
Abstract
Study Design:
Narrative review.
Objective:
To provide an overview on the diagnosis and surgical management of rheumatoid involvement of the lumbar spine. Rheumatoid arthritis (RA) is a chronic inflammatory disease of synovial joints, most commonly appendicular followed by axial. Although cervical spine involvement of RA is well documented, data on lumbar spine involvement and surgical management remains limited.
Methods:
Using PubMed, studies published prior to November 2018 with the keywords “RA, etiology”; “RA, spine management”; “RA, surgical management”; “RA, treatment”; “RA, DMARDs”; “RA, lumbar spine”; “RA, spine surgical outcomes”; “RA, imaging” were evaluated.
Results:
The narrative review addresses the epidemiology, manifestations, imaging, surgical complications, and operative and nonoperative management of RA involvement of the lumbar spine.
Conclusions:
Rheumatoid involvement of the lumbar spine can present with lower back pain, neurogenic claudication, radiculopathy, spinal deformity, and instability. Patients with RA have significantly higher rates of vertebral fractures and complications following surgical intervention. However, in the setting of instability and spinal deformity, thoughtful surgical planning in conjunction with optimal medical management is recommended.
Keywords
Introduction
Surgical Management of the Lumbar Spine in Rheumatoid Arthritis
Epidemiology
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disease primarily involving the synovial joints with a substantial global burden of disease. 1 In the United States, it was estimated that nearly 1.36 million individuals were living with RA in 2014, with a prevalence of 0.5% to 1% and a 3 to 1 ratio of females to males affected. 2,3 The axial skeleton is the third most common location of RA manifestation after hands and feet, with cervical spine involvement affecting 43% to 88% of patients with RA. 4 Although the involvement of this disease in the cervical spine has been well reported and studied, there are few reports of disease manifestation and best treatment practices for the lumbar spine. Lumbar lesions may have been overlooked in patients with RA, since prior to the routine use of biologic medications for RA, many patients sustained cervical spine instability and associated neurological deficits. 5 -9 One study found that 42% of patients with RA had both lumbar and cervical lesions. 4
Anatomy and Pathophysiology
RA is a complicated disease, with a wide range of opinions on the disease, its etiology, and its treatment. 10,11 The disease primarily affects the synovial compartment, with the clinical manifestation of joint swelling reflecting immune activation and synovial membrane inflammation. 11 The triggers for the inflammation are thought to be multifactorial, including environmental and genetic factors that eventually lead to abnormal cytokine release. 12 In the lumbar spine, the facet joints are reported to be the most commonly affected, with synovitis and degenerative changes leading to pain and instability. 13 Because facet joints are fibrocartilaginous synovial joints, facet erosions are thought to involve a similar mechanism as peripheral joints—synovitis with erosion of cartilage and subchondral bone. 14 Endplate erosions also occur with RA lumbar lesions (Figure 1). Although the discovertebral junction is not a synovial joint such as the peripheral or facet joints, histological analysis suggests that erosions of the endplate begin as an enthesopathy at the discovertebral junction. 15 The inflammatory degeneration of collagen at the junction between the disk and the endplates lead to loss of disk space and instability. 14 Other spinal involvements causing symptoms include erosive discitis, spinal stenosis, vertebral collapse, and extension of the inflammatory process from the apophyseal joints. 16 The combination of these changes can result in spinal deformity, including loss of lumbar lordosis and degenerative scoliosis in up to 28% of patients. 4,17,18
