
Abstract
Study Design
Retrospective Cohort
Objectives
To validate the most concise risk stratification system to date, the 5-item modified frailty index (mFI-5), and compare its effectiveness with the established 11-item modified frailty index (mFI-11) in the elderly population undergoing posterior instrumented spine surgery.
Methods
A single centre retrospective review of posterior instrumented spine surgeries in patients aged 65 years and older was conducted. The primary outcome was rate of post-operative major complications (Clavien-Dindo Classification ≥ 4). Secondary outcome measures included rate of all complications, 6-month mortality and surgical site infection. Multi-variate analysis was performed and adjusted receiver operating characteristic curves were generated and compared by DeLong’s test. The indices were correlated with Spearman’s rho.
Results
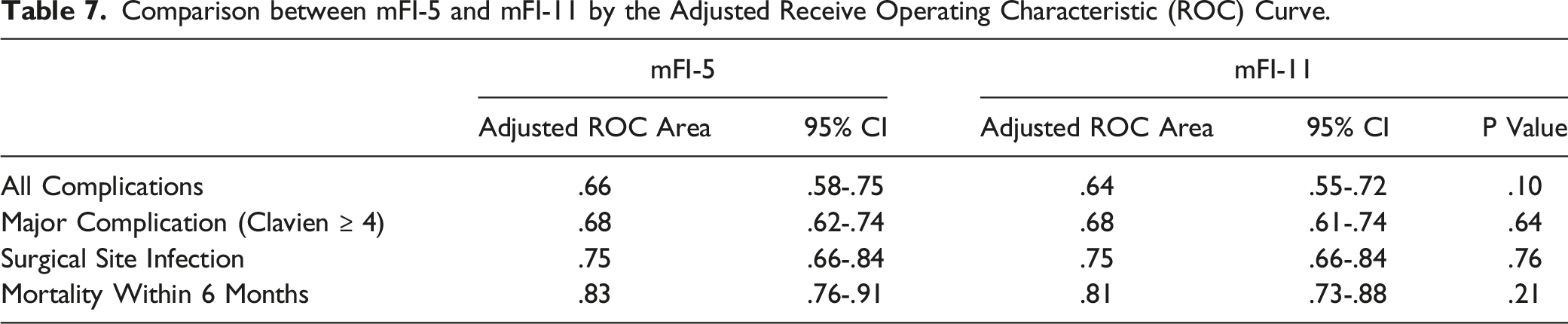
272 cases were identified. The risk of major complications was independently associated with both the mFI-5 (OR 1.89, 95% CI 1.01-3.55, P = .047) and mFI-11 (OR 3.73, 95% CI 1.90-7.30, P = .000). Both the mFI-5 and mFI-11 were statistically significant predictors of risk of all complications (P = .007 and P = .003), surgical site infection (P = .011 and P = .003) and 6-month mortality (P = .031 and P = .000). Adjusted ROC curves determined statistically similar c-statistics for major complications (.68 vs .68, P = .64), all complications (.66 vs .64, P = .10), surgical site infection (.75 vs .75, P = .76) and 6-month mortality (.83 vs .81, P = .21). The 2 indices correlated very well with a Spearman’s rho of .944.
Conclusions
The mFI-5 and mFI-11 are equally effective predictors of postoperative morbidity and mortality in this population. The brevity of the mFI-5 is advantageous in facilitating its daily clinical use.
Introduction
The elderly population, aged 65 years and older, continues to burgeon and is expected to more than double from 703 million in 2019 to 1.5 billion in 2050. 1 This has been accompanied by an increase in the overall incidence of more complex spinal surgeries including instrumentation and fusion. 2 More than this, the greatest surge in these operations is in fact occurring in the elderly population.3,4 Importantly, our study determined that the majority of admissions for these operations were emergency in nature rather than elective. This may in part be explained by the fact that traumatic spinal cord injury peaks in males between the ages of 20-29 and again in those aged over 70 years. 5 Hence, it is essential that an instantaneous easily accessible and validated pre-operative risk stratification tool is readily available to clinicians to rapidly assess this vulnerable but expanding geriatric cohort. 6
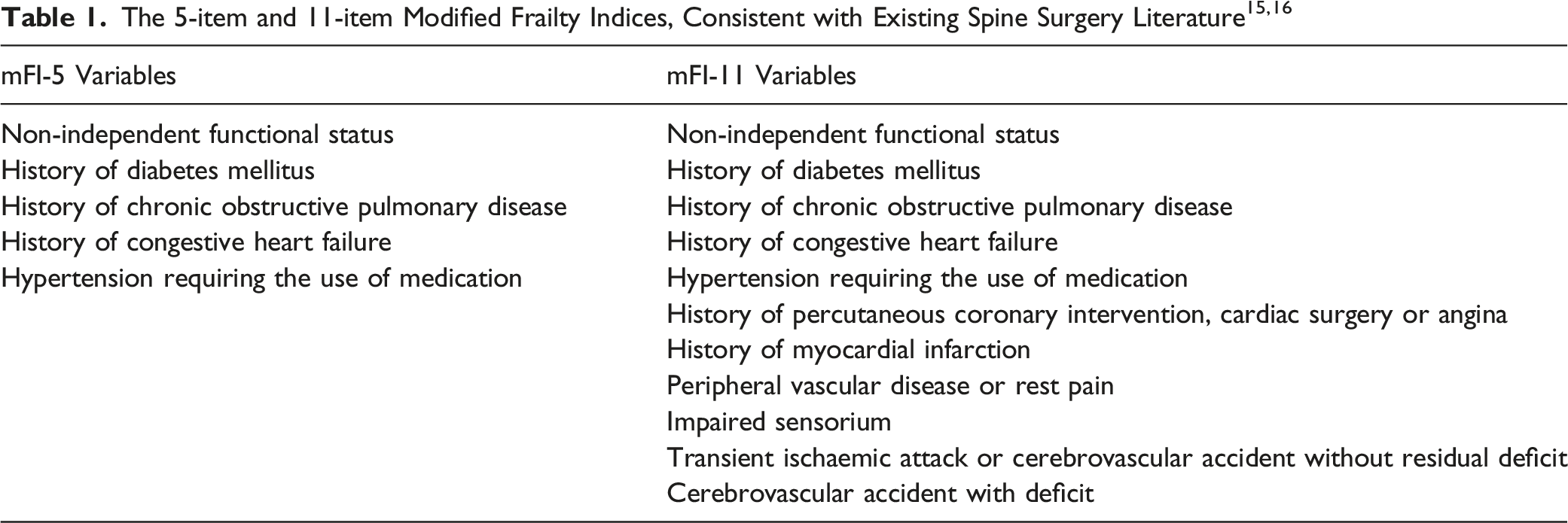
