
Abstract
Study Design:
Retrospective cohort.
Objectives:
To validate the 11-item modified Frailty Index (mFI) as a perioperative risk stratification tool in elderly patients undergoing spine surgery.
Methods:
All consecutive cases of spine surgery in patients aged 65 years or older between July 2016 and June 2018 at a state-wide trauma center were retrospectively reviewed. The primary outcome was post-operative major complication rate (Clavien-Dindo Classification ≥ III). Secondary outcome measures included the rate of all complications, 6-month mortality and surgical site infection.
Results:
A total of 348 cases were identified. The major complication rate was significantly lower in patients with an mFI of 0 compared to ≥ 0.45 (18.3% versus 42.5%, P = .049). As the mFI increased from 0 to ≥ 0.45 there was a stepwise increase in risk of major complications (P < .001). Additionally, 6-month mortality rate was considerably lower when the mFI was 0 rather than ≥ 0.27 (4.2% versus 20.4%, P = .007). Multivariate analysis demonstrated an mFI ≥ 0.27 was significantly associated with an increased incidence of major complication (OR 2.80, 95% CI 1.46-5.35, P = .002), all complication (OR 2.93, 95% CI 1.70-15.11, P < .001), 6-month mortality (OR 7.39, 95% CI 2.55-21.43, P < .001) and surgical site infection (OR 4.43, 95% CI 1.71-11.51, P = .002). The American Society of Anesthesiologists’ (ASA) index did not share a stepwise relationship with any outcome.
Conclusion:
The mFI is significantly associated in a gradated fashion with increased morbidity and mortality. Patients with an mFI ≥ 0.27 are at greater risk of major complications, all-complications, 6-monthy mortality, and surgical site infection.
Introduction
The global elderly population is expected to double to 1.5 billion within the next 30 years. 1 Correspondingly, the overall number of patients aged 65 years and over undergoing surgical procedures is exponentially expanding.1-3 This has translated into an increasing number of spinal surgeries being performed in this vulnerable geriatric population.4,5 There is an urgent need for an objective and accurate pre-operative risk stratification tool to assess frailty and peri-operative risk to guide surgical decision making in this complex subgroup. 6 This is the first study evaluating the modified frailty index (mFI) as a risk stratification tool in elderly patients, defined by the United Nations as aged 65 years and older, undergoing spinal surgery. 7
Frailty is a state of decreased physiological reserve which has resisted universal definition due to its multi-dimensional nature. 8 It is a known independent predictor of increased post-operative morbidity and mortality across a broad range of surgical specialties.3,9,10 Historically, many frailty models have been developed to encapsulate the essence of this state of increased vulnerability. 11 The prevailing 2 diametrically opposed propositions are that of Fried et al who argue frailty is a phenotype composed of a decline in physiological parameters, while Rockwood et al posit that it is the result of an accrual of cumulative deficits.12,13 At their core, these frailty theorems are attempts to distill what clinicians intuitively deduce at the bedside into a quantitative variable along a continuum from frailty to robustness. 14 Various frailty instruments, such as the American Society of Anesthesiologists (ASA) Classification system and the Charlson Comorbidity Index (CCI) have delivered only partial success as pre-operative screening methods in the spine surgery population.15,16
The modified frailty index (mFI) mirrors the Rockwood model of cumulative deficit, with its 11 constituent variables comprising a unique combination of comorbidities. This frailty instrument was first validated by Leven et al in the adult spinal deformity cohort as an independent predictor of post-operative complications and mortality. 17 It has since been observed to be a statistically significant predictor of post-operative morbidity and mortality in specific cohort subgroups such as the extreme elderly population (80 years and older) undergoing spinal surgery by Kweh et al, anterior lumbar interbody fusion population by Phan et al, degenerative spine cohort by Flexman et al and general spine surgery group by Ali et al.18-21 The modified frailty index has also been shown to share a direct relationship with negative post-operative surgical outcomes. 21 However, there is still a need to evaluate and validate the modified frailty index in the general elderly population aged 65 years and over undergoing spinal surgery for any indication given this is an increasingly commonplace clinical scenario of everyday practice.
Methods
Study Hypothesis
In elderly patients aged 65 years and older undergoing spinal surgery, the mFI reliably encapsulates frailty with higher scores being associated with a greater likelihood of major complications, any complication, surgical site infection and mortality.
Study Design
The Alfred Hospital is a statewide Level 1 trauma center with a combined neurosurgery-orthopedic spine service. Following The Alfred Hospital and Ethics Research Committee approval (Approval Number 595/18) to proceed without informed consent given the preservation of patient anonymity, 2 authors (BK and HL) conducted a comprehensive retrospective review by independently extracting relevant baseline and outcome metrics. Discrepancies were resolved by consensus following discussion with a third party (JT). All instances of patients aged 65 years and above who underwent spinal surgery from July 2016 to June 2018 were included. Patients who underwent more than one surgery were recorded as separate encounters.
