
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Racial disparities in postoperative outcomes are unfortunately common. We present data assessing race as an independent risk factor for postoperative complications after spine surgery for Native American (NA) and African American (AA) patients compared with Caucasians (CA).
Methods:
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database was queried for spine procedures performed in 2015. Data was subdivided by surgery, demography, comorbidity, and 30-day postoperative outcomes, which were then compared by race. Regression was performed holding race as an independent risk factor.
Results:
A total of 4803 patients (4106 CA, 522 AA, 175 NA) were included in this analysis. AA patients experienced longer length of stay (LOS) and operative times (P < .001) excluding lumbar fusion, which was significantly shorter (P = .035). AA patients demonstrated higher comorbidity burden, specifically for diabetes and hypertension (P < .005), while NA individuals were higher tobacco consumers (P < .001). AA race was an independent risk factor associated with longer LOS across all cervical surgeries (β = 1.54, P <.001), lumbar fusion (β = 0.77, P = .009), and decompression laminectomy (β = 1.23, P < .001), longer operative time in cervical fusion (β = 12.21, P = .032), lumbar fusion (β = -24.00, P = .016), and decompression laminectomy (OR = 20.95, P < .001), greater risk for deep vein thrombosis in lumbar fusion (OR = 3.72, P = .017), and increased superficial surgical site infections (OR = 5.22, P = .001) and pulmonary embolism (OR = 5.76, P = .048) in decompression laminectomy. NA race was an independent risk factor for superficial surgical site infections following cervical fusion (OR = 14.58, P = .044) and decompression laminectomy (OR = 4.80, P = .021).
Conclusion:
AA and NA spine surgery patients exhibit disproportionate comorbidity burden and greater 30-day complications compared with CA patients. AA and NA race were found to independently affect rates of complications, LOS, and operation time.
Introduction
Despite continued efforts to deliver quality health care throughout the United States, race remains a prevalent and independent risk factor affecting clinical outcomes across all fields of medicine. 1 Inequality in this manner violates the core tenants of Western medicine, the practitioners of which undertake the chief responsibility to deliver excellent and compassionate care to patients irrespective of circumstances such as racial or ethnic makeup. Still, these disparate outcomes persist, including in the fields of orthopedic and spinal surgery. 2 -4
Differential outcomes in spinal cases consistently demonstrate unfavorable trends in length of hospitalization as well as 30-day readmission when analyzed by race, conferring an increased clinical as well as financial burden among often socioeconomically disadvantaged populations. 5,6 These costs are not limited to the patients themselves, extending further to families and communities while creating ripple effects felt within the hospital itself. It is necessary, therefore, to continue our assessment of ever more recent data in order to determine how racial disparities in surgical outcomes are evolving so as to increase awareness among practitioners while continuing to update strategies used for combating inequality in the face of increasing need of surgical care. 7
The literature clearly establishes well-identified disparities between African American (AA) and Caucasian (CA) patients, with the former finding significantly poorer clinical outcomes. However, other racial and ethnic groups are often studied together as a combined cohort, rarely reporting on the burden encountered specifically as it relates to these racial populations. 5,8 -14 Little to no data is currently available regarding Native American (NA) recipients of spinal surgery or among the field of orthopedic surgical research at large. 15 This is of special concern considering the increased incidences of multiple health conditions including obesity, diabetes, physical disability, and substance abuse observed in NA communities often within the context of staggeringly low access to health care. 16 -19
Thorough analysis of the 2015 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) for all spinal procedures identified NA as the third largest subpopulation receiving spinal surgeries, necessitating a more complete analysis of differential delivery of care among American spine patients. Previous national studies of racial disparity have examined outcomes either by assessing individual surgeries or querying specific diagnosis. 6 -8,12,14,20 -26 By comparison, we present racial disparities observed between 3 different races (CA, AA, NA) while also considering 3 common spine surgical procedures: cervical fusion (CF), lumbar fusion (LF), and laminectomy (LN). In so doing, we present a comprehensive epidemiological picture of the current state differential delivery of care within the field of spine surgery.
Methods
Data Source
This investigation utilized data from the 2015 ACS-NSQIP database. The ACS-NSQIP is a national prospective database collecting voluntarily reported patient data from 603 sites across the United States. Among this data the ACS-NSQIP collects over 150 verified variables including patient demographics, comorbidities, preoperative risk factors, intraoperative variables, and 30-day postoperative mortality and morbidity outcomes for patients undergoing major surgical procedures in both the inpatient and outpatient settings.
