
Abstract
Study Design
Retrospective cohort study.
Objectives
Gabapentinoids have been increasingly studied as a non-narcotic option for neuropathic and postoperative pain. However, there is evidence suggesting that off-label use of these medications for the treatment of isolated LBP is not effective. The purpose of the current study was to evaluate prescription patterns for gabapentinoids among patients with isolated low back pain.
Methods
Adult patients with LBP were abstracted from the 2019 M91Ortho PearlDiver dataset using International Classification of Diseases (ICD-10) code M54.5. Patients were excluded if they had a diagnosis of neurologic symptoms, history of spinal surgery, spinal fracture, or conditions for which gabapentinoids are FDA approved. Gabapentinoid and narcotic prescriptions within one year of LBP diagnosis were identified. Patient characteristics and prescriber specialty were extracted from the dataset and predictors of gabapentinoid prescriptions were determined using univariate and multivariate analyses.
Results
Among the 1,158,875 isolated LBP patients, gabapentinoids were prescribed for 11%, narcotics for 8%, and both for 3%. The most common prescriber specialties included: primary care physicians (45%), nurse practitioners (15%), and pain management physicians (5%). Independent predictors of gabapentinoid prescriptions included: female sex, region of the country, and insurance type (P-values <.001).
Conclusions
Of nearly 1.2 million patients with isolated LBP, 14.2% were prescribed gabapentinoids within one year of their LBP diagnosis. Patient characteristics predictive of receiving gabapentinoids were predominantly non-clinical factors.
Introduction
Low back pain (LBP) is a leading cause of disability worldwide.1-3 In the context of the ongoing opioid epidemic, attempting to minimize the use of narcotics is a clear priority.4,5 Non-narcotic modalities 6 and medications7-9 are increasingly considered, however, the evidence for some of these pain management strategies remains limited.
A review of the literature tells us that narcotics are frequently considered for chronic LBP.8,9 Citing the risk of overdose and the development of opioid use disorder, in 2016 the Centers for Disease Control and Prevention (CDC) published guidelines limiting such practices. 4 Nonsteroidal anti-inflammatory drugs (NSAIDs) have been well established for the management of such pain,7-9 however, these medications have well-defined side effects 10 and there has been a desire for additional non-narcotic options.
In recent years, physicians have increasingly turned to gabapentinoids for pain management.11,12 This group includes gabapentin and pregabalin (together referred to as gabapentinoids), which are Food and Drug Administration (FDA) approved as adjunctive therapy in the treatment of seizures and for the treatment of postherpetic neuralgia.13,14 Pregabalin is additionally approved for fibromyalgia, neuropathic pain associated with diabetic peripheral neuropathy, and neuropathic pain associated with spinal cord injury. 13 There is also literature to support the use of gabapentinoids for the treatment of neuropathic pain, 15 radiculopathy,15,16 claudication, 17 and postoperative spine pain.18,19
The question has been raised if gabapentinoids are useful as a non-narcotic option for axial LBP. A randomized control trial of 108 patients with chronic LBP found that, while patients in the gabapentin group reported reduced pain after 12-weeks, there were no differences in pain or disability scores compared to placebo. 20 Additionally, two recent meta-analyses concluded that gabapentinoids were not effective in reducing pain or disability in patients with isolated LBP.21,22 Taken together, the literature does not support the off-label use of gabapentinoids for the treatment of isolated LBP.
As with any medications, the potential advantages of gabapentinoids need to be considered in relation to disadvantages. Gabapentinoid use is associated with side effects, including dizziness, fatigue, difficulties with mentation, and visual disturbances.11,21,22 While initially assumed to have no misuse potential, reports of gabapentin and pregabalin misuse are also appearing.11,12
Despite the lack of support in the literature, it suspected that gabapentinoids are commonly prescribed for isolated LBP. Thus, the goal of the current study was to further characterize the use (and predictors of use) for gabapentinoids for isolated LBP in a large national administrative dataset.
Methods
Study Population
The current study used data from the M91Ortho PearlDiver data set (Colorado Springs, CO). 23 This dataset is composed of national administrative claims data from approximately 91 million orthopedic patients. Since the data is aggregated and deidentified, our Institutional Review Board (IRB) found studies using PearlDiver to be exempt from the informed consent requirement.
