
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To determine the predictive capability between the 5-factor modified frailty index (mFI-5) scores and adverse clinical and radiographic outcomes following single-level transforaminal lumbar interbody fusion (TLIF).
Methods
All patients over the age of 50 undergoing single-level open or minimally invasive TLIF from 2012 to 2021 with a minimum follow-up of 1 year were identified. Deformity, trauma, emergency, and tumor cases were excluded as were patients undergoing revision surgeries. An mFI-5 score was computed for each patient using a set of five factors which included hypertension requiring medication, chronic obstructive pulmonary disease, diabetes mellitus, congestive heart failure, and partially or fully dependent functional status. Univariate and multivariate logistic regression analysis were performed to evaluate the impact of mFI-5 scores on readmissions, reoperations, and postoperative complications.
Results
156 patients were included and grouped according to their level of frailty: no-frailty (mFI = 0, n = 67), mild frailty (mFI = 1, n = 59), and severe frailty (mFI = 2+, n = 30). Multivariate analysis found high levels of frailty (mFI = 2+) to be independent predictors of reoperation (OR: 16.9, CI: 2.7 - 106.9, P = .003) and related readmissions (OR = 16.5, CI: 2.6 - 102.7, P = .003) as compared to the no-frailty group. An mFI-5 score of 2+ was also predictive of any complication (OR = 4.5, CI: 1.4 - 14.3, P = .01) and adjacent segment disease (ASD) (OR = 12.5, CI: 1.2 - 134.0, P = .037).
Conclusion
High levels of frailty were predictive of related readmissions, reoperations, any complications, and ASD in older adult patients undergoing single-level TLIF.
Keywords
Introduction
Frailty is characterized by an age-associated decline in functional reserve of multiple organ systems and contributes to an increased susceptibility to adverse postoperative events including infections, revision surgeries, and mortality.1,2 Several studies have demonstrated the utility of frailty indices in identifying patients at high risk for postoperative complications following various orthopaedic procedures including lumbar fusion.3-5 Although numerous frailty indices have been developed, the modified frailty index remains the most frequently cited index within the literature and most adaptable across spine pathologies. 6 The original 11-factor modified frailty index (mFI-11) is comprised of 11 comorbidities and patient functional status and has been shown to be an effective predictor of adverse outcomes following various forms of thoracolumbar surgery.3,5 However, emerging studies suggest that the truncated 5-factor modified frailty index (mFI-5) may be a more concise and equally effective tool for predicting postoperative complication following spine surgery.1,7,8
Transforaminal lumbar interbody fusion (TLIF) remains a commonly utilized procedure for the treatment of various degenerative pathologies of the spine. TLIF is a dependable procedure that offers relatively easier access to posterior lumbar anatomy, while preserving ligamentous structures and mechanical stability of the spine relative to a traditional posterior approach. 9 However, only a few studies have analyzed the relationship between frailty scores and clinical outcomes following TLIF.1,10 Moses et al 10 found that increasing frailty scores, based on mFI-11, were associated with higher morbidity and a greater likelihood of postoperative complications following single-level TLIF. Large database studies have found both mFI-5 and mFI-11 to be predictive of major complications, reoperations, and morbidity following both posterior lumbar fusion (PLF) and TLIF.1,11 Despite the popularity of both indices, the mFI-5 provides more utility in the clinical setting as it is comprised of only five factors that are readily available in a patient’s chart and is a more rapid, yet equally effective, method of stratifying patients. However, the results of both aforementioned studies are limited by the fact that neither study is able to control for the surgical technique being implemented and had a limited postoperative period of only 30 days.1,11
Although studies have described the utility of mFI-5 scores for several techniques related to lumbar fusion, no studies have explored its capabilities in patients undergoing TLIF. Additionally, there is a paucity of literature assessing the relationship between frailty and the development of long-term postoperative complications, such as pseudarthrosis and adjacent level disease. Therefore, the aim of this study is to determine the utility of mFI-5 scores as a risk stratification tool for the development of adverse clinical and radiographic outcomes following single-level TLIF.