Patient demographic metrics extracted included age, sex, body mass index (BMI), smoking status, diagnosis type (degenerative, trauma, tumor or infection), American Society of Anesthesiologists (ASA) classification, modified frailty index variables and admission type (elective or emergency). Surgical metrics collected were region of spine involved, number of spinal motion segments, operative approach and length of surgery. The Clavien-Dindo classification system of complications was used to grade the severity of adverse events.22,23 The primary outcome measure was the occurrence of post-operative major complications, defined as Clavien-Dindo III or greater, consistent with existing literature.23,24 Secondary outcome measures included all complication rate, mortality within 6 months and surgical site infection rate. Surgical site infection was defined as a wound infection occurring up to 30 days post-operatively or within 12 months if spinal instrumentation was performed. 25
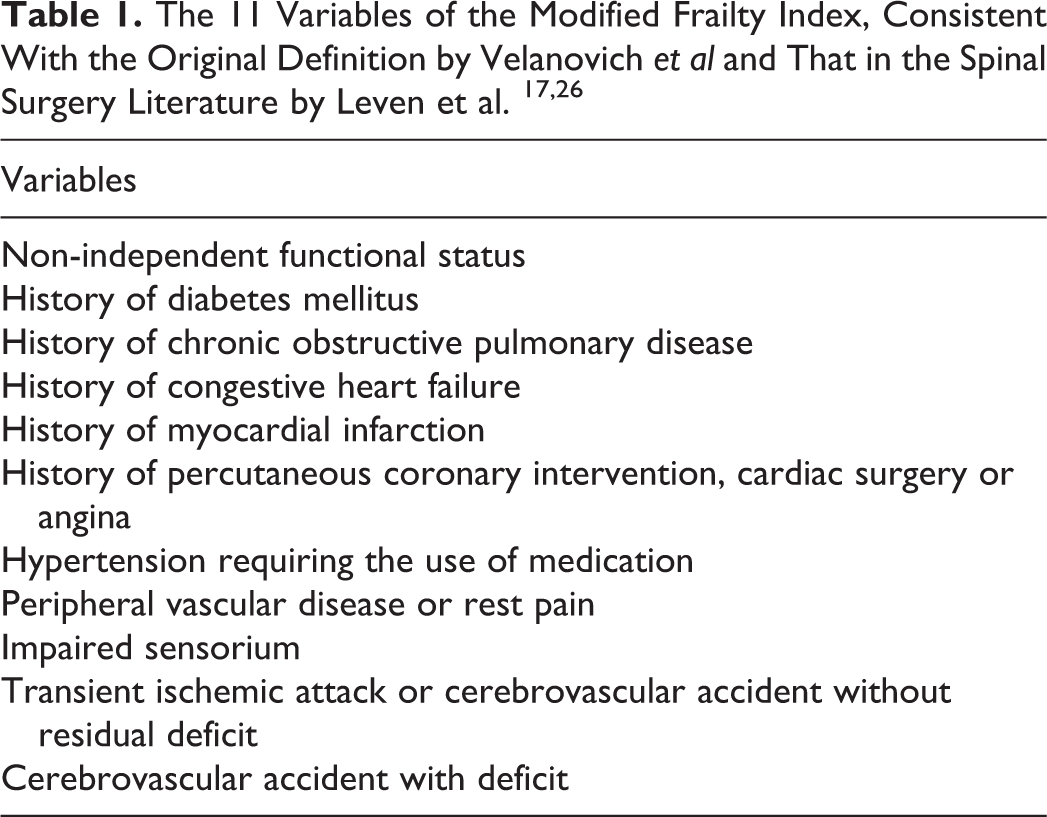
The modified frailty index is composed of 11 variables designed to encapsulate the overall robustness or frailty of a patient.17,26 The 11 constituent conditions, in keeping with the contemporary literature regarding the mFI, are listed in Table 1. 17,19,21 The index is calculated by dividing the number of variables present (n) by 11. A score of less than 0.27 (less than 3 of the 11 variables) was defined as robust. Patients attaining a score greater than or equal to 0.27 were defined as frail. This threshold was selected in accordance with the established literature evaluating the mFI in spinal surgery and other surgical disciplines.17,18,27
Statistical Analysis
Baseline demographic and surgical metric descriptive characteristics were collected. Categorical variables were analyzed with Pearson’s Chi-square test, while continuous variables were analyzed using the Mann-Whitney U test. The cohort was then dichotomized as either frail or non-frail with a threshold mFI of 0.27, and binary logistic regression was performed to determine if there was a statistically significant difference between the 2 groups with respect to the outcome measures. Best-fit models were constructed with the dependent variables being rate of major complications (Clavien-Dindo III or higher), all complication, 6-month mortality and surgical site infections. Stepwise backward regression was performed based upon the univariate P value of .20. Sensitivity analyses of different mFI thresholds was also performed to examine for a gradated increase in risk of primary and secondary outcomes as frailty indices increased. The association between the American Society of Anesthesiologists’ (ASA) score and the primary and secondary measures was also analyzed. Statistical significance was defined as a P-value <.05. STATA/IC version 14.2 (StataCorp, Texas, USA) was used to perform the analyses.