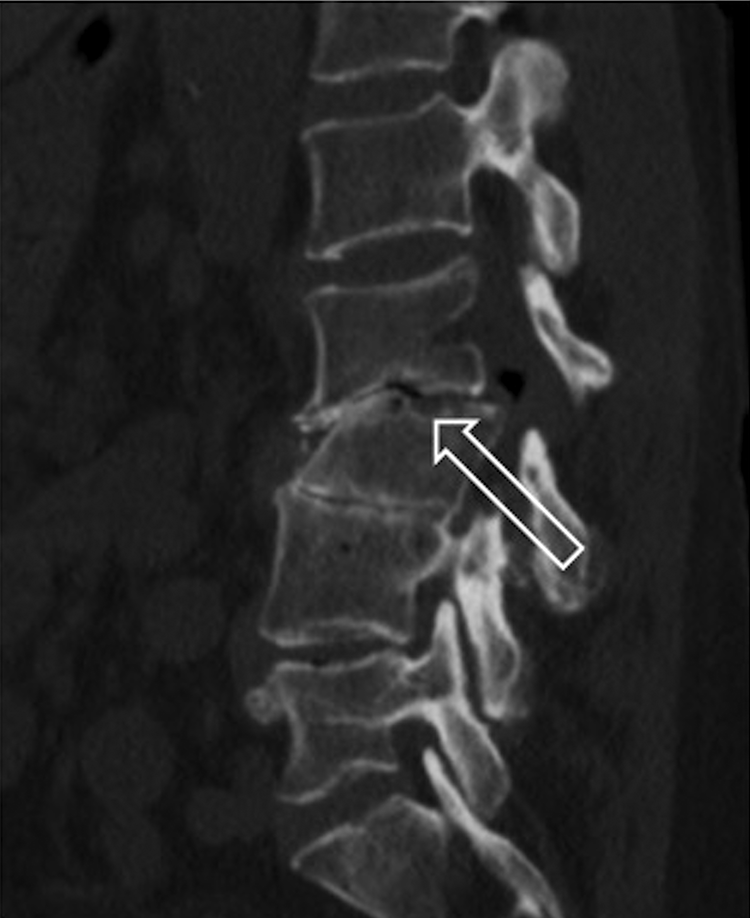
Sagittal computed tomography (CT) of the lumbar spine demonstrating L2-L3 endplate erosive changes (arrow).
Significance
RA has an economic impact on patients’ abilities to sustain employment since patients may experience remission and relapse of their symptoms. 19 Furthermore, patients with RA have higher frequencies of vertebral fractures and higher complication rates following surgical interventions compared to patients without RA undergoing similar interventions. 20,21 The management of RA affecting the cervical spine is well described, but there are limited studies discussing the management of rheumatoid involvement of the lumbar spine.
Manifestations
General
The clinical manifestations of RA are heterogeneous, and the extent of joint involvement and disease progression has been characterized into least erosive disease (LED), more erosive disease (MED), and mutilating disease (MUD), with the latter 2 representing axial joint involvement as well as peripheral joint involvement. 22
Lower back pain occurs in approximately 25% to 40% of patients with RA. 4,23 However, Yamada et al 23 found no association between lower back pain in patients with RA and radiographic findings. Symptoms possibly related to lumbar lesions and concurrent lumbar stenosis include neurogenic claudication and paresthesias. 4 Case reports and series have also identified incidences of patients reporting lower extremity weakness from pathologic fractures, vertebral subluxations caused by mutilating RA, and foraminal stenosis. 24,25 Extra-articular manifestations can be seen with RA as well. There have been case reports of extradural and intradural rheumatoid nodules causing thoracolumbar stenosis and radiculopathy. 26 -28 There have also been case reports of spinal neuroarthropathy secondary to RA, caused by loss of innervation to the spine from cytokine release leading to degenerations in disks, end plates, and facet joints resulting in dislocations. 29
Osteoporosis and Fracture Risk
There is a higher incidence of osteoporosis and low bone mineral density in RA patients compared with controls. 30 Inflammation related to RA and other inflammatory diseases such as ankylosing spondylitis has been presumed to contribute to lower bone mineral densities and increased risk of vertebral fractures. 31,32 However, the association between the use of corticosteroids in RA and increased risk of vertebral fractures remains controversial. Meng et al 30 found a positive correlation between oral glucocorticoid use and risk of major osteoporotic fractures (r = 0.701 and P = .006), consistent with the findings of Arai et al 33 findings of 33% prevalence of vertebral fracture in patients with RA taking glucocorticoids compared with 11% prevalence of vertebral fracture in patients with RA not taking glucocorticoids. In contrast, in a case-control study with 101 patients with RA and 303 controls, Ghazi et al 34 reported an inverse relationship between glucocorticoid use and prevalence of vertebral fractures, consistent with the report of Ørstavik et al 35 report of 255 patients with RA that found no association between corticosteroid use and incident vertebral deformities. However, it is the senior author’s practice to order a DEXA (dual-energy x-ray absorptiometry) scan prior to any spinal fusion. If osteopenia or osteoporosis is identified, the patient is referred appropriately for initiation of antiresorptive medications or anabolic medications such as teriparatide (Eli Lilly, Indianapolis, IN).