Inclusion and Exclusion Criteria
The 2015 edition of the ACS-NSQIP database included 885 502 spinal surgery cases. Patient inclusion criteria consisted of undergoing either a cervical procedure, lumbar vertebral body fusion, or decompression laminectomy as outlined in Surgical Procedure Categorization. Additionally, patients who were either CA, AA, or NA race were included in this study. A total of 4803 unique patients satisfied these criteria for analysis.
Surgical Procedure Categorization
Current Procedural Terminology (CPT) codes were utilized to define 3 categories based on selected representative surgical procedures common in the field of spinal surgery.
Cervical fusion was defined by the following CPT codes: 22 551, anterior or anterolateral approach technique arthrodesis procedures on the spine (vertebral column); 22 552, anterior or anterolateral approach technique arthrodesis procedures on the spine (vertebral column); 22 585, anterior cervical discectomy with interbody fusion (ACDF) arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); 22 554, anterior cervical interbody fusion arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression.
Lumbar fusion was defined by the following CPT codes: 22 630, arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace, lumbar; 22 633, arthrodesis, combined posterior or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment, lumbar; 22 558, anterior interbody lumbar fusion (ALIF) or lateral lumbar interbody fusion (XLIF) arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); 22 612, arthrodesis, posterior, or posterolateral technique, single level; 22 614, posterior lumbar fusion arthrodesis, posterior or posterolateral technique, single level.
Decompression laminectomy was defined by the following CPT codes: 63 005, laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy, 1 or 2 vertebral segments, lumbar, except for spondylolisthesis; 63 035, laminotomy (hemilaminectomy), with decompression of nerve roots(s), including partial facetectomy, foraminotomy, and/or excision of herniated disc each additional interspace; 63 017, laminectomy with exploration and/or decompression, greater than 2 vertebral segments, lumbar; 63 047, laminectomy, facetectomy, and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina, and/or nerve root(s)), single vertebral segment, lumbar; 63 030, laminotomy (hemilaminectomy), with decompression of nerve roots(s), including partial facetectomy, foraminotomy, and/or excision of herniated disc, one interspace, lumbar; 63 042, laminotomy (hemilaminectomy), with decompression of nerve roots(s), including partial facetectomy, foraminotomy, and/or excision of herniated disc, reexploration, single interspace; 63 044, laminotomy (hemilaminectomy), with decompression of nerve roots(s), including partial facetectomy, foraminotomy, and/or excision of herniated disc, reexploration, each additional lumbar interspace; 63 048, laminectomy, facetectomy, and foraminotomy (unilateral or bilateral) with decompression of spinal cord, cauda equina, and/or nerve root(s), each additional segment cervical, thoracic, or lumbar.
Race Subcategorization
Patients were further subdivided into 1 of 3 primary categories as determined by race. The categories were Caucasian (White), African American (Black or African American), and Native American (American Indian or Alaska Native). Other races were excluded due to insufficient reporting in the 2015 ACS-NSQIP.
Data of Interest
Data of interest included patient demography (age, body mass index [BMI], mortality probability, morbidity probability), comorbidities (diabetes, smoking status, dyspnea, chronic obstructive pulmonary disease, congestive heart failure, ascites, hypertension, renal failure, inpatient status, ventilator use), perioperative course (operative time, postoperative length of stay, total length of stay), surgical complications (superficial surgical site infections, organ space surgical site infections, dehiscence, pneumonia, reintubation, pulmonary embolism, renal insufficiency, urinary tract infection, cerebral vascular accident, cardiac arrest, deep vein thrombosis), and postoperative course (return to operating room, 30-day readmission).
Statistical Analysis
Patients subgroups were compared with regard to race and surgical procedure as outlined above. Chi-square tests were used to assess differences in comorbidity rates between race groups for statistical significance, while ANOVA tests were used for patient age, BMI, mortality probability, and morbidity probability.
Multiple regression analysis was performed to compare AA and NA patients with CA patients controlling for age, BMI, and American Society of Anesthesiologists score. This was done in order to determine whether patient race was an independent risk factor for 30-day postoperative outcomes, perioperative course outcomes, and postoperative course outcomes.
Results
Of the 4803 patients in the 2015 ACS-NSQIP database that satisfied our criteria, 4106 (85.5%) were Caucasian, 522 (10.9%) African American, and 175 (3.6%) Native American (Table 1).
