
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Combined sternal and spinal fractures are rare traumatic injuries and present a high risk of spinal and thoracic wall instability. Limited research has addressed the treatment of sternovertebral injuries and biomechanical need for sternal fixation to achieve spinal healing.
Methods:
A 10-year retrospective cohort study was conducted, including patients with sternovertebral fractures admitted to our level-1 trauma centre between 2007 and 2016. Patients who died during hospital admission, military patients, patients with isolated upper cervical spine or lower lumbar spine fractures, and patients lost to follow-up were excluded.
Results:
In 10 years, 73 patients with sternovertebral fractures were included. Mean injury severity score was 24 (range 4-57). Most sternal fractures were located in the sternal body and manubrium. Spinal fractures were type A (52%), B (40%), or C (8%), and were located in the subaxial cervical (21%), upper thoracic (16%), thoracic (21%), thoracolumbar (47%) area; 7 patients had spinal fractures at multiple levels. Fourteen patients (19%) had a neurological deficit. A total of 42 patients received conservative and 31 patients received operative spinal treatment. Two patients (3%) underwent primary sternal fixation. Sternal failure rate was 1% and biomechanical spinal failure rate was 8%, there was no difference in treatment failure between surgical and conservative spinal treatment. Associated thoracic injuries did not influence sternal or spinal treatment outcomes.
Conclusions:
These findings indicate that conservative sternal treatment in presence of spinal fractures is safe and effective. The low spinal treatment failure rates imply that sternal fixation is not necessary to achieve spinal stability.
Keywords
Introduction
Combined traumatic sternal and spinal fractures, also known as sternovertebral fractures, are rare injuries with an estimated incidence of 0.64% in traffic victims. 1 Sternovertebral fractures occur mostly in young male patients and are mainly located in the thoracic spine. They are frequently severely injured patients who suffer not only from multiple associated thoracic injuries (rib and clavicular fractures, intrathoracic organ injuries) but also from injuries in other parts of the body (brain, abdomen, pelvis, and extremities). 1 -17
Sternovertebral fractures are primarily caused by direct-impact forces combined with indirect flexion-compression or flexion-rotation forces due to high deceleration in motor vehicle accidents. 1,5 -9,16 Other frequent injury mechanisms are direct-impact traumas or hyperflexion injuries due to falls from height or the falling of heavy objects on the head or chest. 1,6,8,9
In the 4-column spine model proposed by Berg et al 18 in 1993, the sternum and ribs form an essential fourth column of spinal support, in addition to the well-known anterior, middle, and posterior spinal columns. 19 Several studies have since substantiated the biomechanical significance of the sternum-rib complex. 20 Consequently, a combined sternal and spinal fracture might present a higher risk for spinal and thoracic wall instability than a spinal fracture alone. 6,21 Few studies have addressed sternovertebral fracture treatment and outcomes of conservative or surgical treatment strategies. Available evidence consists of case series with small patient populations. 6,21 Standardized treatment recommendations are lacking. However, the significant contribution of the sternum to spinal stability raises questions regarding sternovertebral fracture treatment and, specifically, the biomechanical need for sternal fixation to achieve spinal healing. Some authors have suggested that surgical fixation of both sternum and spine provides a biomechanical advantage and improved fracture healing. 6 Others have postulated that surgical indications depend on the spinal fracture level, 1 or that spinal fixation alone is sufficient to establish both sternal and vertebral fracture healing. 21
The present retrospective cohort study was performed to assess whether surgical fixation of the sternum is indicated in patients with traumatic sternovertebral fractures in order to achieve uncomplicated healing of both sternal and spinal fractures. We hypothesized that the three main spinal columns provided sufficient thoracic stability and that there was no biomechanical indication for sternal fixation in patients with sternovertebral fractures.
Patients and Methods
Study Design
A retrospective analysis was conducted of all patients who were admitted to the emergency department (ED) of the level-1 trauma center of University Medical Centre Utrecht (UMCU), the Netherlands from January 2007 to December 2016. Data was collected from the trauma registry maintained by the Trauma Care Network of Central Netherlands (TZNMN). All trauma patients with sternovertebral fractures were identified in the registry by searching for the respective Abbreviated Injury Scale (AIS) codes. Data on patients’ demographics, injury mechanism, injury severity, length of hospital stay, and in-hospital mortality was collected. Patients admitted later than 48 hours after injury and patients discharged from ED were excluded. Other exclusions were patients who were lost to follow-up (patients transferred to another hospital and patients who did not visit the outpatient clinic after hospital discharge), patients who died during initial hospital stay, military patients, and patients with isolated spinal fractures located in the upper cervical spine (C0-C2), lower lumbar (L3-L5), and sacral spine since it was thought that these fractures would not likely influence the stability of the thorax. The study was approved by the institutional review board (WAG/mb/16/030 735 and WAG/mb/17/032 781).
Data Collection
Additional information on past medical history, diagnostics, injuries, and treatment was collected from individual electronic patient files. Diagnostic images were thoroughly revised for all patients to ascertain injury type and location. Osteoporosis was defined as a positive DEXA (dual-energy X-ray absorptiometry) scan within 3 months posttrauma. Follow-up duration was defined as the period between hospital admission and the last visit to the Traumatology or Orthopaedics outpatient clinic in our hospital. Sternal fracture classification was divided in 4 fracture locations: manubrium, manubriosternal joint (only in case of fracture dislocations), sternal body, and xiphoid process. Sternal fracture displacement was defined as dislocation of ≥1 shaft width. A senior spine trauma surgeon (FCO) retrospectively classified all spinal fractures according to the AOSpine injury classification system. 22 -24 Spinal fractures were located in subaxial cervical spine (C3-C7), upper thoracic spine (T1-T4), thoracic spine (T5-T9), or thoracolumbar spine (T10-L2). In case of multilevel spinal fractures, the fracture with highest injury severity/instability was decisive for fracture location; in the event of multilevel fractures of equal severity, both locations were registered; in case of consecutive fractures of equal severity extending over 2 spinal levels, the level with most fractures was decisive for fracture location. Neurological deficits were assessed on admission to ED and were defined as N0 (neurologically intact), N1 (transient neurologic deficit), N2 (radiculopathy), N3 (incomplete spinal cord injury), N4 (complete spinal cord injury), or NX (unexaminable patient). Unstable fractures were defined as AOSpine type B or type C fractures.