Imaging
Radiography (X-Ray)
The radiographic hallmarks of RA in the thoracolumbar spine include erosion and fusion of apophyseal and facet joints along with erosions of spinous processes. 36,37 General radiological lumbar lesions were not more prevalent among RA patients compared with population controls, though vertebral fractures were more frequent in RA patients. 38 Disc space narrowing and severity of endplate erosion were correlated with higher RA severity scores (Larsen grades). 4,38 Larsen grade of the wrist was also found to be higher in patients with lumbar facet erosion, compared to patients without these lesions. 4 This is likely because facet joints are synovial joints consisting of fibrocartilage that are very similar to peripheral joints and as such undergo similar inflammatory reactions resulting from RA. 39
Abnormal radiologic findings in the lumbar spine have been reported in 57% of patients with RA. In particular, the most frequent radiographic findings (Figure 2) are disc space narrowing (37%), scoliosis (28%), spondylolisthesis/retrolisthesis (23%), endplate erosion (20%), facet erosion (20%), and osteophyte formation (5%). 4 In another study, 21% of RA patients had vertebral fractures, and the vertebral fractures increased to 33% in patients treated with corticosteroids. 33 These findings are generally consistent with other existing literature. 40,41 In assessing for evidence of spondylolisthesis in patients with RA, Sugimura et al 42 found 36.7% of patients with RA had radiographic evidence of lumbar spondylolisthesis, with significant associations with higher serum CRP levels and history of joint surgery.
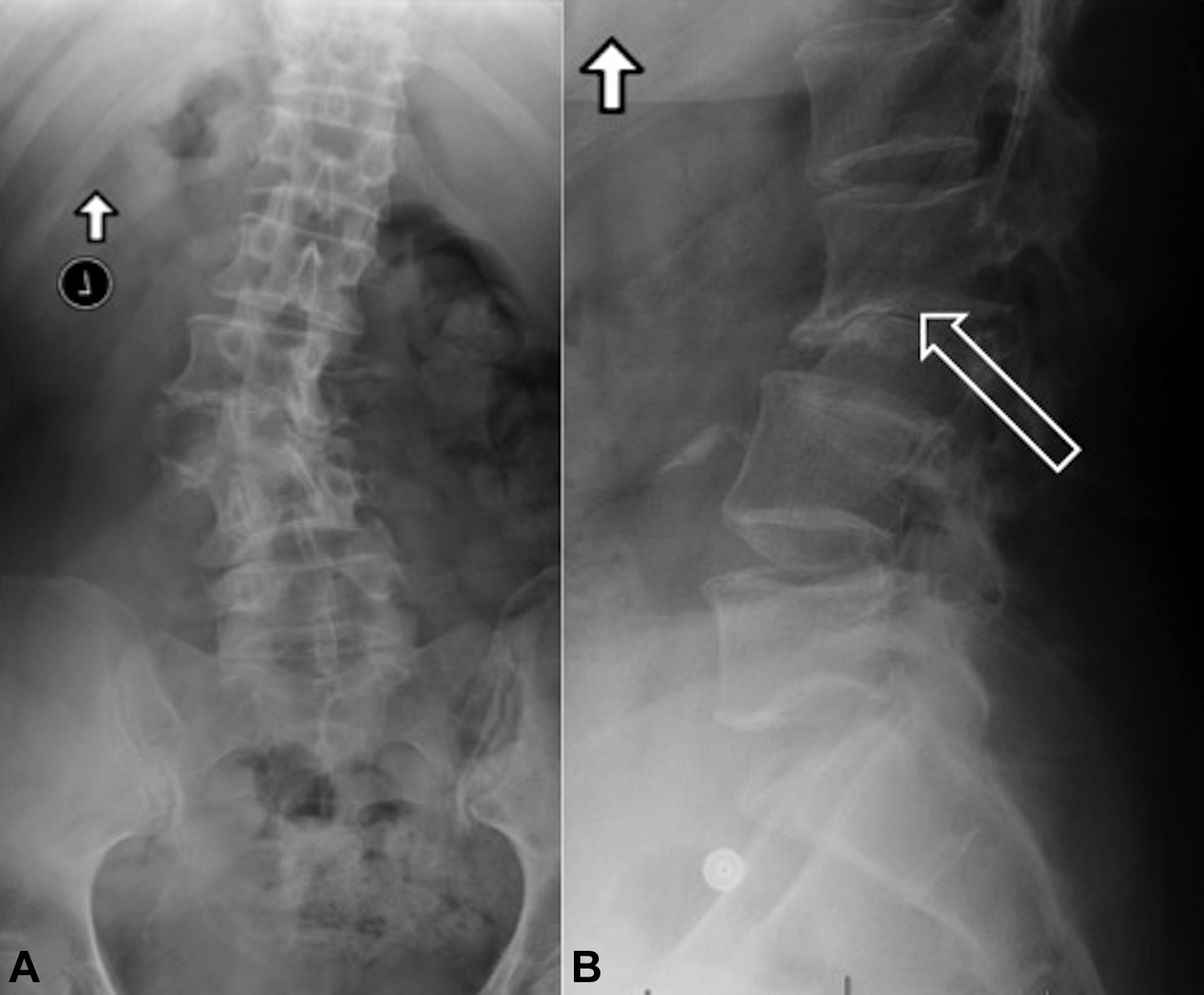
