
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To compare the outcomes and complications of transiliac-transsacral screw fixation (TIS) and lumbopelvic fixation (LPS), the 2 most common fixation methods for nondisplaced and minimally displaced H-/U- type sacral fragility fractures.
Methods
Medical records of patients treated with TIS or LPS for nondisplaced and minimally displaced H-/U-type sacral fragility fractures at 2 level A trauma centers between 2012 and 2022 were analyzed. Postoperative low back pain and mobility levels were assessed as primary outcomes before discharge and at 6 weeks and 6 months postoperatively. Surgery time, blood loss, and surgical complication rates were assessed as secondary outcomes. Statistical analyses consisted of Fisher’s exact tests for frequency distributions and Mann-Whitney-U tests and t-tests for group comparisons.
Results
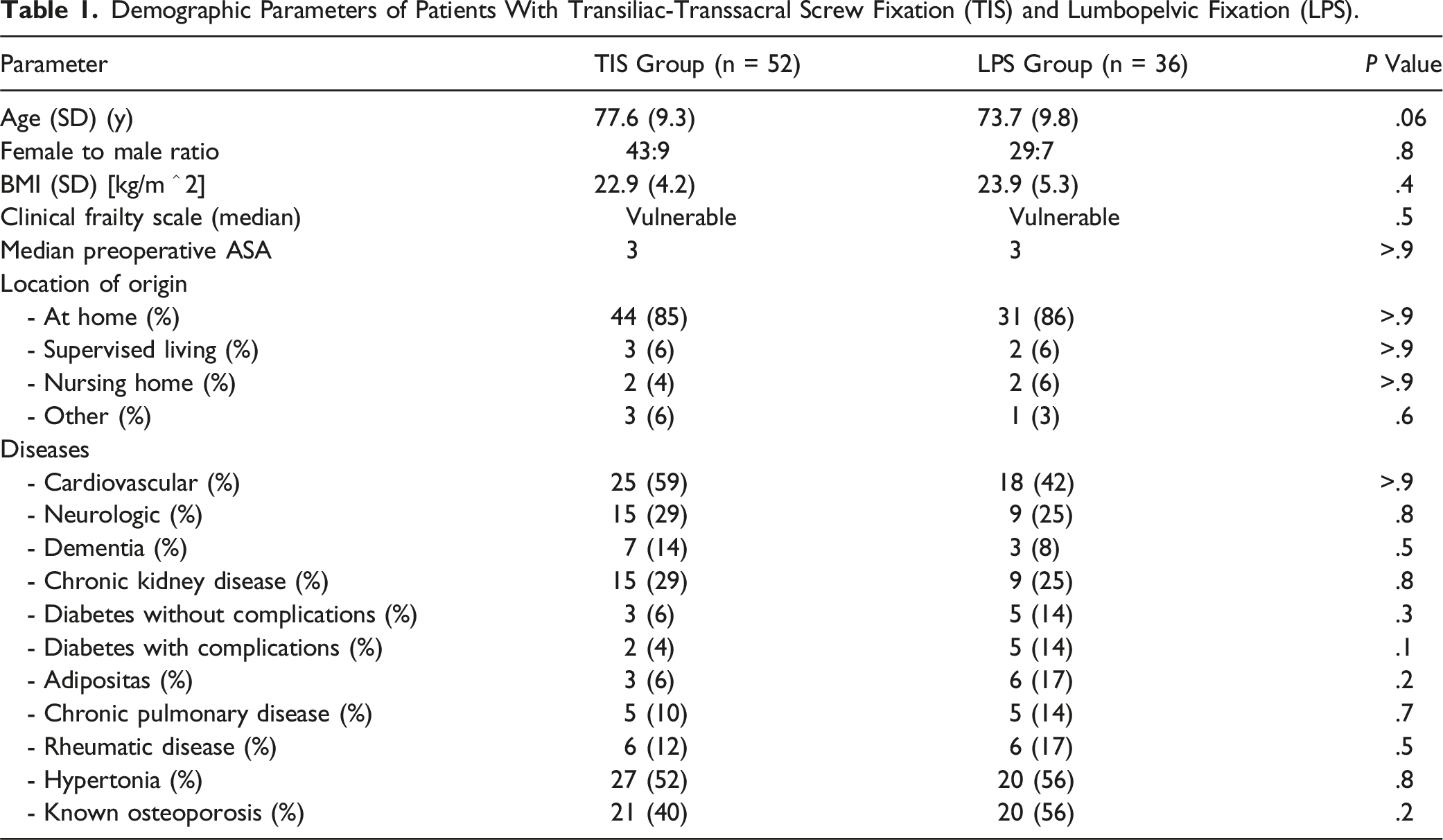
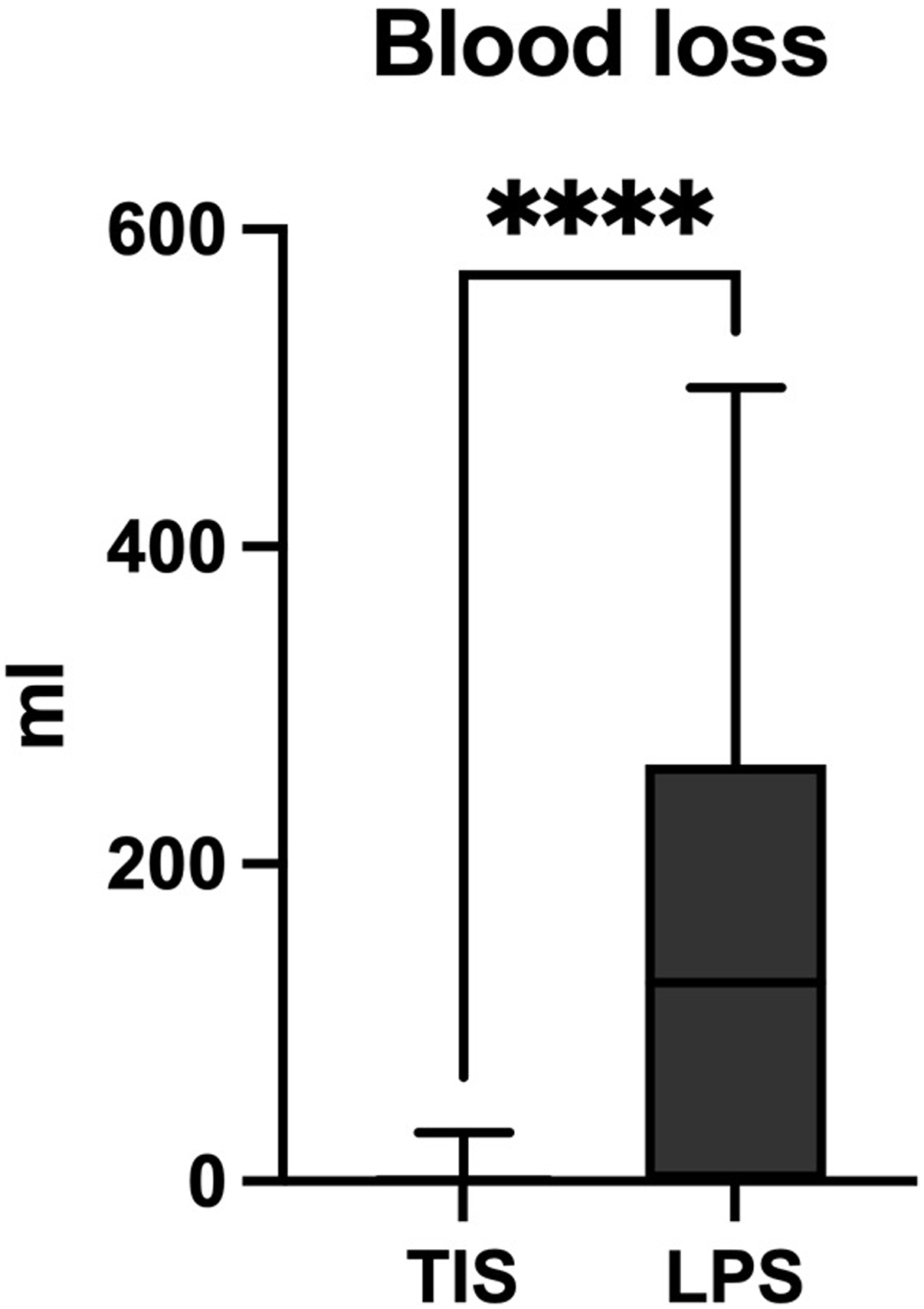
52 patients undergoing TIS (mean age: 78 ± 9 years) and 36 patients undergoing LPS (74 ± 10 years) with no discrepancy in demographic parameters were identified. There were no differences in low back pain levels between the 2 groups before surgery, before discharge, at 6 weeks postoperatively, and at 6 months postoperatively (P > 0.05). There were no differences in mobility levels before surgery, before discharge, at 6 weeks postoperatively, and at 6 months postoperatively (P > 0.05). Duration of surgery was shorter after TIS (36 ± 13 min) compared to LPS (113 ± 31 min) (P < 0.0001). Intraoperative blood loss was lower for TIS (median <20 mL) compared to LPS (median 125 mL) (P < 0.0001). Postoperative radiculopathy was less frequent after TIS (n = 1) compared to LPS (n = 3) (P > 0.05). Median length of stay was shorter after TIS (11 days) compared to LPS (14 days) (P < 0.05). Rates of reoperations directly related to the index surgery were lower after TIS (n = 2) compared to LPS (n = 10) (P < 0.01). Implant failures were observed only after LPS (n = 1).
