
Abstract
Study Design:
This was an ambispective clinical quality registry study.
Objective:
To evaluate utility of 11-variable modified Frailty Index (mFI) in predicting postoperative outcomes among patients ≥80 years undergoing spinal surgery.
Methods:
Consecutive patients ≥80 years who underwent spinal surgery between January 1, 2013, and June 30, 2018, were included. Primary outcome measure was rate of major complication. Secondary outcome measures were (1) overall complication rate, (2) surgical site infection, and (3) 6-month mortality.
Results:
A total of 121 operations were performed. Demographic metrics were (1) age (mean ± SD) = 83.1 ± 2.8 years and (2) mFI (mean ± SD) = 2.1 ± 1.4 variables. As mFI increased from 0 to ≥4 variables, risk of major complication increased from 18.2% to 40.0% (P = .014); overall complication increased from 45.5% to 70.0% (P = .032); surgical site infection increased from 0.0% to 25.0% (P = .007). There were no significant changes in risk of 6-month mortality across mFIs (P = .115). Multivariate analysis showed that a higher mFI score of ≥3 variables was associated with a significantly higher risk of (1) major complication (P = .025); (2) overall complication (P = .015); (3) surgical site infection (P = .007); and (4) mortality (P = .044).
Conclusions:
mFI scores of ≥3/11 variables were associated with a higher risk of postoperative morbidity in patients aged ≥80 years undergoing spinal surgery. The mFI-associated risk stratification provides a valuable adjunct in surgical decision making for this rapidly growing subpopulation of patients.
Keywords
Introduction
Frailty is a universal risk factor for recurrent falls, delirium, institutionalization, and poor postoperative outcome. 1 It is estimated to affect 7% to 11% of individuals older than 65 years, and 25% to 40% of individuals aged 80 years or older. 1
Numerous criteria, including the Fried Frailty Index and the Rockwood Frailty Index, have attempted to classify frailty. 1,2 More recently, the Canadian Study of Health and Aging Frailty Index (CSHA-FI) validated 70 variables as markers of frailty. 3 This has been further refined to form the Modified Frailty Index (mFI), which comprises 11 variables. An individual’s mFI is denoted as n/11, wherein n is the number of the 11 variables satisfied. 3
Various frailty indices have been previously validated as predictors of postoperative complication rates. 4 Farhat et al 5 examined a cohort of 35 334 patients undergoing general surgery and found that an increase in the 11-variable mFI from 0 to 8 variables (0 to 0.73) was associated with a rise in 30-day mortality rate from 3.6% to 51%. The wound infection rate also increased from 9.0% to 12.1% when the mFI rose from 0 to 3 variables (0 to 0.27) in the same cohort of patients. 5 The mFI has also been effective in predicting 30-day mortality and morbidity in patients undergoing spinal surgery, 5 -9 although not in patients aged 80 years or older.
The United Nations defines people aged 60 years and older as older people, and people aged 80 years and older are further classified as the oldest-old population. 10 Frailty is becoming increasingly relevant given that global life expectancy is projected to rise from 71 years in 2010-2015 to 77 years in 2045-2050, and the population aged 80 years or greater in 2017 (137 million) is projected to triple to 425 million in 2050, before further expanding to 909 million in 2100. 10 Consistent with this, there is an increasing number of patients aged 80 years and older who are being considered for, or undergoing, elective or emergency surgery. 11 -14 Although many studies have associated this with increased rates of morbidity and mortality, 15,16 others have demonstrated low complication rates with appropriate patient selection. 17 Therefore, it is timely to validate an accurate tool to assist with preoperative risk stratification in patients 80 years and older who are being considered for surgery. This article aimed to evaluate the utility of the 11-variable modified Frailty Index (mFI) in predicting postoperative outcomes among patients 80 years and older undergoing spinal surgery.
Materials and Methods
Study Design
The Alfred Hospital is a tertiary spine referral center and a state-service level 1 trauma center. The Alfred Hospital Spine Service is a combined neurosurgery and orthopaedic service. The Alfred Hospital has established clinical quality trauma registry and department surgical databases, which contain minimal data sets on patient demographic, details of the diagnosis, the surgery received, and postoperative complications. With approval from the institutional Human Research Ethics Committee, we conducted an ambispective review of consecutive patients, aged 80 years and older, who underwent elective or emergency spinal surgery from January 2013 to June 2018 (inclusive). Medical records of patients who satisfied the inclusion criteria were assessed retrospectively to collect data on body mass index (BMI), smoking status, albumin level, preoperative residence, discharge destination, length of surgery, requirement for blood transfusion, American Society of Anesthesiologists (ASA) classification 18 , and mFI. Primary outcome measures, including complications during hospital admission, surgical site infection, mortality within 6 months, and readmission within 30 days, were recorded. Other outcome measures consist of length of surgery, requirement for blood transfusion, discharge destination, and readmission within 30 days.