Results
Demographics
During the study period of 1st January 2016 to 30th June 2018, there were 348 instances of spinal surgery performed in patients aged 65 years or older. There was a slight predominance of male patients (59.4%) compared to female patients (40.6%). The mean age of the cohort was 73.7 ± 6.0 years (range 65-92), with a smoking rate of 11.4%. Importantly, there was an almost equal division between the elective cases (48%) and emergency operations (52%). The majority of the spinal surgeries performed were in those with a diagnosis of degenerative disease (63.6%). Other common indications of spinal surgery in this elderly population were trauma (20.0%), tumor (10.5%) and infection (5.9%). A posterior approach with instrumented fusion was the most common operative technique employed (42.6%), followed by posterior decompression without instrumentation (42.0%) and an anterior approach (15.7%).
Both the median and mode mFI score was 0.09, while the mean mFI was 0.16 ± 0.14. There were 71 patients (20.3%) with an mFI of 0, 103 (29.4%) with a score of 0.09, 80 (22.9%) with a score of 0.18, 45 (12.9%) with a score of 0.27, 29 (8.3%) with a score of 0.36 and 22 (6.3%) with a score of 0.45 or greater. Following stratification of the cohort by degree of frailty as assessed by the mFI, there was no statistically significant difference in sex, smoking status, BMI, diagnosis or admission type (Table 2). However, patients aged 80 years or older were more likely to register a higher mFI than their younger counterparts.
Preoperative Patient Demographics as Stratified by the Modified Frailty Index (mFI-11).
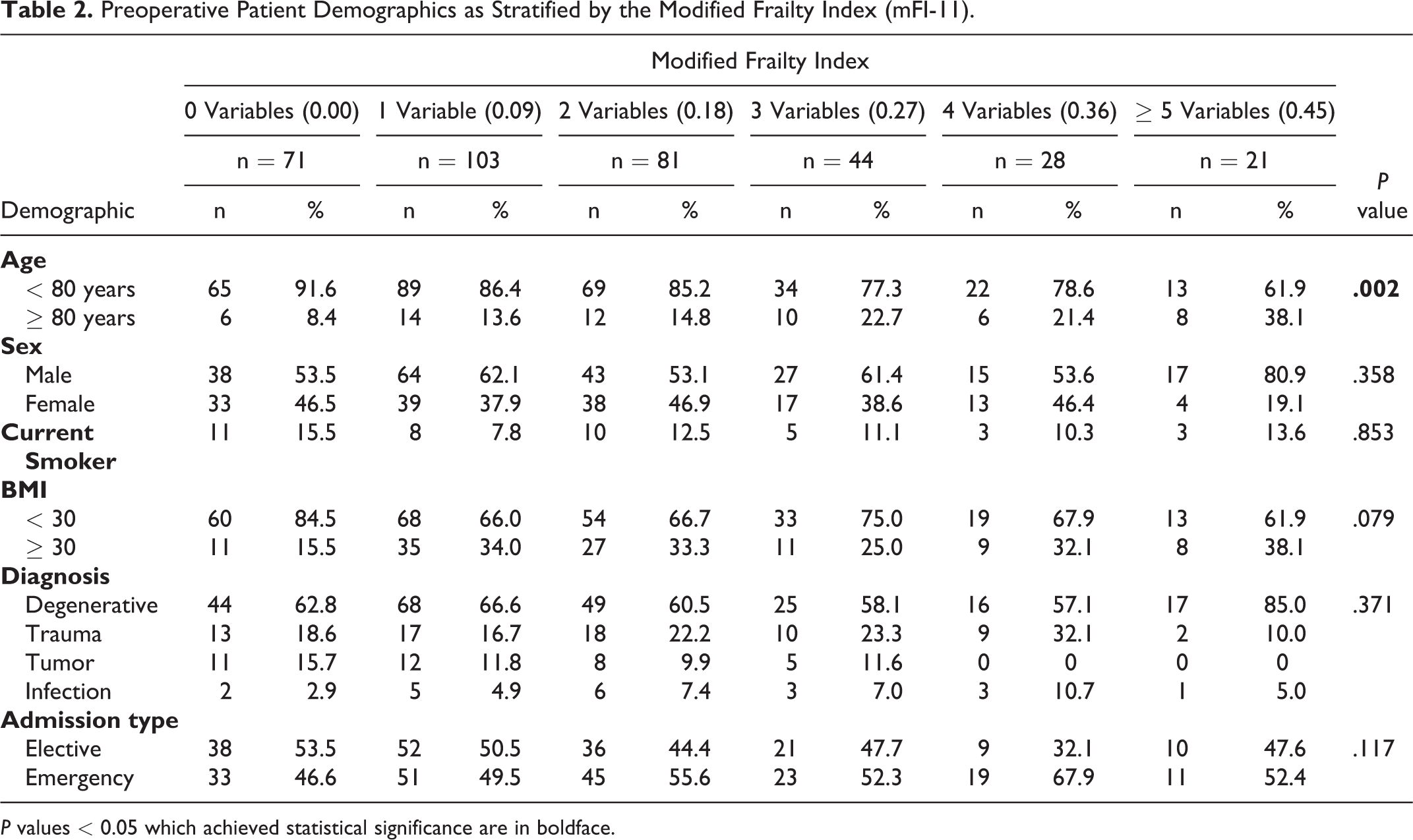
P values < 0.05 which achieved statistical significance are in boldface.