Materials and Methods
Study Design
Institutional review board approval was obtained for this study (PR#21-016). Informed consent was not required for this study and exemption was granted in the IRB given the retrospective nature of the study. A retrospective review of a single institution’s database was performed to identify all patients between 2012 and 2021 who underwent either minimally invasive or open single-level TLIF with direct decompression and posterior stabilization. Patients were included in this study if they met the following criteria: adult over 50 years of age, single-level fusion, availability of medical records with a minimum follow-up of 1 year, and operative indication of degenerative disc disease, lumbar spinal stenosis, or degenerative spondylolisthesis. An age restriction of above 50 was used based upon a systematic review conducted by Spiers et al
12
which found that frailty indices had limited predictive capabilities in younger populations. This cut off is similar to the much of the existing literature on the predictive capabilities of mFI-5.7,13 Deformity, trauma, emergency, infection and tumor cases were excluded as were patients undergoing revision surgeries, multiple procedures, or multilevel fusions. The patient selection criteria for this study are summarized in Figure 1. Flowchart for patient selection criteria.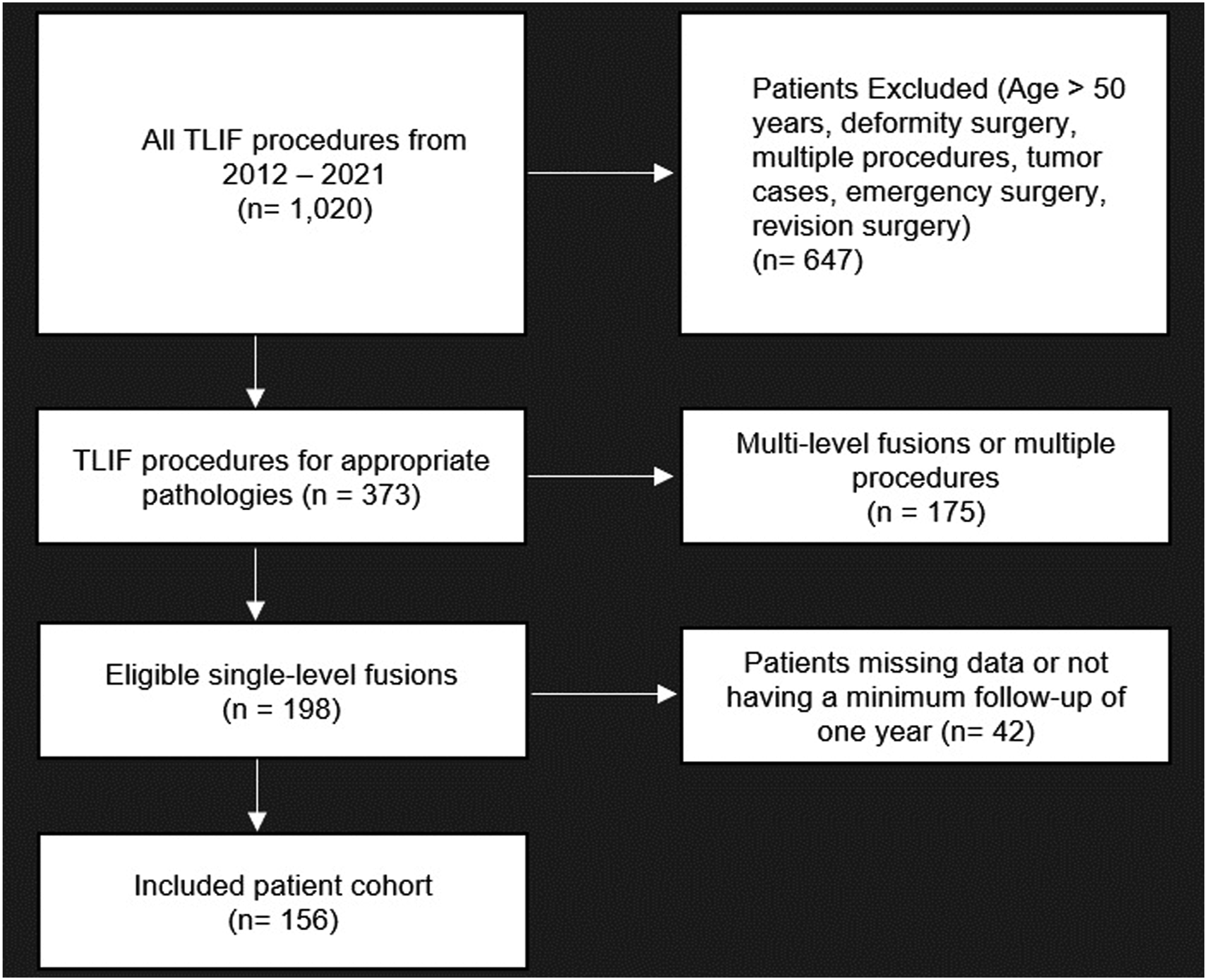
Modified Frailty Index
The mFI-5 is a risk assessment tool derived from the mFI-11 which was based on 11 factors recorded in the American College of Surgeons’ National Surgical Quality Improvement Program (ACS NSQIP) (Chicago, Illinois, United States). 14 The initial index was comprised of 16 variables obtained from the 70-factor Canada Study of Health and Aging Frailty Index. 14 The truncated mFI-5 score, ranging from 0 to 5, was calculated for each patient following thorough review of all preoperative medical clearance forms from various providers and specialists, especially primary care physicians (PCPs). Additionally, review of preoperative evaluations performed by orthopaedic surgeons and anesthesiologists were performed to verify patient comorbidities and functional status.