(A) Anteroposterior Lumbar radiograph demonstrating scoliosis with an apex at L2-L3. (B) Lateral radiograph demonstrating focal kyphosis and erosive endplate changes at L2-L3.
Of note, Lee et al 43 described significant relationships between certain sagittal parameters and clinical outcomes in patients with RA. The study included 120 RA patients and 60 controls, and found that the C7/sacrofemoral distance ratio (C7/SFD) significantly predicted the visual analogue scale (VAS) for back pain (P = .005), and the spinosacral angle (SSA) significantly predicted the Korean Oswestry Disability Index (KODI) and Scoliosis Research Society scores (P = .038 and P = .044, respectively) in RA patients. 43 The authors also reported that the mean C7/SFD ratio was more positive and the SSA lower in RA patients than in matched controls, speculating that spinal misalignment and pelvic abnormalities are closely related in RA.
Magnetic Resonance Imaging (MRI)
MRI is increasingly being used for RA research and in clinical practice because of its capability in detecting early inflammatory changes in bones and joints without exposing patients to ionizing radiation. This ability to identify the key pathological features of RA much earlier than would be seen on radiography is advantageous in earlier treatment of the disease, especially with the advent of newer biologic agents that may benefit patients if started early. 44 MRI has the added benefit of detecting bone marrow edema, thought to be a precursor to the development of erosions in RA as well as a marker of inflammation. In particular with the MRI, clinicians are able to assess for facet effusions and synovitis.