Primary treatment methods were either conservative (including haloframe or a brace) or operative (within 7 days posttrauma). When different treatment methods were applied to multiple sternal and/or spinal fractures, the most invasive treatment method was registered. Glasgow Coma Scale (GCS) was recorded at hospital admission: brain injury was defined according to mild (GCS 13-14), moderate (GCS 9-12), or severe (GCS
Primary outcome parameters were sternal and/or spinal treatment failure, defined as either surgery secondary to conservative treatment or reoperation after primary operative treatment. In the event of treatment failure, the cause of failure was registered as secondary dislocation, nonunion, or technical failure. Nonunion was defined as the absence of callus formation at 3 months posttrauma. Technical failure was defined as malposition of osteosynthesis material or pain due to osteosynthesis material.
Secondary outcome parameters were hospital length of stay (H-LOS), intensive care unit length of stay (ICU-LOS), duration of mechanical ventilation (DOV; all calculated in days), wound infection, and pneumonia. Wound infection was defined as a positive wound culture and was registered for patients undergoing surgery or haloframe treatment. Pneumonia was defined as a positive sputum culture, pulmonary consolidations on X-ray suspected for pneumonia, or empirical treatment for pneumonia.
Statistical Analysis
Patients were retrospectively allocated to either the primary conservative or primary surgical spinal treatment group. All baseline characteristics, primary outcome parameters, and secondary outcome parameters were assessed for the total population and for the respective treatment groups.
Statistical analysis was performed using R Statistics (an open-source integrated development environment for statistical computing). For continuous variables, normality of distribution was assessed using Kernel density scores. Continuous variables were expressed as mean (range) in case of a normal distribution, or as median (interquartile range, IQR) in case of a nonnormal distribution. Significant differences were calculated using the Student’s T test or Mann-Whitney U test, respectively. Categorical variables were expressed as ratio (percentage). Significant differences for categorical variables were calculated through chi-square test or Fisher’s exact test depending on the size of the groups. For all analyses, 2-sided P values <.05 were considered statistically significant.
Results
Between January 2007 and December 2016, a total of 12 120 trauma patients were admitted to UMCU level-1 trauma center. Of these, 1749 (14%) had spinal fractures and 256 patients (2%) had sternal fractures. A total of 116 patients had a combined sternovertebral fracture, corresponding to 1% of all trauma patients, 7% of all patients with a spinal fracture, and 45% of all patients with a sternal fracture. Among the 116 sternovertebral fracture patients, 43 patients were excluded from further analysis (1 military patient, 14 patients who died early after admission before fracture treatment, 14 patients with either isolated upper cervical spine or lower lumbar spine fractures, and 14 patients who were lost to follow-up). The remaining 73 patients were included for further analysis (Figure 1).
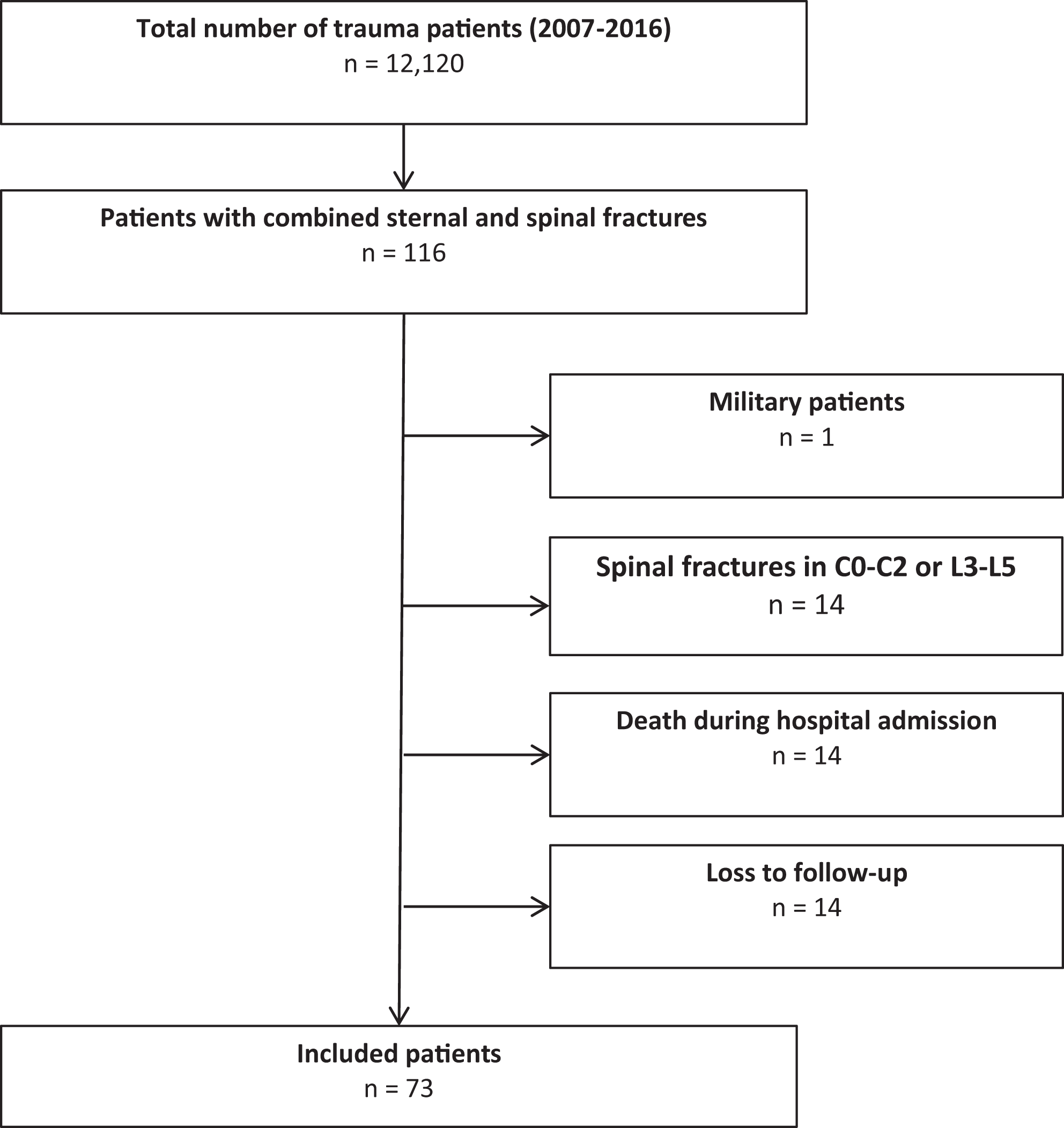
Patient flowchart.