Patients with LBP diagnosed between January and December 2019 were identified using International Classification of Diseases (ICD-10) code M54.5. This diagnostic code captures a wide range of patients with muscular tension or stiffness in the lower back. To ensure the study population was comprised of patients with isolated, axial LBP, patients were excluded if they had diagnoses that included radiculopathy or sciatica.
To be included in the analysis, patients must have been active in the database for at least one year following LBP diagnosis. Patients were excluded if they were younger than 18 years of age. Furthermore, patients were excluded if they had a history of spinal surgery, lumbar vertebral fracture, or conditions for which gabapentinoids are FDA approved (epilepsy, postherpetic neuralgia, diabetic peripheral neuropathy, fibromyalgia, and spinal cord injury). A total of 1,158,875 isolated LBP patients were included in the study (Figure 1). Flowchart detailing initial patient population and all exclusions applied to the sample. Total patients included and excluded are shown.
Outcome Variables
Once the above-noted back pain population was isolated, prescription records were assessed. New onset gabapentinoid prescriptions within one year of LBP diagnosis were analyzed to determine the following: incidence of gabapentin and pregabalin use, incidence of gabapentinoid use relative to narcotics, and prescriber specialty.
Patient characteristics were also assessed. These included: age, sex, Elixhauser Comorbidity Index (ECI, a standardized measure of overall comorbidity burden), geographic region where the patient lived, and insurance type.
Data Analysis
Patient demographic characteristics were compared between LBP patients receiving a gabapentinoid prescription within one year of diagnosis vs LBP patients not receiving a gabapentinoid prescription within this time period. The Pearson chi-squared test was used for sex, geographical region, and insurance type, and the Welch t-test was used for age and ECI. These analyses were followed by multivariate logistic regression.
Data analysis was performed using PearlDiver’s internal software, with statistical significance set at P < .001. Figures were created using Microsoft Excel 16 (Microsoft Corporation, Redmond, WA) and GraphPad Prism 9 (GraphPad Software, San Diego, CA).