MRI offers the most comprehensive evaluation of RA in the spine (Figure 3). It is typically performed to assess for the presence of stenosis and neural element compression associated with deformity. 45 A study of 201 patients with RA used MRI and found lumbar endplate erosions in 70.6% and lumbar facet erosions in 76.6% of patients. 14 The severity of erosions was found to be highest in patients with radiographic evidence of lumbar lesions. Although future studies investigating the specificities of MRI findings to RA and the sequences for best identifying specific lesions are warranted, MRI remains advantageous in evaluating for inflammation in and around the spine, as well as for surgical planning.

Sagittal T2-weighted magnetic resonance imaging (MRI) of the lumbar spine demonstrating erosive changes at L2-L3 and L3-L4.
Computed Tomography Scan (CT Scan)
In the setting of spinal deformity associated with RA, CT scan and 3-dimensional modeling can assist in visualizing the deformity. CT scan is also useful for surgical planning, especially for multilevel constructs.
Treatments
Surgical treatment of lumbar lesions affected by RA are generally tailored to each patient, taking into account location of the lesion as well as the patient’s symptoms. Indications for lumbar spine surgery include radiculopathy and neurogenic claudication with exhaustion of non-operative treatment modalities, as well as pain associated with spinal deformity. It has been shown that surgical management of rheumatoid arthritis leads to better results compared to non-operative treatments. 46 However, the data on surgical management of the lumbar spine is mostly limited to case reports and series.
Lumbar Fusion and Laminectomy:
Posterior lumbar interbody fusion with spinal instrumentation is often used in conjunction with decompression in the setting of instability and rheumatoid spondylitis. 47 Crawford et al 48 reported on 19 patients with RA who had symptomatic lumbar stenosis requiring posterolateral lumbar fusion, along with a matched control group of non-RA patients. Using a clinical outcome scale by Herkowitz and Kurtz, 49 the outcomes were similar between the RA and non-RA groups, with 74% of patients achieving good to excellent results in the RA group and 63% in the non-RA group. In another case-control study with 40 patients with RA and 134 without RA undergoing posterior lumbar fusion for spinal stenosis, symptoms were reduced significantly one year after the surgery in both groups (P = .001), measured by the VAS and KODI. However the RA group’s clinical scores deteriorated in the second year, with the clinical scores being significantly higher than those of the non-RA group (VAS back pain, P = .001; VAS leg pain, P = .024; KODI score, P < .001). 