All 73 patients sustained sternovertebral fractures through a blunt trauma mechanism. Sixty-six percent of patients had a traffic accident, 30% fell from height, and 4% had another mechanism of injury, such as being hit by an object or an animal (Table 1). An example of combined sternovertebral fractures is shown in Figure 2. Seventy-seven percent of patients were male with a mean age of 50 years (range 16-93 years). Mean injury severity score (ISS) was 24 (range 4-57). No patient had osteoporosis and 5 patients (7%) had a history of malignancy, varying from hematological malignancies to melanoma (Table 1). Sixty-three patients (86%) sustained 1 sternal fracture, while 10 patients (14%) had 2 sternal fractures. Thirty-eight patients (52%) had a sternal fracture located in the manubrium, 2 (3%) at the manubriosternal joint, 42 (58%) in the sternal body, and 1 (1%) in the xiphoid process. One patient (1%) had a displaced sternal fracture.
Baseline Characteristics.a
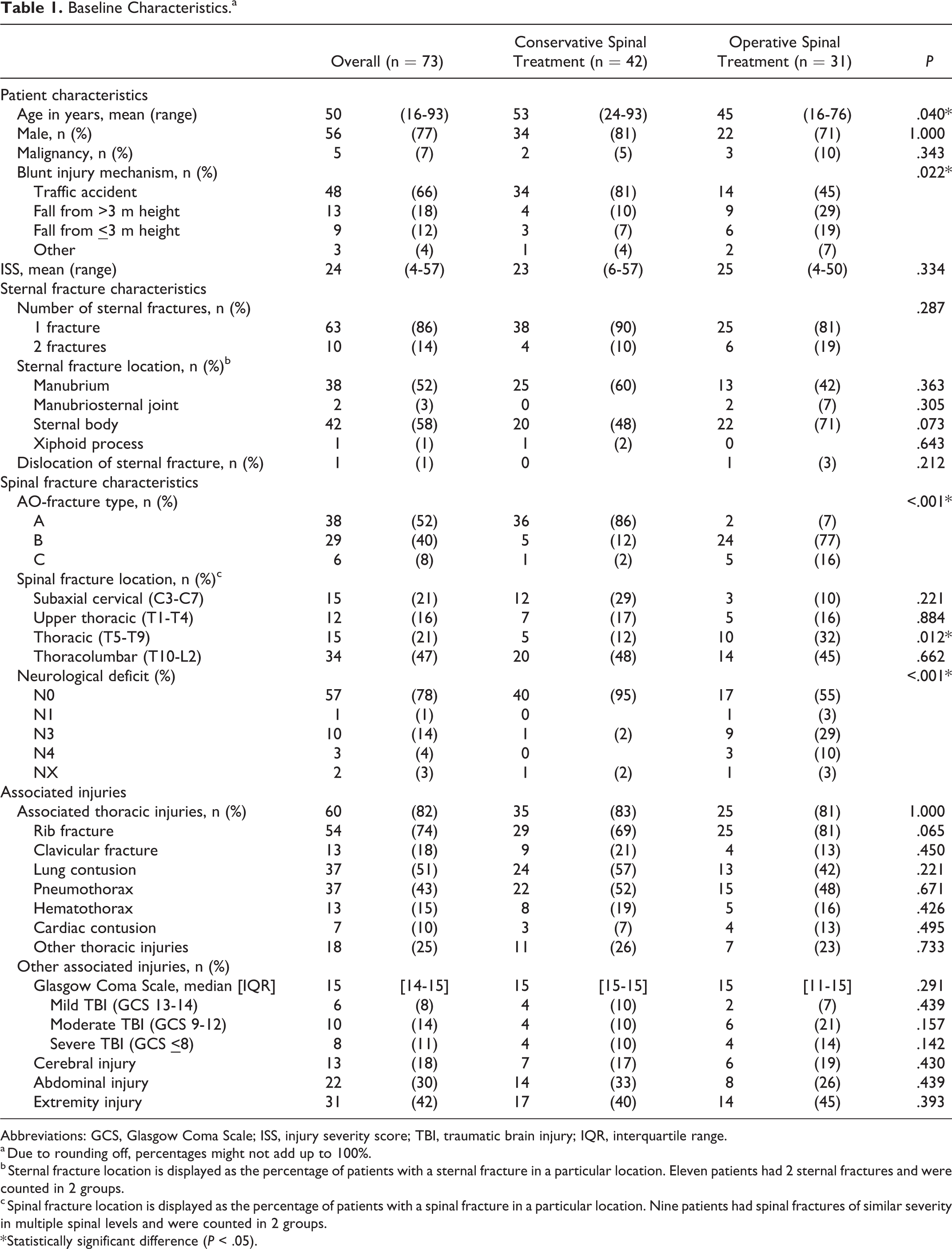
Abbreviations: GCS, Glasgow Coma Scale; ISS, injury severity score; TBI, traumatic brain injury; IQR, interquartile range.
a Due to rounding off, percentages might not add up to 100%.
b Sternal fracture location is displayed as the percentage of patients with a sternal fracture in a particular location. Eleven patients had 2 sternal fractures and were counted in 2 groups.
c Spinal fracture location is displayed as the percentage of patients with a spinal fracture in a particular location. Nine patients had spinal fractures of similar severity in multiple spinal levels and were counted in 2 groups.