Results
Study Population
Among the 1,158,875 isolated LBP patients, within one year of LBP diagnosis gabapentinoids were prescribed for 11% (gabapentin for 85%, pregabalin for 12% pregabalin, and both for 3%), narcotics for 8%, and both for 3%. The distribution of these groups is show in Figure 2. Chart showing the percentage of low back pain patients receiving a gabapentinoid or narcotic prescription within one year of diagnosis (left). Gabapentinoid prescriptions are further broken down into patients receiving a prescription for pregabalin or gabapentin (right).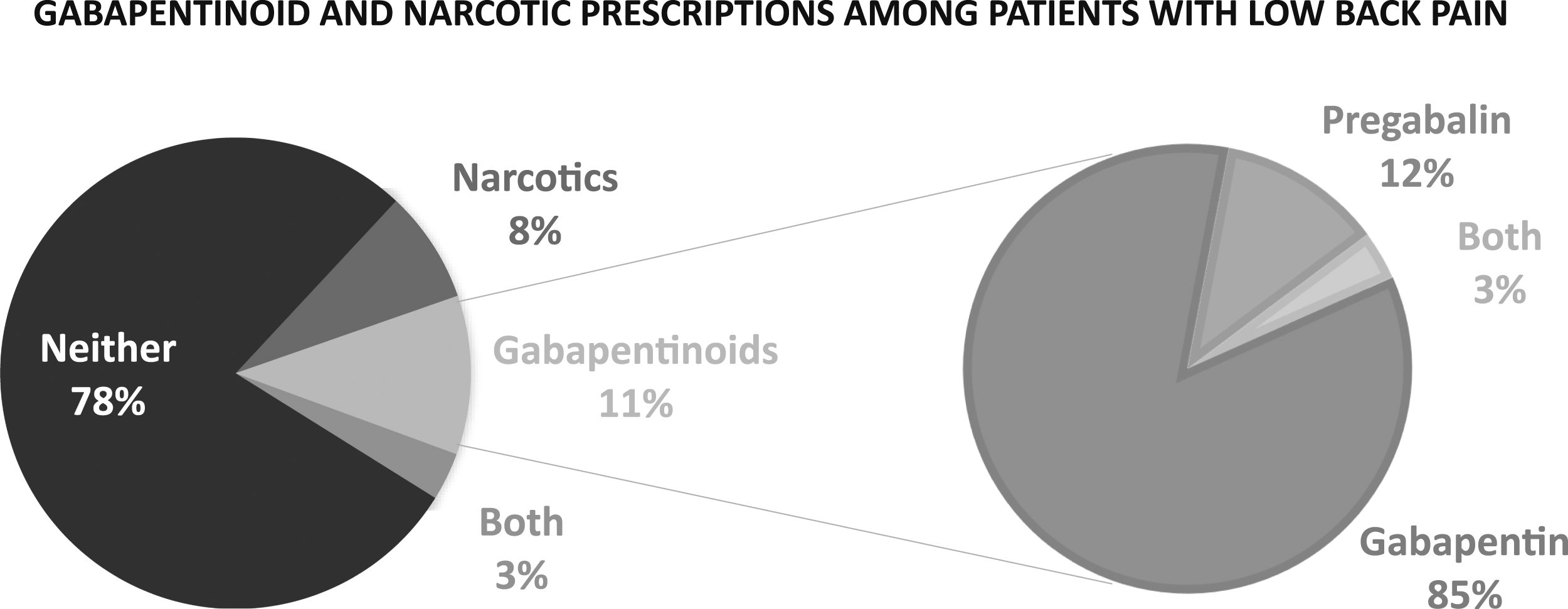
In examining who was prescribing gabapentinoids (Figure 3), primary care made up 45% of prescribers and nurse practitioners made up 15%. The remaining prescribers were pain management (5%), neurology (4%), physical medicine and rehabilitation (4%), psychiatry (3%), rheumatology (2%), orthopedic surgery (2%), unknown (11%), and other fields (9%). Chart depicting percentage of total gabapentinoid prescriptions received by patients with low back pain broken down by prescriber specialty.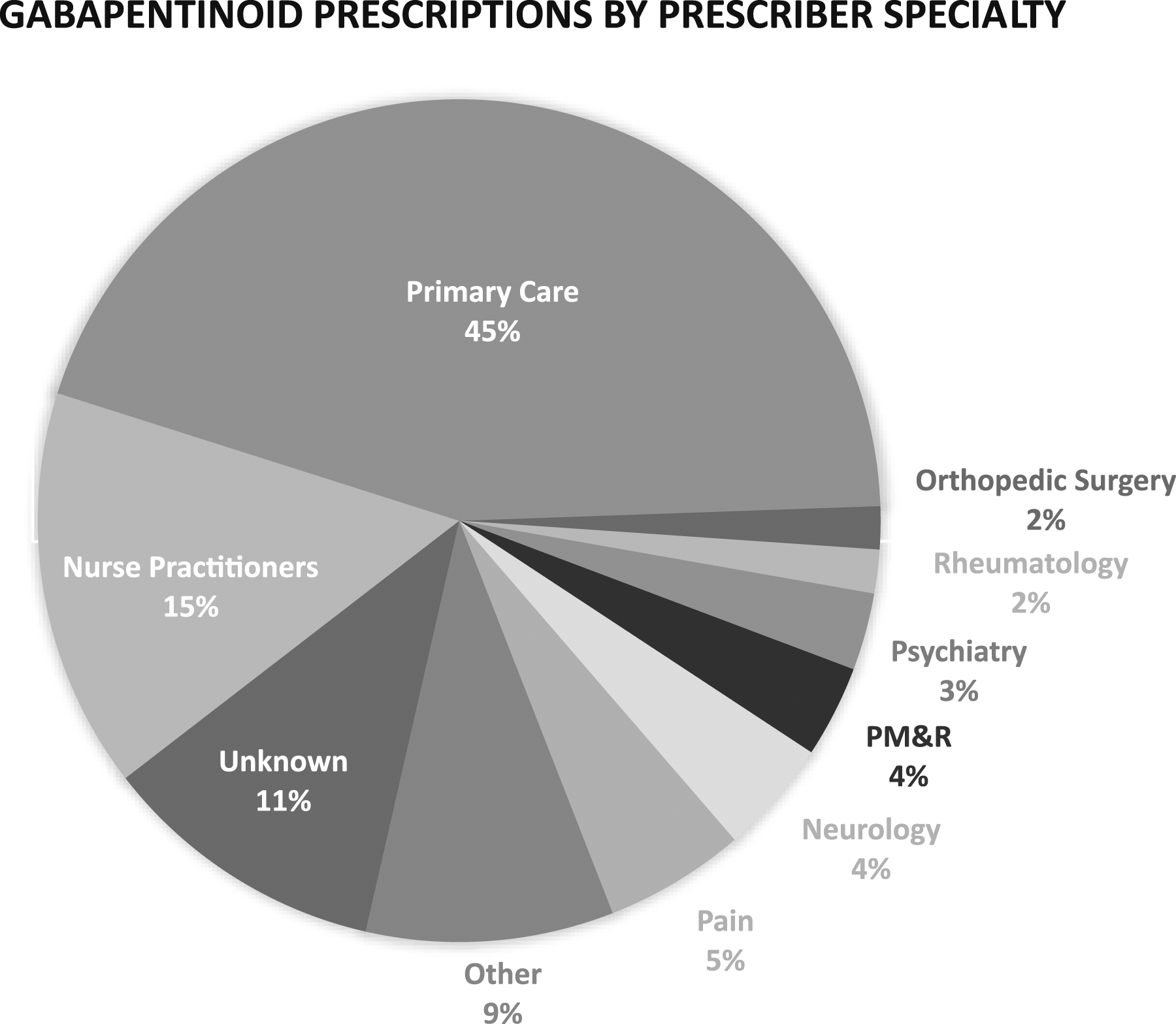