Modified Frailty Index
The mFI consists of 11 variables, including the following: (1) nonindependent functional status; (2) history of diabetes mellitus; (3) history of chronic obstructive pulmonary disease; (4) history of congestive cardiac failure; (5) history of myocardial infarction; (6) history of percutaneous coronary intervention, cardiac surgery, or angina; (7) history of hypertension requiring medication; (8) history of peripheral vascular disease; (9) history of impaired sensorium; (10) history of transient ischemic attack or cerebrovascular accident without deficit; and (11) cerebrovascular accident with deficit. 3,4 The mFI score was calculated as n/11 (where n is the positive number of the 11 variables identified).
Clavien-Dindo Complication Classification
The Clavien-Dindo complication system classifies adverse events during the postoperative course into 5 categories: (1) Class 1 represents any deviation from the normal postoperative course without the need for pharmacological, surgical, endoscopic, or radiological interventions; (2) class 2 complications require pharmacological treatment; (3) class 3 complications encompass those requiring surgical, endoscopic, or radiological intervention; (4) class 4 incorporates life-threatening complications of single or multiorgan failure requiring intensive care unit management; and (5) class 5 constitutes patient death. 19 Major complication is defined as a Clavien-Dindo score of 3 or greater. 20
Statistical Analysis
Univariate and bivariate descriptive and inferential statistical methods were used to investigate demographics, ASA score, surgical metrics, complications, and outcomes between the mFI cohorts. The Fisher exact test was used to analyze univariate categorical data. The sample size was determined to be adequate for the number of predictive variables utilized in the multivariate models using previously described methods. 21 Binary logistic regression analysis was performed for identification of independent predictors of adverse surgical outcomes. Best-fit models were constructed with the dependent variables being as follows: (1) major complications (Clavien-Dindo Classification ≥3), (2) all complications, (3) surgical site infection, and (4) mortality. Selection of baseline covariates as independent variables in the model was based on the univariate P value (<.20). The backward elimination method was utilized in the creation of models. Goodness-of-fit analysis was conducted using the Hosmer-Lemeshow Test and Omnibus Test of Model Coefficients.