Conclusion
Patients with nondisplaced and minimally displaced H-/U- type sacral fragility fractures may preferably be treated using TIS, as it is equivalent to LPS in terms of low back pain reduction and restoration of mobility, but allows for shorter operative time, less blood loss and lower reoperation rates. Prospective randomized studies should be conducted to substantiate our findings and develop distinct treatment recommendations.
Introduction
Spinopelvic dissociation injuries impede the transmission of load from the torso to the lower extremities and are seen in 21% of patients with fragility fractures of the pelvis. 1 Morphologically, these injuries involve the combined disruption of the sacral transverse and vertical integrity, leading to H-, U-, T-, or λ-type fractures (C0 fractures according to the new AOSpine Sacral classification).2,3 From a biomechanical perspective, these fracture types last the integrity of ligamentous tension (anterior, posterior, interosseous SI ligaments) and therefore cannot be equated with the true traumatic spinopelvic dissociation seen in high-energy mechanisms.
Treatment goals are pain reduction, restoration of mobility and prevention of progressive kyphotic deformity. Nonoperative management of H-/U- type spinopelvic dissociations in fragility fractures of the sacrum has demonstrated a 100% failure rate. 4 Consequently, posterior surgical fixation is recommended to restore or bypass the weight -bearing portion of the sacrum. 5 Surgical options for treatment include (bilateral triangular) lumbopelvic stabilization (LPS) and (multiple) transiliac-transsacral screw fixation or bilateral sacroiliac screw fixation, respectively (TIS).5-7 However, there are no clear indications favoring one method over the other due to limited evidence regarding pain control, early mobilization, procedure-related complications, and mortality. 8
To the best of our knowledge, there are currently no prospective or retrospective trials of sufficient sample size to support the use of either LPS or TIS in spinopelvic dissociation injuries (H -type and U -type sacral fragility fractures) in fragility fractures of the sacrum.
In this retrospective, bi-centric comparative cohort study, we aimed to compare the outcomes and complications of TIS and LPS in patients with nondisplaced or minimally displaced spinopelvic dissociation in fragility fractures.
Methods
Our primary hypothesis was that TIS would be non-inferior to LPS regarding postoperative low back pain levels at various time points (at discharge, at 6 weeks, and at 6 months) among patients with nondisplaced or minimally displaced H-/U-type sacral fragility fractures. Our secondary hypothesis was that there would be no difference in postoperative mobility between the 2 treatment groups. Additionally, we hypothesized that TIS would demonstrate superiority in terms of surgery duration, blood loss, and surgical complication rates compared to LPS.
Study data were collected and managed using REDCap electronic data capture tools.9,10 REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources.
Data were obtained from clinical and imaging records. We identified patients with nondisplaced or minimally displaced spinopelvic dissociation in fragility fractures (C0 according to the AOSpine Sacral Classification 2 ) who were treated at 2 level A trauma centers between 2012 and 2022. The inclusion criteria consisted of patients aged between 50 and 94 years, experiencing pain onset within 4 weeks, and undergoing either TIS or LPS procedures, with sacral H-/U-type fracture being the only indication for surgery. Patients with incomplete data or those who waived consent were excluded. Additionally, patients with high-energy mechanism trauma, pelvic fractures associated with malignancies or infections, chronic pelvic injuries, or previous instrumented surgery of the sacrum or inferior lumbar spine (L4 and below) were also excluded.
Patients have been either treated using LPS or TIS. In the LPS group, patients underwent bilateral lumbopelvic fixation using pedicle screws and SAI screws, with or without triangular stabilization involving transiliac-transsacral or bilateral SI screws. Similarly, patients in the TIS group underwent transiliac-transsacral screw osteosynthesis, bilateral SI screw osteosynthesis, or a combination of these techniques.
All procedures were performed by experienced surgeons under fluoroscopic guidance. The choice of procedure was based solely on the surgeon’s discretion.