Amitkumar et al argued that age itself should not be used as the sole factor in determining fitness for surgery. 7 Instead, frailty as a universally accepted state of decreased physiological reserve, has been demonstrated to be an independent predictor of adverse post-operative morbidity and mortality.8,9 Despite many historical indices attempting to distill the essence of frailty into a single scoring index or figure, there has only been partial success in applying the use of these clinical indices to everyday practice.10-12 For example, the 70 item National Surgical Quality Improvement Program (NSQIP) score contained so many variables that its daily use would likely have been precluded by its impractical length. 13 An alternative model is the 11-item modified frailty index originally introduced by Velanovich et al which has been validated in the spinal surgical population, but still remains rather lengthy and cumbersome to calculate.6,14 Our unique validation of the most concise model to date that encapsulates the essence of frailty, the accessible 5-item modified frailty index, is timely and addresses this urgent need for the first time.
Methods
Study Hypothesis
Study Design
All consecutive cases of posterior instrumented spine surgery in patients aged 65 years and older were identified from July 1, 2016 to June 30, 2018 at a single state-wide tertiary centre. After approval from the Alfred Hospital institutional review committee (Approval Number 595/18), 2 authors (B.T.S.K and H.Q.L) independently collected all relevant patient and surgical outcome demographics. Inconsistencies were resolved by consensus mediated by a third party (J.W.T). The 5-item and 11-item modified frailty indices were calculated in keeping with existing spine surgery literature.13,15,16 The mFI-5 is more simply derived with every positive variable being assigned a score of 1. Conversely, the mFI-11 is calculated by dividing the number of positive variables by 11. 16 The severity of post-operative complications was stratified by the Clavien-Dindo classification system.17,18 The primary outcome measure was the occurrence of a major complication (Clavien-Dindo IV or greater).18,19 Secondary outcome measures included the rate of any complication, 6 month mortality and surgical site infection rate. Given all patients in our cohort possessed spinal instrumentation in situ, surgical site infection was defined as occurring within 12 months of the initial operation. 20
Statistical Analysis
Baseline demographic and surgical metric descriptive characteristics were collected. Our cohort was subdivided into non-frail (mFI-5 = 0 or mFI-11 = 0), pre-frail (mFI-5 = 1 or mFI-11 = .09 or .18) and frail (mFI-5 ≥ 2 or mFI-11 ≥ .27) groups.15,21 Categorical variables were compared with the Pearson’s Chi-square test. Multivariate logistic regression analysis was performed for both the mFI-5 and mFI-11. Covariates were predetermined prior to analysis and selected based upon previous studies. These included frailty as defined by mFI-5 ≥ 2 or mFI-11 ≥ .27, BMI ≥ 30, emergency admission, indication for non-degenerative disease or operations at greater than 2 motion levels. The effectiveness of the more concise mFI-5 was then compared to the mFI-11 using the concordance statistic (c-statistic), or area under the receiver operating characteristic (ROC) curve. Statistical significance was defined as a P-value < .05. All analyses were conducted with STATA/IC version 14.2 (StataCorp, Texas, USA).