Surgical Metrics
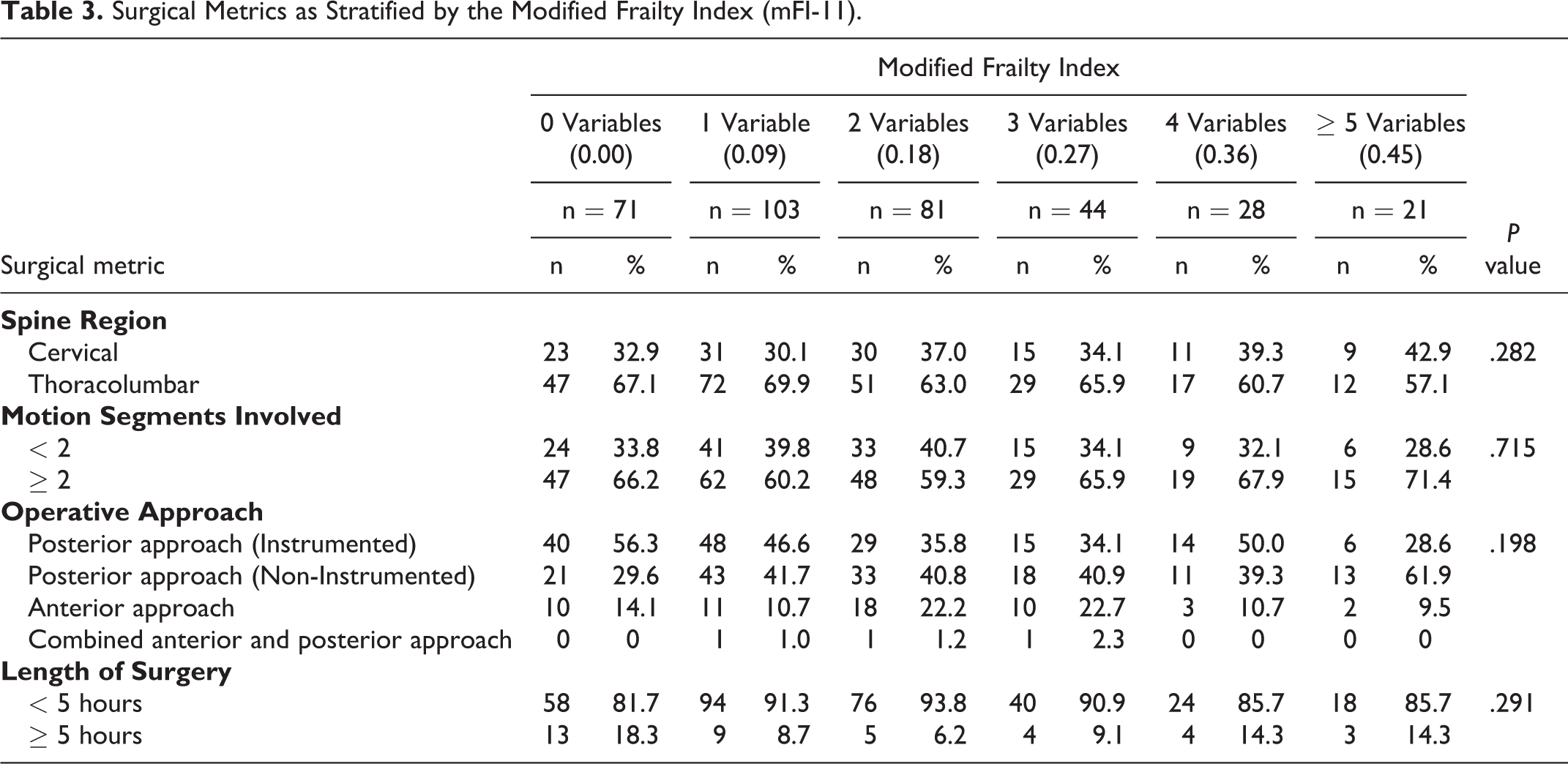
There was no statistically significant difference with respect to the following baseline surgical metrics across the mFI scores (Table 3): spine region (P = .282), number of motion segments involved (P = .715), operative approach either anterior or posterior (P = .198), or length of surgery (P = .291).
Surgical Metrics as Stratified by the Modified Frailty Index (mFI-11).
Post-Operative Surgical Outcome Metrics
As the mFI score increased from 0 to mFI = 0.36 and mFI ≥0.45, all complication rate also rose from 40.9% to 64.3% and 66.7% (P = .028) respectively. Importantly, the risk of major complications demonstrated a gradated increase from 18.3% to 22.7% as the mFI increased from 0 to 0.27, before almost doubling to 42.9% with an mFI ≥0.45 (P = .049). The rate of medical complications (P = .004) but not surgical complications (P = .468) demonstrated a statistically significant rise with the degree of frailty as stratified by the mFI (Table 4).
Postoperative Outcomes as Stratified by the Modified Frailty Index (mFI-11).