Predictors of gabapentinoid Prescription
Univariate Analysis of Characteristics of Patients With Low Back Pain.
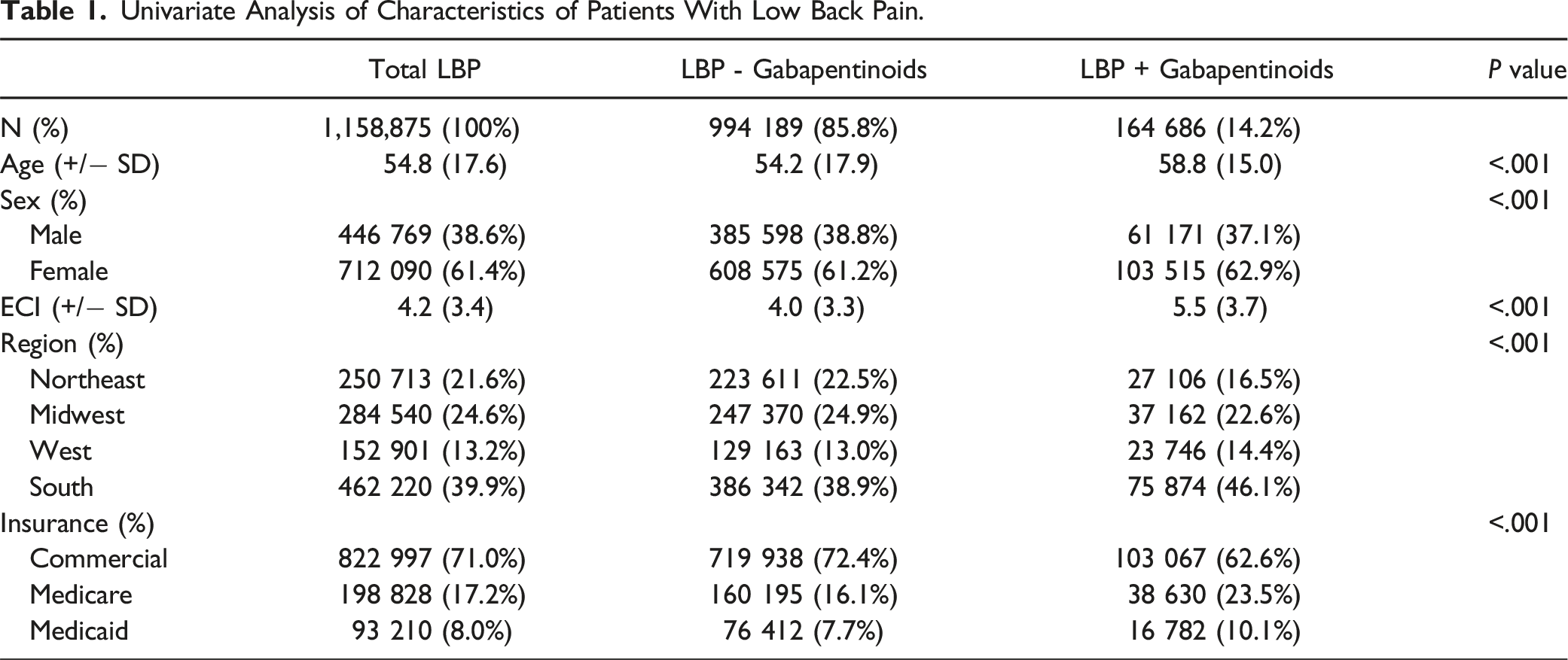
The average age (SD) in years of total, gabapentinoid negative, and gabapentinoid positive patients were 54.8 (17.6), 54.2 (17.9), and 58.8 (15.0), respectively (P-value <.001). The average ECI (SD) of total, gabapentinoid negative, and gabapentinoid positive patients were 4.2 (3.4), 4.0 (3.3), and 5.5 (3.7), respectively (P-value <.001). The number of females (percent) of total, gabapentinoid negative, and gabapentinoid positive patients were 712 090 (61.4%), 608 575 (61.2%), and 103 515 (62.9%), respectively (P-value <.001). Lastly, the breakdown of the locations and insurance providers for patients was statistically different (P-value <.001) between groups.
Multivariate Analysis of Predictive Factors for Gabapentinoid Prescriptions Among Patients With Low Back Pain.
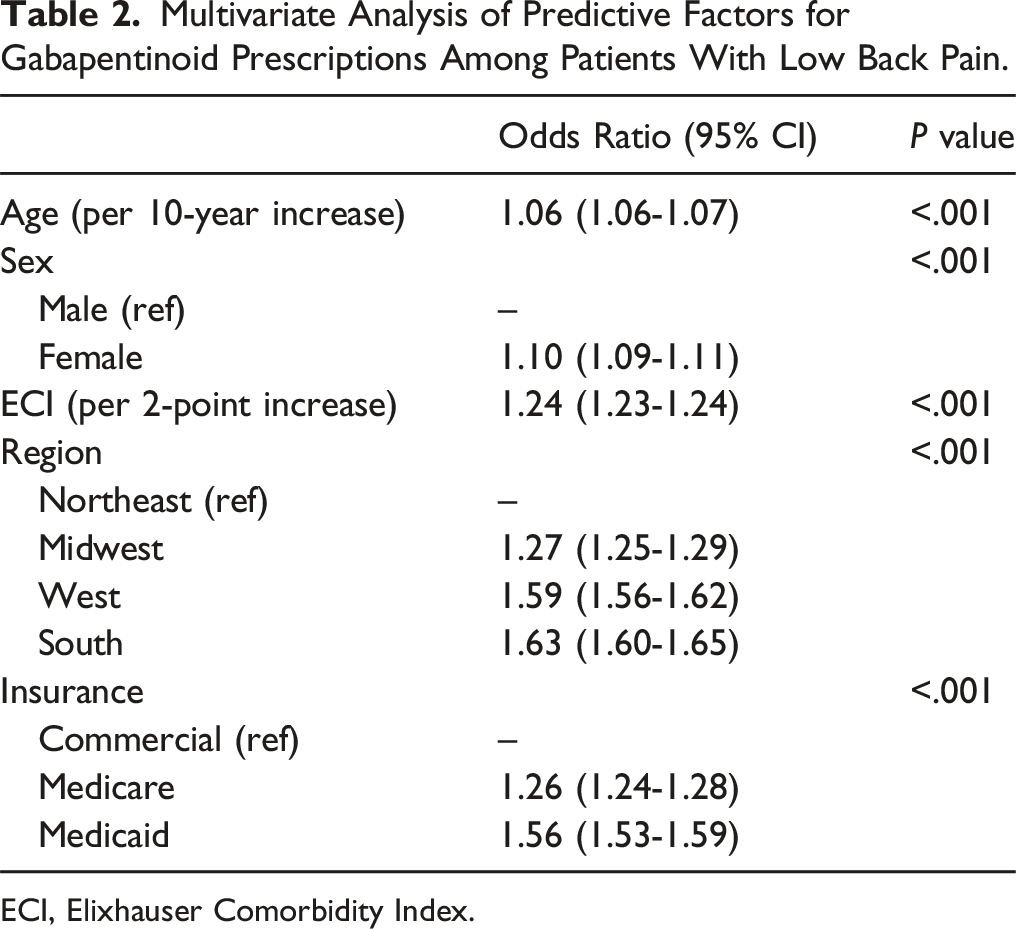
ECI, Elixhauser Comorbidity Index.