Results
Patient Demographics
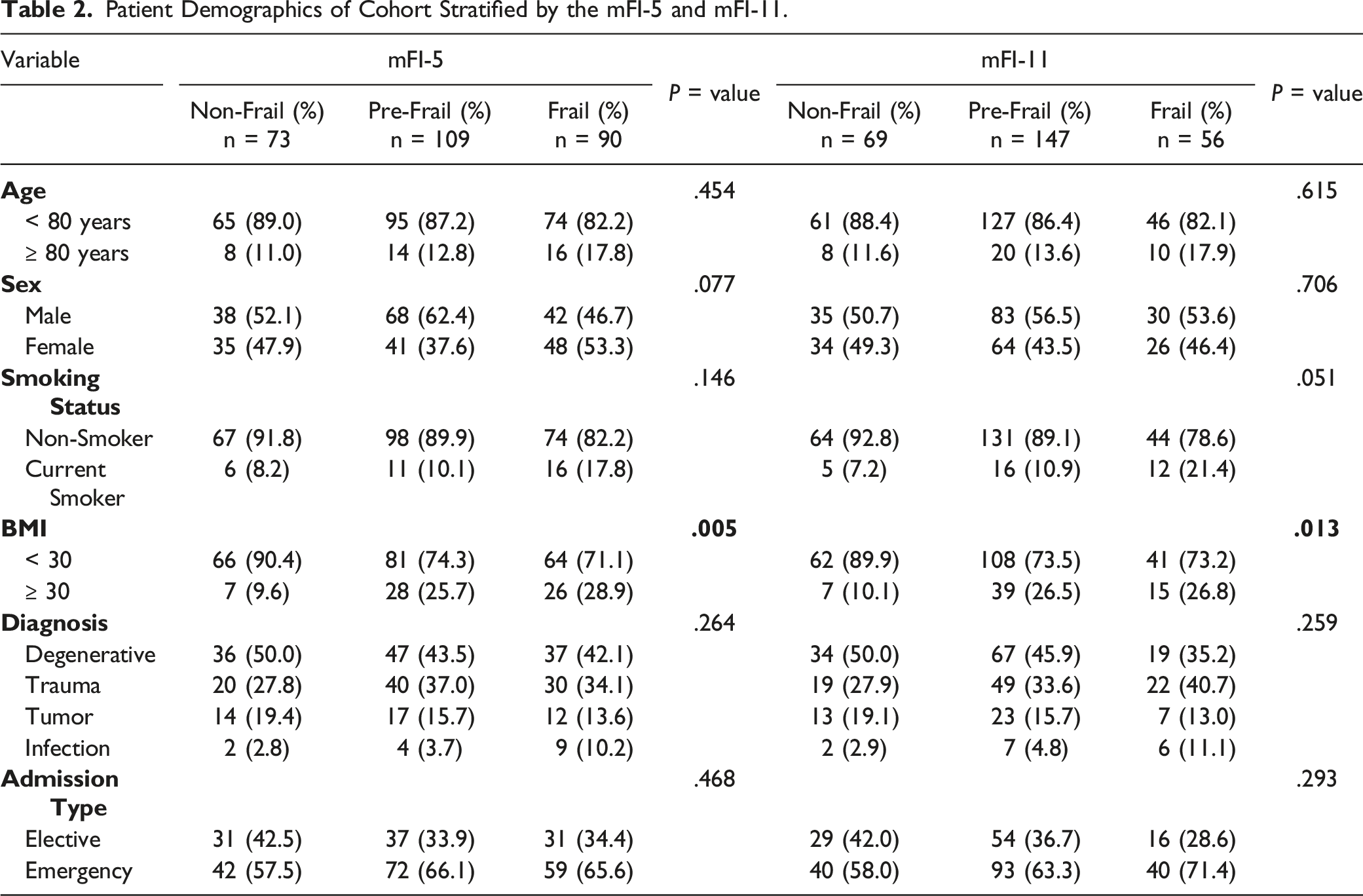
There were 272 cases of posterior instrumented spinal surgery during our study period. The mean age of the cohort was 73.5 ± 5.7 years. There was a slight preponderance of male (54.4%) over female patients (45.6%). With an average BMI of 27.9 ± 6.2, only 12.1% were smokers. The majority of posterior instrumented cases were performed for degenerative disease (44.1%) followed by trauma (33.1%), tumor (15.8%) and infection (1.5%). Emergency admissions (63.6%) were more common than elective ones (36.4%). More than half of this elderly cohort experienced a complication (54.8%), but only 19.5% suffered a major complication. More specifically, 17.3% were noted to have a surgical complication and 32.7% succumbed to a medical complication. The rate of any infection was 23.5%, whilst that of surgical site infection was 8.5%. The readmission rate within 6 weeks was 9.2%, and the 6-month mortality rate was 9.2%.