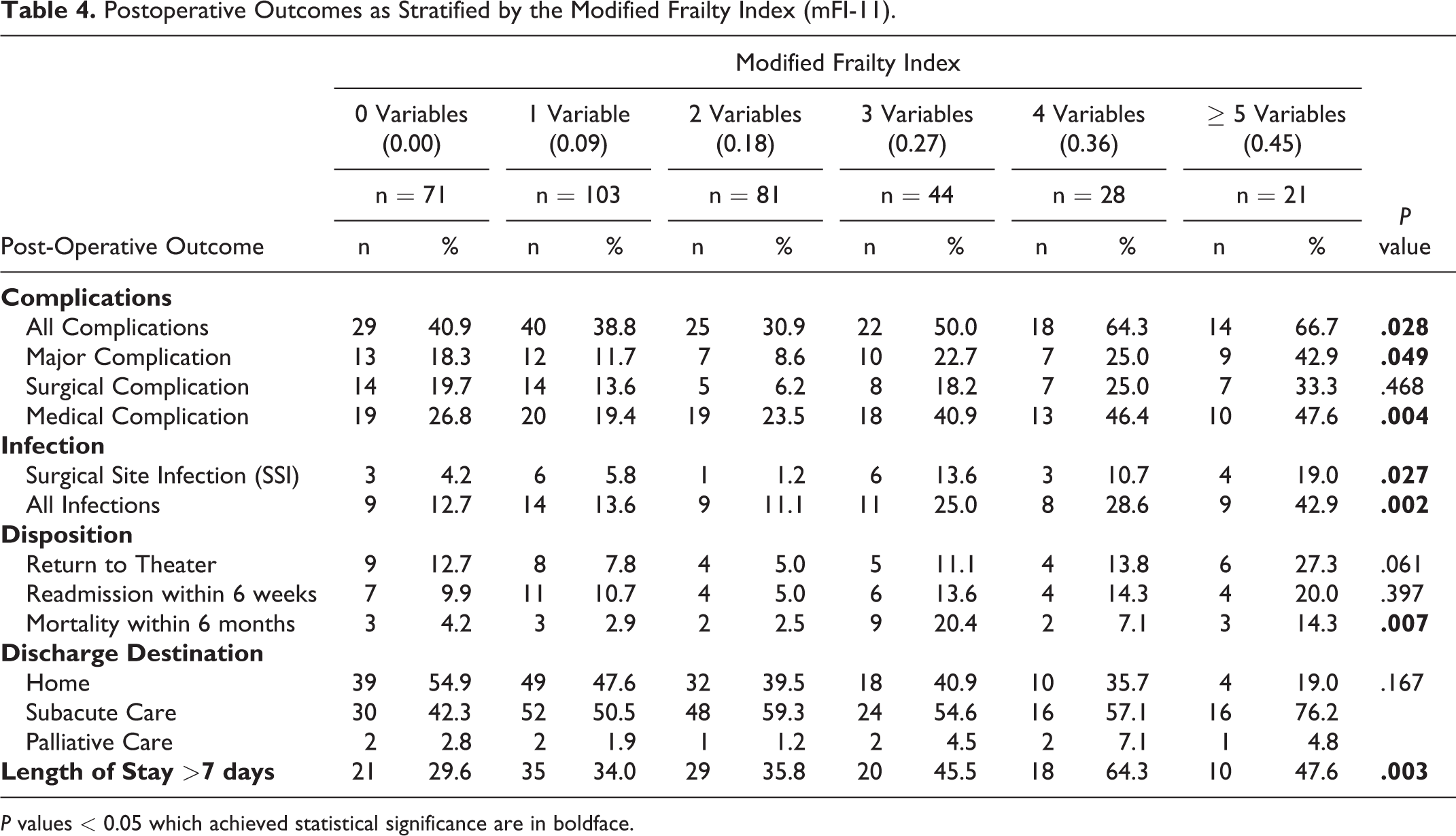
P values < 0.05 which achieved statistical significance are in boldface.
A higher frailty index was associated with a greater likelihood of surgical site infection (P = .027). The surgical site infection rate tripled from 4.2% when none of the frailty indices were present to 13.6% at an mFI of 0.27, before quadrupling to 19.0% when mFI ≥0.45 (P = .027). Additionally, the all infection rate (P = .002) exhibited a stepwise increase from 12.7% (mFI 0) to 25.0% (mFI = 0.27), before ascending to 42.9% (mFI ≥ 0). There was no significant difference across the mFI scores concerning return to theater rate (P = .061) or readmission within 6 weeks (P = .397). However, mortality rate within 6 months was predicted by higher mFI scores (P = .007): 4.2% when none of the mFI variables were satisfied, to 20.4% once 3 variables were present.
A higher modified frailty index score was also associated with a longer duration of admission (P = .003), with 29.6% of patients with zero mFI indices requiring greater than 7 days in hospital compared to 45.5% of those with 3 variables present. There was no statistically significant difference in discharge destination across the mFI spectrum (P = .167).