At our institutions, LPS is performed using standard fluoroscopic technique with a percutaneous system for sacral H-/U-type fragility fractures. In brief, localization of respective levels is performed and cannulated needles are placed through the pedicles of lumbar vertebrae and S1 under fluoroscopic control. Using a guide wire, which is advanced through the needle, pedicle screws are placed after removal of the needle. For SAI placement, we use a sacral entry point at the inferolateral aspect of the S1 foramen and aim towards the obturator outlet teardrop. In case of triangular stabilization, a TIS (S1 or S2 level) or (bilateral) SI screws are inserted subsequently.
TIS fixation using one screw is performed using a technique under fluoroscopic guidance adopted to the proposed procedure by Gardner and Routt.
11
If polymethylmethacrylate (PMMA) augmentation is indicated, we use in-line PMMA augmentation through the cannulation at the lateral masses (Figure 1).
12
In short, after defining the screw path using a guide wire, a 7.3 mm cannulated screw with a washer is advanced until its tip is placed at the near lateral mass. Subsequently, the guide wire is temporarily removed and an 8 G diameter Jamshidi needle is placed through the screw cannulation. Thereafter, 2-3 ml of PMMA are applied. After Jamshidi removal and reinsertion of the guide wire, the screw is further advanced to the far lateral mass. Cement augmentation is repeated in the same fashion at the contralateral site. After completion of cement application, the screw is fully advanced until final tightening is reached. Patients lacking an adequate corridor for the insertion of a single screw undergo treatment with bilateral SI screws utilizing standard fluoroscopic technique. Postoperatively, patients are encouraged to perform weight bearing as tolerated supported by crutches for 6 weeks. Transverse (A) and sagittal (B) CT reconstructed images of 78-year-old patient suffering a nondisplaced sacral H-/U-type fragility fracture showing a sufficiently sized corridor for S1 TIS placement. Surgery was performed using PMMA augmented TIS. First, a guide wire was placed (C). A 7.3 mm cannulated screw was inserted, and the guide wire temporarily removed. Using an 8 G Jamshidi needle, PMMA augmentation was performed at the ipsilateral sacral mass (D). The guide wire was reinserted and the screw further advanced. At the contralateral sacral mass, this procedure was repeated, and the screw advanced until its final position (F). Postoperative radiography showed satisfactory screw positioning and no PMMA leakage in overview (G), outlet (H), and inlet (I) projections.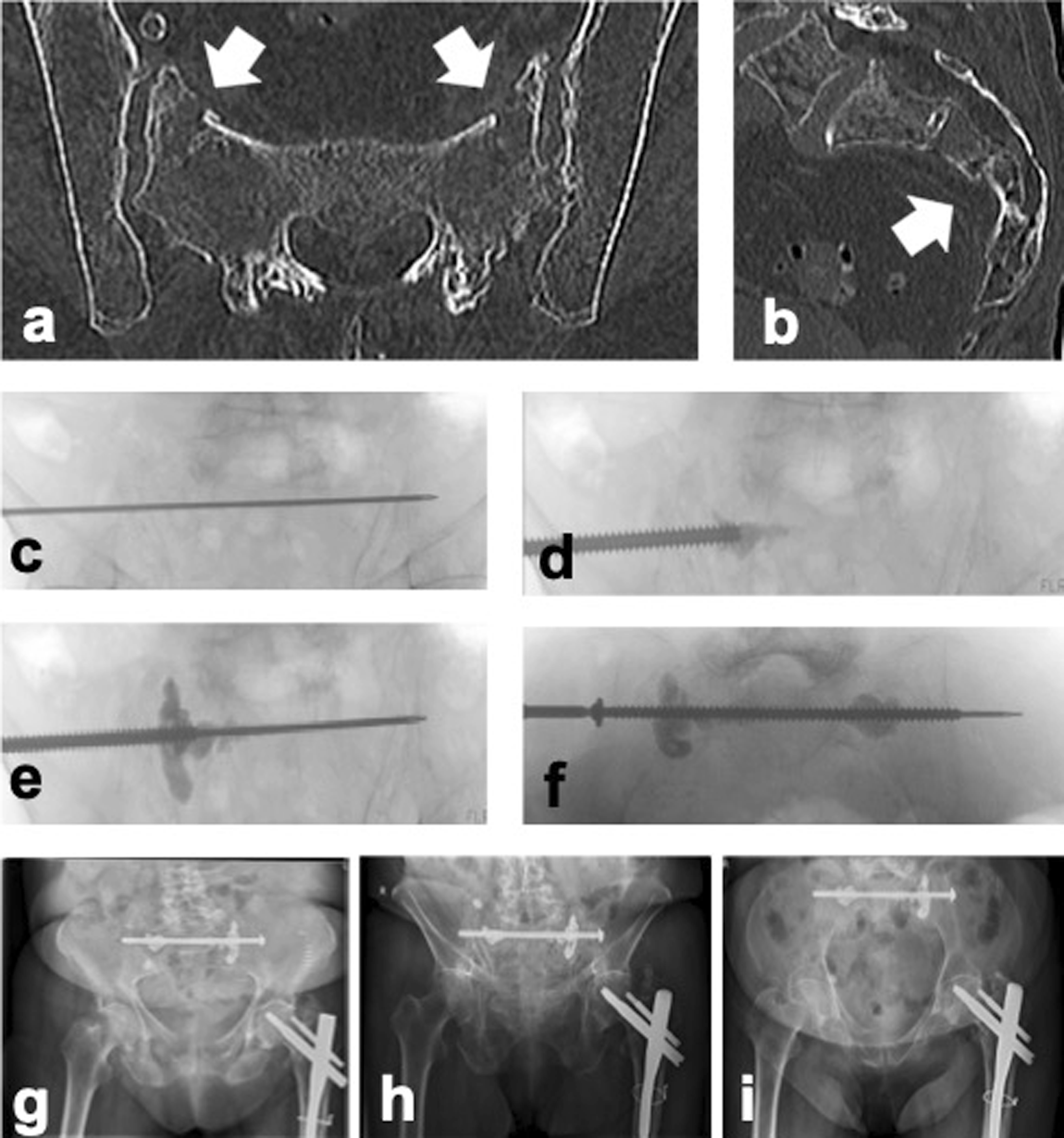
Regular follow-up consultations were scheduled at 6 weeks, 6 months, and one year postoperatively. All available follow-up data was included in the study synthesis.
The primary outcome measure in this study was the change in low back pain during the postoperative period, assessed using the visual analogue scale (VAS). An a priori sample size calculation was performed for the non-inferiority of the primary outcome, based on a minimally clinically important difference (MCID) of 3 points on the VAS. 13 The standard error was estimated as 3.45, calculated from the 95% confidence interval in 13 with an approximate standard deviation of 0.32 and 116 observations. A total of 44 patients were required to achieve a power of 80%. Mobility was assessed as full activity, walking with assistance, walking with assistance by another person, or confined to a wheelchair/bedridden. Secondary outcomes were evaluated only for patients not undergoing concurrent surgery and included the duration of surgery, blood loss, intraoperative and postoperative surgical complications, length of hospital stay, reoperations, implant failures, and mortality.
Statistical Analysis
Statistical analyses were conducted using R (R Foundation for Statistical Computing, Version 4.1.0, Vienna, Austria) and GraphPad Prism (GraphPad Software, Version 9.3.1, La Jolla, California). The sample size calculation was performed using a two-sample t-test. Descriptive statistics were presented as mean and standard deviation (SD) or median and interquartile range. The normal distribution was assessed using the Shapiro-Wilk test. Group comparisons were analyzed using t-tests and Mann-Whitney U tests. Frequency distributions were assessed using Chi-squared tests, and Fisher’s exact tests. The level of significance was set at P = 0.05.
Results
Participants
Demographic Parameters of Patients With Transiliac-Transsacral Screw Fixation (TIS) and Lumbopelvic Fixation (LPS).
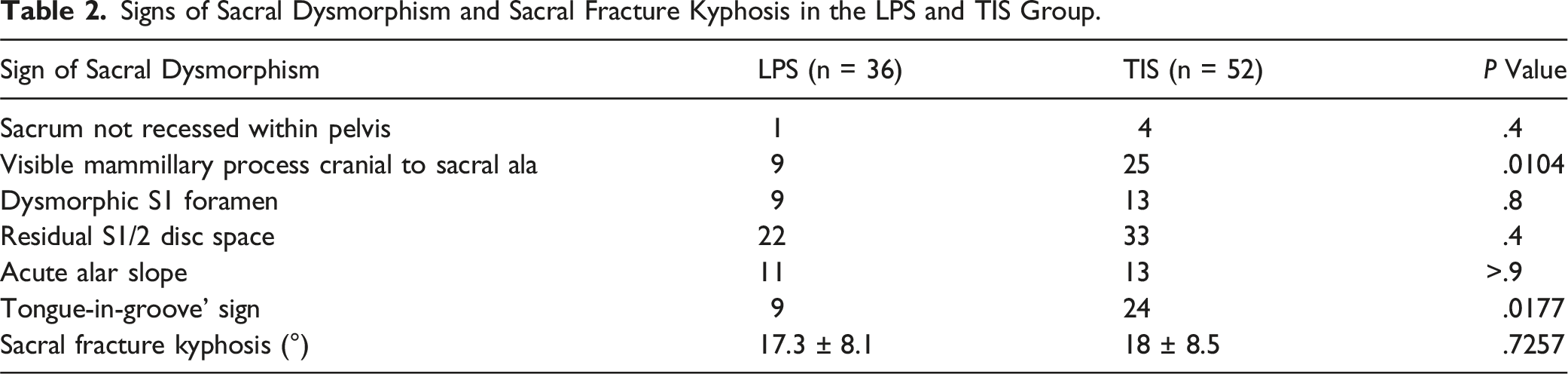
Signs of Sacral Dysmorphism and Sacral Fracture Kyphosis in the LPS and TIS Group.
Screw Configurations and Radiologic Parameters of TIS and LPS Groups.