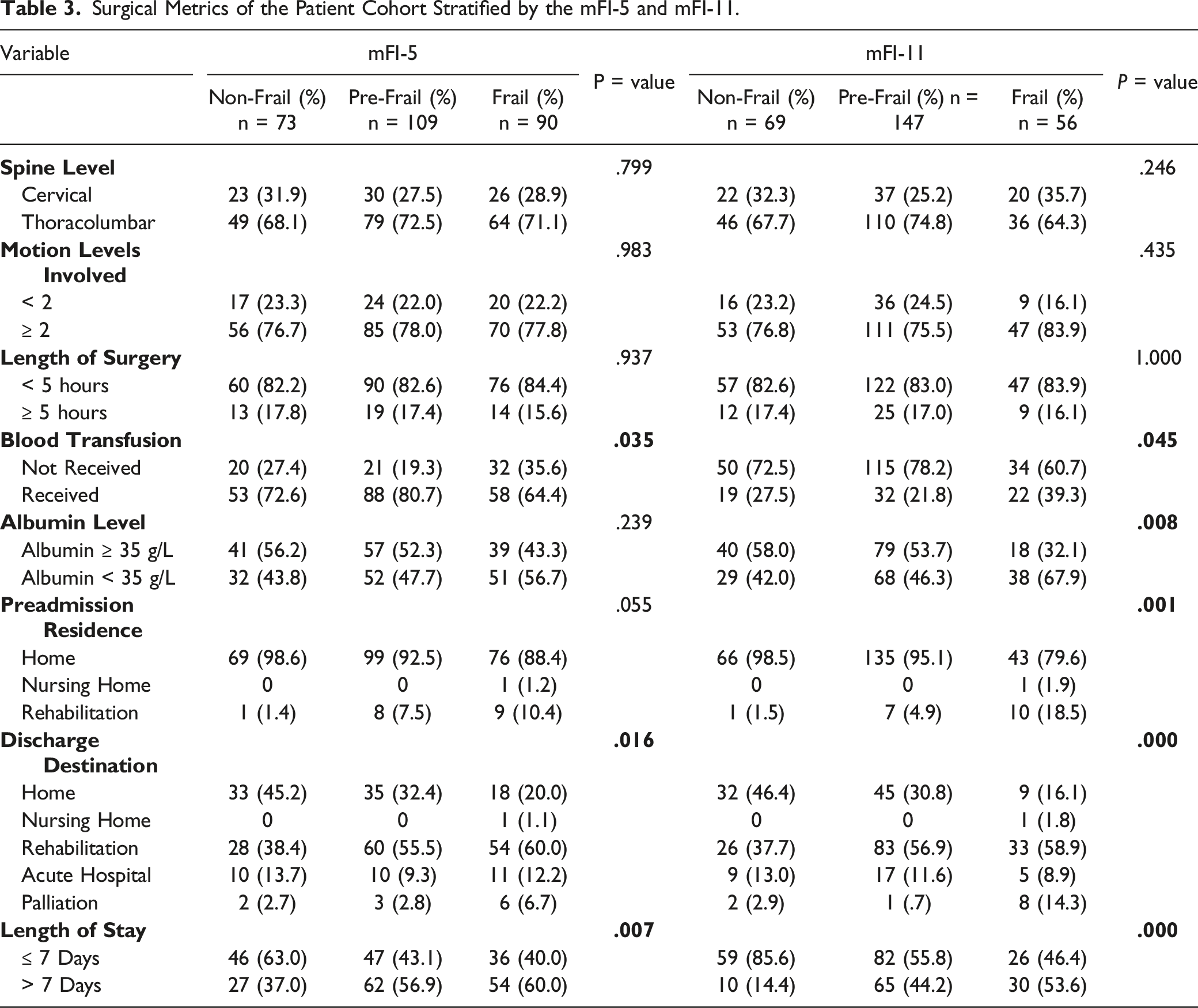
The thoracolumbar spine (70.6%) was more commonly instrumented than the cervical region (29.0%). Constructs often spanned more than 2 motion levels (77.6%) rather than less than 2 (22.4%). Despite this, length of surgery was usually less than 5 hours (83.1%). Interestingly, there was rather liberal use of blood transfusions (73.2%). Patient’s baseline albumin level was almost equally as likely to be greater than ≥ 35 g/L (50.4%) than < 35 g/L (49.6%). The majority of patients were overwhelming admitted from home (89.7%) rather than rehabilitation (18, 6.6%) or a nursing home (1, .4%). Length of stay was usually greater than 7 days (52.6%). The most common discharge destination was rehabilitation (52.2%), followed by home (31.6%), an acute hospital (11.4%), palliation (4.0%) or a nursing home (.4%).
