
Abstract
Study Design:
Retrospective study.
Objectives:
Treatment of spinal tuberculosis in the elderly involves consideration of compromised physiology, which often poses a clinical challenge to the surgeons to balance surgical safety versus deteriorating function. Frailty scoring has been reported as an effective tool to predict mortality and morbidity in cardiovascular surgery and recently in hip fractures. Its use in spinal surgery is scarcely reported.
Methods:
We included elderly patients operated for spinal tuberculosis. Demographic, clinical and radiological profile with operative details of instrumentation, blood loss, surgical duration and mortality were noted. Modified frailty score (MFS) was calculated for each patient. There were 26 patients (males 9, females 17) with a mean age of 73.2 years. The patients were divided into those with 30-day postoperative mortality (M) and those who survived (S). The null hypothesis was that the MFS was comparable in both the groups.
Results:
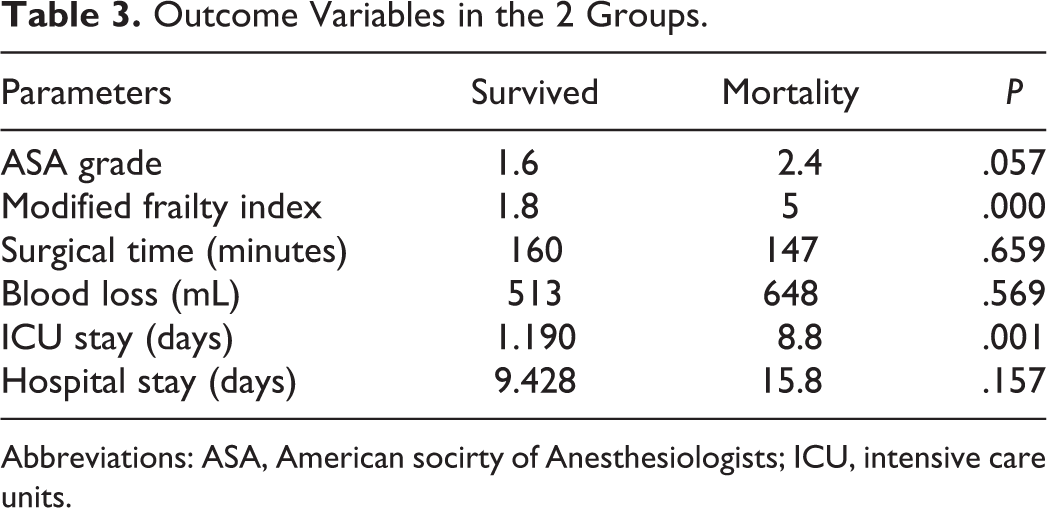
The M group had 5 patients (19.2%) and the S group consisted of 21 patients. There was no statistical difference between the groups with regard to mean age, sex, number of medical comorbidities, ASA (American Society of Anesthesiologists) grade, Frankel grade C or worse, blood loss, and operative time. The mean MFS in M group was 5 and in S group was 1.8, which was statistically significant (P < .001).
Conclusions:
Higher MFS is associated with postoperative 30-day mortality in the elderly patients with spinal tuberculosis undergoing surgery. It can be used as a guide to predict 30-day postoperative mortality in these patients.
