
Abstract
Study Design:
Narrative review.
Objectives:
In this review, we address the question of whether the literature supports the notion that minimally invasive transforaminal interbody fusion (MIS-TLIF) improves outcome as compared with open TLIF (open-TLIF). Short and long-term outcomes, fusion rate, and cost-effectiveness were reviewed.
Methods:
This is a narrative review using various databases. Open-TLIF and MIS-TLIF studies were included and posterior lumbar interbody fusion studies were excluded. A description of paramedian incision in surgical technique was essential to the definition of MIS-TLIF. The present review included 14 prospective observational studies and 6 randomized controlled trials.
Results:
With short-term outcomes, some studies indicate a better outcome with MIS-TLIF regarding intraoperative bleeding, hospital stay, time to ambulation, postoperative narcotic use, and time to resume work. Both MIS-TLIF and open-TLIF surgeries improved Oswestry Disability Index, back pain, and leg pain. Some studies show that MIS-TLIF resulted in lower back pain than open-TLIF. Radiation exposure was higher with MIS-TLIF. In the longer term, clinical outcomes were improved in both MIS and open TLIF groups. Fusion rates were more than 90% in both MIS-TLIF and open-TLIF. Cost-effectiveness and length of surgery had mixed results.
Conclusions:
The potential benefits of MIS-TLIF might be present in the early recovery period after surgery. Long-term outcomes were similar with both MIS-TLIF and open-TLIF.
Introduction
As spinal surgery techniques have evolved, there has been an effort to reduce the morbidity of surgery. This has been especially important in open lumbar spinal fusion because of the significant tissue damage and the relatively long recovery time needed. Minimally invasive spinal surgery (MISS) has been developed to reduce the morbidity of lumbar fusion. Theoretically, MISS may have certain advantages over open surgery because of the smaller incision and potentially less injury to the paraspinal lumbar muscles and ligaments. In this review, we address the question of whether the literature supports the notion that minimally invasive transforaminal interbody fusion (MIS-TLIF) improves outcomes as compared with open TLIF (open-TLIF). We reviewed prospective studies on short-term (less than 6 months) and long-term clinical outcomes and cost-effectiveness analysis.
Materials and Methods
This is a narrative review. We included only open-TLIF and MIS-TLIF studies and excluded posterior lumbar interbody fusion (PLIF) studies. We searched for clinical studies in PubMed with the following keywords: ((transforaminal[All Fields] AND interbody[All Fields] AND (“lumbosacral region”[MeSH Terms] OR (“lumbosacral”[All Fields] AND “region”[All Fields]) OR “lumbosacral region”[All Fields] OR “lumbar”[All Fields]) AND (“Nucl Eng Des/Fusion” [Journal] OR “FUSION”[Journal] OR “fusion”[All Fields])) AND (minimally[All Fields] AND invasive[All Fields])) AND open[All Fields]. A total of 256 articles were included for the initial screen and reviewed by 3 surgeons (CHK, J-SL, J-YH). The EMBASE database was searched with the keywords transforaminal AND interbody AND fusion AND lumbosacral AND prospective, and 10 articles were screened. The Google Scholar database was searched with the conditions transforaminal lumbar interbody fusion AND minimally AND open AND prospective AND comparison, and 4800 articles were screened. Of them, prospective randomized controlled trials or cohort studies were included for further review, but studies comparing open PLIF and MIS-TLIF and single-arm studies were excluded. Only articles that described the use of paramedian incision(s) were considered to be MIS-TLIF articles. Consequently, the present review included 14 prospective cohort studies 1 -14 and 6 randomized controlled trials (Table 1). 15 -20 To summarize patient-reported outcomes, Forest plots were generated with software (RevMan 5, Cochrane Community, London, UK) for studies with available data of means and SDs.
Summary of Previous Studies.
