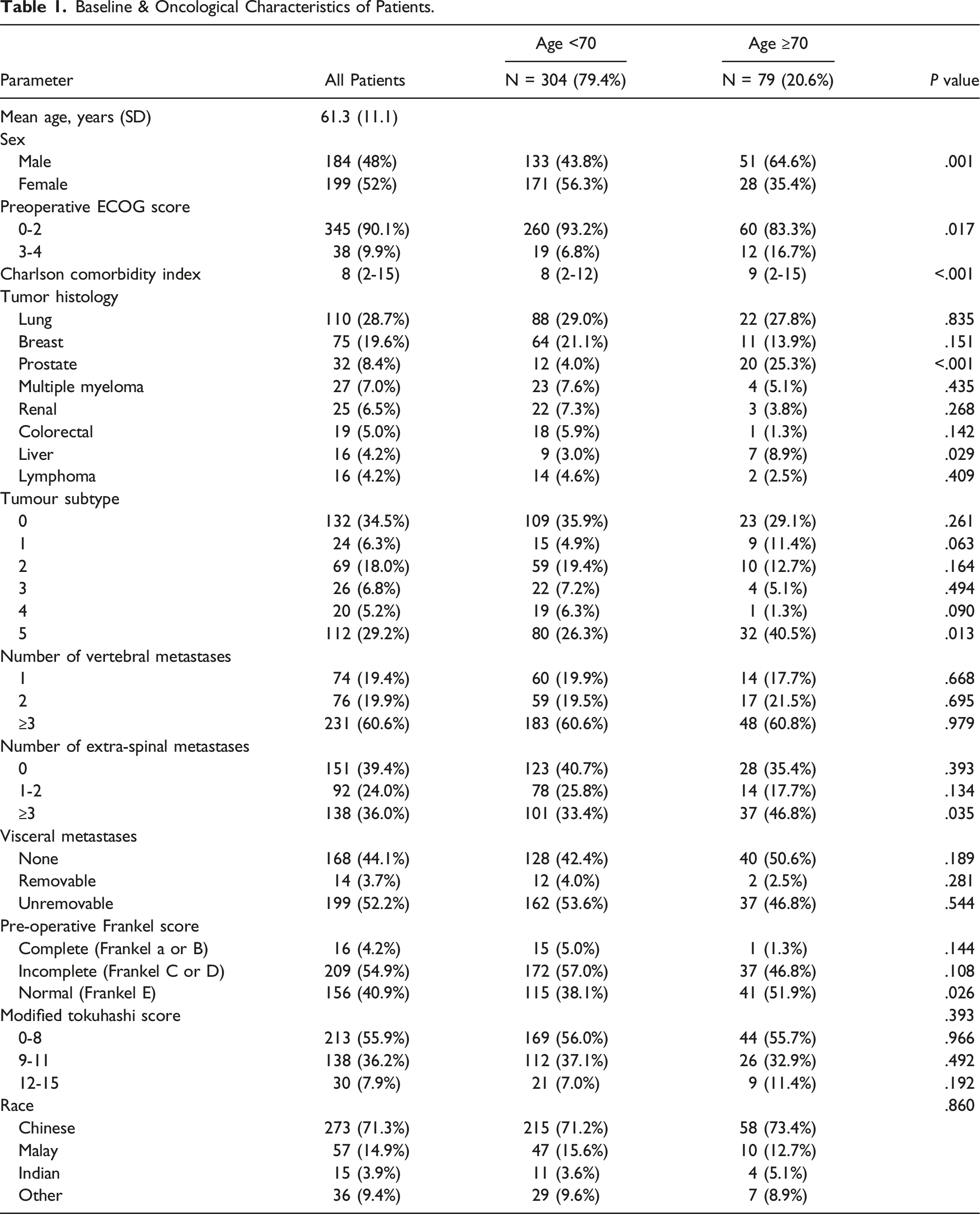
Baseline & Oncological Characteristics of Patients.