Introduction
Spinal tuberculosis in the elderly is on the rise primarily due to longer survival rates. 1 The clinical presentation commonly involves back pain with or without neurological deficit. Medical treatment is usually successful. However, surgical intervention is necessary when pain is incapacitating or when there is a neurological deterioration/compromise. 2 Decisions regarding surgical intervention in the elderly can be tricky and pose as a surgical and medical challenge. The elderly often have a compromised physiology and a variable ability to cope with the surgical stress. Comorbidities and the lack of specialized perioperative care to manage them add to the problem. Surgical challenges include poor bone stock, degenerative spine, appropriate length of the construct, duration of surgery, and blood loss. 2 –4
The capacity of the patient to tolerate the surgical insult is unknown and difficult to predict because of scarcity of standardized data and methods to predict adverse outcomes. Frailty scoring is an emerging concept to assess adverse outcomes in the elderly patient undergoing surgery. 5 This concept has been successfully used in gastric, oncologic, urologic, hepatobiliary, cardiac, and hip fracture surgeries. However, its role in spine surgery has not been studied yet. 6
Elderly patients with spinal tuberculosis are often kept on prolonged bed rest, which significantly diminishes the physiological reserve although they may not have major co morbidities. Surgical stress after such a period of diminished functions can be overwhelming. Thus, in this article we intend to study the usefulness of frailty scoring in elderly patients undergoing surgery for spinal tuberculosis.
Materials and Methods