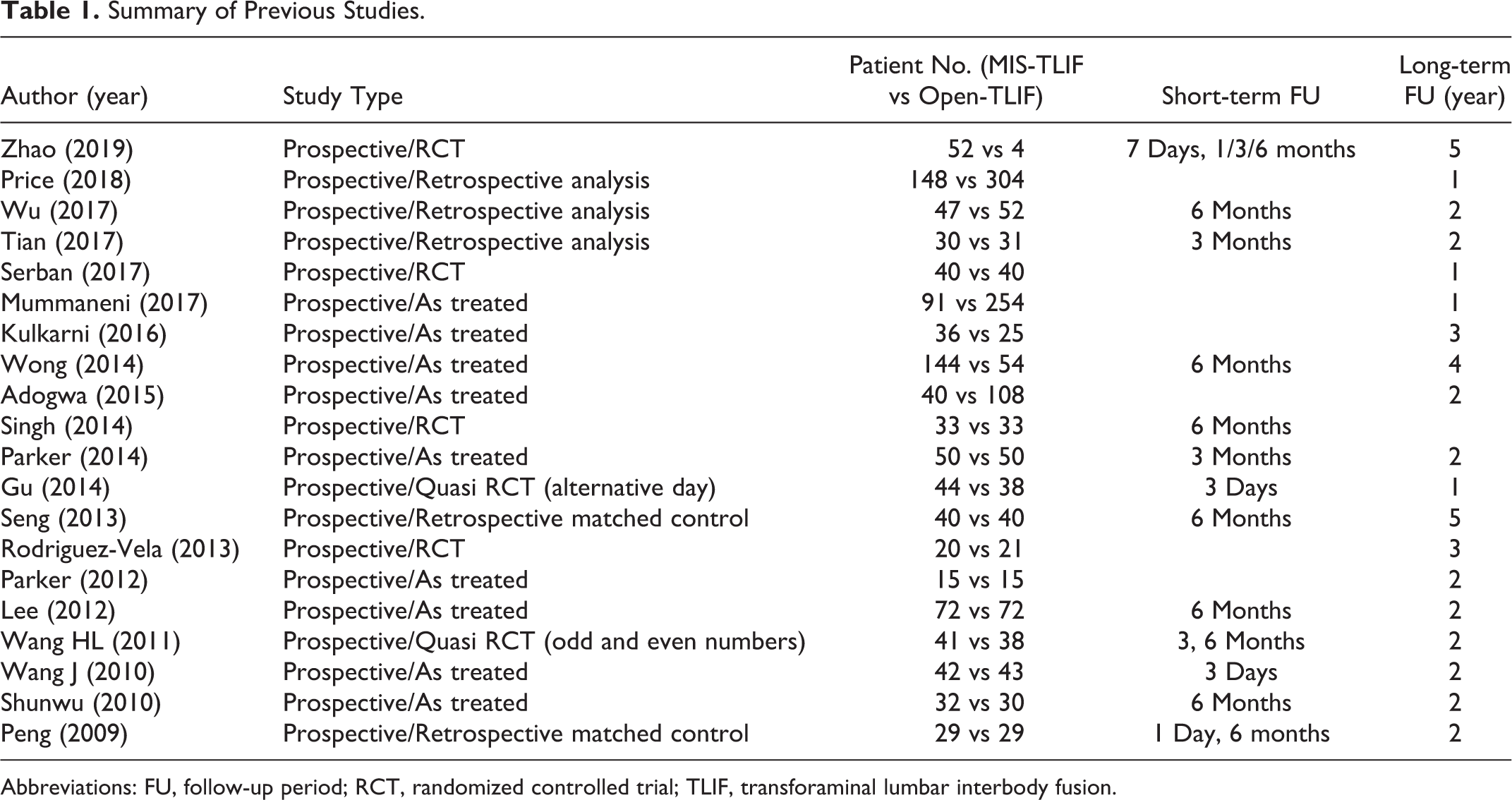
Abbreviations: FU, follow-up period; RCT, randomized controlled trial; TLIF, transforaminal lumbar interbody fusion.