* Statistically significant difference (P < .05).
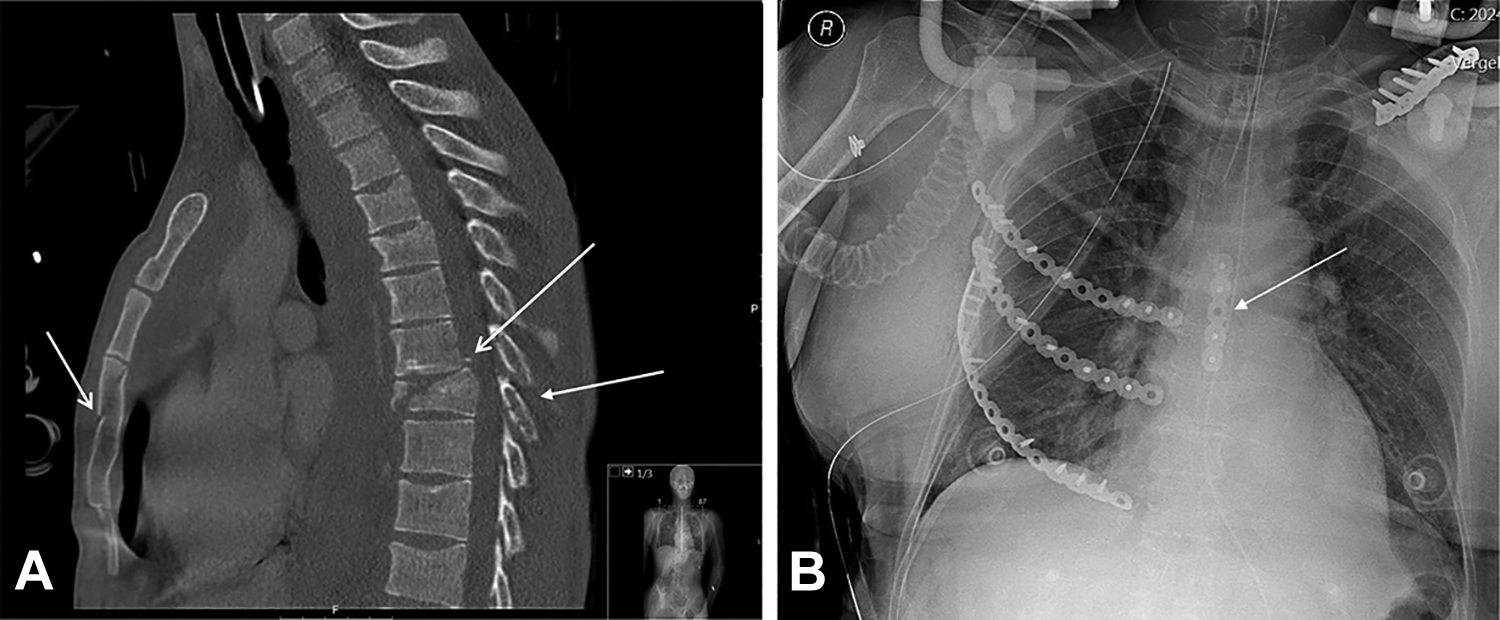
Traumatic sternovertebral fractures. (A) Sagittal views of computed tomography scan of a patient with a combination of sternal and spinal fractures. (B) Postoperative chest X-ray of a patient who underwent sternal fixation in combination with fixation of rib fractures and clavicular fracture.
Fifteen patients (21%) had subaxial cervical spinal fractures, 12 (16%) upper thoracic spinal fractures, 15 (21%) thoracic spinal fractures, 34 (47%) thoracolumbar spinal fractures (12 patients with fractures in T10-T12 and 18 patients with fractures in L1-L2, 4 had fractures in both regions). Among these, 7 patients had spinal fractures of the same severity in multiple spinal levels and were counted in 2 groups. Most patients suffered from an AOSpine type A spinal fracture (n = 38, 52%), while 29 patients (40%) had an AOSpine type B fracture and 6 patients (8%) an AOSpine type C fracture. Neurological deficit was present in 14 patients (19%) and was N1 (n = 1, 1%), N3 (n = 10, 14%), and N4 (n = 3, 4%), respectively. In 2 patients (2%), neurological deficit could not be assessed due to unconsciousness or prehospital intubation and sedation (Table 1).
The majority of patients (82%) had associated thoracic injuries such as clavicular fractures (18%), rib fractures (74%), lung contusion (51%), and cardiac contusion (10%). Other injuries were intracerebral injuries (18%), abdominal injuries (30%), and extremity injuries (42%; Table 1).
Patients stayed 19 days (IQR 10-35 days) in hospital. Thirty-six patients (49%) were admitted to ICU with a median length of ICU stay of 8 days (IQR 4-16 days). They stayed on the ventilator for 5 days (IQR 3-14 days). Twenty-nine patients (40%) developed hospital-acquired pneumonia, and 6 patients (8%) developed a wound infection. Median duration of follow-up was 13 months (IQR 6-22 months; Table 2).