50 Successful treatment of cauda equina symptoms with decompression and fusion have also been described in case reports. 16,51 In another series, decompression and posterior lumbar interbody fusion was successful in treating back and leg pain, with improved gait and activities of daily living. However, high rates of complications were reported, including collapse of adjacent vertebra (57%), instability of adjacent levels (43%), migration of pedicle screws (29%), collapse of bone graft (14%), and infection (14%). 47
Laminectomy/Laminotomy Without Fusion
Recent reports suggest that decompression without fusion may be associated with decreased rates of complications. Seki et al 52 looked at outcomes of 52 patients with RA who underwent surgery for lumbar spinal disorders over a mean of 5.1 years, with 27 who underwent decompression with fusion and 25 who underwent decompression without fusion. The rate of revision and adjacent segment disease was significantly greater in the fusion group. 52 Newer strategies such as laminotomy without fusion, a technique using smaller incisions and sparing the supra- and interspinous ligaments, have also been described. In a large observational study of 1433 patients, RA patients with lumbar spinal stenosis experienced significant and similar improvements in patient-reported outcomes after laminotomy or laminectomy without fusion compared to those without RA (P < .001). Complication rates were found to be similar in both groups at the 1-year follow up. 53
Spinal Deformity (Figure 4)
Although studies on lumbar spinal deformities in patients with RA are limited, lumbar scoliosis has been reported to have a prevalence of 28% to 32% in patients with RA. 4,54 Furthermore, complication rates have been reported to be higher in patients with RA undergoing long spinal fusion for deformity correction than in patients without RA. A recent outcomes study on long spinal fusion for scoliosis in 28 matched patients with and without RA found that patients with scoliosis and RA had significantly more major complications (deep wound infections, epidural hematomas, instrumentation failure, pseudoarthrosis, respiratory complications, death, etc) and secondary procedures than those with scoliosis alone (23 vs 11; P < .001, and 14 vs 6; P < .001, respectively). 