Results
Short-Term Outcomes
For the purposes of reviewing the literature, we considered articles reporting outcomes of 6 months or fewer to be short-term outcomes. These studies focus on operative time, exposure to radiation, intraoperative bleeding, hospital stay period, postoperative narcotics use, return to work, and complications. There were 17 articles showing results of those parameters. 1 -12,15 -19
Results during the perioperative period were reviewed. Operative time was variable. Two studies showed that operative time was significantly shorter with MIS-TLIF by 40 minutes 6 and 70 minutes 16 ; 5 studies showed no difference 3,5,10,15,20 ; and 9 studies showed that operative time was significantly longer with MIS-TLIF by 10 to 90 minutes than with open-TLIF. 1,4,7 -9,11,12,14,17 The exposure to radiation was compared in 9 studies, and all studies showed significantly higher exposure to radiation with MIS-TLIF than open-TLIF, 2,3,5,7,10,11,15,19,20 58 fluoroscopic shots versus 8 fluoroscopic shots, 11 1.9 versus 0.75 mSv, 2 and longer fluoroscopic time (45-116 vs 17-82 s). 3,5,7,10,15,19,20 Intraoperative bleeding was significantly decreased by a range of 100 to 500 mL with MIS-TLIF than with open-TLIF in 11 studies. 1,2,5 -8,10,11,14,16,19 However, blood loss was not found to be significantly different between MIS-TLIF and open-TLIF in 6 studies. 9,12,15,17,20,21 Days before ambulation was significantly shorter by 1 day 4,5,7 or 2 days 10 with MIS-TLIF than open-TLIF. Hospital stay was significantly shorter by 1 day, 9,12,15,17,20,21 2 days, 5,9,17 3 days, 7,10,12,14,19 and 4 days, 3 with MIS-TLIF, but Wang et al 15 and Mummaneni et al 21 showed no difference between groups. The period of time that patients used opioid pain medication was reported in 2 articles; one showed that MIS-TLIF reduced total time of narcotic use by 2 days, 12 and another article reported reduction by 6 weeks. 8 The amount of morphine-equivalent medication use was significantly decreased by 16 to 30 mg during postoperative week 1 with MIS-TLIF. 5,10 The time to return to work was shorter with MIS-TLIF than with open-TLIF by 8.5 days 12 in 1 article and 4 weeks in 2 articles. 8,15