Patient mFI-5 Variables.
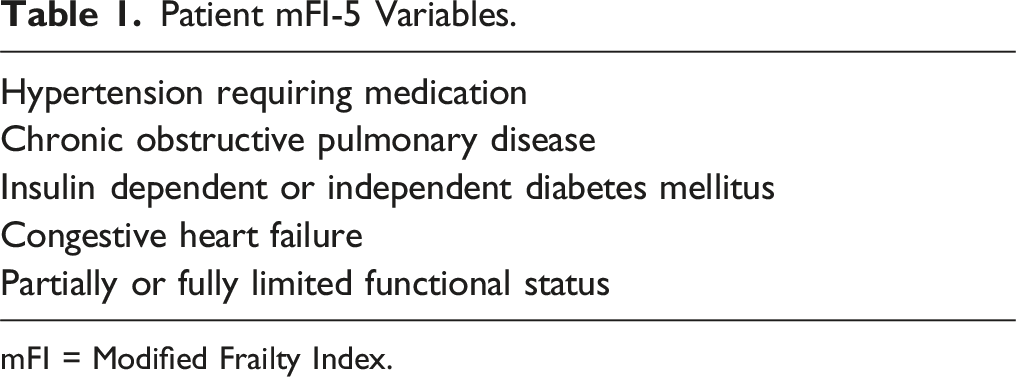
mFI = Modified Frailty Index.
Clinical/Radiographic Outcomes
Demographic data, including age, gender distribution, and BMI, as well as procedural technique (open or minimally invasive TLIF) were recorded for each patient from postoperative notes. Perioperative data was also collected to evaluate the length of stay (LOS), estimated blood loss (EBL), operative time, and disposition status. All postoperative medical records and follow-up visits were thoroughly reviewed to identify and evaluate all possible postoperative complications in our cohort. These complications included urinary tract infections (UTIs), deep and superficial surgical site infections (SSIs), durotomy, hardware failure, pseudarthrosis and adjacent level disease. Rates of readmission or reoperation related to the index procedure were also obtained and evaluated.
Radiographs were performed utilizing anteroposterior (AP) and lateral standing X-ray imaging and were obtained at follow-up visits. CT scans were ordered for patients who displayed clinical symptoms concerning for pseudarthrosis including return of presurgical pain, worsening pain, or neurologic symptoms such as numbness or tingling. Fusion status was determined by the Bridwell-Lenke grading system. 15 Patients with a grade of 3 or 4 on imaging and associated clinical symptoms were considered to be cases of clinically significant pseudarthrosis. Similarly, patients were identified as having clinically significant adjacent segment disease (ASD) if they had symptoms suggestive of ASD and supportive radiographic evidence. Radiographically, ASD was defined as the presence of 1 or more of the following criteria: ≥3 mm anteroposterior translation, onset of ≥10° segmental kyphosis, and/or ≥50% loss of disc height. 16
Surgical Procedure
All procedures were performed by two of four fellowship trained orthopaedic spine surgeons via the same technique. Selection criteria for operative technique used was determined by multiple factors. Preoperative MRI imaging and evaluation of patient-specific anatomy by attending spine surgeons as well as patient preference ultimately led to the selection of either an open or minimally invasive approach.