Treatment Methods and Outcomes.a
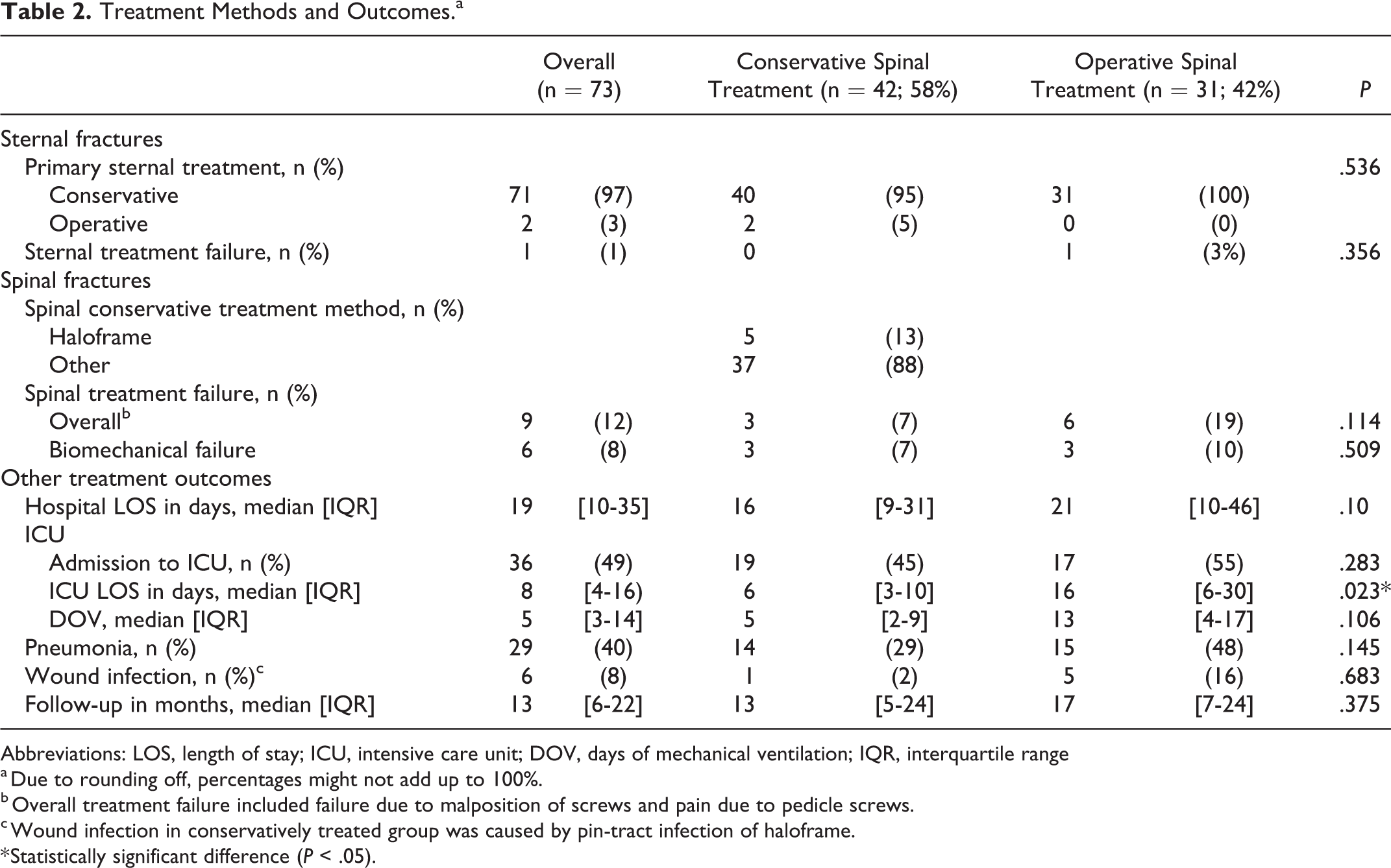
Abbreviations: LOS, length of stay; ICU, intensive care unit; DOV, days of mechanical ventilation; IQR, interquartile range
a Due to rounding off, percentages might not add up to 100%.
b Overall treatment failure included failure due to malposition of screws and pain due to pedicle screws.
c Wound infection in conservatively treated group was caused by pin-tract infection of haloframe.
* Statistically significant difference (P < .05).
Patients who later had surgery for their spinal fractures were younger (45 [range 16-76] vs 53 [range 24-93] years, P = .040), had more often had fallen from height than patients who were conservatively treated for their spinal injury (48% vs 17%, P = .022). Furthermore, they had more often unstable type B or C fractures (93% vs 14%, P < .001), which was more often located in the thoracic spine compared with the conservatively treated group (32% vs 12%, P = .012; Table 1). These fractures were also more often accompanied by spinal cord injury (42% vs 2%, P < .001; Table 1). There was no difference in ISS or in associated injuries between patients who had surgery for their spinal injury and patients who did not (Table 1). There was no difference in hospital stay hospital (21 vs 16 days, P = .10) or in days on the ventilator (13 vs 5 days, P = .106) even though patients in the operative treatment group stayed longer in ICU (16 vs 6 days, P = .023). There were no significant differences in pneumonia or wound infection between the conservative and surgical treatment groups (Table 2).
Treatment and Outcome of Sternal and Spinal Fractures
Seventy-one patients (97%) were conservatively treated for their sternal fractures. The 2 patients who underwent primary fixation of their sternal fracture were both treated conservatively for their spinal fracture and thus included in the conservative spinal treatment group (Table 2). Indications for sternal fixation were the presence of 2 sternal fractures in combination with multiple bilateral rib fractures (n = 1), and respiratory insufficiency due to flail chest, thoracic wall deformity, and sternal dislocation of almost 1 shaft width (n = 1). Both these patients underwent simultaneous fixation of ribs and sternum.
Forty-two patients (58%) had a conservative treatment for their spinal fractures (Table 2). Five patients (13%) received a halo frame and 37 patients (88%) received other treatment, such as a Philadelphia collar, or no additional treatment. Thirty-one patients (42%) underwent primary operative treatment for the spinal fractures.
Twenty-nine of 35 patients (83%) with type B or C spinal fracture and 13 of 14 patients (93%) with a neurological deficit underwent surgical treatment (Table 1). Two patients with associated unstable subaxial cervical fractures were treated conservatively with haloframe. The remaining 4 patients were treated conservatively because of severe psychiatric disease during initial hospital admission, unilateral facet fracture, benign neglect policy due to old age and lumbar fracture, and neurologic deficit (central cord lesion) in combination with stable type A spinal fractures, respectively.
Treatment Failure
Overall sternal treatment failure occurred in 1 patient (1%). This patient had surgical treatment for the thoracic spine fracture, conservative sternal treatment failed due to secondary dislocation of the sternum (Table 2).