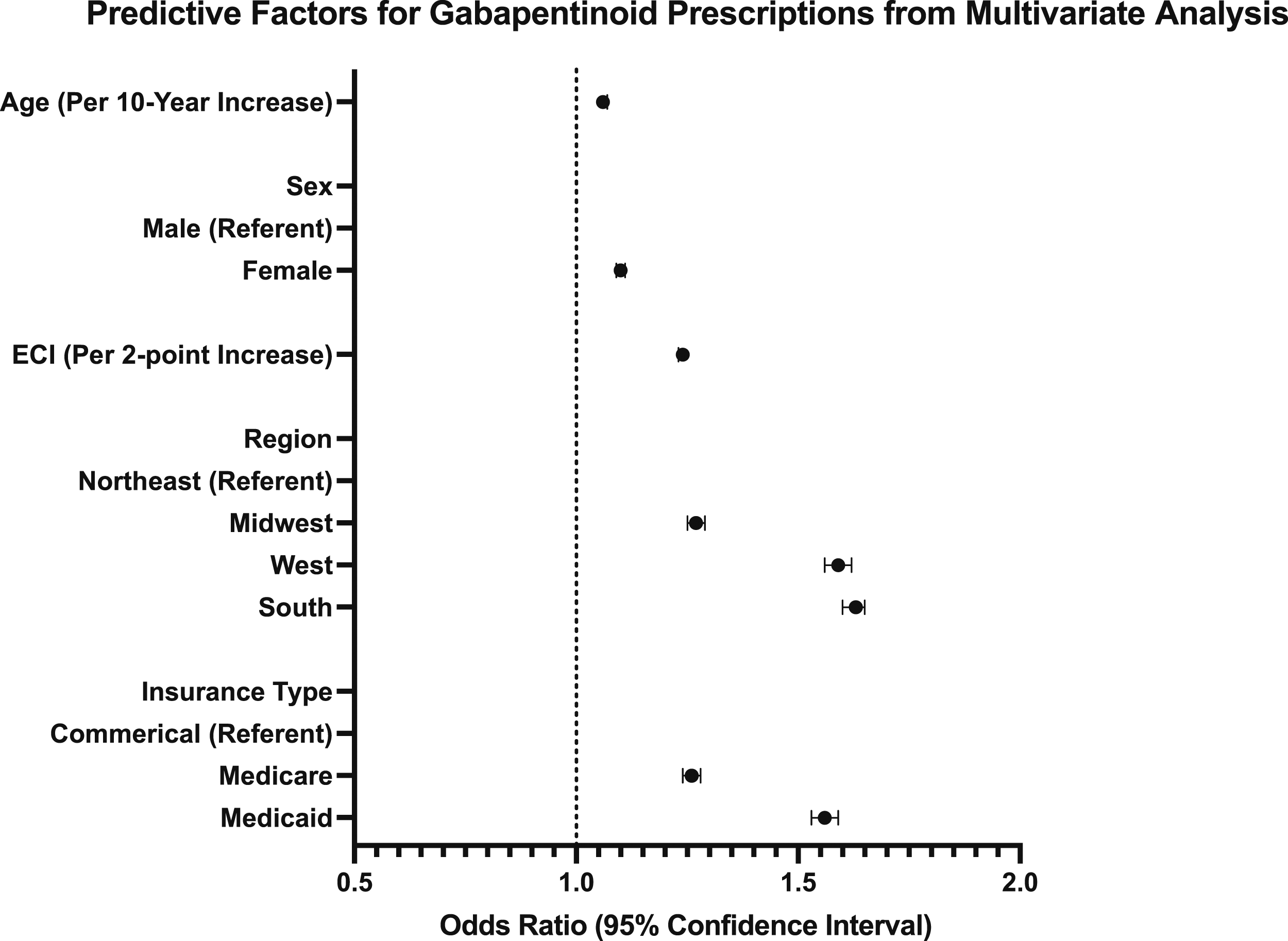
Forest plot depicting predictive factors for gabapentinoid prescriptions among patients with low back pain. Data points indicate mean and 95% confidence interval (CI). Controlled for age and Elixhauser Comorbidity Index (ECI).