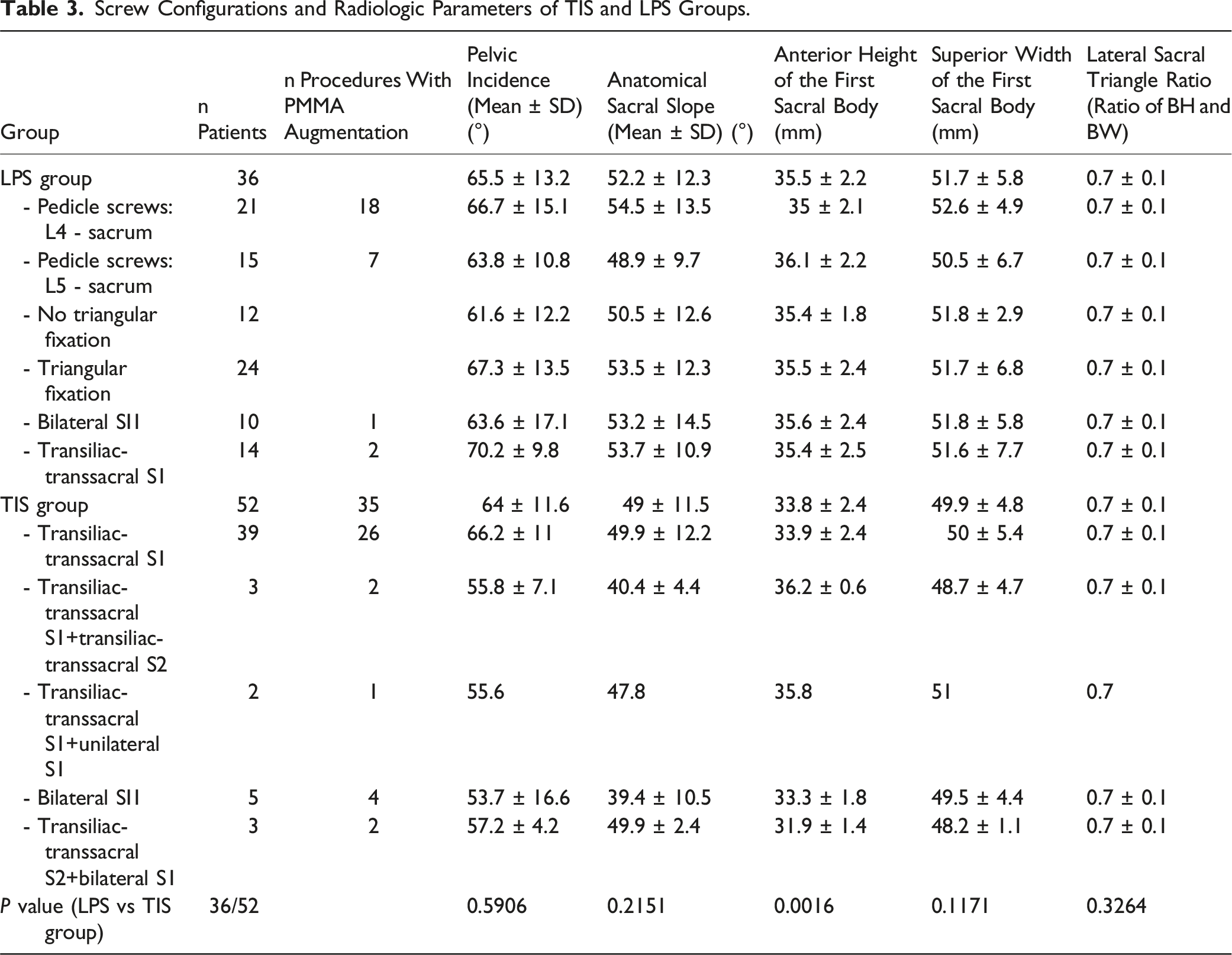
None of the patients in either group presented with acute neurological impairment resulting from the injury. In the TIS group, various screw configurations were utilized, with a single transiliac-transsacral screw at the S1 level being the most frequently employed configuration. Additionally, 35 patients (67%) in the TIS group underwent PMMA augmentation of the screw as part of the procedure. In the LPS group, 12 patients (33%) underwent lumbopelvic stabilization and 24 patients (67%) underwent bilateral triangular fixation (10 patients with bilateral SI screws, 14 patients with transiliac-transsacral screws at the S1 level). Further details regarding the screw configurations can be found in Table 3.
Osteosynthesis of the anterior pelvic ring was conducted during the same hospitalization as the index surgery in five patients (10%) in the TIS group and three patients (8%) in the LPS group. Subsequent orthopedic procedures involving the trunk, pelvis, and lower extremities during the follow-up period were performed in 6 patients (12%) in the TIS group (posterior decompression (n = 2), vertebroplasty (n = 4)) and in nine patients (75%) in the LPS group (posterior decompression (n = 5), vertebroplasty (n = 3), hip arthroplasty revision (n = 1).
Primary Outcomes
Low Back Pain & Pain Medication
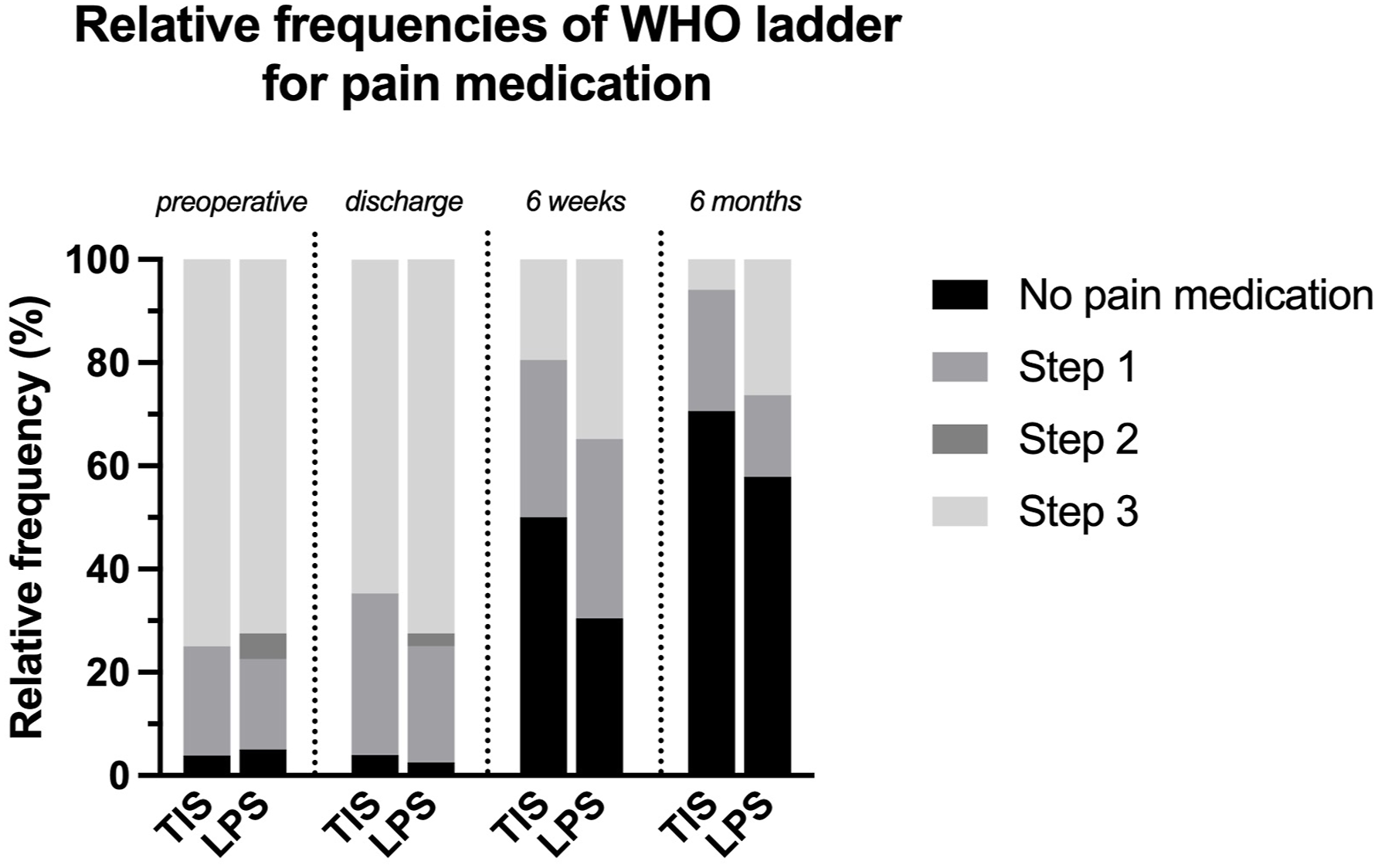
Postoperative low back pain levels showed a decline in both the TIS group and the LPS group, with a trend towards a more rapid decrease observed in the TIS group (Figure 2). However, there were no statistically significant differences in reported low back pain levels between the 2 groups preoperatively (P = 0.2) at discharge (P = 0.3), at 6 weeks postoperatively (P = 0.3), and at 6 months postoperatively (P = 0.8). Levels of pain medication requirements were not significantly different at the preoperative stage (P = 0.9), at discharge (P = 0.6), at 6 weeks (P = 0.2), and at 6 months (P = 0.3) postoperatively (Figure 3). Likewise, the frequencies of reported pain medications did not vary significantly between both groups at any of the timepoints (P > 0.2). Low back pain levels at discharge, at six weeks, and at six months postoperatively. There were no significant differences between both groups. Symbol – mean; whiskers – SD. Relative frequencies of WHO Pain medication ladder steps preoperatively, at discharge, at six weeks, and at six months postoperatively. There were no significant differences between both groups.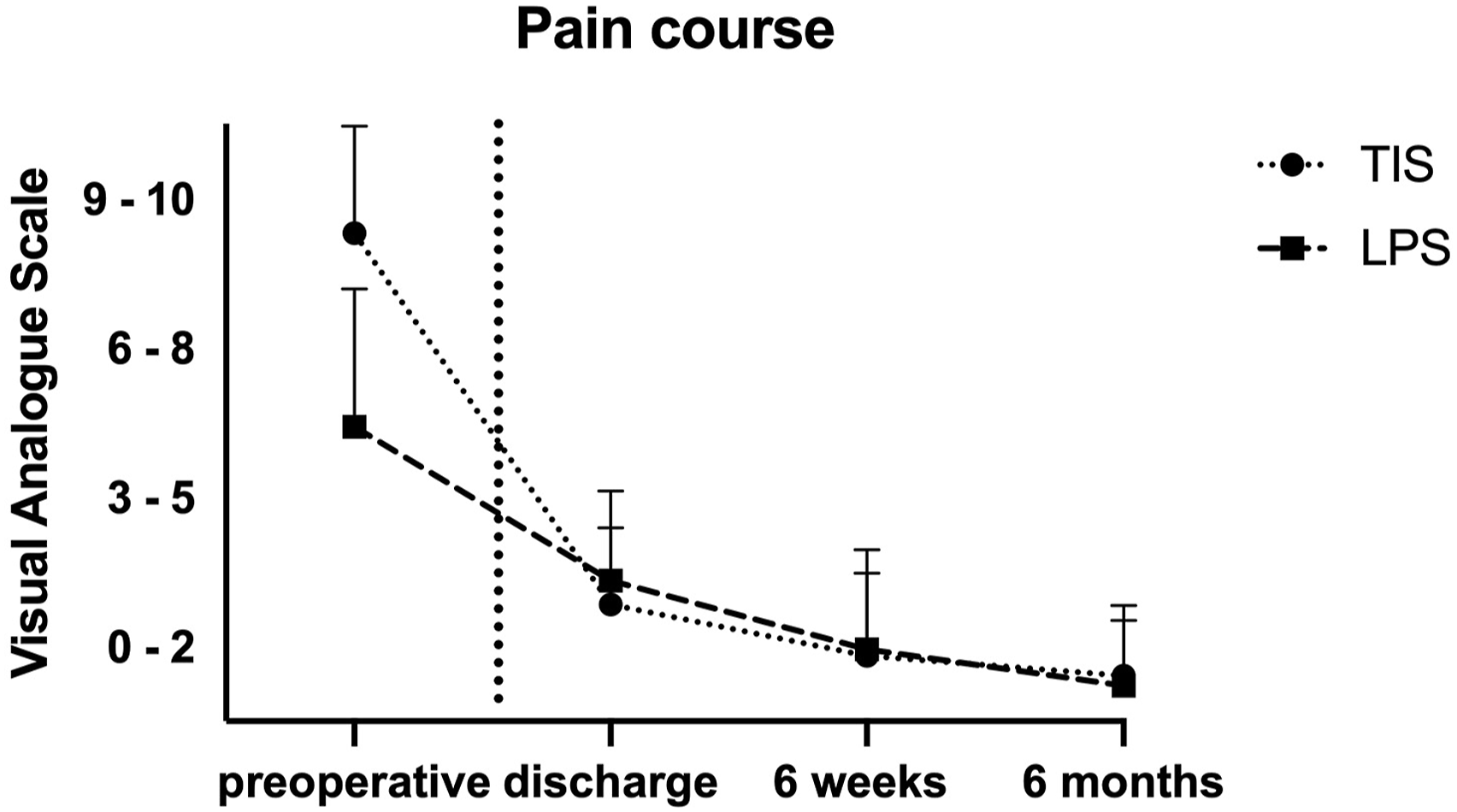
Mobility
The majority of patients in both the TIS group and the LPS group were able to regain ambulation with or without the use of walking aids during the postoperative period. Specifically, at six weeks postoperatively, 36 patients in the TIS group and 29 patients in the LPS group were able to walk independently or with the assistance of walking aids (Figure 4). Mobility levels preoperatively, at discharge, at six weeks, and at six months postoperatively. There were no significant differences between both groups. Symbol – mean; whiskers – SD.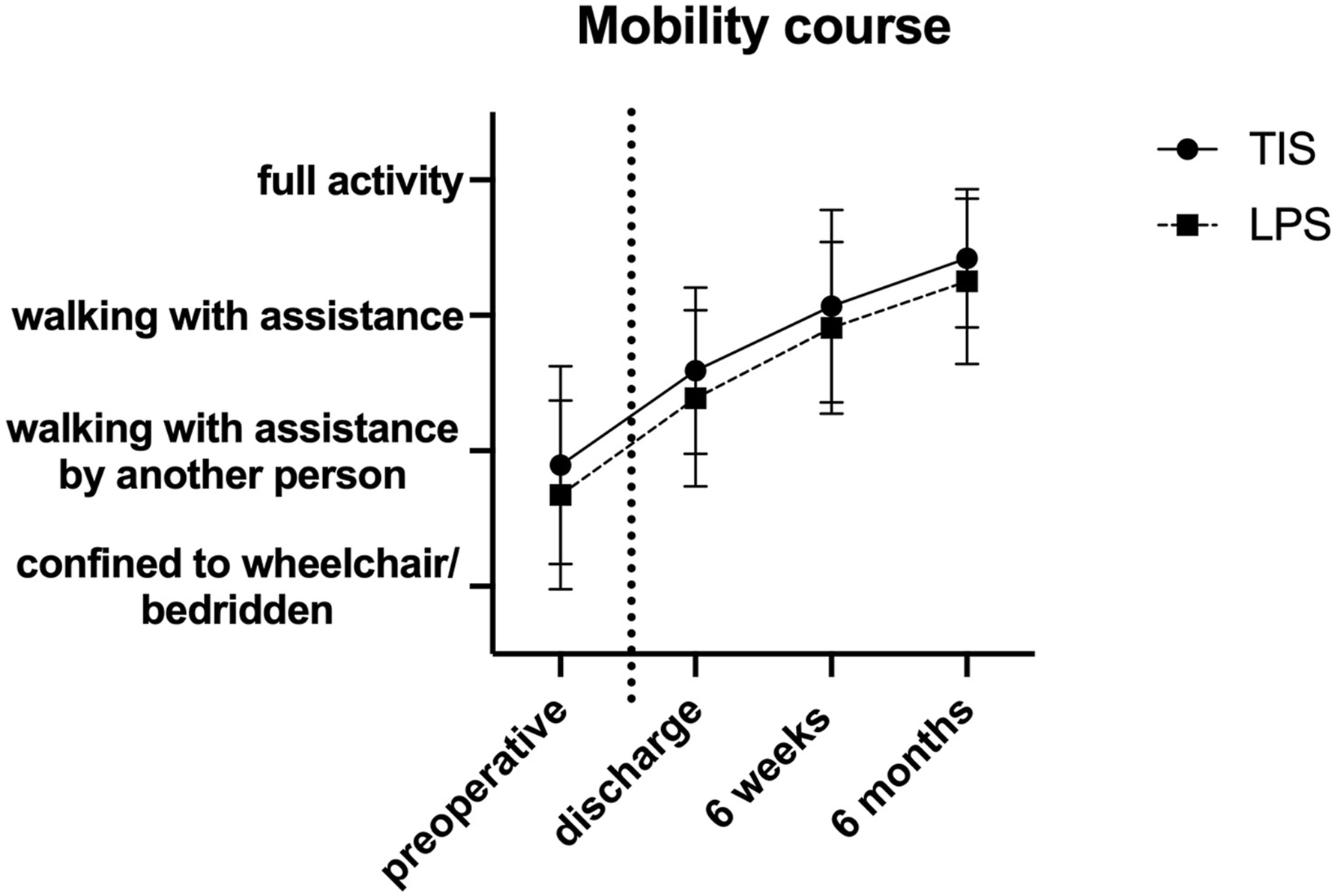
There were no significant differences observed between the 2 groups in terms of mobility levels before surgery (P = 0.2), at discharge (P = 0.3), at 6 weeks postoperatively (P = 0.3), and at 6 months postoperatively (P = 0.4).