All MI-TLIF procedures utilized intraoperative fluoroscopy to visualize and identify the correct levels. Care was taken to initiate a starting point at the pedicle, lateral to the facet joint at the most proximal level. Incisions were connected cranial-to-caudal in a paramedian or Wiltse fashion. A 24-mm docking port was then inserted and docked over the facet joint after tubular retractors were used and sequential dilation of the paraspinous soft tissue was performed. Trocars were bilaterally introduced over the pedicles at the surgical levels. Guide wires were then bilaterally placed into the pedicles; appropriate placement was confirmed utilizing fluoroscopy, and wires were taped to the patient. Next, a high-speed burr was used to remove the inferior articular facet of the level above and the superior articular facet of the level below the site of decompression. The traversing nerve root was then identified and retracted. Annulotomy was performed after the disc space was identified.
Discectomy was performed using a series of shavers and curettes, and trial cages were then used to determine the correct size. After the disc space was filled with local bone graft (from facet/lamina) and allograft, a non-expandable PEEK cages (DePuy Synthes®, Lumbar cage, Concorde Bullet, Massachusetts, United States) was placed in all patients. The cage size was determined on a patient-specific basis with best intraoperative fit affected by preoperative disc height. Next, a pedicle tap was used to obtain correct screw trajectory. Pedicle screws were then placed, and correct positioning was confirmed via fluoroscopy. Electromyographic potential was tested across both the pedicle tap and screw with an acceptable threshold of 10 mA. Finally, rods were placed, and the caps were applied. Once this was done, the wound was thoroughly irrigated, and the fascia was closed with absorbable Vicryl suture. The skin was closed with absorbable Monocryl suture, final confirmatory imaging was taken, and the patient was extubated promptly.
All open TLIF procedures utilized utilized fluoroscopic guidance to identify the appropriate levels. A midline skin incision was then made and dissection was carried down from the skin to the deep dorsal lumbosacral fascia. Periosteal type dissection was carried down to expose the spinous process and facet joints of the implicated vertebral level. A facetectomy and subsequent laminectomy were performed using a high-speed burr. An annulotomy was made, followed by complete discectomy and endplate preparation. Trial cages were then inserted to establish the correct size. The disc space was then filled with the same mixture of local bonegraft and allograft, followed by the insertion of a PEEK cage as outlined in the MI-TLIF procedure. Similarly, bilateral pedicle screws and rods were placed using standard anatomic landmarks and fluoroscopy. Once this was done, the wound was thoroughly irrigated, and the fascia was closed with absorbable Vicryl suture. The skin was closed with absorbable Monocryl suture, final confirmatory imaging was taken, and the patient was extubated promptly.
Statistical Analysis
Three patient cohorts were constructed based on level of frailty. Percentages were calculated for all dichotomous variables and means values with standard deviations were generated for continuous variables. Univariate analysis was conducted to compare demographics, comorbidities, and postoperative complications across the varying cohorts based on mFI-5 scores. Categorical or dichotomous variables were compared using chi-squared tests. Continuous variables were assessed using one-way analysis of variance (ANOVA) tests which has been previously described in the literature.10,17 Multivariate logistic regressions were performed to evaluate the impact of mFI-5 scores on the odds of developing any of the previously mentioned complications found to be significant in the univariate analysis as compared to an mFI-5 score of 0. Preoperative demographic variables including BMI, age, and gender were included in the regression to assess if mFI-5 scores were independent predictors for adverse events. Odds ratios, 95% confidence intervals, and P-values for each variable were calculated from the regression. All statistical analyses were performed using SPSS version 24.0 (IBM Corp., Amonk, NY, USA). P-values less than .05 were considered statistically significant.
Results
Study Population/Demographics
Patient Demographics and Operative Technique Used.