This was a retrospective study performed in a single institution. A total of 295 patients of spondylodiscitis were operated between 2005 and 2015. We identified 26 consecutive patients who underwent spinal surgery for tuberculosis satisfying the inclusion/exclusion criteria. Inclusion criteria were (1) patient age more than 70 years and (2) culture-proven tuberculosis. Exclusion criteria included (1) age less than 70 years and (2) negative culture or culture showing growth other than mycobacteria. Data was obtained from electronic medical records (orthopedic/medical history and preoperative anesthesia and physician notes) and institutional PACS (Picture Archiving and Communication Systems).
Indications of surgery included failed conservative treatment for 3 months, spinal instability, or progressive or dense neurological deficit. Demographic details of patients are presented in Table 2. Histopathology and culture/sensitivity tests were done in all the patients. Postoperatively antituberculous drugs were started in consultation with chest physician as per institutional protocol.
The modified frailty score (MFS) 7 based on 19 of the potential 70 Canadian Study of Health and Aging clinical deficits was used to measure frailty (Table 1). Each clinical deficit was given 2 points except mobility status was given 3 points. Each deficit was given 0 points if not present and 1 point if it was present. Ambulatory patients without assistive device were given 0 points, patients ambulatory with support (walker/stick) were given 1 point, and nonambulatory patients (wheelchair-bound) were given 3 points. Other parameters recorded were American Society of Anesthesiologists (ASA) grade, operative time, blood loss, length of hospital stay, intensive care unit (ICU) stay and preoperative neurological deficit using Frankel system (Table 2).