Secondary Outcomes
Duration of Surgery & Blood Loss
For patients without concurrent surgery, in the TIS group, duration of surgery (36.3 ± 12.5 minutes) was significantly shorter compared to the LPS group (113 ± 30.5 minutes) (P < 0.0001; Figure 5). Intraoperative blood loss was significantly lower in the TIS group (median <20 mL) compared to the LPS group (median 125 mL) (P < 0.0001; Figure 6). However, there was no significant difference in the frequency of intraoperative blood transfusions between the TIS (n = 1) and LPS (n = 2) groups (P = 0.6). Boxplots showing the duration of surgery of both groups. Only cases with specified duration and without concomitant procedures were analyzed (n TIS = 39; n LPS = 25). There was a significant difference. **** - P < .0001; line - median; whiskers – range min to max. Boxplots showing the intraoperative blood loss for both groups. There was a significant difference. **** - P < .0001; line - median; whiskers – range min to max.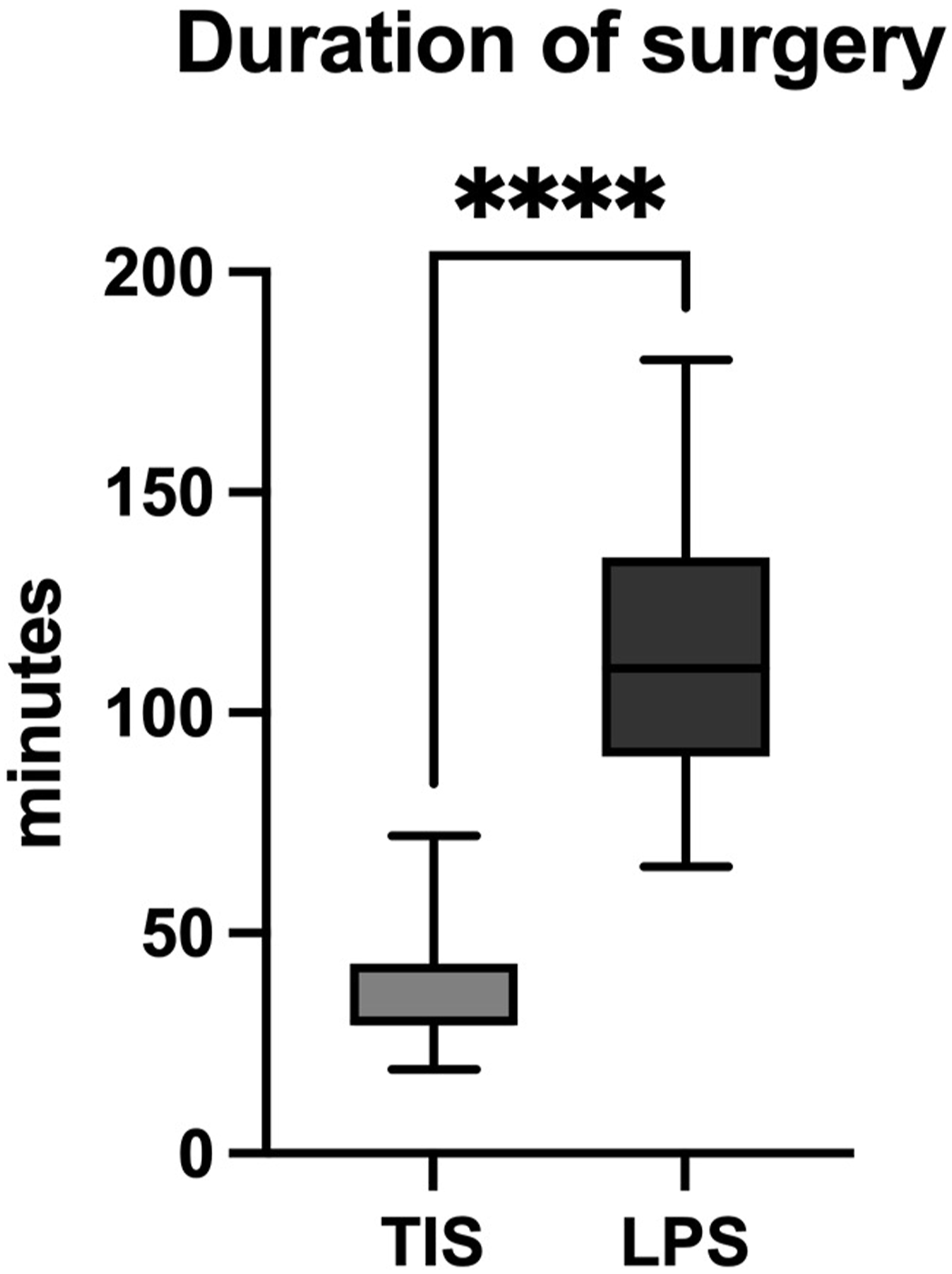
Intraoperative Adverse Events
The occurrence of surgical intraoperative adverse events was observed in five patients of the TIS group and four patients of the LPS group (P > 0.9). In the TIS group, these events primarily included cement leakage that did not require further intervention (n = 5). Likewise, in the LPS group, adverse surgical events consisted of cement leakage not requiring further intervention (n = 4).
General intraoperative adverse events were observed in 2 patients of the TIS group and 2 patients of the LPS group (P > 0.9). In the TIS group, these events included a tooth fracture (n = 1) and laryngeal edema following an allergic reaction (n = 1). Notably, no cardiovascular or pulmonary intraoperative adverse events were reported in the TIS group. Conversely, in the LPS group, one patient experienced a cardiovascular event and another patient suffered from acute bleeding anemia.
Postoperative New Onset Neurological Impairment
Postoperative new onset radicular impairment occurred less frequently in the TIS group compared to the LPS group, but there was no significant difference (P = 0.3).
In the TIS group, one patient who underwent PMMA augmented transiliac-transsacral S1 screw and unilateral sacroiliac screw osteosynthesis experienced new onset S1 hypesthesia. This impairment did not require any further intervention and did not show improvement up to 6 months postoperatively. Radiographic evaluation did not reveal any leakage of PMMA outside of the bone.
In the LPS group, postoperative new onset radicular impairment was observed in three patients. One patient presented with an L4 motor palsy. Postoperative CT and MR imaging revealed no evidence of screw mispositioning or nerve root compression. Despite this, the patient did not exhibit short-term recovery and subsequently underwent surgical decompression 7 days later. However, there was no motor improvement observed up to 6 months following the operation. Another patient in the LPS group experienced mild postoperative L4/5 weakness, which was found to be due to sacroiliac screw mispositioning. This patient recovered after revision surgery. One patient with postoperative L5 hypesthesia in the LPS group recovered without requiring any intervention.