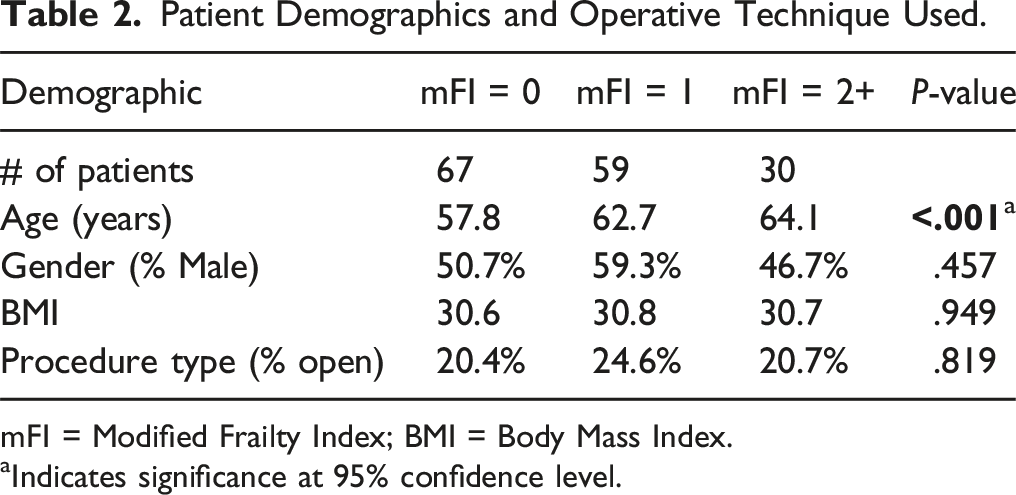
mFI = Modified Frailty Index; BMI = Body Mass Index.
aIndicates significance at 95% confidence level.
Perioperative Data
Perioperative Data and Disposition Status.
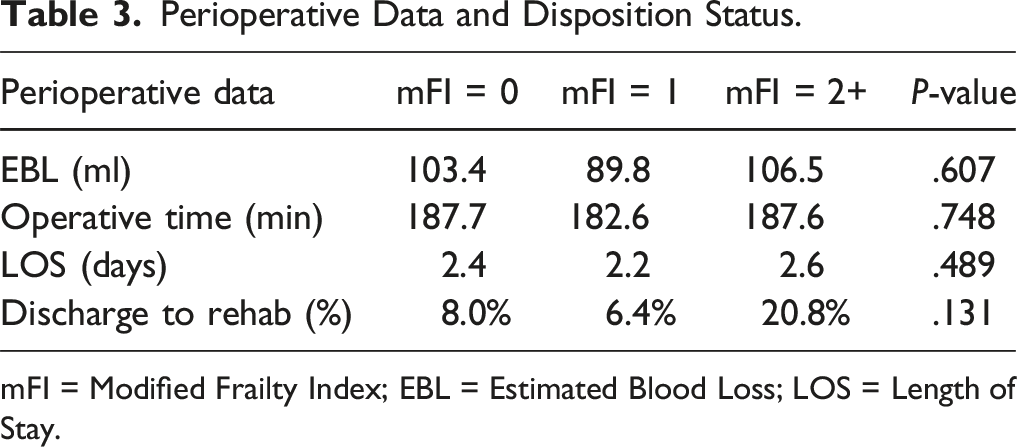
mFI = Modified Frailty Index; EBL = Estimated Blood Loss; LOS = Length of Stay.
Postoperative Complications
Reoperation Rates, Readmission rates, and Postoperative Complications.
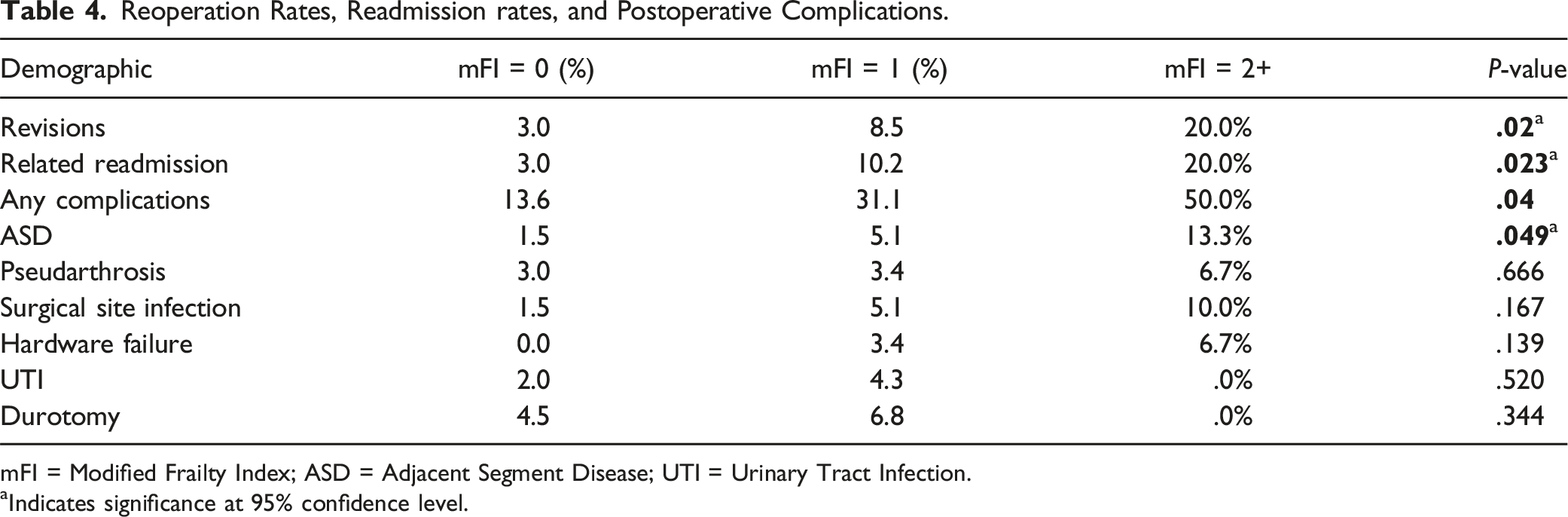
mFI = Modified Frailty Index; ASD = Adjacent Segment Disease; UTI = Urinary Tract Infection.
aIndicates significance at 95% confidence level.
Rates of all short-term complications, within 3 months following surgery, are also recorded in Table 4. Only the following short-term complications were observed in our cohort: SSI, hardware failure, UTI, and durotomy. Rates of SSIs (mFI 0: 1.5%, mFI 1: 3.4%, mFI 2+: 10.0%; P = .167) and hardware failure (mFI 0: .0%, mFI 1: 4.3%, mFI 2+: 6.7%; P = .139) increased in association with increasing levels of frailty. However, the differences observed were not found to be significantly different across the 3 groups. No significant association was observed between increasing frailty and rates of UTI or durotomy.