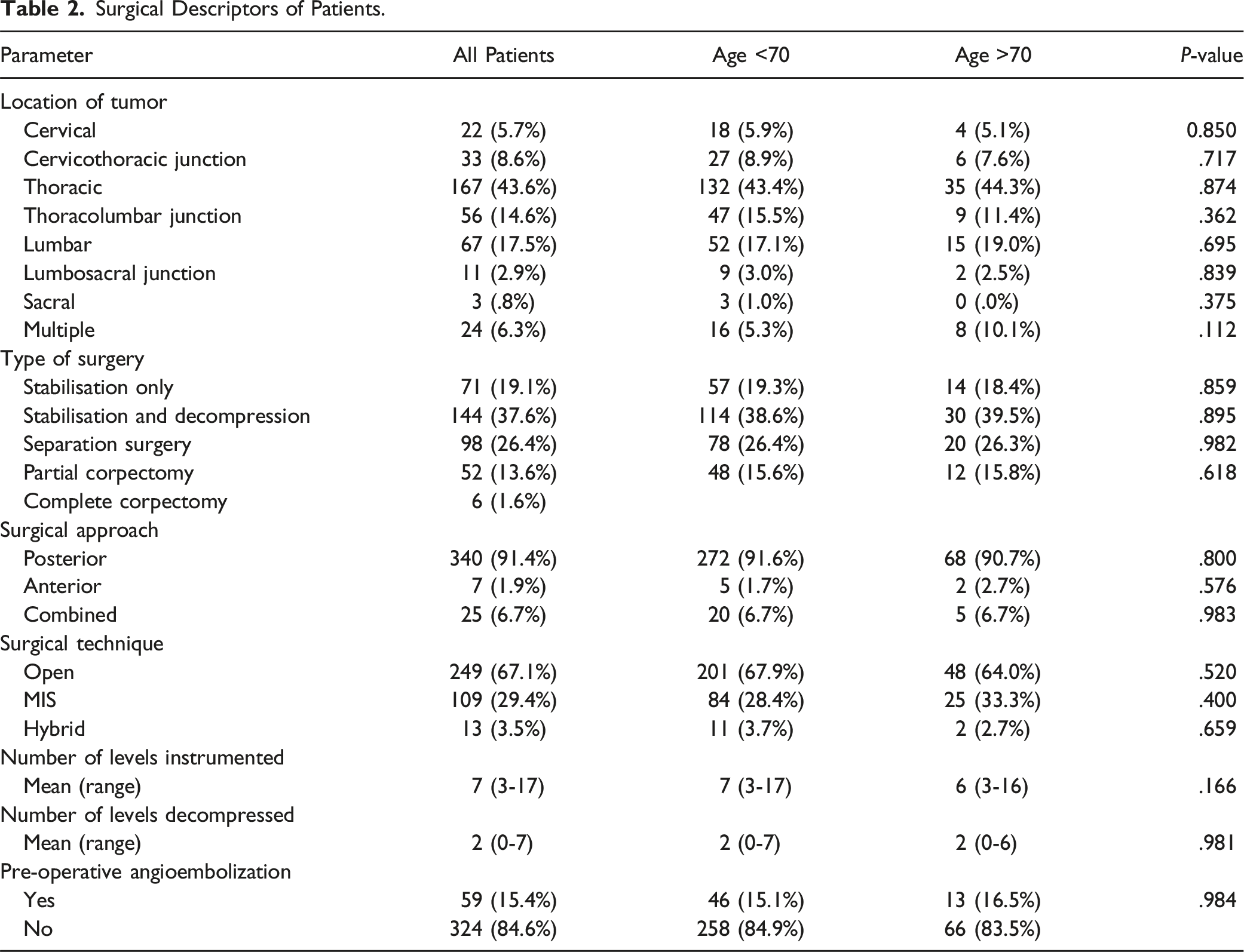
Surgical Descriptors of Patients.
Surgical and Clinical Outcomes.
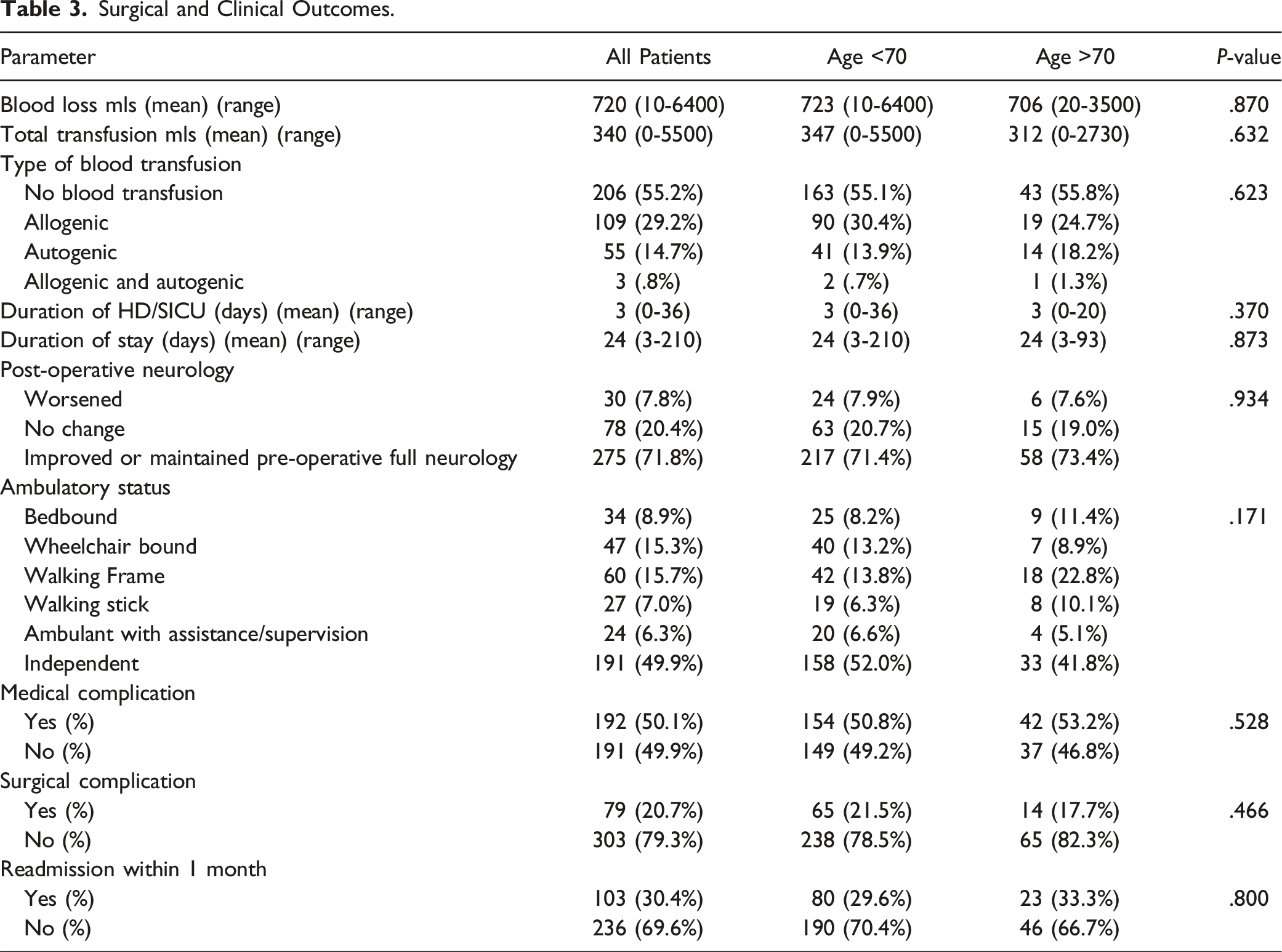
The results on neurological evaluation revealed that in patients ≥70-yrs, 58/79 (73.4%) patients had improved or maintained pre-operative normal neurological function, 15/79 (19.0%) had no change and 6/79 (7.6%) had worsening of their post-operative neurological function. Patients aged <70-yrs were more likely to ambulate independently (52.0% vs 41.8%), although this was not statistically significant. For <70-yrs, 239/304 (78.6%) patients were able to walk with a walking aid or with assistance or independently as against 63/79 (79.7%) patients for ≥70-yrs in Table 3. This difference was not significant. In ≥70-yrs patients who were Frankel (C+D)14/37 (37.8%) remained Frankel (C+D) and 22/37 (59.7%) improved to Frankel-E. In patients ≥70-yrs who were Frankel-E 39/41 (95.1%) patients remained Frankel-E and only 2/41 (4.9%) patients became Frankel (C+D) post-surgery (Figure 1). This was similar to <70-yrs patients. However, patients aged <70-yrs who were Frankel (A+B) pre-operatively were more likely to experience neurological recovery and improve to Frankel B 8/15 (53.3%) of patients. There was only one patient who was Frankel (A+B) in the ≥70-yrs group, and this patient did not improve. Pre-operative and Post-operative Frankel Scores for both groups.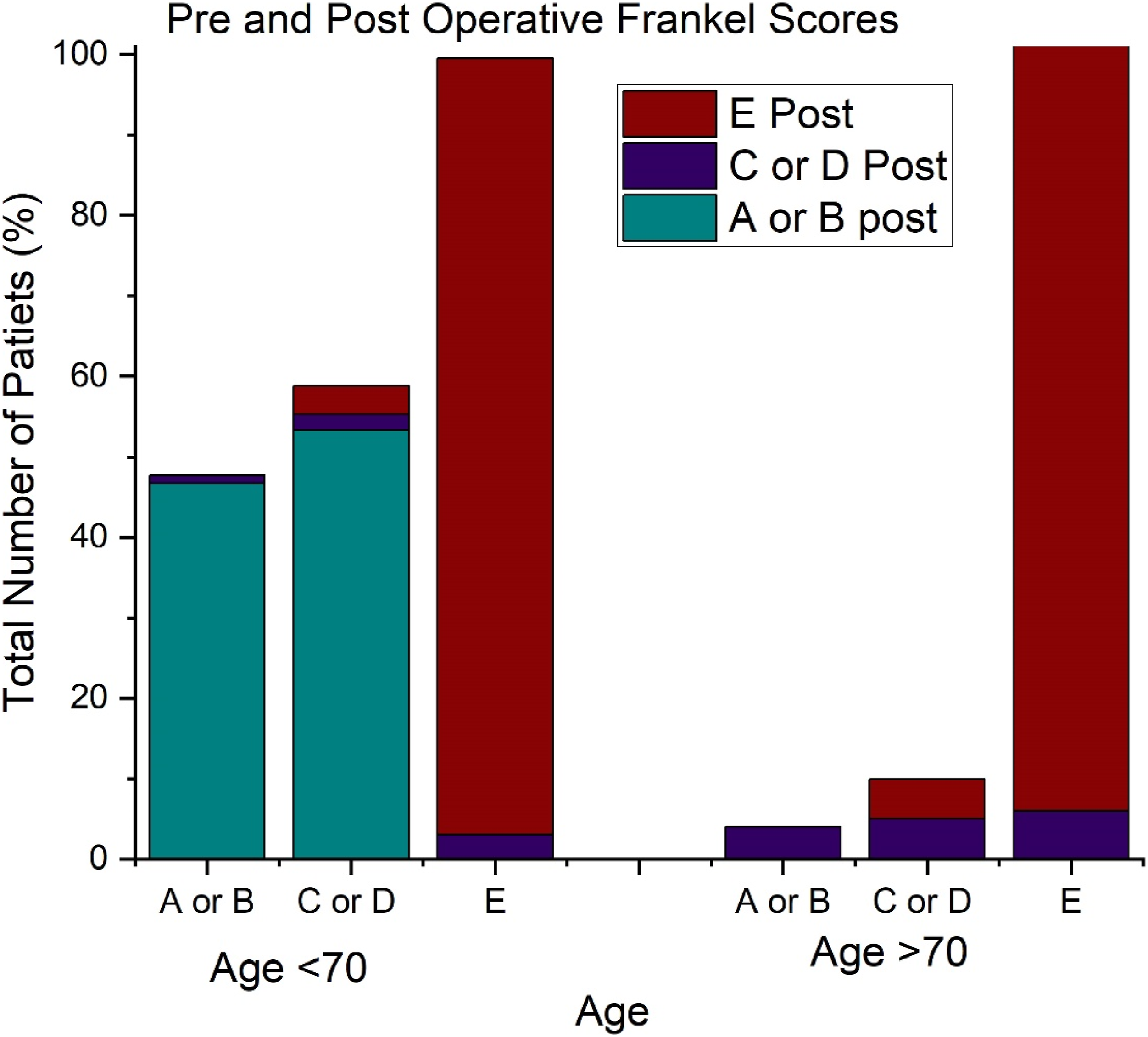
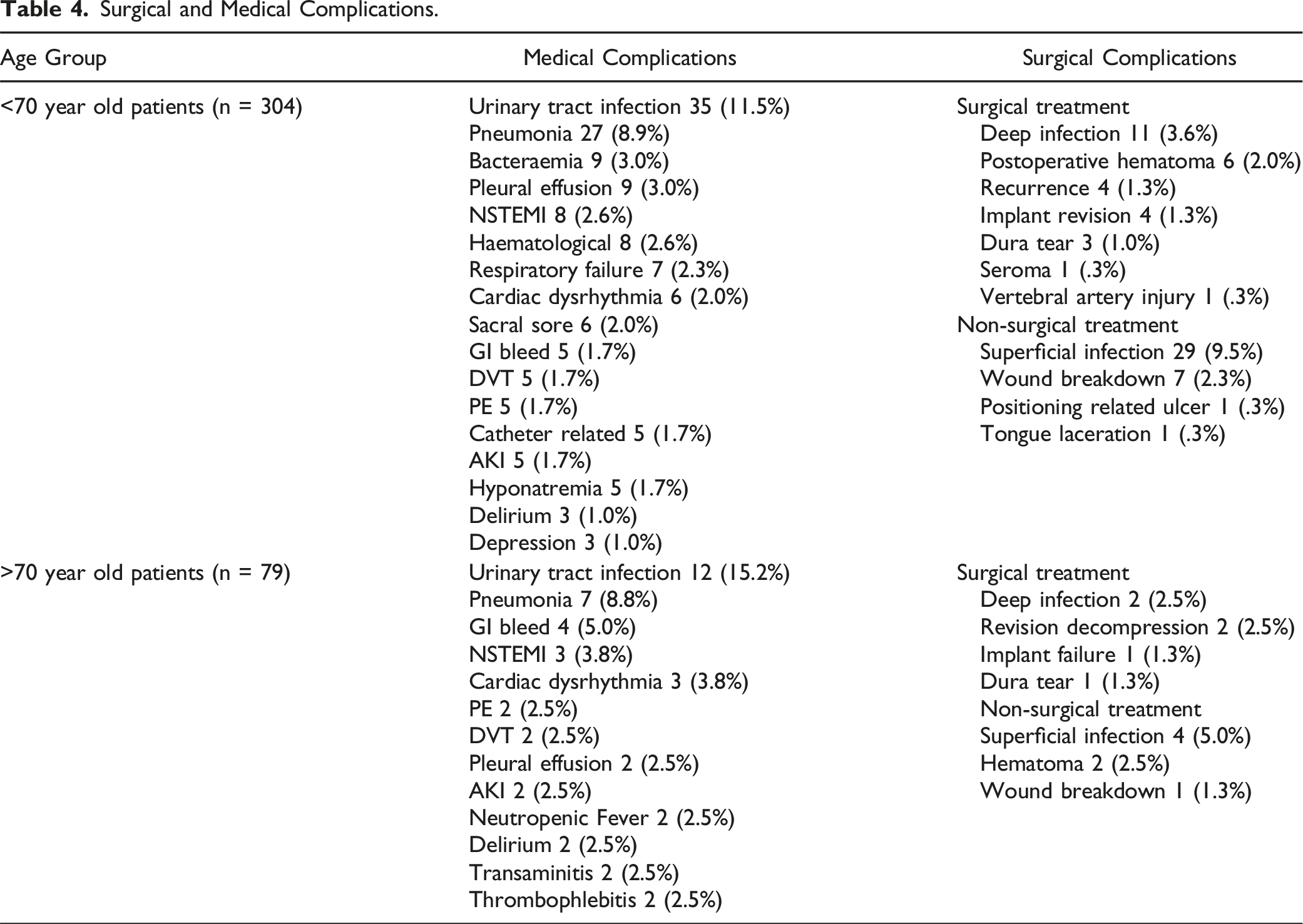
Surgical and Medical Complications.
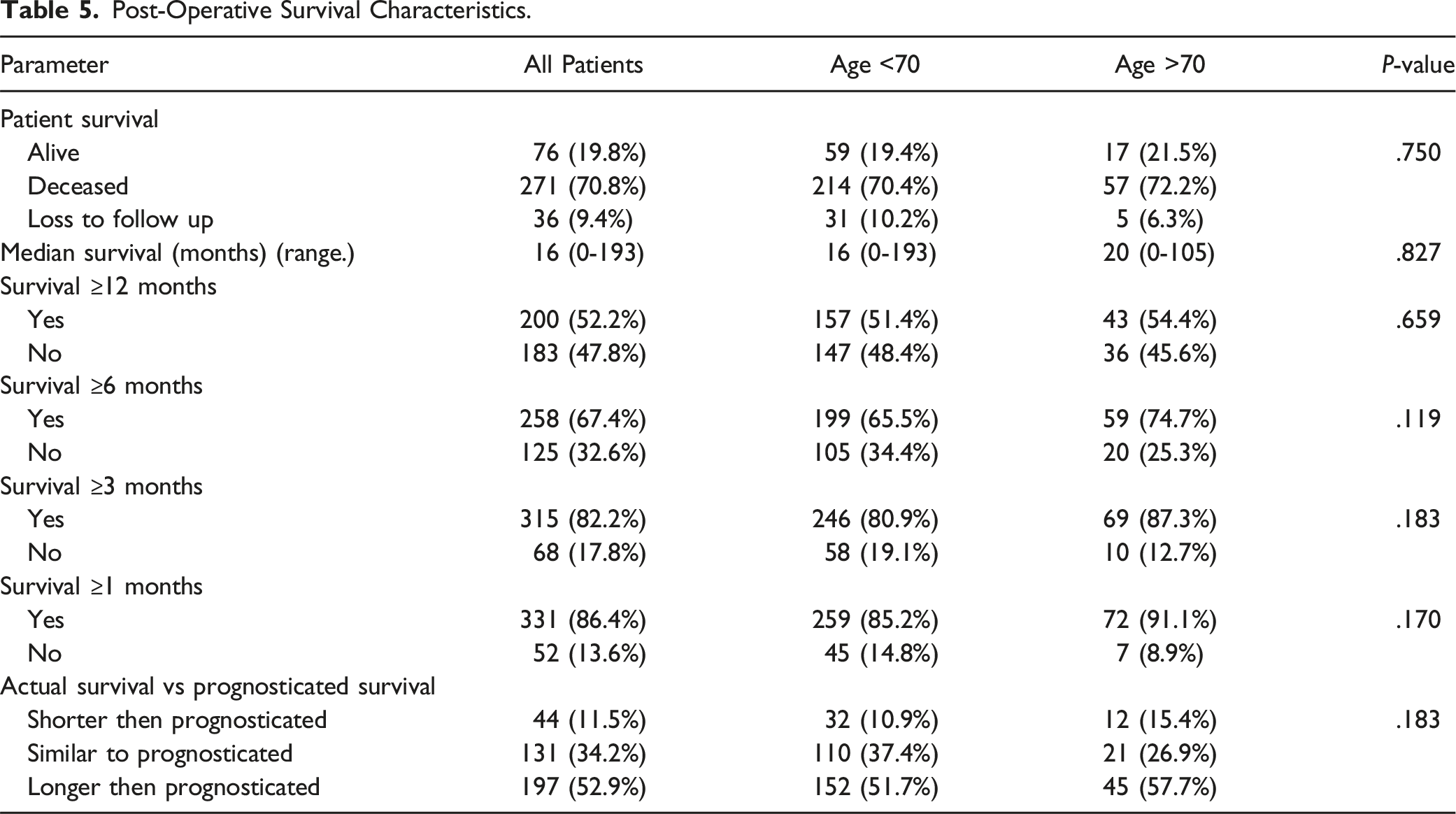
Analysis of the survival indicated that the ≥70-yrs group had a trend to increased survival at 1, 3, 6 and 12-mths with a higher median survival (20 vs 16-mths, see Figure 2). However, this was not statistically significant. On the Kaplan Meier curve there was no significant difference in survival between both groups. The modified Tokuhashi score accurately prognosticated survival in only 110 (37.4%) of the <70-yrs patients and 21 (26.9%) of the ≥70-yrs patients. It tended to underestimate survival with 152 (51.7%) of the <70 patients