Overall, spinal treatment failed in 9 patients (12%), the majority located in thoracic spine fractures (Table 3). When only biomechanical failure was considered, the overall spinal treatment failure rate was 8%. There were no significant differences in biomechanical treatment failure rates between the conservative and surgical spinal treatment groups (Table 2).
Treatment Failure per Treatment Group.a
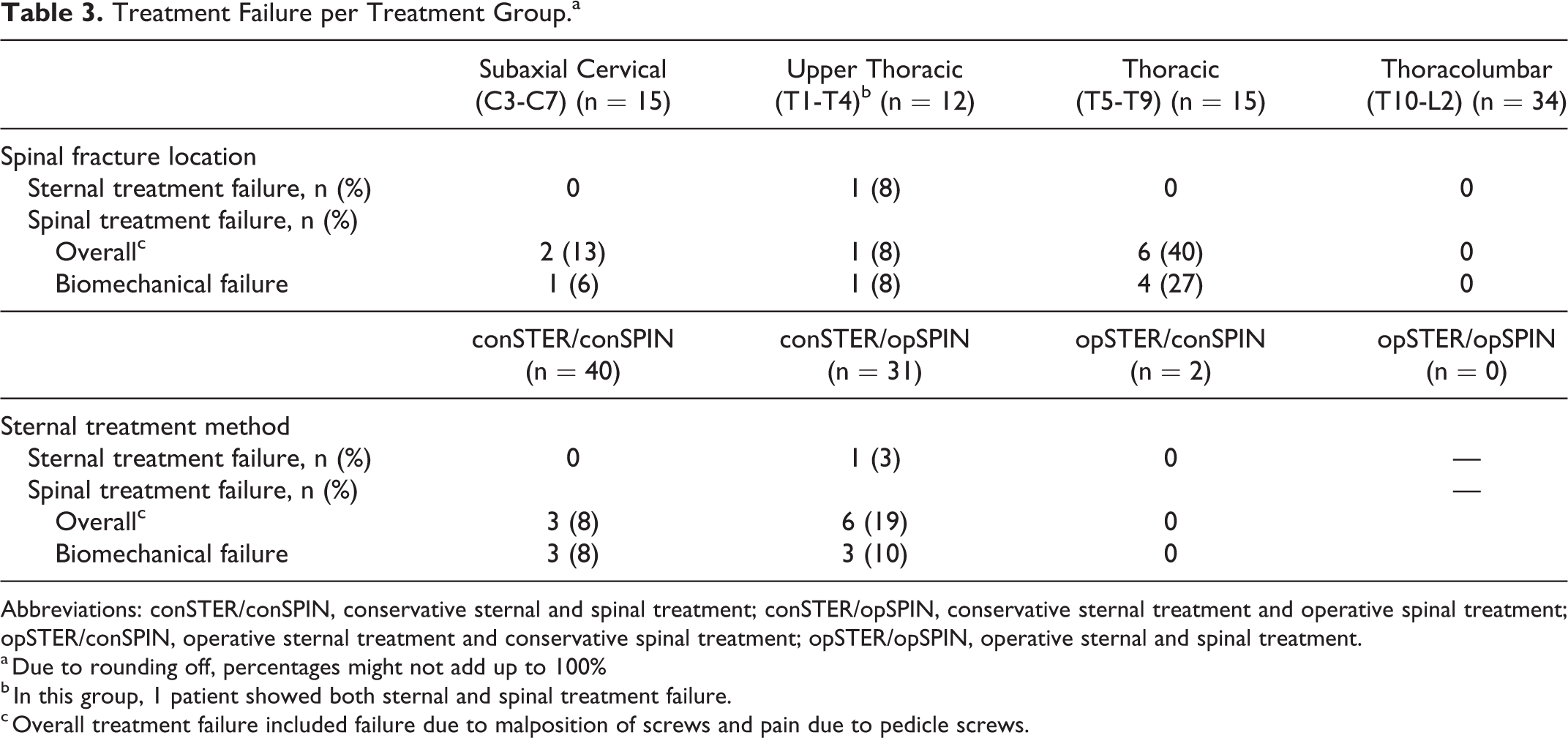
Abbreviations: conSTER/conSPIN, conservative sternal and spinal treatment; conSTER/opSPIN, conservative sternal treatment and operative spinal treatment; opSTER/conSPIN, operative sternal treatment and conservative spinal treatment; opSTER/opSPIN, operative sternal and spinal treatment.
a Due to rounding off, percentages might not add up to 100%
b In this group, 1 patient showed both sternal and spinal treatment failure.
c Overall treatment failure included failure due to malposition of screws and pain due to pedicle screws.
Three patients (8%) who were treated conservatively for both sternal and spine fractures (conSTER/conSPIN, n = 40) had a failing conservative treatment of the spinal fracture (Table 3). The failures were caused by secondary dislocation of an associated odontoid fracture in combination with a thoracic spine fracture, secondary dislocation of subaxial cervical fracture, and one secondary dislocation of T4-T6 thoracic spine body fractures (type B fractures in T3 and T6, type A fractures in T4 and T5). In hindsight, the fractures in the last 2 patients were unstable and should have undergone primary surgical fixation based on the surgical algorithm for the AOSpine injury classification system. 25
Six patients (19%) who had conservative sternal treatment and operative spinal treatment (conSTER/opSPIN, n = 31) had a failure of their operative spinal treatment. Three out of 6 patients who failed had a genuine biomechanical spinal failure due to nonunion of a thoracic spinal fracture (type B fracture in T6 and T7), secondary dislocation of type B T3-T5 fractures, and a secondary dislocation of an associated odontoid fracture in combination with T4-T6 type B fractures, respectively. Technical failure was the reason for reoperation in the 3 other patients: 2 had malpositioned screws in the thoracic spine, and 1 patient had pedicle screws removal from the subaxial spine (after consolidation of the fracture) due to severe pain (Table 3).