A total of 6 cases of symptomatic pseudarthrosis were noted at follow-up and confirmed with CT imaging. The severe-frailty group had the highest rate of pseudarthrosis at 6.7%, followed by the mild-frailty group at 3.4% and no-frailty group at 3.0% (Table 4). However, despite the stepwise increase in rates of pseudarthrosis, the differences were not found to be significant. 8 cases of radiographic ASD were identified in our cohort. Increasing levels of frailty showed a significant increase in rates of ASD (mFI 0: 1.5%, mFI 1: 5.1%, and mFI 2+: 13.3%; P = .049).
Multivariate Logistic Regression Utilized to Determine Impact of mFI-5 Score on Adverse Post-Operative Outcomes.
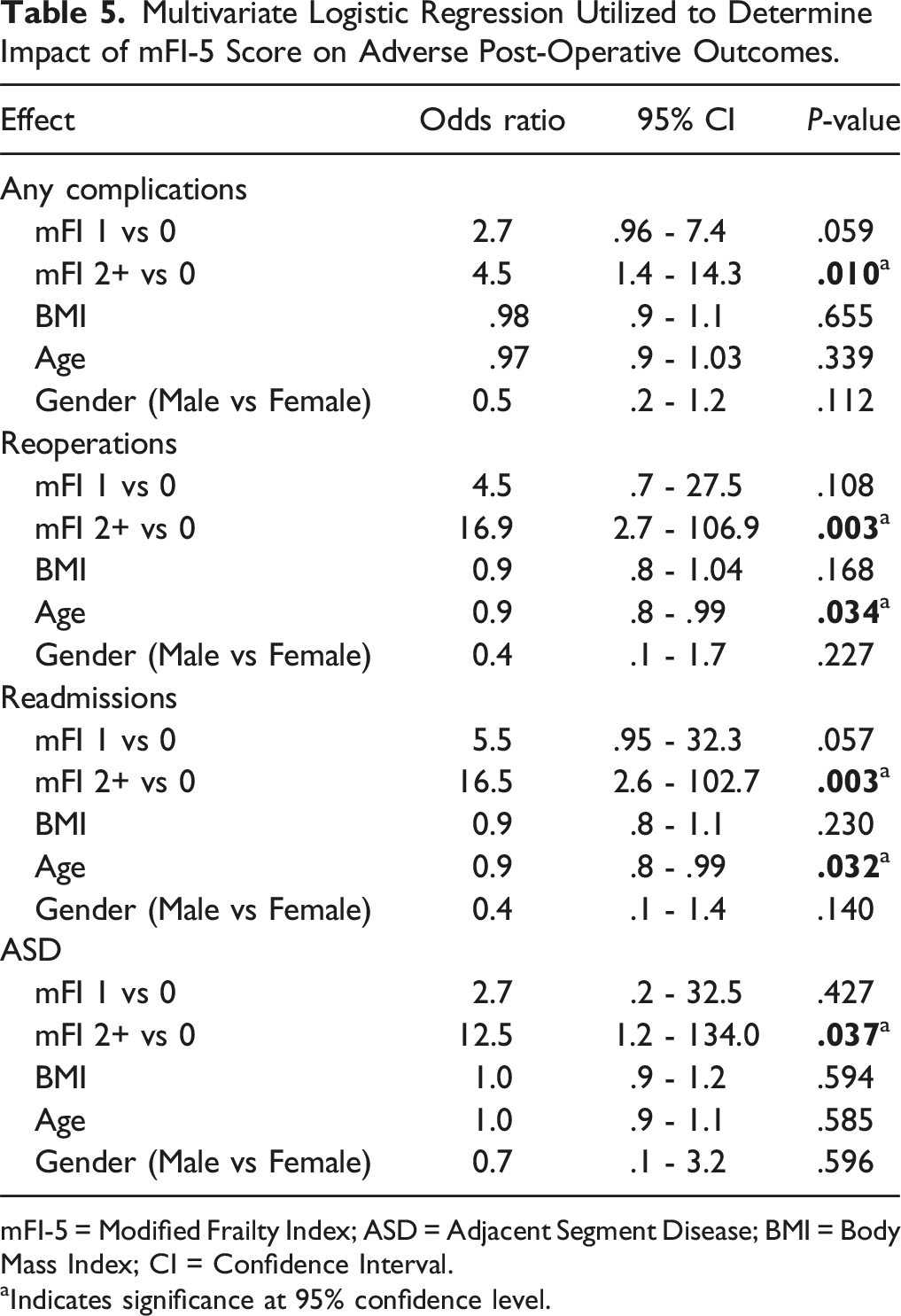
mFI-5 = Modified Frailty Index; ASD = Adjacent Segment Disease; BMI = Body Mass Index; CI = Confidence Interval.
aIndicates significance at 95% confidence level.
Discussion
The increasing lifespan of the average American is associated with an increasing demand for procedures, such as TLIF, necessary to address degenerative changes of the spine. Although age is associated with poor outcomes, several studies have found age to be an inappropriate surrogate for risk of postoperative complications following TLIF.18,19 Frailty, or the physiological reserve to manage external stressors, has been shown to be a more accurate predictor of postoperative adverse events. Several frailty indices have been developed; however, the mFI-5 has quickly gained popularity as it utilizes concise, objective and readily available data. More recently, mFI-5 has shown promising predictive capabilities following various forms of spine procedures including lumbar arthrodesis.1,8
Our study is the first of its kind to analyze for an association between mFI-5 and adverse events in 156 patients undergoing single-level TLIF. As expected, increasing levels of frailty were significantly associated with older age. Despite the differences observed in age across frailty cohorts, multivariate regression analysis did not find age to be associated with an increased risk of adverse events. Additionally, the results of this study found no significant association between frailty and perioperative outcomes including mean EBL, operative time, LOS, or rate of disposition to a rehabilitation center. Moses et al 10 found that higher levels of frailty, based on mFI-11, were associated with increased LOS as well as lower rates of postoperative disposition home. Database studies have also found higher levels of frailty, based on mFI-5, to be associated with decreased rates of disposition home and increased LOS following an analysis of 1- and 2-level posterior lumbar fusions.1,20 However, these studies have pooled various surgical techniques together which may influence the outcomes observed.