Modified Frailty Score Clinical Deficits.
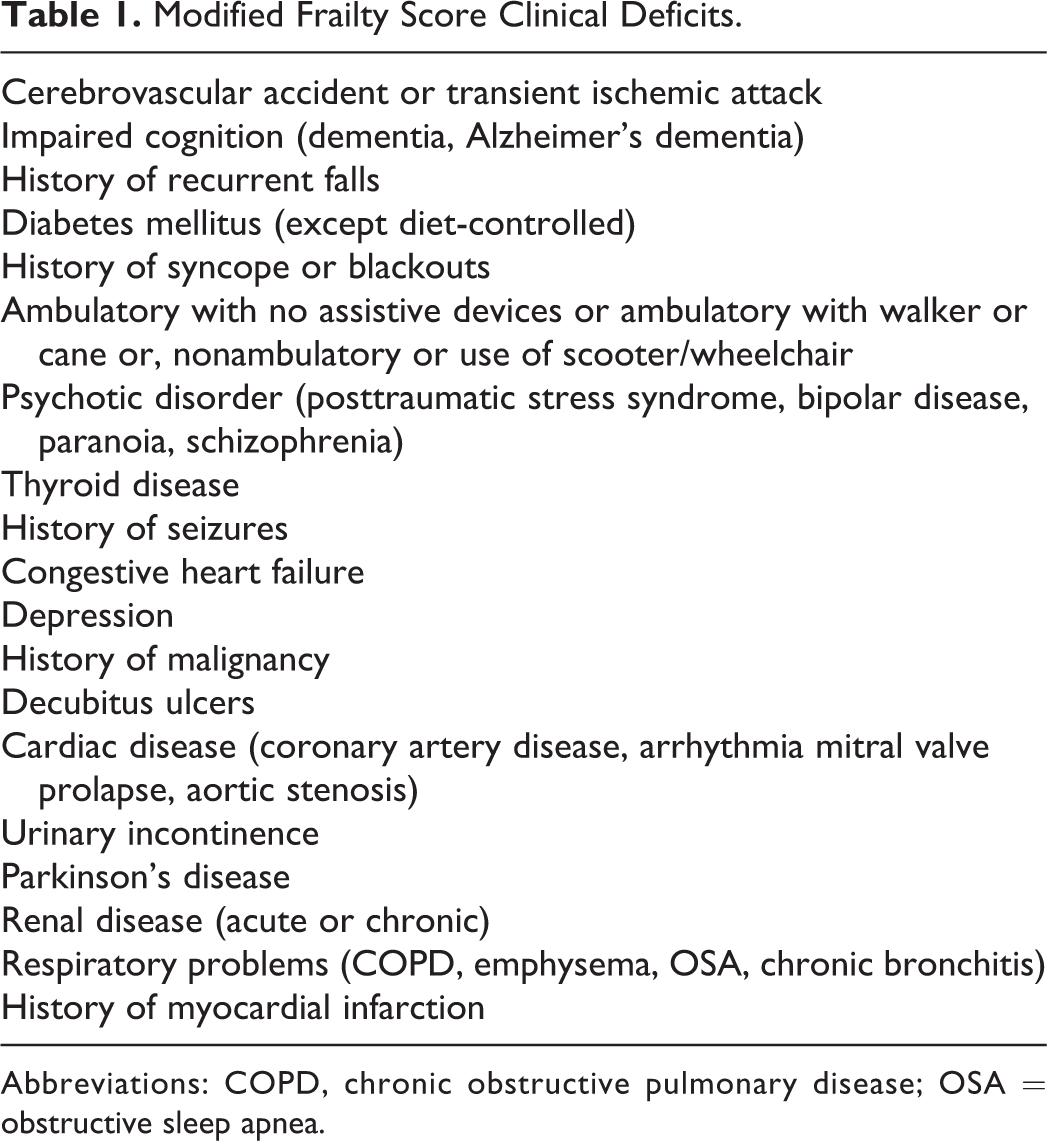
Abbreviations: COPD, chronic obstructive pulmonary disease; OSA = obstructive sleep apnea.
Demographic and Surgical Details of Patients.
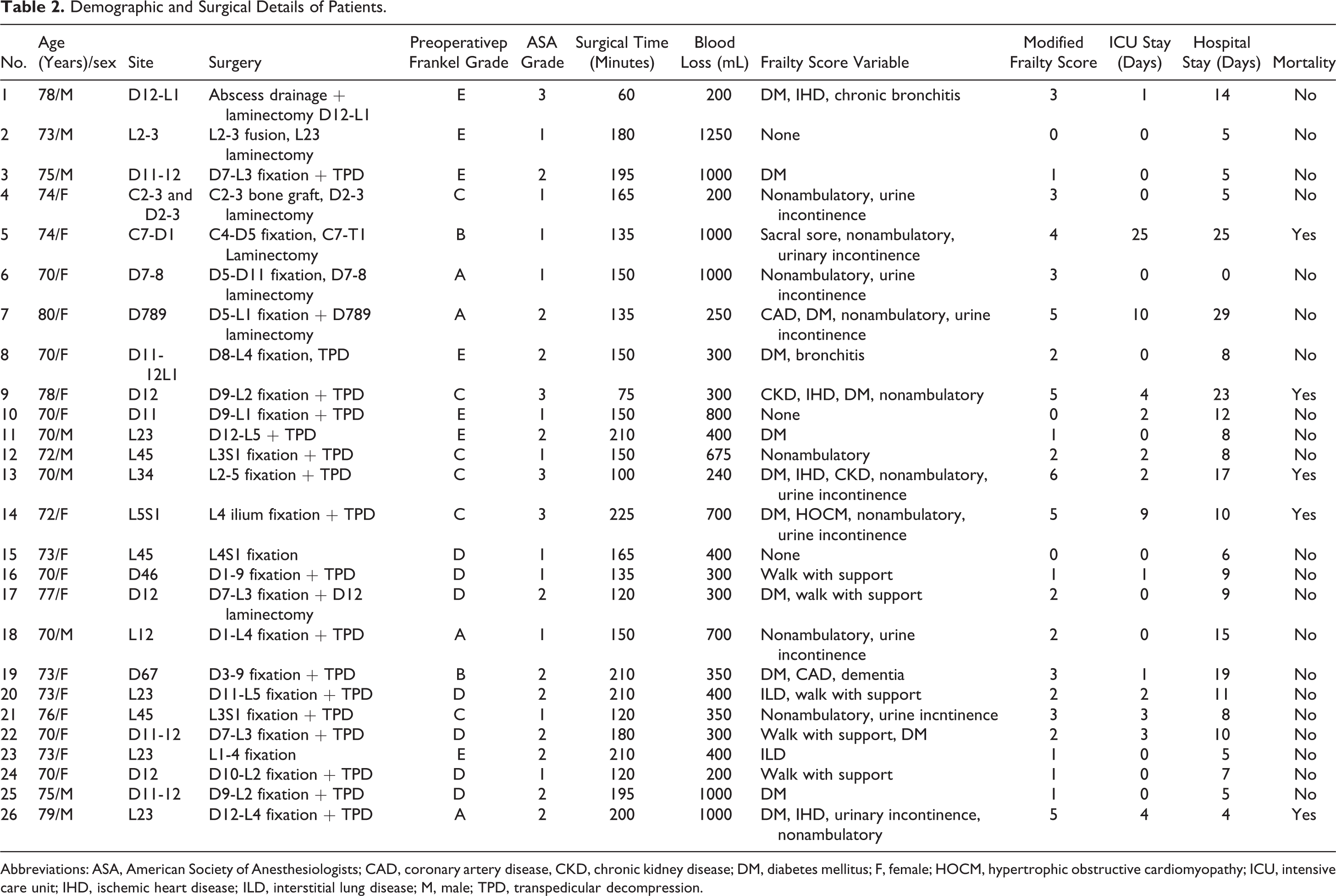
Abbreviations: ASA, American Society of Anesthesiologists; CAD, coronary artery disease, CKD, chronic kidney disease; DM, diabetes mellitus; F, female; HOCM, hypertrophic obstructive cardiomyopathy; ICU, intensive care unit; IHD, ischemic heart disease; ILD, interstitial lung disease; M, male; TPD, transpedicular decompression.
Patients were divided into 2 groups: those with postoperative 30-day mortality (M) and those who survived (S) and the aforementioned parameters were statistically tested. None of the patients had surgical complications requiring increase in hospital/ICU stay and causing mortality. There were no patients who refused surgery in the presence of indication for surgery.
Results
There were 26 patients including 9 males and 17 females. The average age was 73.2 years (range 70-80 years). There were 5 patients in the mortality group and 21 patients who survived. The preoperative neurology was Frankel A (4 patients), Frankel B (2 patients), Frankel C (6 patients), Frankel D (7 patients), and Frankel E (7 patients). The site of lesion, surgery performed, ASA grade, MFS, surgical time, blood loss, length of ICU stay, and length of hospital stay for each patient are shown in Table 2. Six variables including ASA grade, MFS, surgical time, blood loss, length of ICU stay, and length of hospital stay were statistically tested in the mortality and survived group as shown in Table 3. All patients were operated with posterior alone surgery except 1 patient (case 4) who was operated via anterior approach for cervical lesion.