17 The authors concluded that factors related to the higher rates of complication in surgical management of scoliosis in patients with RA may be due to the combination of poor bone quality and a weakened immune system due to RA therapy. Ohishi et al 55 reported that in their study of 26 RA patients with lumbar scoliosis, the initial Cobb angles were inversely related to the progression of scoliosis, contrary to what has been reported for degenerative scoliosis. This finding suggests that the progression and underlying characteristics of spinal deformities related to RA may involve different processes such as disease effects on bone and therapy-related adverse effects reported by other studies, as compared to degenerative scoliosis not associated with RA. 17,54,55
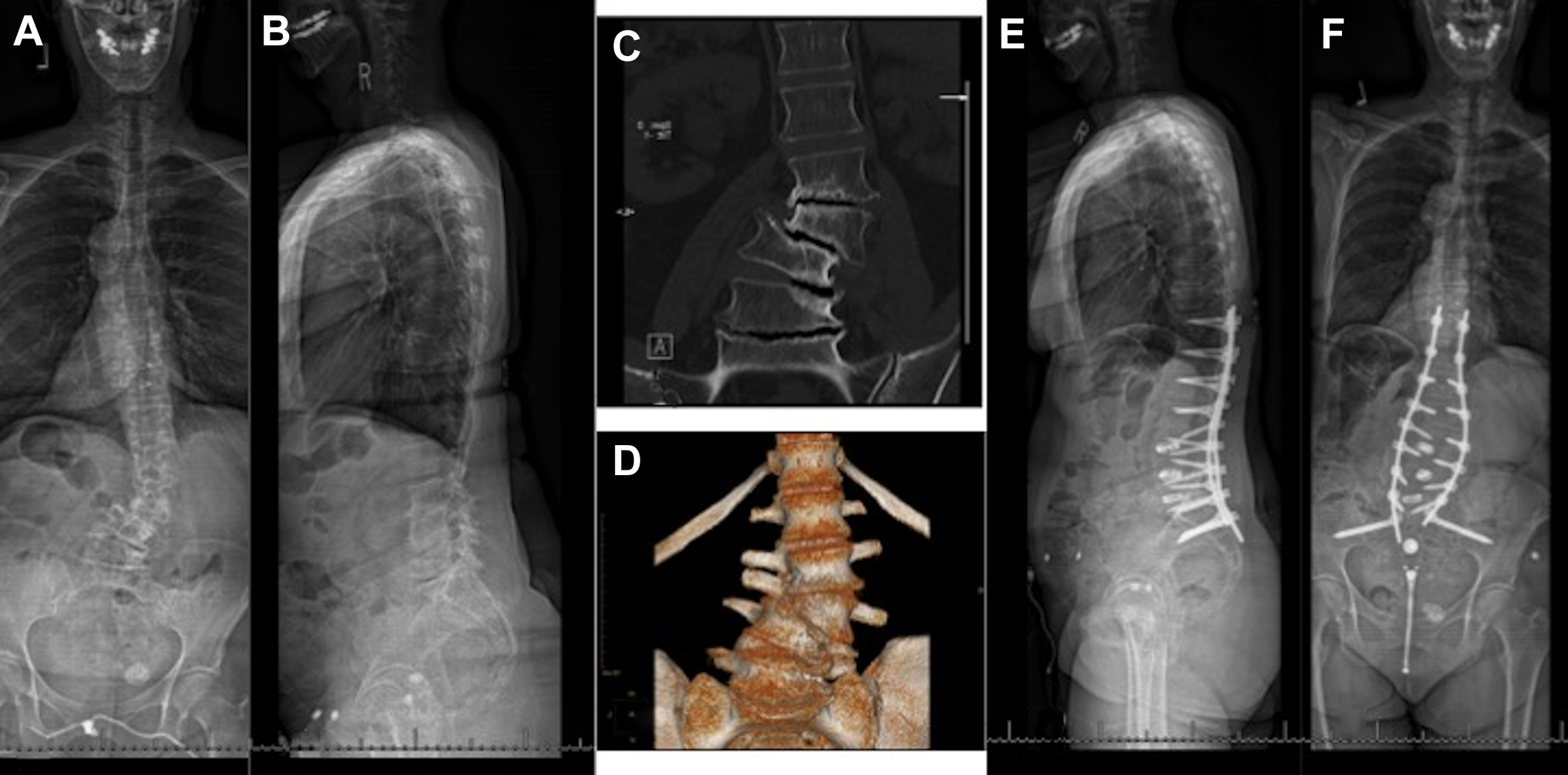
A 67-year-old woman with rheumatoid arthritis (RA) presents with back pain and radicular symptoms. (A, B) Anteroposterior and lateral scoliosis radiograph demonstrates a lumbar scoliosis with an apex at L3-L4 and loss of lumbar lordosis. (C, D) Coronal computed tomography and 3-dimensional reconstruction demonstrates the multilevel endplate erosions and degenerative disc disease. (E, F) The patient was treated with a T11-pelvis instrumentation, L3-L4, L4-L5, L5-S1 interbody fusion. At 18 months postoperative, she is doing well with improved radicular symptoms but with some axial symptoms.
Disease-Modifying Antirheumatic Drugs (DMARDs)
Recent advances in pharmacologic management of rheumatoid arthritis has reduced the number of patients who reach end-stage joint destruction. 56 DMARDs used to manage RA include methotrexate, leflunomide, azathioprine, hydroxychloroquine, and biologic modifiers such as tumor necrosis factor inhibitors and interleukin-1 inhibitors. These are immunosuppressive medications, and are generally stopped one half-life prior to surgery to reduce the risk of infection, and restarted once healing has occurred, around 2 weeks after surgery. 57 In deciding whether to hold medications or not, the risk of infection and delayed healing must outweigh the risk of disease flare-ups hindering rehabilitation.
Saleh et al 58 in their review of pre- and perioperative management of RA, reports that methotrexate continuation prior to surgery showed no short- or long-term increases in infection risk or complications. However, it is cautioned that methotrexate should be held 1 week preoperatively and at least 1 to 2 weeks postoperatively in elderly patients or in those with comorbidities that affect drug metabolism. 58
For patients on leflunomide monotherapy, there have been reports of substantially increased risk of surgical wound infections. 59 Therefore it is recommended to discontinue leflunomide 1 to 2 days prior to the procedure, and begin cholestyramine to rapidly reduce blood levels of active metabolites. 58,60 Leflunomide may be restarted 1 to 2 weeks postoperatively after the wound has healed, and antibiotics have been discontinued.