Sensitivity analysis of mFI was conducted by evaluating the correlation of a graduated increase in mFI from ≥1 variable (≥0.09) to ≥5 variables (≥0.45) in predicting (1) major complications; (2) all complications; (3) surgical site infections, and (4) mortality. The association between graduated increases in ASA score and complications was also analyzed. Statistical significance was defined as a P value of less than .05. All statistical analyses were performed using STATA/IC version 14.2 (StataCorp, College Station, TX).
Results
Demographics
From January 2016 to June 2018, there were 115 patients who underwent 121 cases of spinal surgery (Table 1). The mean (±SD) age was 83.1 years (±2.8), with the oldest patient being 93 years. More than half (59.5%, n = 72) of the surgeries were performed in male patients. The mean mFI was 2.1 (±1.4) out of the 11 variables (mFI scores of 0.19 ± 0.13), whereas the median was 2 out of the 11 variables (0.18). The mean ASA grade was 2.9 (±0.6).
Preoperative Patient Demographics.
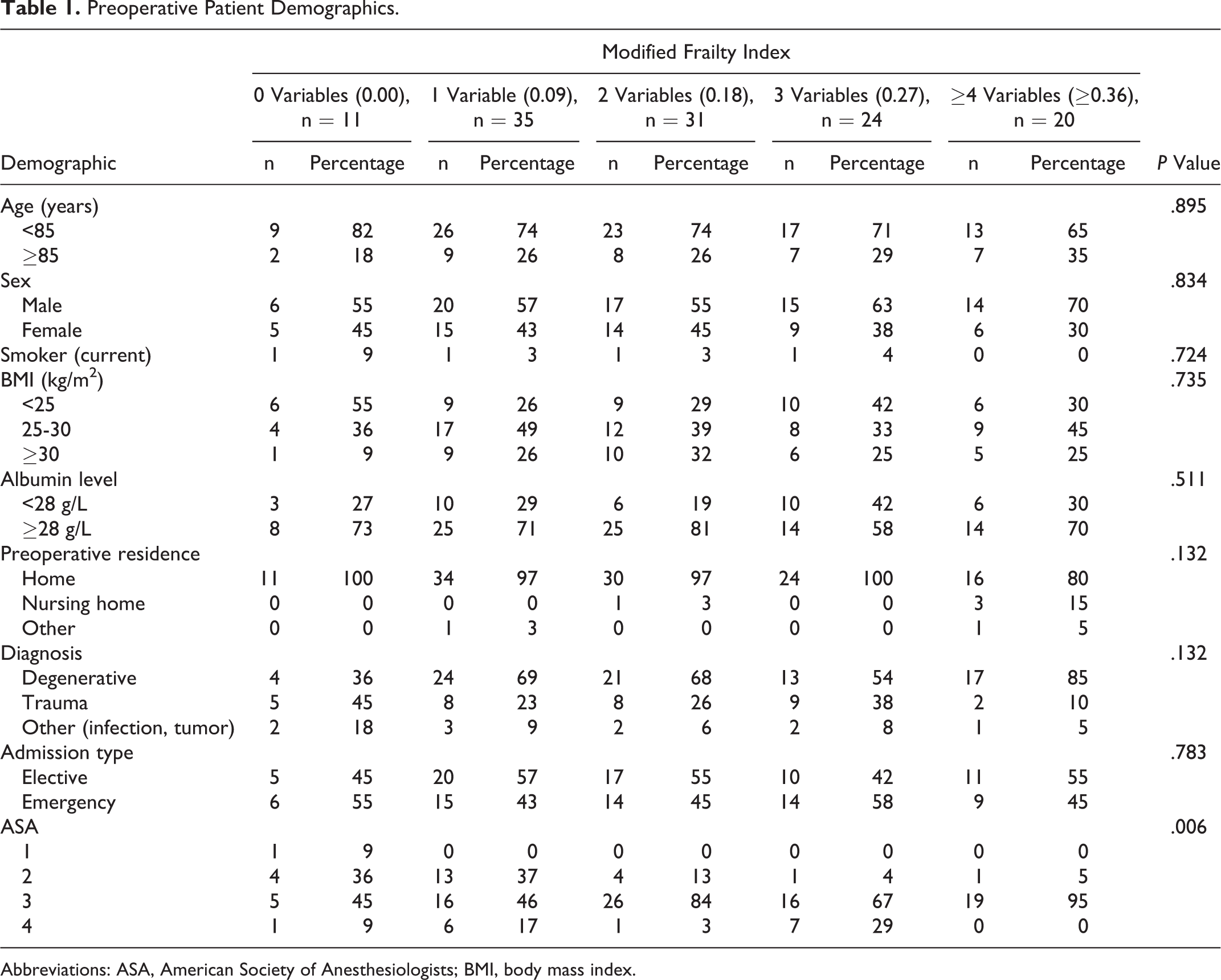
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
A total of 11 (9.1%) patients had a mFI of 0 variables, 35 (28.9%) had a mFI of 1 variable (0.09), 31 (25.6%) had a mFI of 2 variables (0.18), 24 (19.8%) had a mFI of 3 variables (0.27), and 20 (16.5%) had a mFI of ≥4 variables (≥0.36). There was no statistically significant difference across mFIs with respect to age, sex, smoking status, BMI, albumin level, preoperative residence, diagnosis type, or admission type. Those patients with higher mFI scores registered higher ASA scores (P = .006) than their less frail counterparts.
Surgical Metrics
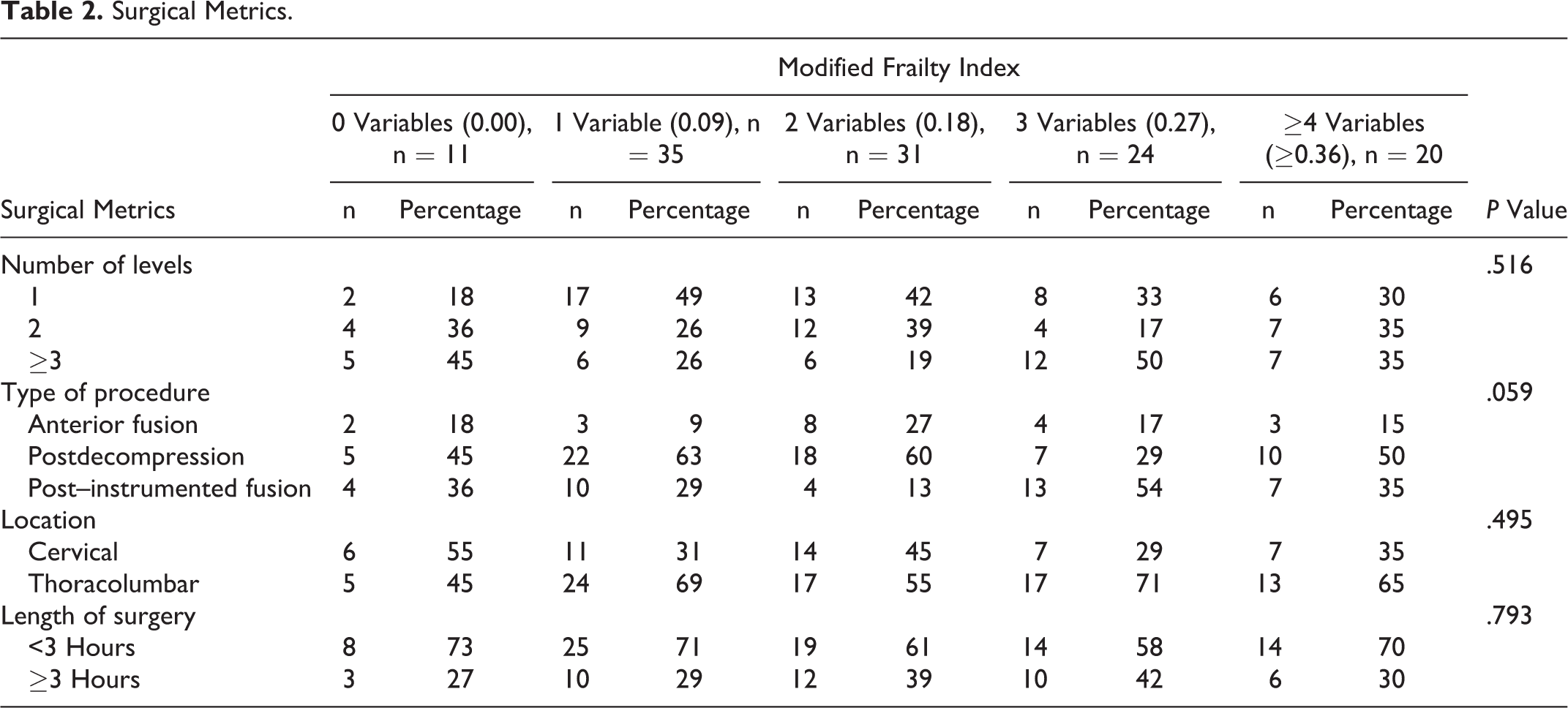
There was no significant difference in the number of surgical levels per operation (P = .516), type of procedure performed (P = .059), location of surgery (P = .495), or duration of surgery (P = .793) between cohorts (Table 2).