Descriptive Statistical Summary of Spine Surgeries Presented in 2015 ACS-NSQIP.a
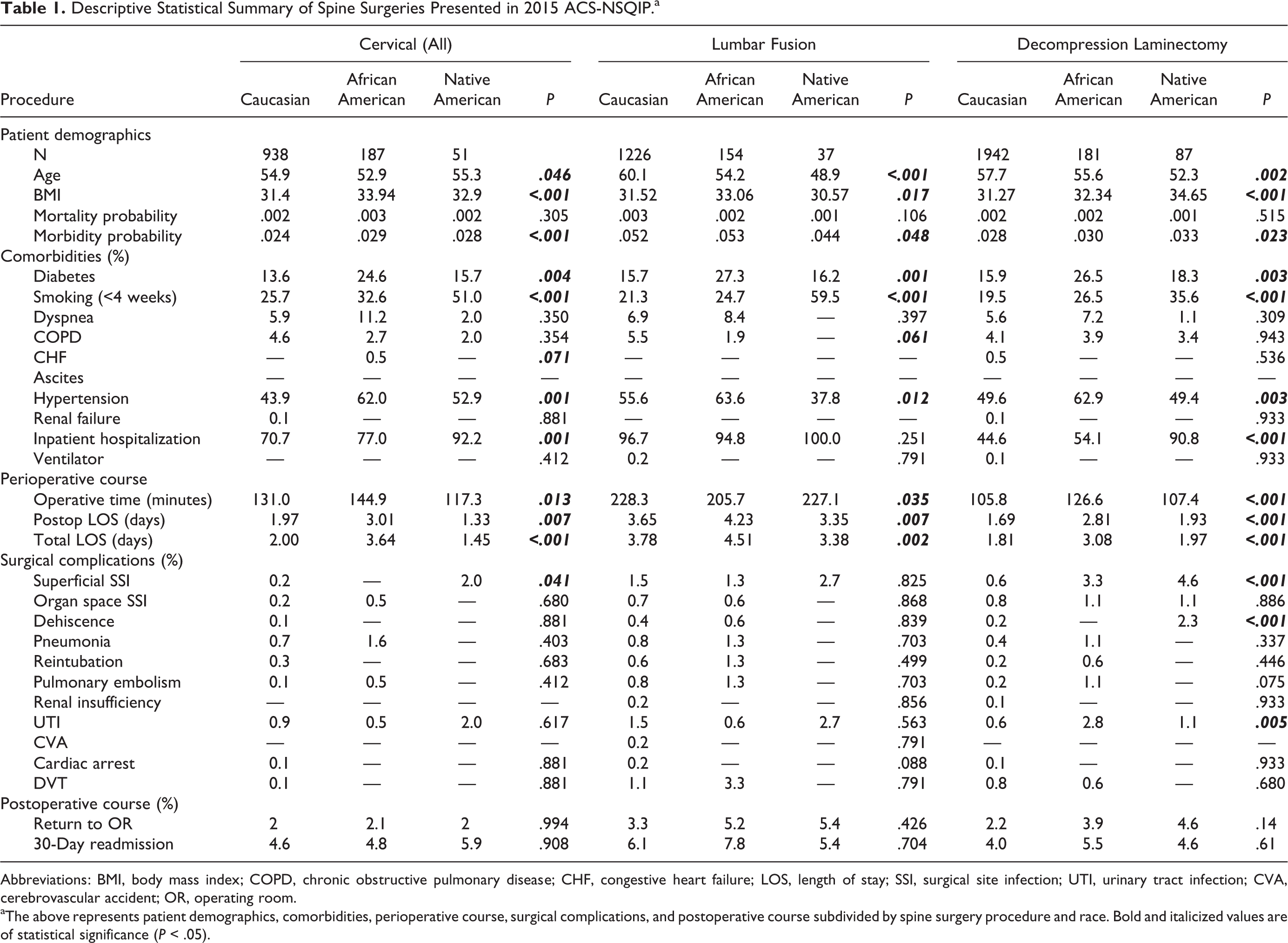
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; LOS, length of stay; SSI, surgical site infection; UTI, urinary tract infection; CVA, cerebrovascular accident; OR, operating room.
aThe above represents patient demographics, comorbidities, perioperative course, surgical complications, and postoperative course subdivided by spine surgery procedure and race. Bold and italicized values are of statistical significance (P < .05).