Independent Risk Factor of Post-Operative Outcomes
Age >80, smoking, BMI >30, emergency admission, posterior instrumented fusion procedure, cervical spine surgery (vs thoracolumbar spine), non-degenerative etiology (versus degenerative), number of spinal motion segment ≥2, albumin level <35 g/L and mFI or ASA score were incorporated into the multivariable model. Multivariate logistic regression analysis with a mFI cutoff of 0.27 was conducted (Table 5). Patients with an index less than 0.27 were deemed non-frail, and patients with an index equal to or greater than 0.27 designated frail in alignment with currently accepted definitions in the literature on mFI.17,18,27 Frailty with 3 or more variables of the mFI was an independent risk factor for all complications (OR 2.93, 95% CI 1.70-15.11, P < .001), major complications (OR 2.80, 95% CI 1.46-15.35, P = .002), surgical site infection (OR 4.43, 95% CI 1.71-11.51, P = .002) and mortality within 6 months (OR 7.39, 95% CI 2.55-21.43, P < .001).
Independent Predictors of Surgical Outcomes Identified With Multivariate Logistic Regression Analysis Stratified by the Modified Frailty Index (mFI-11).

P values < 0.05 which achieved statistical significance are in boldface.
An underlying diagnosis other than degenerative spinal disease was the most strongly associated factor with mortality within 6 months (OR 7.83, 95% CI 2.16-28.41, P = .002), and also conferred a poorer prognosis compared to degenerative diagnosis when determining all complication rate (OR 1.81, 95% CI 1.07-3.05, P = .027). Instrumented posterior fusion was also negatively related to major complications (OR 3.71, 95% CI 1.89-7.29, P < .001), all complications (OR 4.13, 95% CI 2.52-6.79, P < .001, surgical site infection (OR 4.74, 95% CI 1.46-15.42, P = .010) and mortality within 6 months (OR 3.87, 95% CI 1.13-13.28, P = .031).
Unsurprisingly, the subgroup of our elderly cohort aged over 80 years was at greater risk of mortality within 6 months (OR 7.16, 95% CI 2.37-21.61, P < .001).
Relationship of the mFI and ASA to Surgical Outcomes
The modified frailty index is linked to post-operative surgical outcomes in a gradated fashion (Table 6). There is a stepwise increase in rate of major complications from an odds ratio of 2.93 (95% CI 1.70-5.12, P < .001) at an mFI ≥0.27, rising to 3.21 (95% CI 1.54-6.70, P = .002) at a threshold of ≥0.36 and 6.07 (95% CI 2.20-16.76, P = .000) once an mFI ≥0.45 is achieved. In contrast, neither an ASA score of greater than 3 (P = .079) or 4 (P = .075) were statistically significant associations.
Dose-Response Relationship of Modified Frailty Index (mFI-11) and American Society of Anesthesiologists’ Score With Surgical Outcomes.
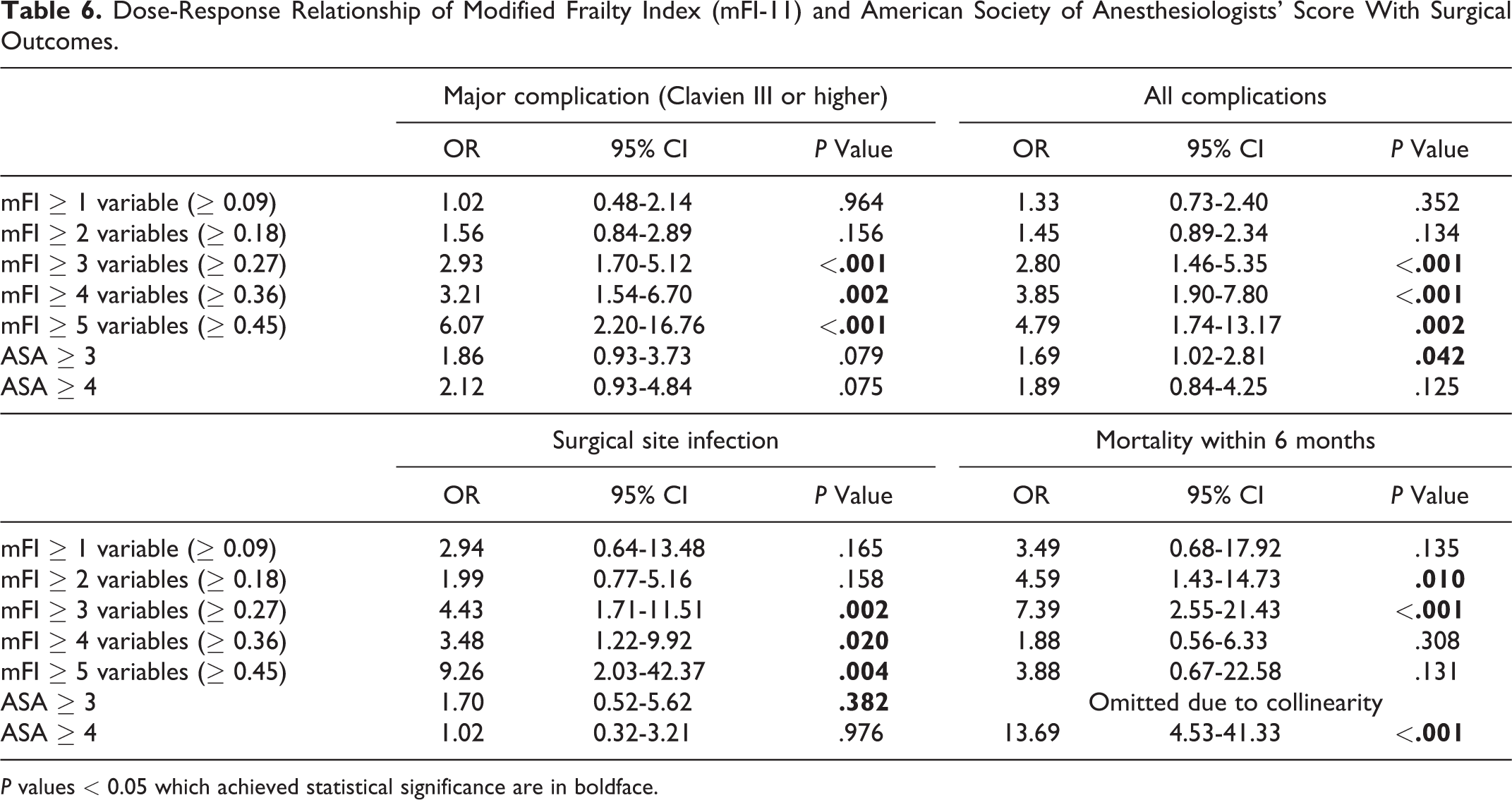
P values < 0.05 which achieved statistical significance are in boldface.