Surgical Metrics.
Postoperative Surgical Outcome Metrics
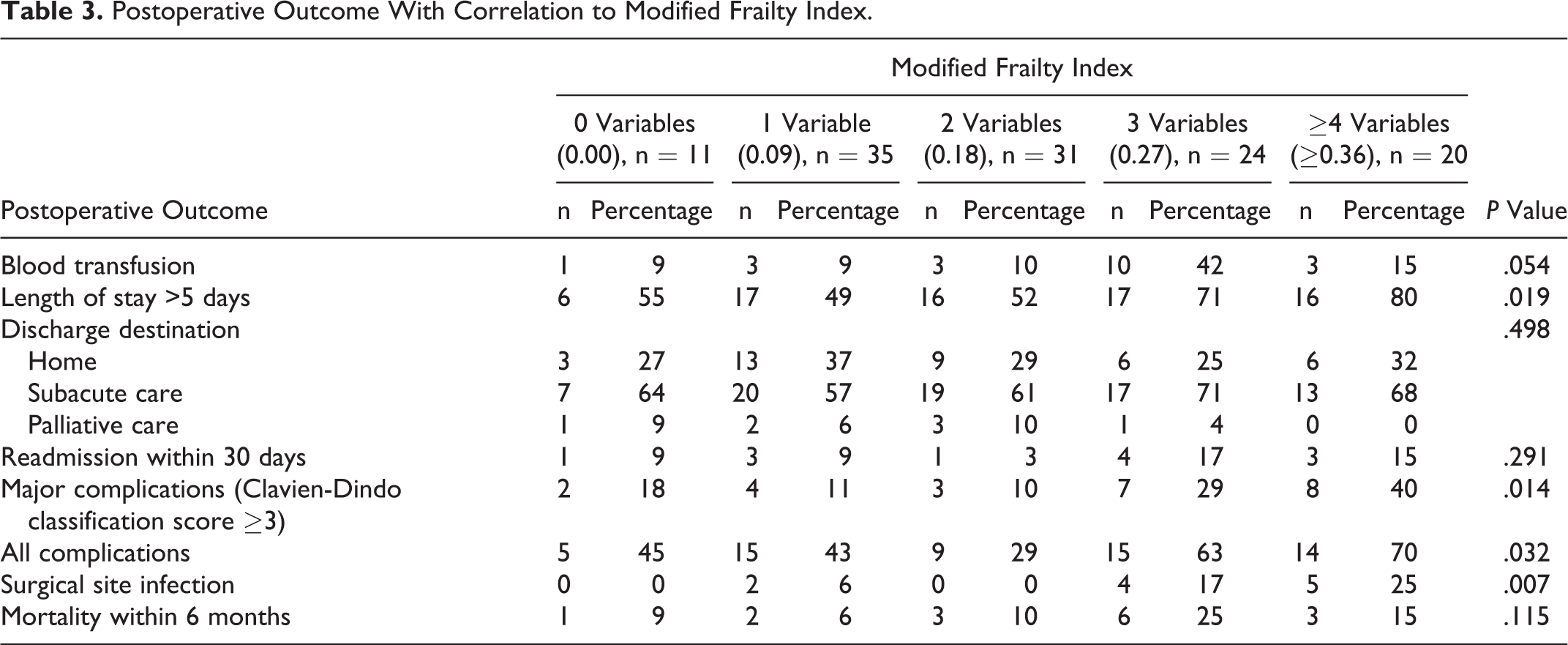
A significant difference in postoperative outcomes was observed between the mFI cohorts. As the mFI increased from 0 to ≥4 variables (≥0.36), the attendant risk of major complications, all complications, and surgical site infection increased from 18.2% to 40.0% (P = .014), 45.5% to 70.0% (P = .032), and 0% to 25.0% (P = .007), respectively. Additionally, lengthy acute hospital admission of >5 days was also increased as mFI increased from 0 to ≥4 variables (≥0.36; 54.5% vs 80.0%, P = .019). However, mortality within 6 months was indifferent between the cohorts (P = .115). There was no significant difference in requirement for blood transfusion (P = .054), discharge destination (P = .498), or readmission within 30 days (.291) observed between cohorts (Table 3).