Cervical Procedures
All cervical fusion procedures totaled 1176, including 938 CA, 187 AA, and 51 NA patients with significant differences among mean age (54.9 ± 11.1, CA; 52.9 ± 10.6, AA; 55.3 ± 11.3, NA; P = .046), mean BMI (31.4 ± 6.83, CA; 33.9 ± 7.39, AA; 32.9 ± 6.40, NA; P < .001), and mean morbidity probability (mean: .024 ± .012, CA; .029 ± .016, AA; .028 ± .009, NA; P < .001). AA and NA patients had higher comorbidity burdens including significantly higher rates of diabetes (13.6% CA; 24.6% AA; 15.7% NA; P = .004) and hypertension (43.9% CA; 62.0% AA; 52.9% NA; P = .001) for AA patients and increased rates of smoking (25.7% CA; 32.6% AA; 51.0% NA; P < .001) and need for inpatient hospital stay (70.7% CA; 77.0% AA; 92.2% NA; P = .001) among NA. AA had on average a day and a half longer length of hospital stay (2.00 days, CA; 3.64 days, AA; 1.45 days, NA; P < .001), whereas NA patients had significantly shorter operative times (131.0 minutes, CA; 144.9 minutes, AA; 117.3 minutes, NA; P = .013). AA race was an independent risk factor for longer operation (β = 12.212, 95% CI = 1.058 to 23.366, P = .032) and length of average hospital stay (β = 1.541, 95% CI = 0.731 to 2.081, P < .001), where NA patients experienced clinically significant albeit statistically insignificant differences in shorter operative times (β = −18.033, 95% CI = −37.941 to 1.875, P = .076) and shorter length of average hospital stay (β = −1.028, 95% CI = −2.473 to 0.418, P = .163). NA race was found to be an independent risk factor for superficial surgical site infections (SSIs) in the 30-day postoperative period (OR = 14.577, 95% CI = 1.072 to 198.192, P = .044) (Table 2).
Associations Between Race and Surgical Spine Procedure.a
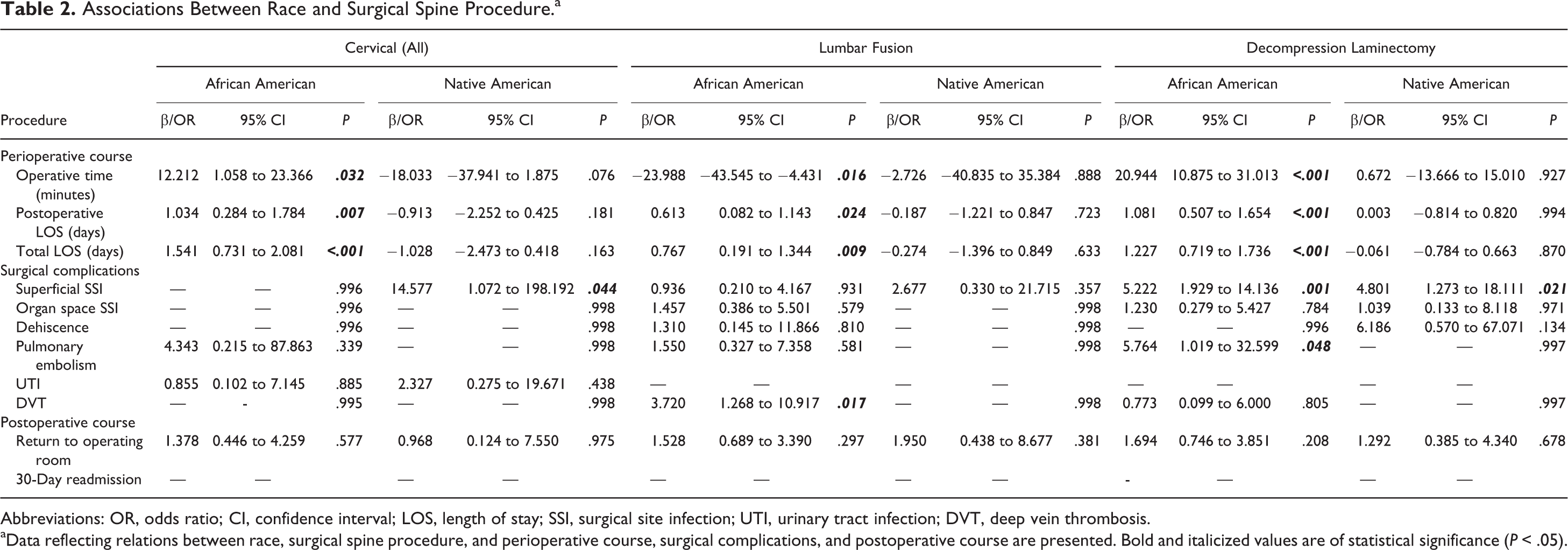
Abbreviations: OR, odds ratio; CI, confidence interval; LOS, length of stay; SSI, surgical site infection; UTI, urinary tract infection; DVT, deep vein thrombosis.
aData reflecting relations between race, surgical spine procedure, and perioperative course, surgical complications, and postoperative course are presented. Bold and italicized values are of statistical significance (P < .05).