Baseline Demographics Stratified by the mFI-5 and mFI-11
Patient Demographics of Cohort Stratified by the mFI-5 and mFI-11.
Surgical Metrics Stratified by the mFI-5 and mFI-11
Surgical Metrics of the Patient Cohort Stratified by the mFI-5 and mFI-11.
Association of mFI-5 and mFI-11 Frailty Scores with Primary and Secondary Outcomes
Post-Operative Surgical Outcomes Stratified by the mFI-5 and mFI-11.
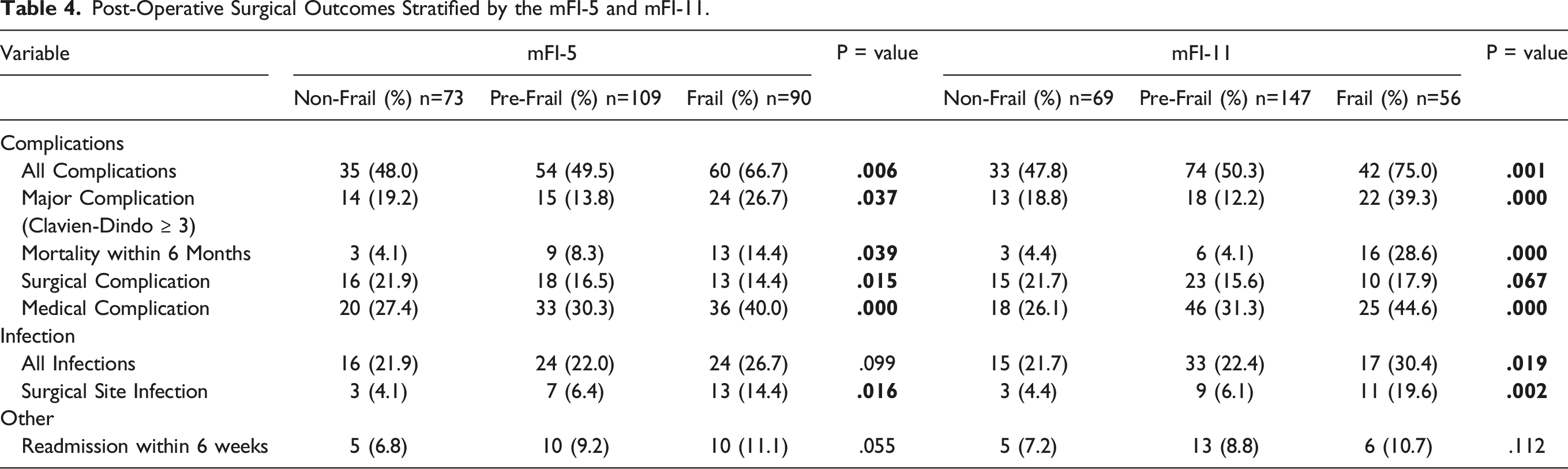
A similarly strong statistically significant association was observed when stratifying the cohort with the mFI-11. Non-frail patients were at much lower risk of any complication (47.8%) compared to those designed as pre-frail (50.3%) or frail (75.0%, P = .001). Continuing this trend, higher mFI-11 scores was also associated with greater risk of major complications (P = .000). There was also a 7 times higher chance of mortality within 6 months if a patient was frail (28.6%) rather than pre-frail (4.1%) or non-frail (4.4%, P = .000). The rate of surgical complications (P = .067) and medical complications (P = .000) also correlated in a gradated fashion with escalating frailty index scores. Finally, the rate of all infections was also much greater in frail rather than non-frail patients (30.4% vs 21.7%, P = .019). This trend held true with respect to surgical site infection, with frailty again portending poorer outcomes (19.6%) as opposed to pre-frail (6.1%) or non-frail (4.4%, P = .002). The mFI-11, much like the mFI-5, was not associated with readmission within 6 weeks (P=.112).