Postoperative Outcome With Correlation to Modified Frailty Index.
Independent Predictors of Surgical Outcomes
As shown in Figure 1, the rates of mortality and morbidity were considerably increased in the mFI ≥3 variables (≥0.27) cohort when compared with the mFI <3 variables (<0.27) cohort. Binary multivariate analysis was conducted with mFI stratified into 2 categories: (1) low-frailty cohort, with mFI <3 variables (<0.27), and (2) high-frailty cohort, mFI ≥3 variables (≥0.27). By virtue of their univariate P values, gender, BMI, type of admission (elective or emergency), presence of instrumentation, type of approach (anterior or posterior), location of surgery (cervical spine or thoracolumbar spine), etiology of pathology (degenerative or nondegenerative), number of spinal levels (<3 or ≥3), albumin level, and mFI or ASA score were incorporated into the multivariable model.
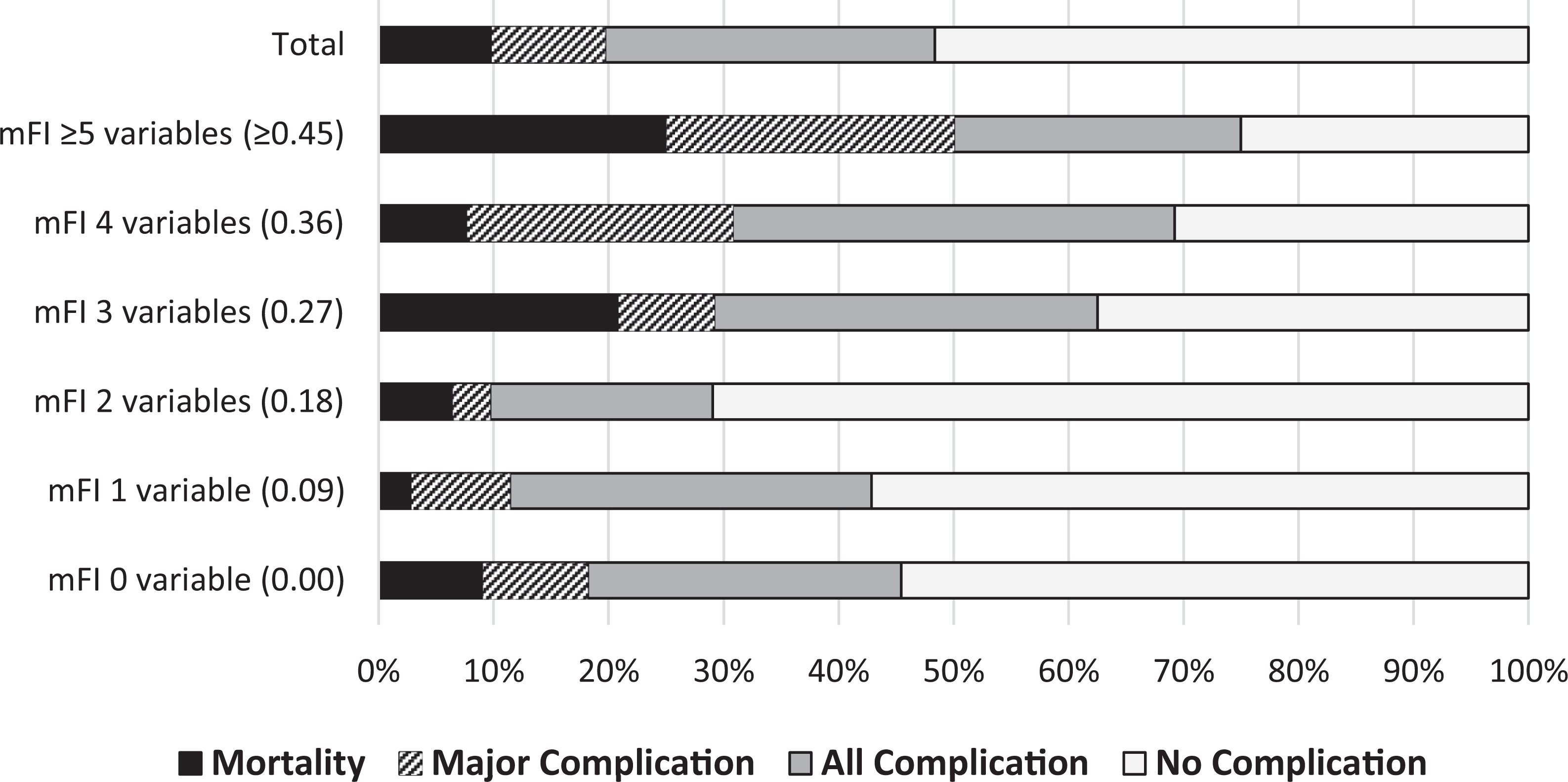
Stacked bar chart of mortality and morbidity with increasing modified Frailty Index (mFI).