This finding continues when attempting to stratify incidence of all complications following spinal surgery. An mFI ≥0.27 carries a risk ratio of 2.80 (95% CI 1.46-5.35, P < .001) which rises in a stepwise manner to 3.85 (95% CI 1.90-7.80, P < .001) when mFI ≥ 0.36 and 4.79 (1.74-13.17, P = .002) when the mFI rises above 0.45. Similarly, an elderly patient who satisfies 5 variables of the mFI has an odds ratio of 9.26 of surgical site infection (95% CI 2.03-42.37, P = .004), compared to OR 4.43 (95% CI 1.71-11.51, P = .002) if only 3 variables are present. The ASA score was not associated with all complication rate in a stepwise fashion incidence (Table 6).
The incidence of mortality within 6 months rises from OR 4.59 (95% CI 1.43-14.73, P = .010) to OR 7.39 (95% CI 2.55-21.43, P < .001) as the mFI rises from greater than 0.27 to 0.36 (Table 6). The ASA score as a predictor of mortality had to be omitted due to collinearity during the multivariate analysis.
Discussion
An increasing number of elderly patients are undergoing spinal surgery despite 25-40% of them exhibiting frailty, a reversible and dynamic state of decreased physiological reserve.4,5,8,28 This trend reflects the belief that appropriate spinal surgery significantly improves the functional status and quality of life in the elderly, while simultaneously being equally as cost effective as surgery in younger patients.29-31 Accurate and efficient peri-operative risk stratification of surgical patients has been demonstrated to improve post-operative outcomes, reduce complication rate and increase patient satisfaction.20,32 However, previous scoring frailty indices in this elderly spinal cohort have been problematic. 33
For example, the detailed 70-item Canada Study of Health and Aging Frailty Index has been statistically validated, but its lengthy nature is likely to preclude its daily use by clinicians.17,34 Other indirect markers of frailty such as gait speed or grip strength are subject to fluctuation at time of assessment, as well as inter-observer variability.35,36 The 11-item modified frailty index represents an objective tool that was developed by Velanovich et al and has been advocated by Moskven et al as a pragmatic means for assessing frailty in the spinal surgery population.6,26 This analysis is the first to demonstrate that in an elderly cohort undergoing spinal surgery for any indication, the modified frailty index is associated with increased post-operative morbidity and mortality incidence.
Our validation of the mFI in the elderly cohort undergoing spinal surgery is important given the current controversial literature regarding its utility in other specialties. Banaszek et al found that the mFI predicts length of stay and mortality in patients with traumatic spinal cord injury only in those aged less than 75 years but not in the elderly beyond this. 27 Similarly, Charest-Morin et al determined that the mFI failed to predict acute care complications in elderly patients, defined as aged 65 years and over, who were undergoing elective non-complex surgery for degenerative spine disease. 37 Finally, Bourassa-Moreau et al concluded that sarcopenia, but not the modified frailty index, was a predictor of post-operative adverse events. 38
However, the mFI has been found to be a successful predictor of 30 day morbidity and mortality in populations undergoing spinal surgery for adult spinal deformity by both Leven et al, and in the general spinal surgery group by Ali et al.17,18 Furthermore, this frailty tool has recently been validated as a preoperative assessment tool in the elderly population aged 80 years and older undergoing spinal surgery of any kind. 21 In this cohort at the extreme of age, the mFI was demonstrated to be an independent predictor of major complications, all complications and surgical site infection but also correlated in a stepwise fashion with increasing hazard risk. 21 It was evident from the aforementioned contradictory evidence that there was an urgent need for clarification regarding the role of the mFI in the evaluating the general elderly population, aged 65 years and over, undergoing spinal surgery for all indications. This study’s findings provide support for mFI scoring and subsequent risk-stratification.