With the introduction of tumor necrosis factor–α (TNF-α) inhibitors, such as infliximab, etanercept, and adalimumab, more severe forms of RA have been better managed, and reduced the number of patients progressing to end-stage joint destruction. 58 Although there have been conflicting reports regarding increase in surgical infection risk with TNF-α inhibitors, a recent retrospective review of 50 359 patients found that patients who took a TNF-α inhibitor within one administration interval prior to surgery (with or without other DMARDs) had a 10-fold increase in the rate of infection. 61 -63 Giles et al 62 found that patients with RA who developed serious postoperative infections were more likely to be treated with a TNF-α inhibitor than the noninfected group (P = .041). In their analysis, prescription of TNF-α inhibitor therapy was also significantly associated with the development of a serious postoperative infection (odds ratio 4.4, 95% confidence interval 1.10-18.41), even after controlling for age, sex, disease duration, prednisone use, and other factors. Although currently there are no guidelines for perioperative management of DMARDs for spine surgery, the 2017 American College of Rheumatology/American Association of Hip and Knee Surgeons guideline for elective total hip or total knee arthroplasty state that TNF-α inhibitors should be discontinued at least 1 dosing cycle prior to surgery. 64 Although there is lack of evidence regarding the optimal time to restart biologic medications, it is also recommended that they be restarted after evidence of wound healing, typically 14 days, and without clinical evidence of nonsurgical site infections. 58,64
The senior author’s practice is to discuss with the patient’s rheumatologist and to hold DMARDs at a minimum of 2 weeks pre- and postoperative.
Complications
Compared to patients without RA, patients with RA who undergo surgical management have worse subjective scoring outcomes and increased rates of complications. 21,48 Common complications include wound infections, pseudoarthrosis, nonunion, implant complications, and adjacent level degeneration. A recent outcomes study of posterolateral lumbar fusion showed that compared to patients without RA, those with RA had almost a 3-fold increase in complications such as radiographic evidence of nonunion (P = .001), implant failure (P = .032), symptomatic adjacent segment disease (P = .001), and infection (P = .031). 50 Overall complication rates of patients with RA who underwent lumbar fusion ranged from 37% to 47.5%, with 37.5% requiring revision. 48,50 A limitation of these studies is a small sample size. In a recent nationwide analysis of 52 818 patients undergoing noncervical spinal fusions, no difference in mortality rate (P = .99) was found between patients with RA and patients without RA. However, those with RA were found to have significantly higher rates of infections (P = .032), implant-related complications (P = .01), incidental durotomies (P = .001), and urinary tract infections (P = .001). 18
Adjacent Segment Disease (ASD)
ASD is a known complication of fusion surgery in RA patients, with an incidence of up to 60% and significantly higher than those who undergo lumbar decompression alone. 52 Of note, Kang et al 50 found that among the patients with complications after posterolateral lumbar fusion (47.5% in the RA group and 17.1% in the non-RA group, P < .001), those with RA had a significantly higher incidence of ASD (P = .001). Rates of revision surgery have also been shown to be increased in RA patients undergoing lumbar decompression with fusion (37%) compared to decompression without fusion (4%) in a study of 52 patients (P = .004), with 73% of these revisions found to be indicated due to symptomatic ASD (P = .03). 52 One recent study showed that compared to patients without RA, RA was associated with a 4.5 times increased risk of post–fusion-related ASD requiring subsequent surgery, and that 3-segment fusion was associated with a 2.7 times higher risk of ASD requiring surgery than 1- or 2-segment fusion. 65 In patients with extensive spinal deformity in the setting of RA that require long spinal fusion, the decision to extend the fusion to the sacrum or only to L5 used to be controversial. 66 In the senior author’s practice, if 3 or more levels require fusion and the patient has low bone mineral density (osteopenia or osteoporosis), the fusion is extended to the sacrum and instrumentation placed in the ilium.
Conclusion
Rheumatoid involvement of the lumbar spine appears to be more common than previously described. Symptoms resulting from lumbar lesions are not negligible and can be substantial in some patients with RA. In all patients with RA, lumbar lesions should be examined in addition to the cervical spine and peripheral joints. With regard to treatment, patients with RA require special consideration when undergoing surgery due to generally increased rates of complications, with some exceptions (laminotomy or laminectomy alone). The rates of revision surgery, adjacent segment disease, and other complications have been shown to be higher in those who underwent decompressive surgery with fusion compared with those who underwent decompressive surgery without fusion. However, in the setting of instability and spinal deformity, a fusion may be needed and thoughtful surgical planning is recommended.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.