Outcome Variables in the 2 Groups.
Abbreviations: ASA, American socirty of Anesthesiologists; ICU, intensive care units.
The value of MFS (P < .0001) and length of ICU stay (P = .001) was significantly higher and statistically significant in mortality group. Other parameters did not show statistically significant difference between mortality and survived group.
Discussion
“Frailty” is a multidimensional syndrome characterized by decreased physiological reserve, physical ability, and cognition and reduction in organ function putting the individual to be at risk due to surgical stresses. Frail patients are highly vulnerable to untoward postoperative outcome, which is seen by variable performance by same aged individuals. 8,9 Thus the assessment of “frailty” is critical in the elderly. The prevalence of frailty in older patients is well established in recent literature. 8 –10 The prevalence rates vary from 41.8% to 50.3% in several studies involving older patients undergoing cardiac and noncardiac surgery. Frailty affects short- and long-term morbidity and mortality. 8,10,11 The ideal assessment tool for frailty should help in risk stratification and to identify potential modifiable risk factors. Various tools have been described to assess frailty, which includes grip strength, gait speed, Edmonton frailty scale, comprehensive assessment of frailty score, and modified frailty index to name a few. 12
Predictive models for postoperative morbidity in spine surgery are scarcely discussed in literature. Hirose et al 13 studied validity of E-PASS scoring to predict morbidity after spine surgery. The E-PASS system is composed of a preoperative risk score, a surgical stress score, and a comprehensive risk score. They found it to be useful in predicting morbidity. However, the cohort included had undergone various types of surgeries (cervical laminoplasty/laminectomy, anterior cervical fusion, thoracic and lumbar disorders, scoliosis, etc) and had wide age presentation (8-88 years). Cusimano et al 14 presented a systemic review on causes of readmission within 30 days after neurosurgical spine procedures. They highlighted importance of patient related factors (age and comorbidities) associated with postoperative morbidity and readmission. ASA grades 15 and various comorbidity indices described in the literature 16,17 do not measure “frailty” of a patient with any comorbidities. Therefore, there arises a need for a frailty assessment tool in spine surgery especially in elderly who are prone to adverse outcomes.
MFS is a simple, easy, and reproducible system and comprehensively covers various factors affecting individual’s surgical performance. 7 Preoperative immobility has been shown as preoperative risk factor affecting postoperative mortality in elderly patients operated for tuberculosis. 18 Ambulatory status of the patient has been given special consideration in this scoring system. Thus, we used MFS for predicting frailty in our cohort of patients. Patel et al 7 successfully used MFS to predict mortality and morbidity in elderly patients undergoing surgery for fracture neck of femur.
Indications of surgery in spinal tuberculosis include progressive neurodeficit, profound deficit at presentation, or spinal instability which affects ambulation and daily activities. These patients are often subjected to prolonged bed rest causing muscle wasting, which plays a major role in frailty syndrome. The variables of ambulatory status and pressure sores in MFS signify muscle wasting and thus frailty. In our study, we found that MFS was significantly higher in patients with mortality and patients requiring ICU stay.
There were a few limitations in our study. This is a small cohort of patients; however, it can be attributed to the relatively less number of patients being operated upon at this age. Since this was a retrospective study, we had to depend on documented data for scoring, which might be inaccurate. This study was done in highly specific cohort and results could not be validated generally to any elderly undergoing spine surgery. However, MFS can be applied to other specific conditions like “frail” looking elderly requiring surgery for osteoporotic fractures with neurological involvement or degenerative scoliosis causing disability, and so on, in the future studies. Customized scoring system to assess frailty for patients undergoing spine surgery should be developed in future research.
Conclusion
We believe that MFS is a useful guide in predicting postoperative morbidity and mortality of elderly patients undergoing spine surgery for tuberculosis. Such scoring can help in better preoperative counseling of patients and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.