and 45 (57.7%) of the ≥70-yrs patients outliving their prognosis in Table 5. Kaplan Meier Curves for survival estimates for both groups. Post-Operative Survival Characteristics.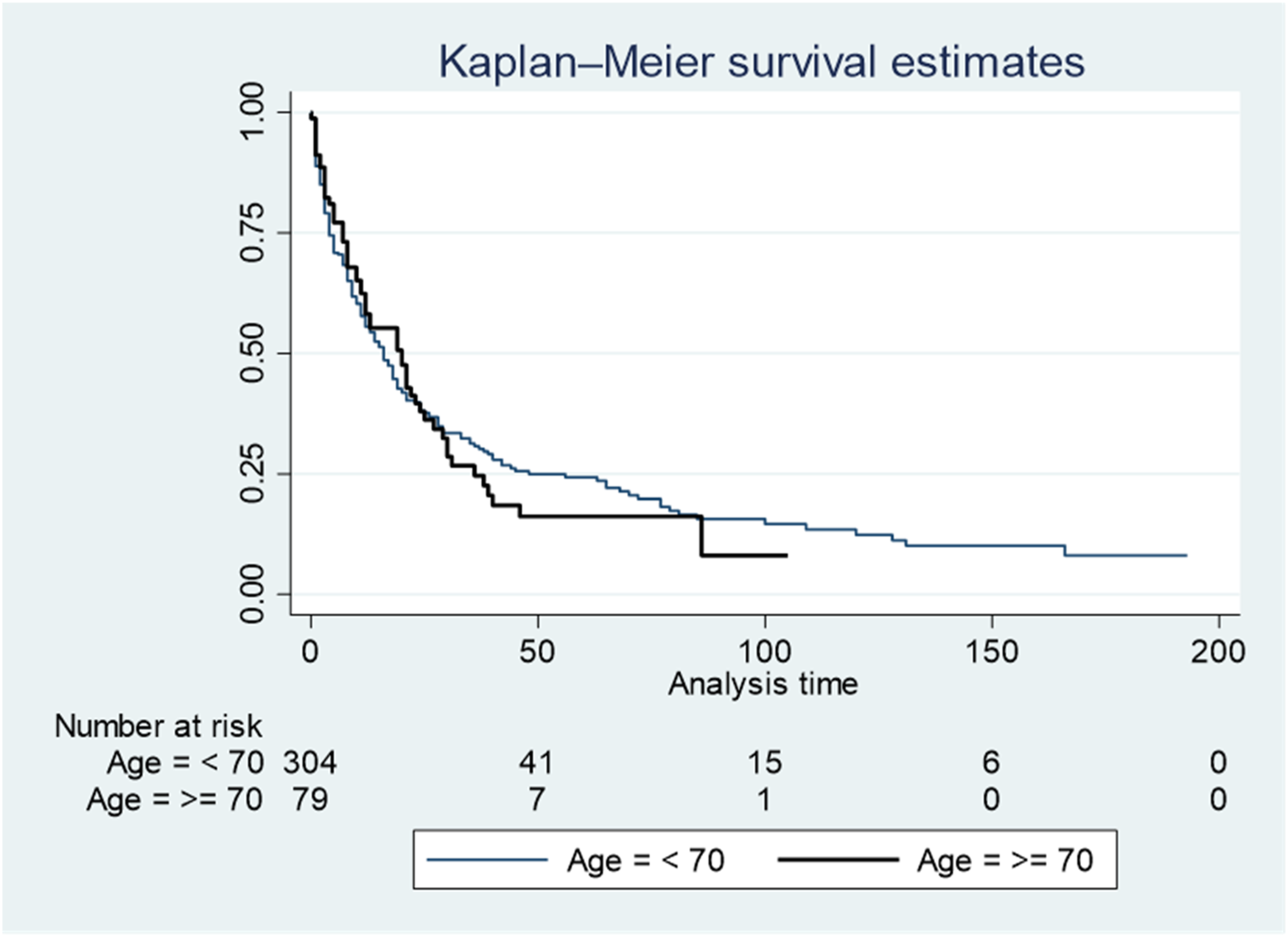
Discussion
Our study analysed a total of 412 patients of which 383 were finally included, where patients aged ≥70-yr comprised roughly one fifth of the cohort. Our study showed no significant difference in neurological outcome, ambulatory status, post-operative complication rate and post-operative length of survival between patients aged <70-yrs and ≥70-yrs. To our knowledge, the largest study comparing outcomes in elderly patients of different age groups undergoing surgery for symptomatic MESCC is by Amelot et al. 9 In a multicentre study of 1266 patients, patients were divided into groups of <70-yrs, 70-80-yrs, and >80-yrs, and improvements in Frankel score were seen in all groups of patients, although younger patients tended to have greater improvements post-operatively.