Length of Stay
The median length of stay in the TIS group was 11 days, which was significantly shorter compared to the LPS group with a median of 14 days (P = 0.0047; Figure 7). Boxplots showing the length of hospital stay of both groups. There was a significant difference. * -P < .05; line - median; whiskers – 10-90 percentile.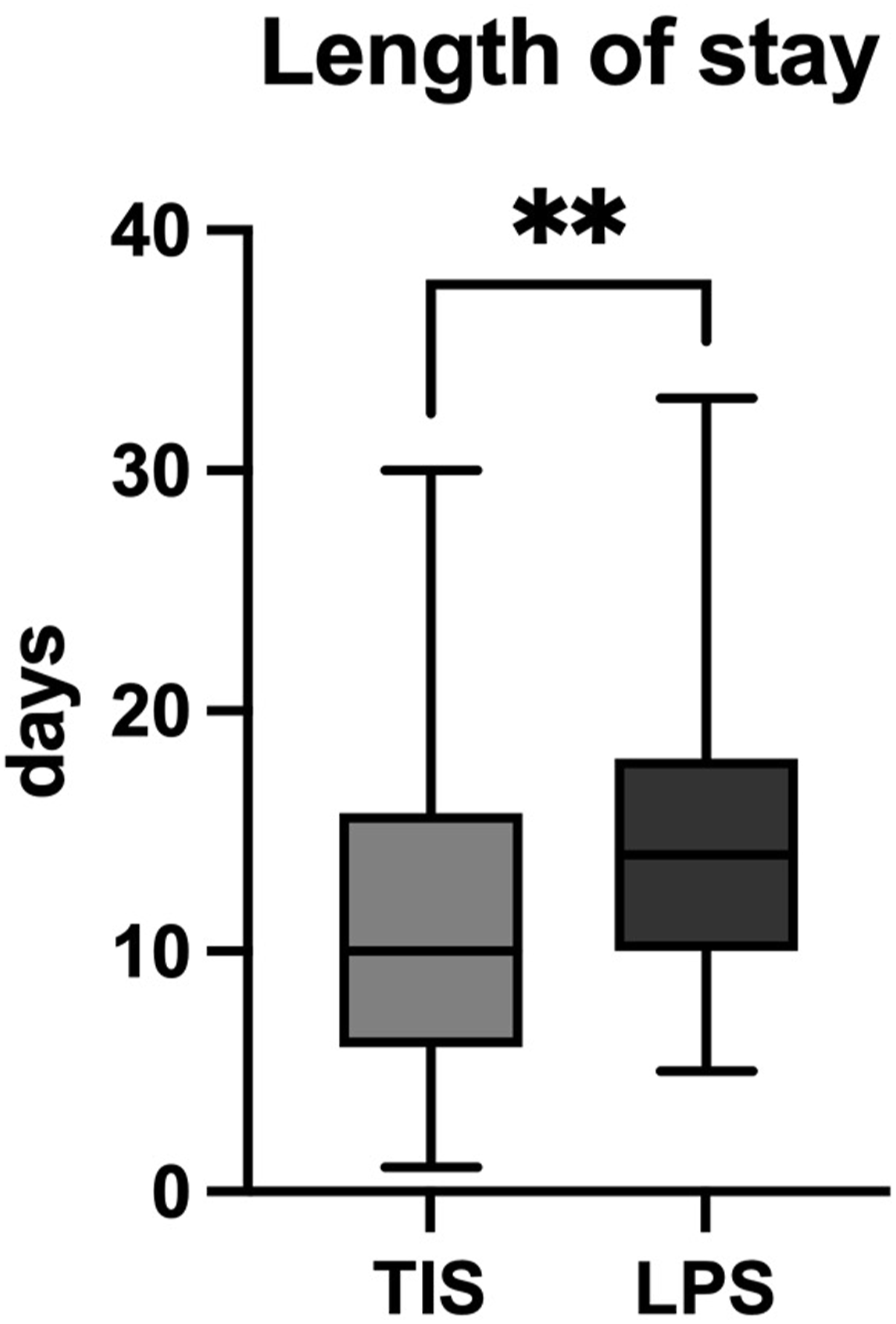
Reoperations Directly Related to the Index Surgery
The TIS group exhibited a significantly lower rate of reoperations directly related to the index surgery (n = 2) compared to the LPS group (n = 10; Figure 8; P = 0.0028). Relative frequencies of reoperations directly related to the index surgery.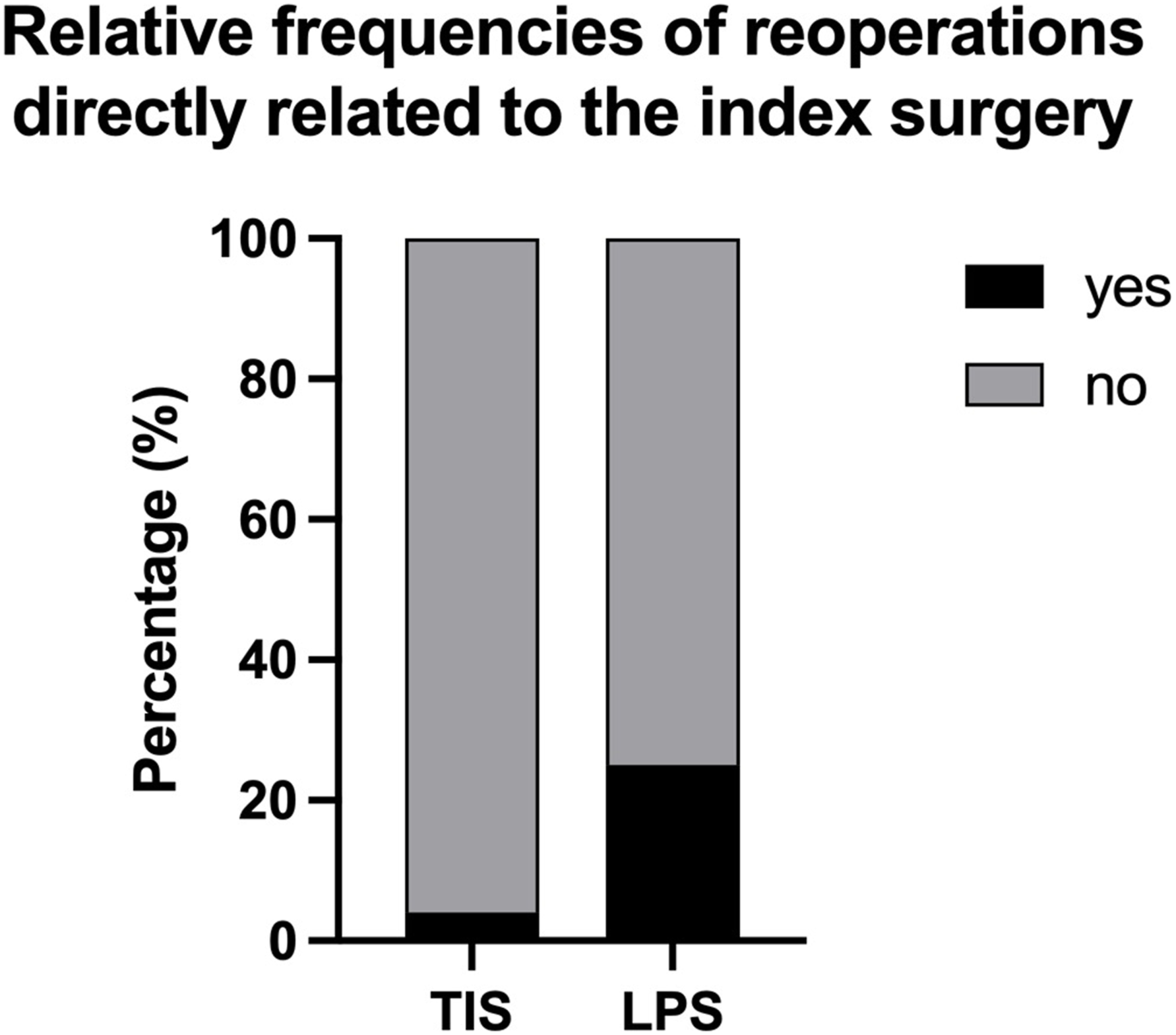
In the TIS group, one patient required revision surgery (transiliac-transsacral S1 screw replacement with PMMA augmentation and posterior plating) 7 weeks postoperatively due to an L5 motor deficiency caused by atraumatic screw migration. Another patient presented with a painful nonunion of the anterior pelvic ring one year postoperatively and subsequently underwent anterior symphyseal plating.
In the LPS group, three reoperations were necessary due to superficial or deep postoperative wound infection of the posterior midline approach. Another patient with mild postoperative L4/5 weakness resulting from sacroiliac screw malposition underwent sacroiliac screw replacement on the first postoperative day. Additionally, one patient underwent surgical decompression 7 days after surgery due to postoperative L4 palsy. Two patients developed ASD at L3/4 2 years after the initial operation and underwent extension of the posterior fusion to L3. Furthermore, three patients in the LPS group underwent implant removal due to implant loosening, suspected chronic hardware infection, and ASD prophylaxis.
Reoperations Not Directly Related to the Index Surgery
In the TIS group, one patient experienced traumatic screw dislocation (no PMMA augmentation) after a fall 22 days after the index surgery. This patient underwent revision surgery with PMMA augmented transiliac-transsacral screw and lumbopelvic fixation from L5 to the pelvis. Another patient in the TIS group was diagnosed with an L5 fracture and concomitant L5 motor deficit three months after the index operation, leading to a conversion surgery to lumbopelvic fixation from L4 to the pelvis. A third patient in the TIS group, who had previously undergone fusion at L4/5, presented with ASD at L3/4 with an L4 motor deficit four months after transiliac-transsacral screw fixation. This patient underwent lumbopelvic fixation from L2 to the pelvis and anterior lumbar interbody fusion (ALIF) at L5/S1.
Implant Failure
No implant failures were seen in the TIS group. Implant failures were only observed in the LPS group (n = 1). One patient in the LPS group experienced SAI screw breakage three months after the initial surgery, but no further intervention was necessary.
Mortality
During the follow-up period, 2 patients in the TIS group died. One of these patients, who had pre-existing serious medical conditions, opted to discontinue therapy following a multidisciplinary consultation and succumbed 12 days after the operation.
Discussion
In this retrospective bi-centric comparative cohort study, we evaluated the outcomes and complications of TIS and LPS in patients with H-/U- type spinopelvic dissociations in fragility fractures of the sacrum. Our findings indicate that both TIS and LPS are effective in reducing low back pain and restoring mobility during an average 52-month follow-up period. However, TIS demonstrated advantages in terms of shorter surgery duration, reduced blood loss, and lower rates of reoperations directly related to the index surgery.