Two patients who had operative sternal treatment and conservative spinal treatment (opSTER/conSPIN) developed no failures in both sternal and spinal treatment. There were no patients who had surgery for both sternal and spinal fracture (opSTER/opSPIN).
Subgroup analysis based on spinal fracture stability showed a significant difference in treatment failure rate between stable and unstable spinal fractures (3% vs 23%, P = .006).
The presence or absence of rib fractures was not significantly associated with sternal (2% vs 0%, P = 1.0) or spinal treatment failure (13% vs 11%, P = 1.0).
Subanalysis of Sternal Fractures in Combination With Thoracic Spine Fractures Only
Sub analysis of patients with combined sternal fractures and thoracic spine fractures only (n = 41) showed no difference in sternal failure rates between patients who had spinal fracture fixation and patients who had conservative treatment for their spinal fractures (4% vs 0%, P = 1.0, Table 4); nor was there any difference in (biomechanical) spinal failure between patients who had spinal fracture fixation and conservative treated patients; as described previously, 2 patients had a genuine biomechanical spinal failure due to nonunion of a thoracic spinal fracture and 1 patient developed a secondary dislocation of T4-T6 thoracic spine body fractures after conservative treatment (8% vs 6%, P = .81, Table 4).
Treatment Failure in Thoracic Spine Fractures.a
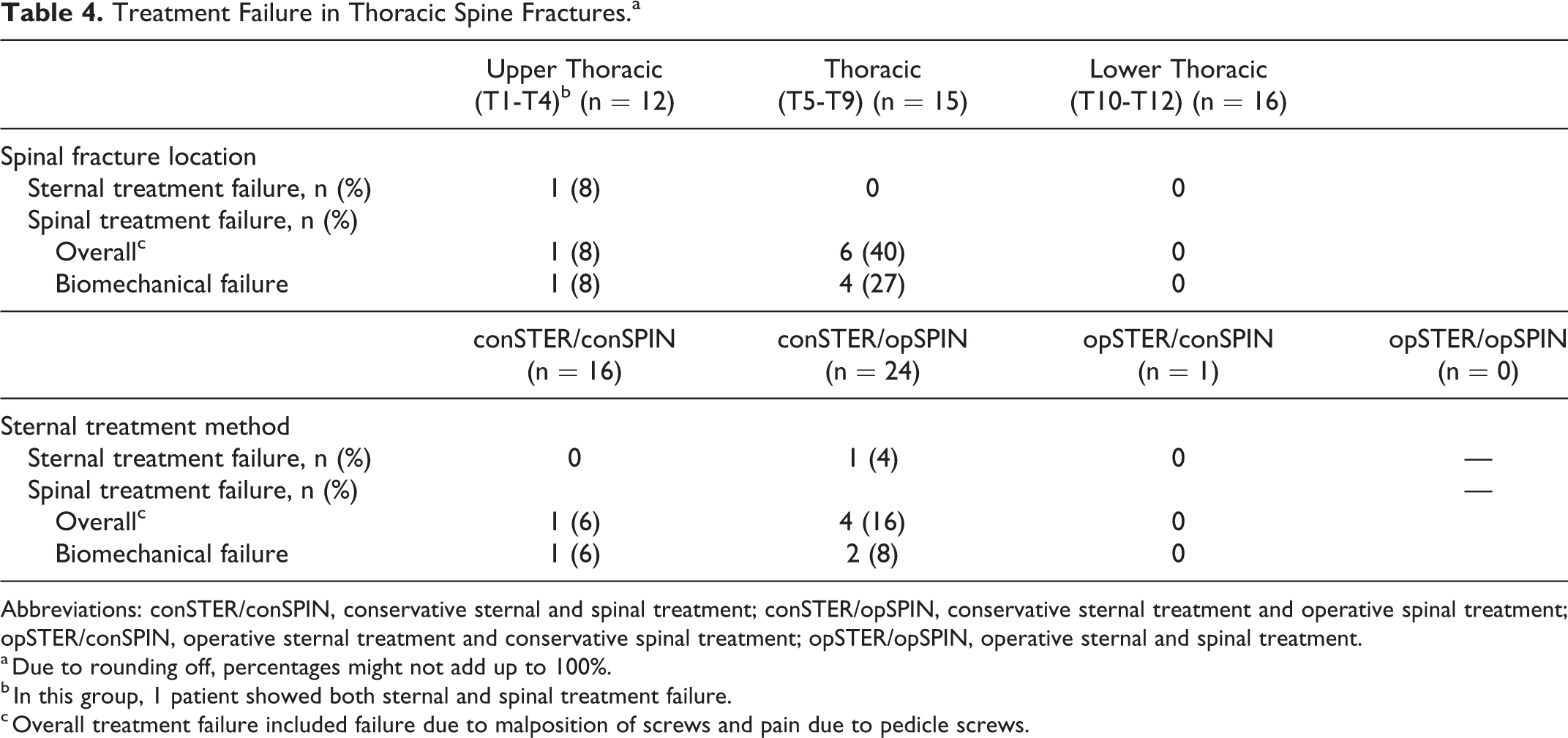
Abbreviations: conSTER/conSPIN, conservative sternal and spinal treatment; conSTER/opSPIN, conservative sternal treatment and operative spinal treatment; opSTER/conSPIN, operative sternal treatment and conservative spinal treatment; opSTER/opSPIN, operative sternal and spinal treatment.
a Due to rounding off, percentages might not add up to 100%.
b In this group, 1 patient showed both sternal and spinal treatment failure.
c Overall treatment failure included failure due to malposition of screws and pain due to pedicle screws.