Lumbar Fusion
Lumbar fusion procedures totaled 1417, including 1226 CA, 154 AA, and 37 NA with significant differences among mean age (60.1 ± 12.8, CA; 54.2 ± 11.1, AA; 48.9 ± 12.9, NA; P < .001), mean BMI (31.5 ± 6.64, CA; 33.1 ± 7.11, AA; 30.6 ± 7.07, NA; P = .017), and mean morbidity probability (.052 ± .024, CA; .053 ± .024, AA; .044 ± .015, NA; P = .048). AA and NA patients demonstrated significant elevations in comorbidity burdens, with AA patients having higher rates of diabetes (15.7% CA; 27.3% AA; 16.2% NA; P = .001) and hypertension (55.6% CA; 63.6% AA; 37.8% NA; P = .012), while NA patients evidenced lower rates of hypertension (55.6% CA; 63.6% AA; 37.8% NA; P = .012) with higher rates of patient-reported smoking (21.3% CA; 24.7% AA; 59.5% NA; P < .001). AA patients had a shorter operative time (205.7 minutes, AA; 228.3 minutes, C; 227.1 minutes; NA) and had about a day longer length of stay (4.51 days, AA; 3.78 days, C; 3.38 days, NA). Race was an independent factor affecting both operative time and average length of stay (LOS), where AA patients had significantly shorter operative times (β = −23.988, 95% CI = −43.545 to −4.431, P = .016) and longer average length of stay (β = 0.767, 95% CI = 0.191 to 1.344, P = .009). AA race was an independent risk factor for deep vein thrombosis (OR = 3.720, 95% CI = 1.268 to 10.917, P = .017). NA race was not found to be independently predictive in lumbar fusion outcomes.
Decompression Laminectomy
Decompression laminectomies numbered 2210 in the available data, including 1942 CA, 181 AA, and 87 NA with significant differences among mean age (57.5 ± 15.6, CA; 55.6 ± 13.0, AA; 52.3 ± 14.7, NA; P = .002), average BMI (31.3 ± 6.62, CA; 32.3 ± 6.14, AA; 34.7 ± 6.64, NA; P < .001), and morbidity probability (.028 ± .019, CA; .030 ± .023, AA; .033 ± .015, NA; P = .023). AA and NA patients had higher comorbidity burdens including higher rates of diabetes (15.9% CA; 26.5% AA; 18.3% NA; P = .003) and hypertension (49.6% CA; 62.9% AA; 49.4% NA; P = .003) among AA patients, while NA patients demonstrated elevated rates of patient-reported smoking (19.5% CA; 26.5% AA; 35.6% NA; P < .001) and need for inpatient hospitalization (44.6% CA; 54.1% AA; 90.8% NA; P < .001). AA patients had a longer operative time (126.6 minutes, AA; 105.8 minutes, CA; 107.4 minutes, NA) and a day longer average length of stay (3.08 days, AA; 1.81 days, CA; 1.97 days, NA). AA race was found to be an independent risk factor for longer operative times (β = 20.944, 95% CI = 10.875 to 31.013, P < .001) and a longer average length of stay (β = 1.227, 95% CI = 0.719 to 1.736, P < .001). AA race was an independent risk factor for pulmonary embolism (OR = 5.764, 95% CI = 1.019 to 32.599, P = .048) and both AA and NA race were independent risk factors for superficial SSI (OR = 5.222, 95% CI = 1.929 to 14.136, P = .001, AA; OR = 4.801, 95% CI = 1.273 to 18.111, P = .021, NA).