Binary logistic regression analyses revealed that mFI ≥3 variables (≥0.27) conferred higher risk of (1) major complications (OR = 3.23; 95% CI = 1.16-8.99; P = .025), (2) all complications (OR = 3.46; 95% CI = 1.27-9.42; P = .015), (3) surgical site infection (OR = 12.82; 95% CI = 2.00-81.87; P = .007), and (4) mortality (OR = 4.04; 95% CI = 1.04-15.71; P = .044). Instrumented surgery (OR = 3.19; 95% CI = 1.01-10.04; P = .048) and surgery involving 3 or more spinal levels (OR = 2.96; 95% CI = 1.04-8.39; P = .041) increased the risk of major complications. Instrumented surgery (OR = 6.70; 95% CI = 1.98-22.73; P = .002), nondegenerative diagnosis (OR = 5.44; 95% CI = 1.51-19.59; P = .010), and posterior approach (OR = 6.86; 95% CI = 1.40-33.62; P = .018) also predicted postoperative complications. Surgical site infection was positively associated with cervical spine surgical site (OR = 5.58, 95% CI = 1.07-28.96, P = .041; Table 4). The Hosmer-Lemeshow Test and Omnibus Test of Model Coefficients confirmed satisfactory goodness of fit.
Independent Predictors of Surgical Outcomes Identified With Multivariate Logistic Regression Analysis.
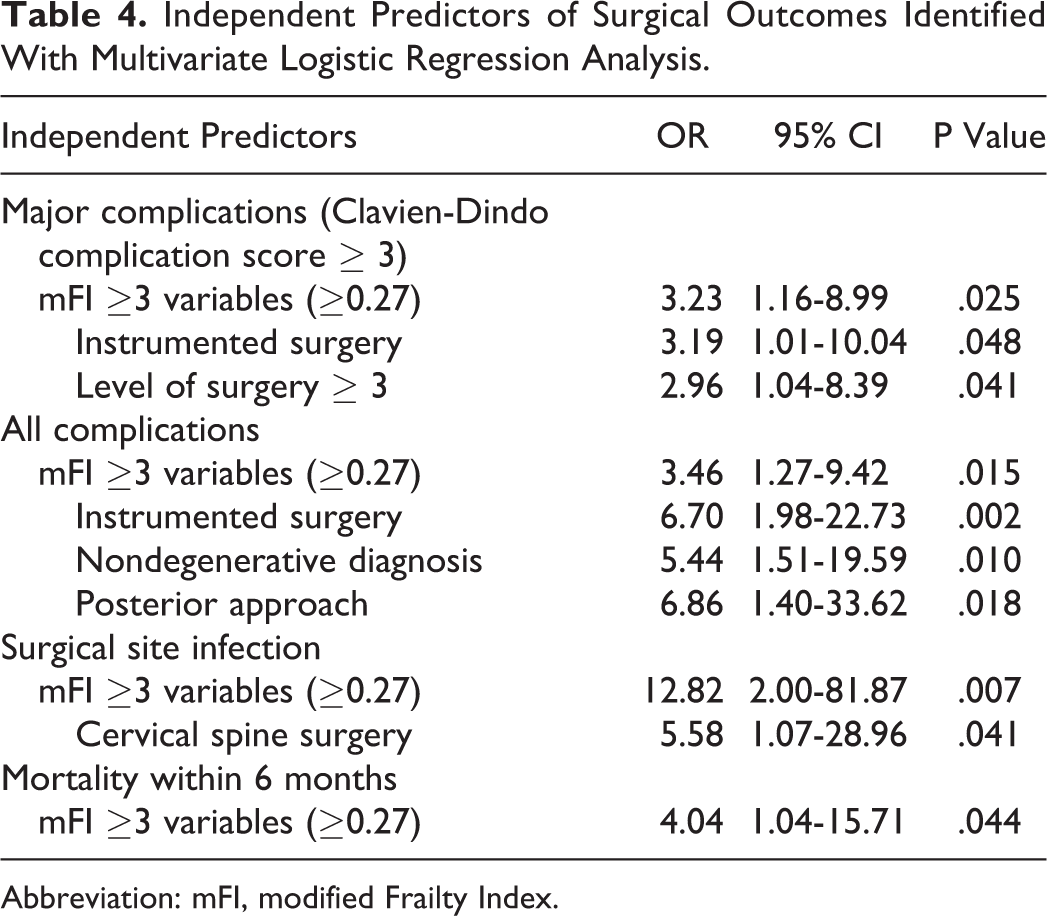
Abbreviation: mFI, modified Frailty Index.