In our study there was no significant difference in improvement of neurological status post operatively with 73.4% of our ≥70-yrs patients improving neurologically or maintaining normal neurological status compared to 71.4% of the <70-yrs patients. However, in our study there was a significantly higher number of ≥70-yrs patients (51.9% vs 38.1%) (P = .026) presenting with Frankel-E normal neurological status, which was in contrast to Amelot et al, 9 who found that older patients tended to present with worse neurological status. In our study the Frankel-E patients were mostly treated for spinal instability rather than MESCC. Nevertheless, when comparing pre-operative to post-operative Frankel scores, 95.1% of Frankel-E patients remained Frankel-E in the ≥70-yrs group as compared to 96.5% in the <70-yrs group. Furthermore, 59.5% of the pre-operative Frankel (C+D) patients in the ≥70-yrs group improved to Frankel-E compared to 58.7% in the <70-yrs group. It was not possible to compare outcomes in patients who were Frankel (A+B) as there was only one ≥70-yrs, who presented with this Frankel score.
There was a trend to increased survival in ≥70-yrs group at 1, 3, 6 and 12-mths. In contrast, Amelot et al 9 found survival expectancy to be significantly longer in patients <70-yrs (P = .02). This was despite the significantly worse ECOG (3-4) scores and CCI scores in the ≥70-yrs group. de Andrade et al 16 found that preoperative function in terms of the Karnofsky performance score and ECOG score were significant predictors of survival and in a meta-analysis by Luksanapruksa et al, 17 an ECOG score of 3-4 was found to be a significant independent predictor of patient survival, while in a retrospective cohort study of 1613 patients by Elsamadicy et al, 18 the CCI was found to be an independent predictor of adverse events. The increased survival in our ≥70-yrs group may be due to a significant difference in tumor histology with a significantly increased number of patients with prostate cancer (P < .001) or slow-growing Modified Tokuhashi subtype-5 tumours. Tumour histology has been shown to be the most important independent factor in predicting survival13,19 and the slow progression of the underlying primary disease may have led to increased survival in the ≥70-yrs group.
Surgery has been shown to improve neurological outcome in the postoperative period by de Andrade 20 and Patchell et al, 4 but it’s effectiveness in older patients is still unclear. In our study ≥70-yrs had a comparable improvement in ambulatory status and survival to <70-yrs. This is in contrast to the study by Chi et al, 8 who showed there was no difference in ambulatory status between patients ≥65-yrs treated with surgery and radiation vs radiation alone. Our findings were similar to that of Itshayek et al, 10 who found that in a series of 40 patients aged ≥65-yrs, there was a significant improvement in ambulatory status and 43% (17/40) patients retained their ability to ambulate for ≥1 year. In a prospective study by Kanda et al, 11 of 65 patients aged <70-yrs and 36 patients aged ≥70-yrs there was a significant improvement in performance status, activities of daily living, and quality of life, regardless of age.