Increasing levels of frailty were found to be predictive of adverse long-term outcomes, including readmissions, reoperations, and following TLIF. Multivariate logistic regression found the severe-frailty group to be at a significantly greater risk of reoperations (OR = 16.9, P = .003) and readmissions (OR = 16.5, P = .003) as compared to the no-frailty group. Similarly, the odds of developing any postoperative complication increased by 4.5 times in the severe-frailty group as compared to the no-frailty group (P = .01). However, despite higher rates of postoperative complications in higher frailty groups, no significant differences were observed in specific short-term complications observed in our study including UTIs, SSIs, durotomy, or hardware failure. Similarly, Moses et al 10 found greater mFI-11 scores to be associated with the development of complications increasing from 10.3% in their no-frailty group to 63.6% in their severe-frailty group. Interestingly, their study found no association between frailty and reoperations. 10 Weaver et al 1 found mFI-5 to be an independent predictor of SSIs, UTIs, any complications and reoperations following posterior fusions.
As previously mentioned, Moses et al 10 found several associations between frailty and adverse outcomes following single-level TLIF using mFI-11 scores. The findings of this present study demonstrate that mFI-5 may be comparable to mFI-11 index at predicting overall complications. Additionally, mFI-5 may offer advantages in identifying patients requiring a revision surgery, whereas mFI-11 may offer more utility in identifying patients requiring a longer postoperative stay or disposition to a rehab center. However, the mFI-5 index offers additional benefits over other frailty indices as it is a much more concise screening tool comprised of objective and readily available patient information. Nonetheless, both studies further solidify the relationship between frailty and adverse postoperative complications in single-level TLIF.
This study is one of the first to analyze for an association between frailty and long-term complications including pseudarthrosis and ASD. Miller et al 21 found higher levels of frailty to be predictive of developing pseudarthrosis using the adult spinal deformity frailty index. Although our study found no relationship between frailty and pseudarthrosis, we did find increasing levels of frailty to be associated with significantly higher rates of ASD (mFI 2+: 13.3%, mFI 1: 5.1%, mFI 0: 1.5%, P = .049). Several studies have shown increased age to be an important risk factor for ASD,22,23 while other studies have identified BMI as a more effective predictor.24,25 However, our multivariate analysis, which included both age and BMI, found that only high levels of frailty were independently associated with increased odds of developing ASD (OR = 12.5, P = .037). These findings suggest that frailty may be a more accurate surrogate for predicting ASD over other patient specific variables.
It has been theorized that biomechanical changes following lumbar fusion are likely responsible for the development of ASD. These changes include increased facet loading, intradiscal pressure, and mobility at adjacent vertebral levels which may exacerbate degenerative changes of the spine. 26 Frailty has been shown to be associated with diminished bone mineral density, muscle mass and physical function.27,28 Therefore, patients with high levels of frailty may be less capable of tolerating the additional biomechanical stress placed on adjacent levels following lumbar arthrodesis, thereby predisposing them to an increased susceptibility to ASD. Our findings suggest that the mFI-5 score may be an adequate risk stratification tool for ASD and reoperations to assist orthopaedic surgeons in identifying patients who are poor candidates for operative management of degenerative lumbar disease.
The present study is constrained by several important limitations. First, the retrospective nature of this study, using data from a single-institution, results in an inherently small sample size compared to much larger database studies or meta-analyses. This is reflected in the wide ranges of odds ratios generated from the multivariate analyses performed given the rare outcome measures analyzed. Also, patients that were treated with revision surgery or developed complications addressed at outside institutions were not recorded in the study. Additionally, our study did not include preoperative radiographic parameters related to sagittal alignment which have been associated with the development of ASD and reoperations following TLIF. Future studies should perform a prospective analysis of frailty while controlling for potentially confounding variables including sagittal alignment, bone mineral density and additional patient comorbidities in a larger sample of patients. Despite these limitations, this is the first study to analyze the impact of pre-operative mFI-5 scores in patients undergoing single-level TLIF. Furthermore, this study remains the first to find an association between high levels of frailty and the development of ASD. Our findings may be used as a point of reference for orthopaedic spine surgeons to better inform patients of their relative risk of reoperation and postoperative complications based on their frailty risk profiles. Additionally, mFI-5 scores may be used to better manage high risk patients through preoperative optimization as well as more frequent follow up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Emami receives grants/research support from NuVasive. Dr. Hwang is a consultant for Stryker Spine. None of these are applicable to the current study. For the remaining authors, none were declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional review board approval was obtained for this study.