Multivariate Analysis of Demographics and Index Scores
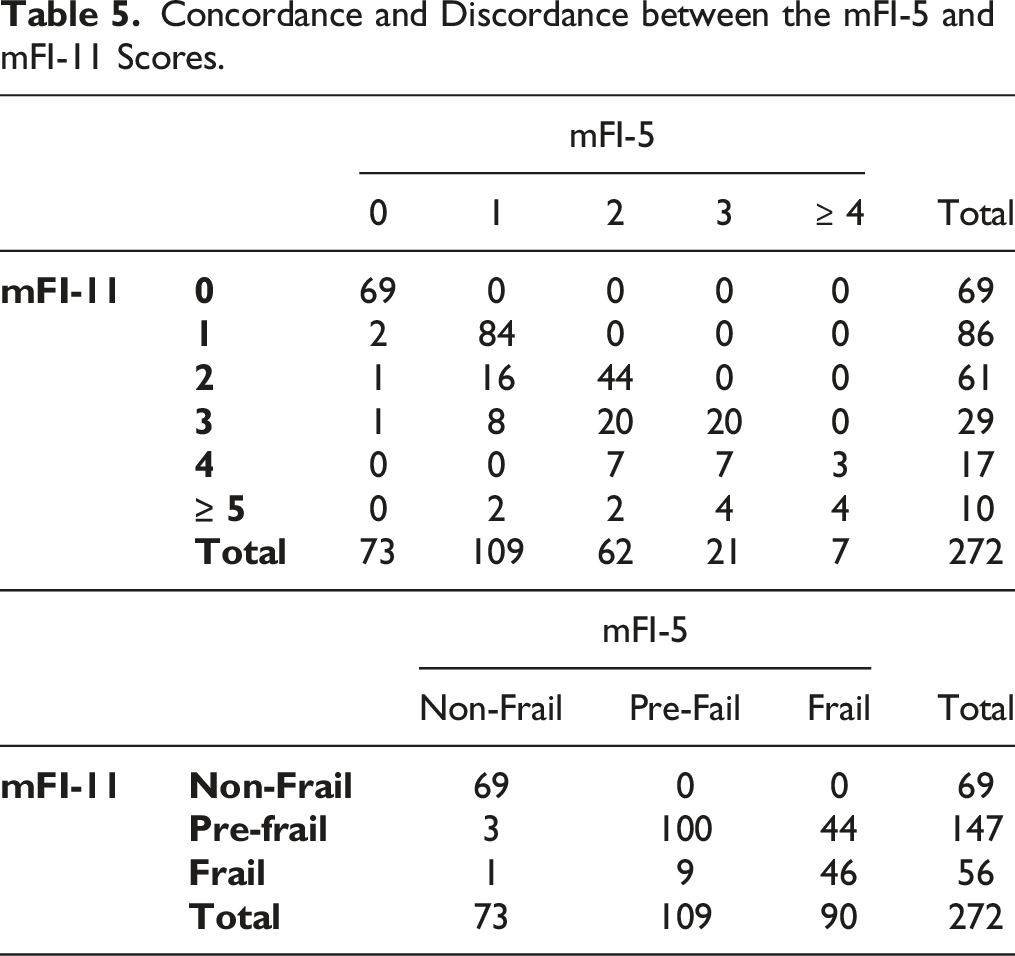
Concordance and Discordance between the mFI-5 and mFI-11 Scores.
Independent Risk Factors of Surgical Outcomes Identified with Multivariate Logistic Regression Analysis as stratified by the mFI-5 and mFI-11.
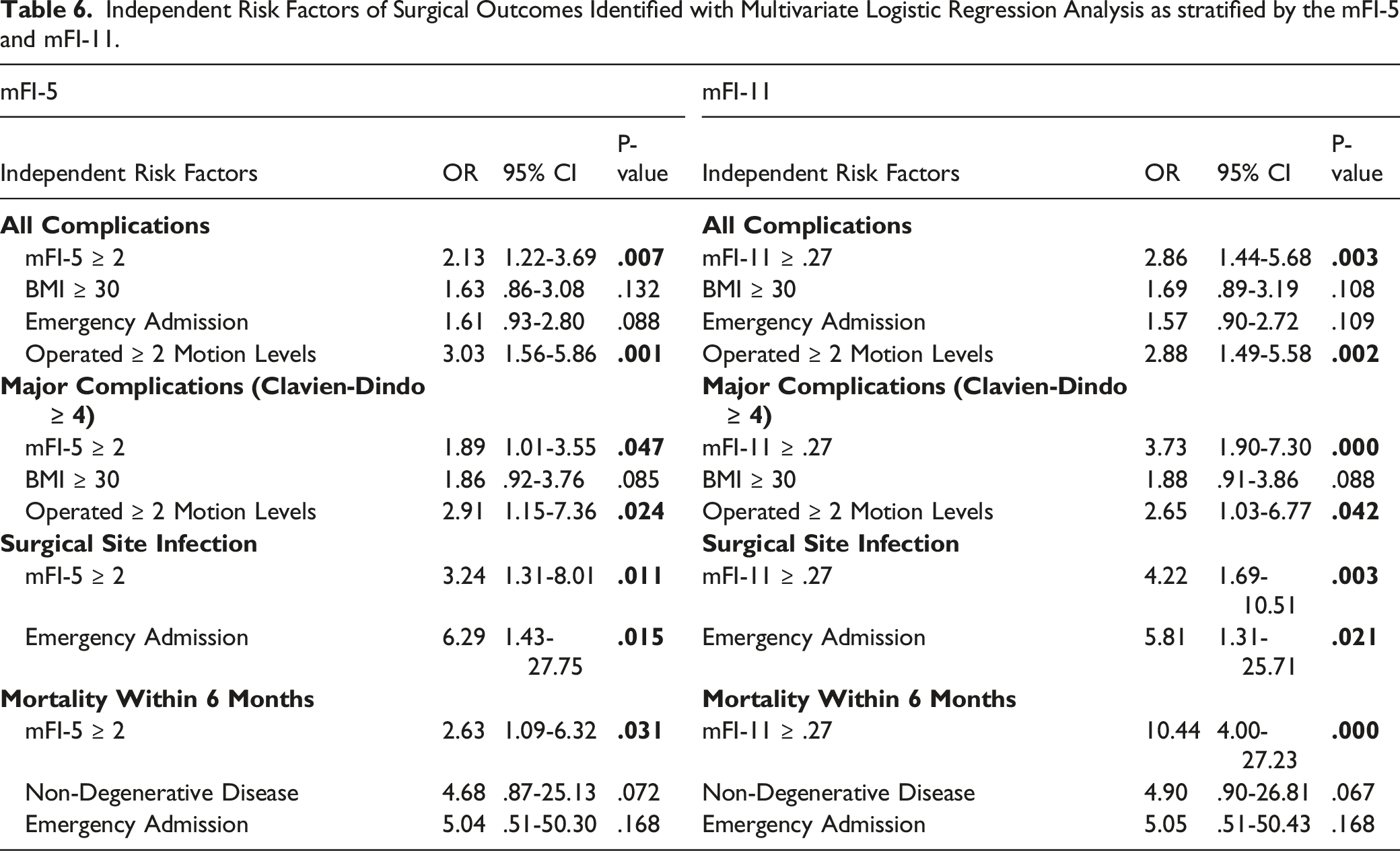
When dichotomizing the cohort with the mFI-11, it is notable that frailty appeared to portend overall worse outcomes compared with the mFI-5. For example, the risk of all complications possessed a odds ratio of 2.86 (1.44-5.68, P = .003) whilst the risk of major complications was more than 3 times greater (OR 3.73, 95% CI 1.90-7.30, P = .000). Moreover, there was heightened risk of surgical site infection if the mFI-11 threshold of .27 was achieved (OR 4.22, 95% CI 1.69-10.51, P = .003). Finally, frail patients as designated by the mFI-11 were more than ten times greater risk of mortality within 6 months (OR 10.44, 95% CI 4.00-27.23, P = .000)
Comparison between mFI-5 and mFI-11 by the Adjusted Receive Operating Characteristic (ROC) Curve.
Discussion
The global population is universally aging. 1 It is also noteworthy that the old age dependency ratio, which is the proportion of the population aged 65 years and over, also continues to rise. 1 As such, the United Nations anticipates that the elderly cohort will expand from 9% in 2019 to 16% in 2050. 1 Consequently, this elderly population is both increasing in number and living longer thereby leading to increased rates of complex instrumented spinal surgery.2-4 Given 63.6% of our study cohort were admitted on an emergency rather than elective basis, there is an urgent need for an accurate and easily applied risk stratification system to assess frailty. Our study is the first to validate the most concise frailty model to date, the 5-item modified frailty index, in the elderly population undergoing complex instrumented spinal surgery.
The post-operative surgical outcomes of elderly patients undergoing spinal surgery with instrumentation is mixed and heavily dependent upon their preoperative frailty status. 22 On 1 hand, Andersen et al and Glassman et al have found that superior functional outcomes in the elderly population can be achieved with fusion over simple decompressive surgery in appropriately selected patients.23-25 Agarwal et al even advocated that interbody fusion could be safely performed in the appropriate elderly patient with a subsequent low rate of complications. 26 This finding was supported by Kilincer et al and Okuda et al who both similarly determined there was no significant variation in complication rates between the younger and older groups of patients undergoing posterior lumbar interbody fusions.27,28 Finally, Costa et al also found that spinal fixation and fusion in the elderly improved quality of life as measured by both the Visual Analogue Scale and Oswestry Disability Index. 29