Recently, Gross et al 6 proposed an algorithm for the treatment of H-/U-type spino-pelvic dissociation injuries using TIS and LPS, considering factors such as the level of the transverse fracture component and the availability and size of a transiliac-transsacral corridor based on a cohort of 23 patients. Yet, the clinical advantages and performance of TIS in high-grade posterior lesions has not been thoroughly investigated. To our knowledge, this is the first retrospective study with an adequate sample size and follow-up period to examine the clinical outcomes of either LPS or TIS in H-/U- type spinopelvic dissociations in fragility fractures of the sacrum. Previous clinical studies addressing this topic lacked control groups and have investigated high-energy fractures, a variety of different pelvic fracture types, and small sample sizes.4,14-16
In cases of sacral H-/and U-type fractures, LPS offers the restoration in multiple planes, including the horizontal and vertical planes of the lumbosacral junction. 17 Compared to lumbopelvic stabilization alone, biomechanical studies have demonstrated superior stability of triangular lumbopelvic fixation constructs. 18 Therefore, it is considered the standard of care for high-energy fractures. 19 However, there is a lack of clinical evidence as to when triangular stabilization is superior to lumbopelvic stabilization in the geriatric population with low-energy or atraumatic spinopelvic dissociation injuries. Although biomechanical studies and recent recommendations favor triangular over lumbopelvic stabilization, in cases with minimal displacement, lumbopelvic stabilization without triangular fixation component may be sufficient even in high-energy trauma. 20
However, it is important to note that LPS may not be necessary in older patients with low energy/atraumatic spinopelvic dissociation (AOSpine Sacral type C0), unless there is significant involvement of the lumbar spine, such as the presence of new onset neurological impairment. This is in contrast to high-grade spinopelvic dissociation resulting from high energy trauma, which often involves the destruction of stabilizing surrounding tissues.
The percutaneous technique of TIS screw placement was introduced by Chip Routt in 1993 for sacroiliac (SI) screw placement. 21 Safe screw corridors can be identified using Carlson’s antero-superior pointed ‘vestibule concept’. 22 The rationale for using TIS instead of bilateral SI screws is based on the increased stability provided by screws that reach the opposite sacroiliac joint. 23 Additionally, TIS allows for better distribution of craniocaudal forces along the longer screw length, increased screw thread purchase in the opposite iliac cortex, and greater compressive forces on the fracture and/or sacroiliac joint.24,25 However, the use of TIS remains limited to the treatment of non-displaced fragility fractures of the pelvis (FFP II) and reduced (FFP III and IV) posterior Denis zone 1 and 2 lesions exhibiting sufficiently sized corridors for safe screw placement.
As a consequence, our study specifically included patients with fragility fractures that were nondisplaced or minimally displaced (AOSpine Sacral type C0) and caused by atraumatic or low-energy trauma. As a result, the study population primarily consisted of geriatric patients, whose demographic characteristics were representative of the typical medical and general health conditions expected in this population.
No significant differences in low back pain levels, pain medication usage, and mobility were observed between the TIS and LPS groups at the time of hospital discharge in our study. However, in a prospective, non-randomized, case-controlled study by Mendel et al 26 involving 73 patients with bilateral fragility fractures of the sacrum, greater restoration of mobility was reported at discharge in patients treated with bisegmental transsacral stabilization compared to LPS. It is important to note that their study had a shorter follow-up period that only extended until discharge and included patients with less severe injuries. Given the significantly shorter length of hospital stay in the TIS group in our study, and the fact that discharge is typically considered when pain levels and mobility are deemed satisfactory, further evaluation of the potential benefits of TIS in terms of pain and mobility may be warranted, such as through a prospective study design.
The shorter surgery duration and reduced blood loss observed in the TIS group compared to the LPS group align with our expectations and are consistent with findings from previous studies.26,27 The use of percutaneous 3D navigated TIS insertion may contribute to safer and more accurate screw placement, although it does result in a longer surgery duration compared to fluoroscopically guided TIS insertion (53 ± 13 min in previous study 16 vs 36 ± 13 min in this study).
In comparison to TIS, pedicle screw instrumentation is essential in LPS. Despite being uncommon, the misplacement of pedicle screws presents a significant risk to neural structures. Screw mispositioning reportedly necessitates revision rates ranging from 0.3% to 8.6% similar to the 3% reoperation rate reported in the present study.28-30 Advanced techniques, such as robot-assisted pedicle screw placement, has been shown to result in significantly greater positioning accuracy while significantly reducing intraoperative radiation time and dosage compared to the conventional open freehand and conventional minimally invasive fluoroscopic techniques.31,32 Moreover, technological advancements of next-generation robotic systems, incorporating a real-time optical camera and multijointed arm, can further enhance positioning accuracy, 33 which subsequently decreases the rate of neurologic impairment attributable to implant malpositioning.
In our study, reoperation indications directly related to the index surgery, such as superficial/deep infection and ASD, were observed. However, these complications were not observed after TIS fixation in our study or reported as common in the literature.14,26
Implant loosening is a commonly reported complication following percutaneous screw osteosynthesis of the posterior pelvis. In a study by Kramer et al, 16 they reported a screw loosening rate of 19% in their cohort of 56 patients treated with TIS for various fragility fractures of the pelvis. Interestingly, a posterior H-type configuration was not associated with screw loosening. Biomechanically, screw loosening is influenced by the nutation/counternutation of the sacroiliac joint (SIJ), leading to rotational moments that cause the screw to rotate within the cancellous bone of the ala. 24 Screw fixation perpendicular to the fracture line/SIJ provides compression at both sites, increasing friction at the SIJ and enhancing resistance to upward vertical shear forces between the sacrum and the innominate bone. In cases of osteoporotic bone with lower bone quality, compression forces are reduced, which can contribute to screw loosening. Some authors recommend the use of multiple TIS inserted from opposite directions in cases of bilateral vertical sacral fractures.6,24 In our TIS cohort, 39 of 52 patients received only one TIS, and atraumatic screw loosening and migration was only seen in one case (3%) without PMMA augmentation. Recent studies have demonstrated that PMMA augmentation and angular displacement of the ilium in relation to the screw at the level of the lateral mass can reduce the combined angular displacement in flexion and internal rotation in human pelvic cadavers with fragility fractures. 12 However, the use of PMMA carries the risk of leakage and subsequent neural compromise, particularly to the L5 nerve root. 34 Nonetheless, among the 35 patients receiving PMMA augmentation in our study, no complications related to PMMA leakage were observed. In summary, our findings indicate, that one TIS with PMMA augmentation is safe and sufficient for the treatment of nondisplaced and minimally displaced sacral U-type fragility fractures.
Our study has several limitations that should be acknowledged. Firstly, the retrospective nature of the study design introduces inherent biases and limitations in data collection and analysis. For example, mobility was not systematically assessed based on a specific score due to the retrospective nature of the study. Secondly, the lack of randomization and absence of a treatment algorithm resulted in the choice of procedure being based solely on the surgeon’s preference, which may have introduced selection bias. It is possible that fractures with larger dislocation were more likely to be stabilized using LPS. However, it is important to note that only nondisplaced and minimally displaced fractures (AOSpine Sacral type C0) were included and that the fracture types were similar between the LPS and TIS groups, minimizing the potential impact of this bias on our findings. In the sample size calculation, we assumed a substantial difference in VAS scores between the 2 groups. However, our findings indicate that the difference in VAS scores between the groups was minimal, suggesting that the initially defined difference may not be relevant in relation to the primary outcome. Additionally, some baseline parameters, such as the preoperative ambulation status were unavailable in the medical records, and patient reported outcome measures were not collected.
Conclusion
In this retrospective bi-centric comparative cohort study of nondisplaced and minimally displaced sacral H-/U-type fragility fractures, TIS fixation was comparable to LPS in terms of low back pain reduction and mobility restoration. However, TIS showed several benefits, including shorter surgery duration, reduced blood loss, shorter hospital stay, and lower reoperation rates. Additionally, the use of PMMA augmentation in TIS is believed to enhance stability and prevent common failure modes. Although not the primary focus of our study, the potentially lower overall costs associated with TIS, considering the aforementioned factors and implant expenses, should not be underestimated. While based on our findings, we recommend the use of PMMA-augmented TIS over LPS for the treatment of nondisplaced and minimally displaced sacral H-/U-type fragility fractures, prospective randomized studies should be conducted to substantiate these findings and develop distinct treatment recommendations.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Jan Gewiess, Ysaline Emilie Roth, and Christoph Albers. The first draft of the manuscript was written by Jan Gewiess and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partly funded by the Wyss Foundation USA.