Dose-Response Relationship of the mFI in Rate of Complications
Analysis involving a graduated increase in mFI demonstrated a positive relationship between increasing mFI and the risk of (1) major complications, (2) all complications, and (3) surgical site infections. The odds ratio of major complication increased from 3.23 (95% CI = 1.16-8.99; P = .025) in patients with a mFI of ≥3 variables (≥0.27) to 11.85 (95% CI = 1.68-83.61) in those with an mFI of ≥5 variables (≥0.45; P = .013). An mFI of ≥3 variables (≥0.27) carried an all-complication odds ratio of 3.46 (95% CI = 1.27-9.42; P = .015), which rose to 8.92 in patients with an mFI of ≥5 variables (≥0.45; 95% CI = 1.13-70.47, P = .038). A higher mFI was also associated with a greater likelihood of surgical site infection, with an odds ratio of 12.82 (95% CI = 2.01-81.87; P = .007) increasing to 48.93 (95% CI = 3.13-765.27) in those with an mFI of ≥3 variables (≥0.27) compared with patients with an mFI of ≥5 variables (≥0.45; P = .004). An increase in mFI from ≥3 to ≥5 variables (≥0.27 to ≥0.45) was also associated with a commensurate increase in mortality, from an odds ratio of 4.04 (95% CI = 1.04-15.71; P = .044) to 14.51 (95% CI = 1.49-140.94; P = .021). However, risk of mortality was not increased in the cohort with mFI ≥4 variables (≥0.36).
mFI Score Versus ASA Score
ASA scores did not predict major complications, all complications, surgical site infection, or mortality (P > .20; Table 5). The Spearman rank correlation coefficient between mFI and ASA was 0.2572, indicating a weak concordance.
Dose-Response Relationship of mFI and ASA Scores in Surgical Outcomes.
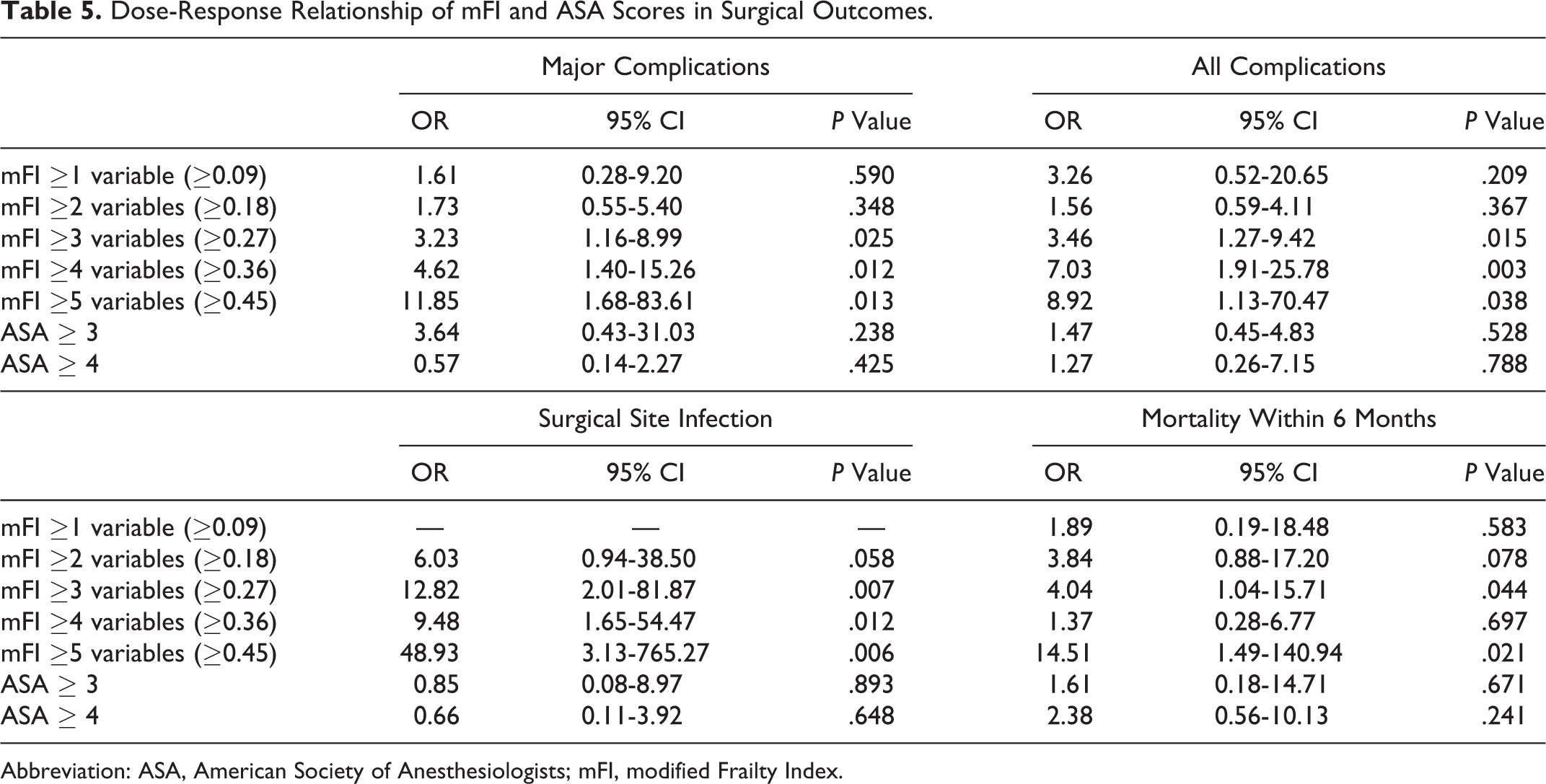
Abbreviation: ASA, American Society of Anesthesiologists; mFI, modified Frailty Index.