Discussion
Low back pain (LBP) remains one of the leading causes of disability worldwide. 24 In wake of the ongoing opioid epidemic, reducing narcotic use is a high priority for patients, physicians, and systems.25-28 For some indications, non-narcotic analgesic alternatives exist – such as gabapentinoids – however, evidence does not support their use for axial LBP.20-22 Thus, the present study aimed to evaluate the incidence, provider specialty, and predictive factors for gabapentinoid prescriptions among patients diagnosed with isolated LBP in a large national health administrative database.
A large sample of over a million patients with isolated LBP was identified for the current study. Of these, 14% were prescribed gabapentinoids within a year of their diagnosis of LBP. This is high for an indication that is not supported by literature.20-22 For comparison, 11% of the study population was prescribed narcotics with or without gabapentinoids.
In terms of prescribing physicians, gabapentinoids were most frequently prescribed for the isolated LBP patients by primary care physicians (45% of all prescriptions). This may be due to practice patterns as well as who is most seeing this patient population with isolated back pain. While this was the first study to our knowledge examining the use of gabapentinoids for patients with isolated low back pain, specifically, these findings are in line with a previous study examining overall trends in gabapentinoid use in the United States from 2003 to 2016, which reported approximately 46% of gabapentinoid prescriptions being made by primary care physicians. 29
The current study went on to evaluate which patients were most likely to be prescribed gabapentinoids for isolated LBP. Female sex was identified as an independent predictor, potentially in line with previous literature suggesting women report higher low back pain severity and poorer response to treatment compared to men. 30 Geography in the US was also associated with being prescribed gabapentinoids, aligning with previous studies which report regional variations in gabapentinoid prescriptions, with providers in the South being most likely to prescribe. 31 Finally, patients with Medicare or Medicaid insured patients were more likely to receive a gabapentinoid prescription than those with Commercial insurance. The reason underlying such variations remain unclear; however, past studies have identified patient insurance plan as an independent predictor of prescriptions for pain management. 32
The current study does have limitations. For one – as with any work using administrative data – the accuracy of the findings is limited to that of the data coded. Gabapentinoid prescriptions would be thought to be accurately coded within the dataset. However, it would be difficult to quantify the duration of LBP symptoms based on insurance claims. Given this limitation, chronicity of symptoms could not be assessed as a predictor for gabapentinoid prescriptions. Lastly, although all patients included the present study were diagnosed with isolated LBP, components of neurologic symptoms could only be excluded by administrative coding.
While outside the purview of this exploratory analysis, future studies may investigate the influence of individual patient and provider preferences on gabapentinoid prescribing patterns. Areas of interest include further examining why gabapentinoids are being prescribed for LBP predominantly in primary care settings, and the role of gabapentinoids in conjunction with other pain management strategies, such as physiotherapy or injection therapy.
In sum, of nearly 1.2 million isolated LBP patients identified, 14.2% were prescribed gabapentinoids within one year of their LBP diagnosis, a number greater than narcotics and prescribed most commonly be primary care physicians. Several factors were identified as independent predictors of gabapentinoid prescription, include patient sex, region of residence, and insurance plan. While clinicians are being encouraged to shift away from the use of narcotics for isolated LBP, evidence does not well support gabapentinoids for this indication and its off-label use for this population may be questioned.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yale School of Medicine Fellowship for Medical Student Research.