Discussion
Treatment outcomes of our 10-year patient cohort suggest that sternal fixation is not essential to achieve sternal and spinal stability. Only 1 patient (1%) had sternal treatment failure, and 6 patients (8%) developed biomechanical failure of their spinal fractures. Conservative sternal treatment in association with spinal fractures is safe and effective and does not influence spinal healing. Furthermore, there was no significant difference in failure between conservative and operative spinal treatment; 3 patients developed a failure of initial spinal treatment after conservative treatment and 3 after operative treatment. In both groups, there was a patient with failure of an associated, conservatively treated, type A odontoid fracture in combination with a thoracic spine fracture. One could question whether there was a genuine biomechanical failure since it was the odontoid fracture that dislocated and not the spinal fracture. Genuine biomechanical treatment failure after operative treatment was likely caused by the fact that, in hindsight, the segmental stabilization was too short. Biomechanical failure after conservative spinal treatment was caused by misinterpretation of the stability of the spinal fracture.
Traumatic sternovertebral fractures are rare injuries. 1,10,17 In 10 years, only 116 patients with these injuries were admitted to our level-1 trauma center, corresponding to 1% of all trauma patients. Sternovertebral fractures mainly occur in relatively young male patients, 1,5 which was confirmed in the current study. Patients in the operative spinal treatment group were younger than those in the conservative treatment group, perhaps due to a different injury mechanism (more high-energy falls), leading to a higher incidence of unstable spinal fractures, neurological deficits, and thoracic spinal fractures. Corresponding to previous studies, the predominant trauma mechanism was a traffic accident, followed by falls from height. 1,5 -9,26 Mean ISS was 24 and many patients sustained associated thoracic and other injuries, demonstrating that sternovertebral fractures occur primarily in polytrauma patients. Median GCS was relatively high and only 10% of patients suffered from severe brain injury, possibly because most patients with severe brain injury died during hospital admission and were not included in analysis.
The 4-column model postulates that sternum and ribs provide an essential fourth column of spinal support. 18 However, in the current cohort of sternovertebral fracture patients, both sternal treatment failure (1%) and biomechanical spinal treatment failure rates (8%) were relatively low, particularly when considering the high injury burden of our polytrauma patient cohort.
Earlier studies by Krinner et al 6 and Labbe et al 21 reported (when study results were combined) a much higher treatment failure rate in the conSTER/conSPIN group (100% sternal failure and 50% spinal failure) than in our cohort. This difference is most likely due to the fact that all patients in their treatment group had missed spinal fractures. On the other hand, treatment outcomes in the conSTER/opSPIN group (0% sternal and spinal failure) were better than in our cohort, perhaps due to small sample sizes. In another small study by Huang et al, 16 vertebral height loss and kyphotic angulation were highest in conSTER/conSPIN group, followed by opSTER/conSPIN and conSTER/opSPIN, and lowest in opSTER/opSPIN group. Homagk et al 1 recommended surgical treatment for all sternovertebral fractures, except for fractures of the ascendant type (sternal fractures with concomitant lumbar spinal fractures), but did not report treatment outcomes. In the present study, no supportive evidence could be found for this elaborate surgical treatment of sternal fractures.
Consistent with other reports, most sternal fractures were located in the sternal body or manubrium. 1,5,8,9 In our study, only 1 patient had a displaced sternal fracture, while other authors reported displacement rates up to 50%. 5,6,21 This difference may be caused by our rather strict definition of displacement; in our experience, only displacement of ≥1 shaft width has biomechanical relevance to sternal stability. Indications for sternal fracture fixation are sternal instability, primary or secondary fracture dislocation, fracture nonunion, respiratory insufficiency due to severe pain, or sternal deformity. 27 In our cohort, 2 patients underwent primary surgical fixation due to respiratory insufficiency, sternal instability and/or thoracic wall deformity. In both cases, sternal healing was achieved after fixation. In 1 patient, who received conservative sternal treatment and surgical spinal treatment, sternal treatment failed due to secondary sternal dislocation. Notably, this patient later developed sternal nonunion after secondary sternal fixation, which required a reoperation, and spinal failure of his unstable thoracic spinal fracture, also requiring multiple reoperations.
In the present cohort, the majority of the spinal fractures were located in the thoracolumbar spine. Although the sternum contributes to thoracic wall stability, concomitant spinal fractures were not limited to the thoracic spine even though upper cervical spine and lower lumbar fractures were excluded from analysis. This is in accordance with other studies. 1,3,4,7 -15 Some authors argue that biomechanics resulting in combined sternal and spine fractures are different for the different levels of spinal fractures and that the 4-column spine model can mainly be applied to the combination of sternum and thoracic spine fractures. 1,16 For that reason, a separate analysis was performed of patients with combined sternal and thoracic spine fractures only. Again, there was no difference in sternal or spinal failure rates between patients who had conservative or operative treatment of the thoracic spine.
Subgroup analysis revealed a significantly higher biomechanical failure rate in unstable spinal fractures compared to stable spinal fractures. However, due to subgroup allocation (based on the spinal injury with highest severity), one case of treatment failure was registered in the unstable fracture group (with operative treatment), while treatment failure occurred in his concomitant type A odontoid fracture. Treatment failure of surgically treated unstable fractures was therefore overestimated in statistical analysis. Nonetheless, biomechanical treatment failure of conservatively treated unstable fractures remains much higher than in the other treatment groups. This finding also confirms previous reports that spinal fixation is recommended in unstable spinal fractures. 25 This emphasizes the importance of correct classification of the spinal fracture as was shown in the current study where treatment failure in 2 patients was caused by incorrect interpretation of the fractures as being stable.
Few studies have addressed treatment outcomes of sternovertebral fractures. Prospective studies are lacking, and available retrospective studies have small patient populations, or do not report sternal or spinal treatment outcomes. 6,16,21,28 -32 To our knowledge, this study is the largest study on the treatment outcomes of sternovertebral fractures to date with a follow-up of 12 months, allowing the detection of long-term treatment outcomes and complications.
One of the limitations of the present study is its retrospective, single-center study design, which has an inherent risk of information bias. However, since a prospective trauma registry was used a complete series of all trauma patients in our region over a 10-year period was available. Furthermore, although the present study reports treatment outcomes for the largest patient cohort with sternovertebral fractures, the study population is still relatively small.
In conclusion, sternovertebral fractures are rare traumatic injuries with low treatment failure rates for both sternal and spinal fractures, indicating that sternal fixation is not compulsory to establish spinal stability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.