Indeed, we determined that patients who scored an mFI ≥0.27 were subject to an almost 3 times greater rate of major complication (OR 2.80, 95% CI 1.46-5.35, P = .002) or any complication (OR 2.93, 95% CI 1.70-1.5.11, P < 0.001). The risk of death was also more than 7 times greater (OR 7.39, 95% CI 2.55-21.43, P < .001). This frailty instrument therefore may be useful in counseling pre-operative elderly patients awaiting spinal surgery.
Indeed, the mFI may function as an initial screening pre-operative instrument and also a risk quantification tool given its association with major post-operative complication in a gradated fashion. For example, an mFI of 0.09 is associated with a low incidence of major post-operative complication (OR 1.02, 0.48-2.14). A rapid rise in complication rates were observed with an index of 0.36 (OR 3.21, 95% CI 1.54-6.70) and doubled at an mFI of 0.45 (OR 6.07, 95% CI 2.20-16.7). The stepwise relationship continues when the mFI is used to stratify all complication risk, escalating from an odds ratio of 2.80 (95% CI, 1.46-5.35) at an mFI of 0.27 to 4.79 (95% CI, 1.74-13.17) with an mFI of 0.45.
Several complex risk stratification tools already exist and could be employed in specific circumstances by the spinal surgeon. For instance, use of the index developed by Passias et al specifically for cervical surgery, the tool validated by Shaw et al in those awaiting lumbar surgery and that by Ahmed et al in spinal tumors.39-41 Unfortunately, it remains unclear if these historical tools are still valid as screening instruments in the elderly population. On the other hand, this study demonstrates to clinicians that the mFI is a simple and clinically applicable tool for stratifying complication rates in the general elderly cohort undergoing spinal surgery.
This tenet is consistent with the way in which the mFI is applied in other surgical specialties. Adams et al found it useful in predicting all complications and life-threatening complications in a cohort of patients who underwent head and neck surgery. 42 Additionally, Karam et al noted its reliability as a predictor of adverse events in the vascular surgery field, while Farhat et al successfully utilized the mFI in a general surgery setting.43,44 What these preceding studies suggest is that the modified frailty index is a valid screening tool which, when applied across a broad range of surgeries, finds its own balance and statistical validity. Indeed, when Velanovich et al first formulated the 11 variable modified frailty index from the NSQIP database, they intended for its universal use in all surgical patients irrespective of specialty. 26 We propose that the mFI should be applied widely rather than as a specific sub-specialty tool as has been recently seen.13,27,37,38
For this particular elderly subgroup, the alternative risk stratification system of the ASA score was not a statistically significant predictor of longer-term post-operative surgical outcomes. The ASA classification system has previously been evaluated and deemed a useful short-term predictor of 48-hour post-operative mortality risk by Hopkins et al, or even 30-day mortality risk by Pateder et al. However, the ASA did not correlate in a stepwise fashion with the rate of major complications, all complications, surgical site infection or 6-month mortality risk in our study.45,46
Beyond its use in risk stratification, the mFI may also identify candidates who may benefit from pre-operative optimization.47,48 Chan et al highlighted that it is vital to recognize that frailty is a modifiable and potentially reversible state with appropriate peri-operative intervention. 49 This is reflected within the 11-item modified frailty index by several dynamic variables, such as hypertension requiring the use of medication or non-independent functional status. A holistic approach to improving frailty status, ranging from nutritional to cognitive techniques, has been shown to be of benefit in the elderly population. 50 Improved mobility leading to independent function, or even dietary changes with reduced sodium intake resulting in excellent non-pharmacological management of hypertension, are modifiable risk factors which could be improved prior to spinal surgery. This is well supported by de Labra et al, who concluded in their comprehensive systematic review that physical exercise interventions even in the frail elderly were likely to be of benefit. 51
The accuracy of the mFI in assessing frailty importantly also assists in identifying patients who may benefit from post-operative enhanced recovery after surgery (ERAS) protocols. Implementation of these standardized recovery plans has been demonstrated in the spine surgery population to accelerate functional recovery and decreased post-operative morbidity.52,53 This study’s findings may assist clinicians in both pre-operative assessment and optimization as well as post-operative management of the frail.
A strength of this study is the large sample size that provided adequate statistical power. A robust study design with well-defined inclusion criteria for patients within our retrospective review also lent a substantial sense of internal validity. The selection criteria was broad and inclusive of all patients undergoing any form of spinal surgery in order to impart a degree of external validity. Our statistical analysis was also based upon an original dataset of a contemporary cohort of patients, rather than a pre-existing population who may have been subjected to outdated surgical techniques. On the other hand, the retrospective nature of our study is a weakness. Additionally, all patients were recruited from a single center. Future studies would benefit from a prospective multi-center design to further evaluate the utility of the modified frailty index in both a general and subgroup setting.
Conclusion
The modified frailty index is strongly associated in a gradated fashion with increased post-operative morbidity and mortality in the elderly population aged 65 years and older undergoing spinal surgery. There is a significantly higher incidence of major complications, all-complications and surgical site infection if patients possess an mFI ≥ 0.27. We have demonstrated that the mFI is a valuable objective tool which can be used by clinicians to guide peri-operative decision making and risk stratification in this especially vulnerable cohort.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.