This was countered by others who did observe a higher rate of complications with instrumented fusion in the elderly compared to standard surgery. 29 In particular, Duan et al warned of the potential harm caused by instrumentation in the elderly without appropriate preoperative risk stratification. 30 The estimated increase in life-threatening complications sharply increased from 2.3% in those patients undergoing decompression alone, compared to 5.6% if undergoing fixation and fusion. 30 In evaluating this conflicting evidence, Endres et al summarized these findings to contend that spinal instrumented surgery, in the appropriately selected cohort of non-frail elderly patients, has a measurable benefit.6,7,23,27,31 In other words, a preoperative risk stratification instrument which accurately encapsulates the frailty status of an elderly patient is desperately needed. Ironically, the essence of frailty has long been intuitively appraised by clinicians by the bedside either consciously or unconsciously. It is a state of decreased physiological reserve, and the ease with which low or minimal fluctuations in external or internal factors can lead to disproportionately negative patient outcomes due to the lack of this physiological reserve.8,9,32,33
For this reason, the abbreviated 5-item modified frailty index was introduced by Subramaniam et al to provide a readily accessible tool for clinicians to objectively evaluate frailty in preoperative candidates. 13 The mFI-5 was initially validated in the general surgical population and demonstrated similar correlation with clinical outcomes as the more length and burdensome 11 item scale.13,34 The advantage of the mFI-5 is its brevity making it of greater practical applicability in the clinical setting. It has since been validated by Khalafallah et al regarding brain tumors, Segal et al with respect to vertebral augmentation procedures, Balla et al prior to ventral hernia repairs and in the field of orthopedics by Traven et al and Wilson et al.35-39
Our novel findings argue that mFI-5 and mFI-11 are equally robust independent predictors of all of the primary and secondary post-operative outcome measures. Patients designated frail by the mFI-5 and mFI-11 were at increased risk of all complications, major complications (Clavien Dindo ≥ 4), surgical site infection and 6-month mortality. On rudimentary review, it does appear that the mFI-11 may be a more powerful discriminator than the mFI-5 given the higher odds ratio of adverse outcomes between the dichotomized cohorts of non-frail and frail. However, the mFI-5 crucially exhibits an extremely high correlation coefficient with the mFI-11 (.944). Additionally, the c-statistics between the 2 indices were remarkably similar and did not demonstrate any statistically significant difference.40,41 This is consistent with the findings of Weaver et al who determined an association between mFI-5 scores and increased postoperative complications when they attempted to validate the index exclusively in a cohort undergoing lumbar fusion surgery. 42
The benefits of the more concise mFI-5 are threefold. Firstly, in the pre-operative phase an easily applicable accurate risk stratification instrument enables efficient informed pre-operative counselling to occur.8,43 In this way, Hersey et al noted that frail patients identified by the mFI-5 who may not be suited for a longer and more complex spinal surgical instrumented operation can be identified. 44 This provides valuable opportunity for critical prophylactic optimization measures such as preoperative physiotherapy suggested by Fors et al or medical management of comorbidities to be instituted. 