Discussion
The mFI has been previously associated with postoperative complications and mortality in a mixed spinal surgery cohort by Ali et al, 7 an adult spinal deformity surgery population by Leven et al, 3,9 and surgical complications in patients undergoing lumbar and cervical fusion surgery. 3,6 -9 However, no previous studies have specifically addressed the utility of mFI in elderly patients undergoing spine surgery. This study is unique because it examines the ability of the mFI, once dichotomized, to prognosticate the outcome of spinal surgery in patients 80 years and older.
The mFI provides an objective measurement of frailty, which is easily applicable in the clinical setting and is associated with less interassessor variability than previously utilized indices. 7,22 As a relatively concise score, it strikes a balance between being both practical and valid compared with more unwieldy indexes, such as the 70-variable CSHA-FI. 6 Beyond this, the mFI has been further abbreviated to the 5-variable mFI and has been shown to predict postoperative morbidity following posterior lumbar fusion surgery. 23
Consistent with a number of previously reported studies, 3,6 -8 our findings suggest that the 11-variable mFI has utility in stratifying the 80 years and older subpopulation into low and high risk according to a threshold score of 3 variables (0.27). We observed that the mFI of ≥3 variables (≥0.27) was strongly associated with an increased risk of complications, surgical site infection, and mortality. We also observed a substantial increase in morbidity and mortality as the mFI increases from ≥3 variables (≥0.27) to ≥4 variables (≥0.36) and ≥5 variables (≥0.45). This is congruent with prior studies in spinal surgery, which have also showed comparable stepwise increases in morbidity and mortality as mFI increases. 3,6 -9
The ability of the mFI to risk stratify patients 80 years and older undergoing spinal surgery carries even greater significance because the ASA score, in an identical population, did not correlate with any of the postoperative outcome measures. 17,24,25 Previous studies evaluating the ASA score have shown varying results. Fu et al 26 and Somani et al 27 contended that a higher ASA score predicted higher morbidity rates compared with lower ASA grades in a spinal surgery population, whereas Whitmore et al 28 contested that the ASA score was not predictive of complications. Importantly, these studies were performed in the general, rather than the 80 years and older population. We posit that at this extreme of age, the mFI proves superior to the ASA because of its unique combination of variables, which accurately captures the patient’s frailty status.
The mFI is increasingly relevant in light of an ageing population and improved surgical techniques, which potentially leads to an increased likelihood of operative management in elderly patients. 29 Interestingly, when the elderly undergo spinal surgery, it appears that the overall outcome remains favorable in a majority of patients. 30,31 Gerhardt et al 31 reviewed the outcome of patients who underwent lumbar decompression surgery aged 80 years or older and reported that 63.2% of these patients experienced an improvement in preexisting neurological deficits. Most of the patients (91%) also had improvement in neurogenic claudication and/or sciatica by the time of hospital discharge. 31 Similarly, Bouloussa et al 30 found a high rate of self-reported satisfaction after undergoing lumbar spine surgery in patients older than 85 years. 30 We propose that, among carefully selected patients, advanced age should not be a contraindication to spinal surgery. The mFI score can play a valuable role in risk stratifying and selecting suitable surgical candidates in the elderly population.
The utility of the Frailty Index for prediction of surgical risk will enable the surgeon to have a more informed discussion with patients aged 80 years and older and will assist the patient and their family in balancing the risks, benefits, and expected outcomes of spine surgery in this patient population.
The primary limitation of this study is the inability to further stratify the cohort and perform detailed subgroup analysis. This relates to the relative infrequency of patients 80 years and older requiring elective or emergency spine surgery. Moreover, this data is derived from a single center, although the center is the state-designated level 1 trauma center and receives a high volume of patients requiring spine surgery and is, therefore, likely to represent contemporary treatment for patients with spinal disease. Future studies in this domain should incorporate multiple centers and their registries, with propensity cohort matching, to further identify independent predictors of outcome of the individual mFI variable as well as other comorbidity indices in this expanding population of patients.
Conclusion
Presence of ≥3 out of 11 mFI variables (a score of ≥0.27) was associated with significantly higher risk of postoperative morbidity in patients 80 years and older undergoing spinal surgery. The mFI-associated risk stratification provides a valuable adjunct in surgical decision making for this rapidly growing subpopulation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.