Focusing on the peri-operative complications, we noted that patients ≥70-yrs had a higher incidence of medical complications (53.2% vs 50.8%) (P = .538) and a comparatively lower rate of surgical complications (17.7% vs 21.5%) (P = .466) when compared to the <70-yrs. Amelot et al, 9 reported a significant association between increased age and increased complication rate; perioperative complication rate was 33.3% in patients >80 yrs, 23.9% in 70-80 yrs, and 17.9% for <70 yrs (P = .004). One possible reason for the high complication rate in our study is the high CCI with median of 8 (range 2-15). This index has been found to be a robust predictor of 30-day perioperative complications, 21 patients with a CCI score of ≥2 had over five times the odds of a 30-day complication compared to patients with score = 0-1. In our study the most common medical complications were UTIs and HAP, which occurred in 12.3% and 8.9% of patients respectively. The most common surgical complications were wound related with 13 (3.4%) patients requiring reoperation for deep infections and 33 (8.6%) requiring antibiotic treatment for superficial wound infections. Luksanapruksa et al, 22 found that the most common surgical-related complications were wound dehiscence/infections (10.2%), hematomas (2.29%), and hardware problems (1.52%). The most common medical complications were delirium (11.2%), pneumonia (3.98%), and DVT (2.36%).
There was an unplanned hospital readmission rate of 30.4%, and patients ≥70-yrs were found to have a non-significantly higher rate of unplanned readmission within 1-mth (33.3%vs29.6%). In a previous study of unplanned readmissions in patients post spinal metastases surgery from our centre, Kumar et al,23,24 found that ECOG >1 (P = .057) and CCI >7 (P = .01) were significant risk factors for unplanned readmission. This may explain the higher rate of readmission in our older patients who had higher ECOG and CCI scores.
It is important to note the tendency of the modified Tokuhashi score to under-predict survival as it does not consider recent advances in oncological treatment or specific tumour subtypes25,26 and in a review by Zoccali et al, 27 it had a predictive accuracy of 63%. In our study, its under-predicted survival in 57.7% of the patients ≥70-yrs. Using the modified Tokuhashi Score as a criterion for surgical decision making may lead to patients being incorrectly precluded from undergoing surgery due to an inaccurate survival prognosis. 28
Our data suggests that patients ≥70-yrs have a more unpredictable postoperative course with a significant complication and readmission rate. This should be anticipated and communicated to the patient prior to surgery, and patients should understand their increased risk of perioperative complications and early readmission after discharge. However, this should not preclude elderly patients from being offered surgery as 79.7% of ≥70-yrs were able to ambulate post-surgery with no significant decrease in survival. In this study, the median postoperative survival in ≥70-yrs was 20 (0-105) months which was comparable to the median postoperative survival of 11.2 months reported by Kanda et al, 11 and 13.9 months reported by Amelot et al 9
Patient pre-morbid functional status as well as tumor histology have been found to be the most important predictors of survival and this should be considered rather than chronological age.16,29 A multidisciplinary approach with oncologist and geriatrician input is vital in elderly patients with MSD to improve prognostication and medical management.
Limitations
Limitations of our study include the retrospective nature of the study with variations in surgical and medical treatment over time and with different treating surgeons. Secondly, it was not possible to collect a matched cohort of patients with similar demographic and oncological profiles. Thirdly, we did not collect the preoperative and postoperative oncological treatment, which was outside the scope of this study, but likely to play an important role in determining patient survival. Fourthly, further stratification of the >70 group to patients aged 70-80 years and >80 years would have been beneficial in view of the increasing life expectancy of the population; however, this was not possible due to the small number of >80 patients, 13 (3.4%) patients. Finally patient reported outcomes and quality of life scores are not reported as this data was not routinely recorded in the first half of the study, and this is a limitation of our study. However, we believe that our findings in terms of neurological outcomes and ambulatory outcomes are also relevant outcomes to report post-operatively.
Conclusion
In summary, patients ≥70-yrs have comparable improvement in neurological status, ambulatory status and survival compared to younger patients. Therefore, age should not be a contraindication to spinal surgery in elderly patients with spinal metastases. However, surgery for spinal metastases in patients ≥70-yrs is associated with higher complication rates, which must be communicated to the patient and addressed by a dedicated multidisciplinary approach to ensure optimal outcomes in elderly patients.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Hui Si Jian, Mr. Sahil Athia, Ms. Laranya Kumar for their help in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.