45 The clinical benefit of the mFI-5 over the more length mFI-11 is its components can be more easily obtained during clinical history and used by the clinician with a simple threshold of 2 variables to instantly dichotomize a patient into a lower or high risk surgical candidate. This has already been observed and implemented and endorsed in other surgical specialties such as orthopaedics. 38 More than this, pre-frail or frail patients post-operatively can be managed with enhanced recovery pathway protocols. 46 These comprehensive targeted protocols can be tailored to address the specific needs of the identified frail patients ranging from appropriate nutritional supplementation to appropriate multimodal analgesia in the setting of existing comorbidities. 46
Finally, Flexman et al noted that risk stratification is of particular importance given the rate of resource consumption of our value-based healthcare system. 47 McGirt et al emphasized that effective predictive models enables efficacious allocation of finite resources. 48 For example, we found that frail patients designated by the mFI-5 were also more likely to be discharged to another hospital or rehabilitation (P = .016) and experience longer lengths of stay greater than 7 days (P = .007). Although our validation of the mFI-5 was retrospective, this association still represents valuable forewarning when attempting to streamline the healthcare system as a whole. 48 Balanced against this, Challener et al acknowledged the vital role of such risk classification systems but also sought to remind clinicians that any potential cost reductions should not be to the detriment of the current individual patient being managed. 49 Our unique validation of the concise yet accurate mFI-5 addresses all of these needs for the first time.
The strengths of our retrospective cohort study were a concrete inclusion criteria over a defined period with a consecutive non-selective method of participant selection. All primary and secondary outcome measures were adequately powered to achieved statistical significance for both the 5-item and 11-item modified frailty indices. More than this, the correlation coefficient was a convincing value of > .9. Not only is there a sense of internal validity imparted by these factors, but the fact that the study was undertaken at a tertiary state-wide academic centre is intended to lend a degree of external validity. As an added benefit, our contemporary data is unique and derived from the era following 2012 when the NSQIP database ceased collection of variables that previously enabled calculation of the 11-item modified frailty index. The major weakness of our study was its retrospective nature and the fact that data was from a single centre. Future larger multi-centre prospective randomized controlled international studies would be of benefit.
Conclusions
We have demonstrated that the concise and more easily applied 5-item modified frailty index is equally as effective a measure of frailty as the more lengthy 11-item scale. Age itself should not be a decisive factor when risk stratifying preoperative elderly patients undergoing posterior instrumented spinal surgery. The brevity of the now validated 5-item modified frailty index will facilitate its use by clinicians on a regular basis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.