Discussion
Disparity in American health care delivery has been clearly documented elsewhere; however, our aim in this analysis was to interrogate the degree to which differential quality of care was afforded to spine surgery patients as documented in the 2015 ACS-NSQIP database. Our analysis of 4803 spine surgery patients illustrates that disparities persist among 3 common surgical procedure categories along racial lines. These findings are in agreement with results previously reported by Seicean et al, in which analysis of spine surgeries performed from 2006 to 2012 and documented in the ACS-NSQIP database demonstrate comparable trends in similar patent populations. 14 Specifically, our analysis shows that AA patients continue to have longer lengths of hospitalization during their postoperative course by one full day compared with the CA cohort and that postsurgical complication rates including deep vein thrombosis and pulmonary embolism are significantly elevated in AA patients. In addition, we were able to identify a newly developing trend of increased rates of superficial SSI for AA after laminectomy in the 2015 dataset previously unreported by Seicean et al. 14 The logical although disheartening conclusion is not only that AA race continues to remain an independent risk factor for disparate outcomes in spine surgery as it pertains to postoperative complications and length of postoperative hospital stay, but that in the decade between 2006 and 2015 AA patients have developed still worsening rates of race-related outcomes with regard to infection rate.
Further discrepancies were observed in our cohorts of study as explained by NA race. NA often presented with intermittent comorbidity burden compared with CA and AA cohorts throughout all surgical procedures studied; however, they were reliably heavier consumers of tobacco products, consistent with self-reported tobacco use trends of NA communities documented in the literature. 27,28 Although consistently undergoing shorter operative times and length of postoperative hospitalization across all surgeries studied, NA patients incurred higher rates of superficial SSIs and required substantially greater likelihoods of inpatient hospitalization for cervical procedures and decompression laminectomies compared with other races. We theorize this may be in part due to as yet unidentified regional differences in surgical care provided by locations with a significant NA population, but at this time we cannot interrogate this question further as the ACS-NSQIP database does not provide data on the individual institutions. Furthermore, it is possible that customs and practices unique to NA individuals may contribute to these disparate outcomes. Regardless, our data suggests that NA experience greater wound-related complications than those documented among other races following spine surgery, necessitating special consideration when addressing this patient population.
Differences were also observed with regard to the frequency of racially correlated disparity within specific spine surgery procedures. Decompression laminectomies and related surgeries represented the category of surgical procedures with the greatest number of differential outcomes dependent on race, with both AA and NA race representing independent predictors of inferior quality of care. This is in contrast to the smaller impact explained by AA and NA race for cervical procedures or the lack of any predictive effect for NA race in lumbar fusions. This warrants future interrogation, as it indicates procedures that are less technically challenging may present the greatest risk for disparate outcomes as explained by race. It is possible that this can be explained due to greater standardization of procedures requiring greater technical skill or that these surgeries may require a greater degree of postoperative follow-up, which in turn can potentially reduce observable differences in care provided to racial groups.
Limitations
This is a retrospective review of the 2015 ACS-NSQIP database, which includes prospectively collected data from 603 hospitals across the United States. This study therefore is limited by both its retrospective nature and by the limits of the ACS-NSQIP data fidelity. As a retrospective study, our findings cannot be established with the same degree of certainty as a definitive causal relationship between race and surgical outcomes as it would be in an ideal randomized control trial. The ACS-NSQIP only collects postoperative complication data that falls within the 30-day period following surgery. Therefore, disparities in long-term outcomes of spinal surgery cannot be studied from this data. The database also does not provide institutional variables pertaining to contributing hospitals, including patient and community populations specifically served by hospitals participating in the ACS-NSQIP. As such, data gathered may not be entirely representative of the American demography. However, the ACS-NSQIP database has been reliably demonstrated by Huffman et al to be a reliable surrogate for analysis of postsurgical outcomes, justifying its use in this study. 29
Conclusion
We report findings from an analysis of a national database consisting of surgical outcomes across over 600 medical centers and 4803 spine surgery patients assessing whether race was an independent risk factor for complications following cervical procedures, lumbar fusion, or decompression laminectomy. Our results suggest that AA race was an independent risk factor for greater length of hospital stay and for increased rates of postoperative complications across all categories of spine surgery studied. In addition, NA race was also found to be an independent risk factor relating to superficial surgical site infections in cervical procedures and decompression laminectomies. While we do not expect change to be instantaneous, there remains a clear need for greater awareness of racial disparities in the spine surgery community in order to provide greater egalitarianism in care provided to these patients. Perhaps through continued investigation as to the underlying reasons for these disparities we may one day report that all patients in need regardless of race may equally benefit from the excellent care possible through the hands of a skilled practitioner of the surgical arts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.