Short-term patient-reported outcomes (6 months or less) were reported in 11 articles. 1 -5,7,8,10,15,16,19 We included studies that reported parameters of Oswestry Disability Index (ODI), Visual Analogue Score for the Back (VAS-B) and Leg (VAS-L). All studies showed significantly improved scores compared with preoperative values, whereas several studies showed better improvement after MIS-TLIF (Figure 1). VAS-B was significantly lower with MIS-TLIF than with open-TLIF during postoperative days 1 to 3 in Peng et al 7 and Wang et al 3 at 3 months postoperatively by Tian et al 4 and 6 months by Peng et al, 7 Wong et al, 2 Singh et al, 16 and Wu et al. 1 However, no difference of VAS-B was reported between MIS-TLIF and open-TLIF at postoperative day 3 by Gu et al, 19 at 3 months by Parker et al 8 and Wang et al, 15 and at 6 months by Lee et al, 10 Seng et al, 5 and Wang et al. 15 ODI and VAS-L were not different between the 2 surgical groups during postoperative days 1 to 3, 3,7,19 at 3 months postoperatively 4,8,15 and 6 months postoperatively. 1,5,7,10,15,16 However, Shunwu et al 14 showed lower ODI at 6 months postoperatively, and Wong et al 2 showed lower ODI and VAS-L at 6 months postoperatively with MIS-TLIF as compared with open-TLIF. 2
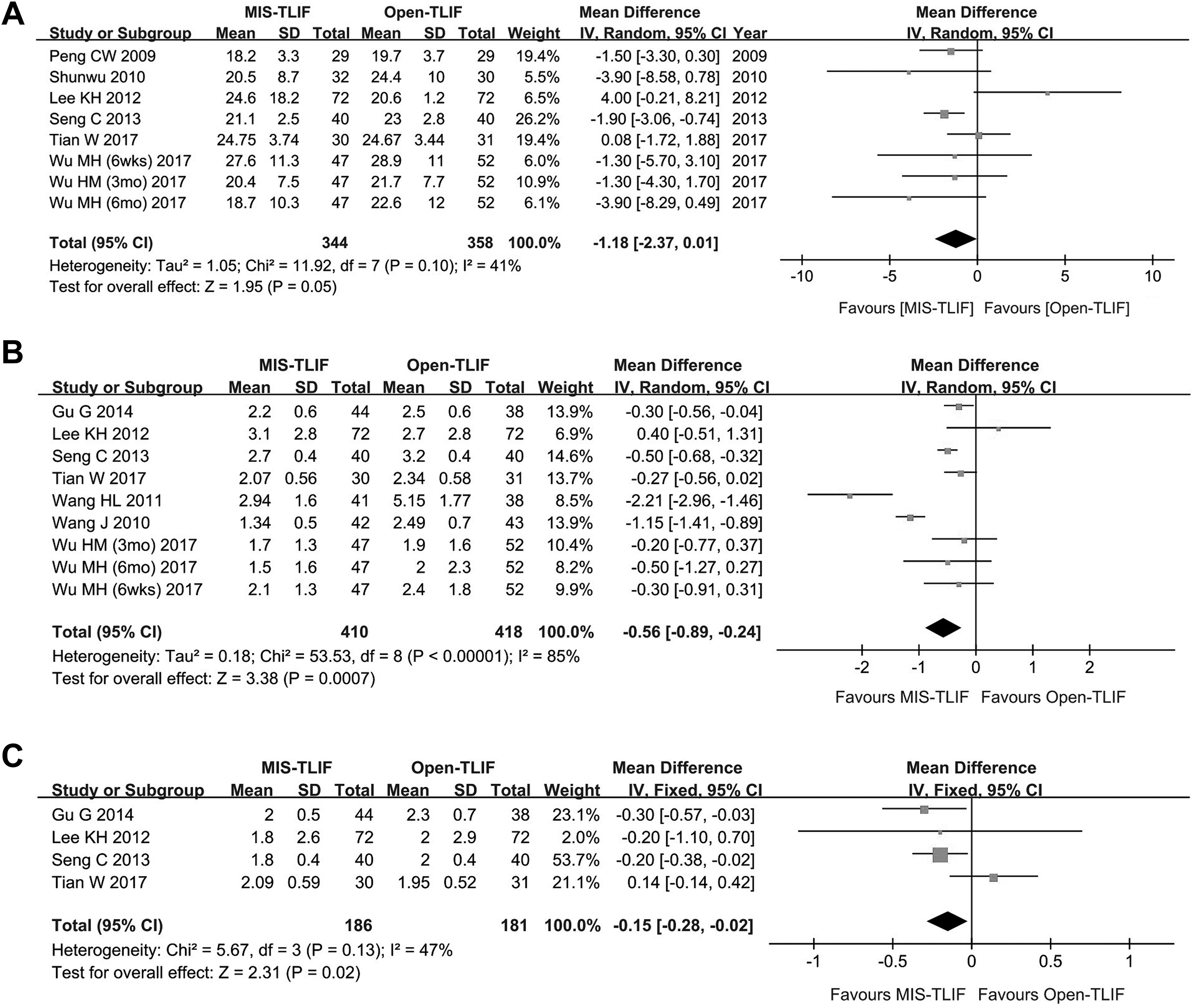
Forest plots for short-term clinical outcomes. Studies with available data of means and SDs are included in the graphs. The graph shows odds ratios and 95% CIs of each study. The pooled data show means and odds ratios of each parameter. A. Oswestry Disability Index. B. Visual Analogue Score for Back pain. C. Visual Analogue Score for Leg pain.
Complications were described in 12 articles, but statistical analysis were available in 2 of these articles. 1 -3,5,6,8 -10,15,17 -19 Gu et al 19 showed no difference in overall complication rate between open-TLIF (12.1%) and MIS-TLIF (11.4%; P = 1.0), whereas Wong et al 2 reported higher overall reoperation rate after open-TLIF (20.4%) than MIS-TLIF (8.3%; P < .01). 2 In the other 9 articles, complication rates were reported, but statistical comparisons between open and MIS-TLIF were not performed. These articles reported that the postoperative neurological deficit rate was 5% to 7.8% with MIS-TLIF and 9.3% with open-TLIF. 2,3 Surgical site infection was reported to be 1% to 4% after MIS-TLIF and 2% to 8% after open-TLIF. 6,8,15,17,19 Leakage of cerebrospinal fluid occurred in 3.5% to 8% after MIS-TLIF and 3.7% to 5% after open-TLIF. 2,3,8,18,19 Revision surgery for screw malposition was necessary in 2.1% to 5% after MIS-TLIF and 2% to 5.6% after open-TLIF. 2,3,8,18 Cage migration was reported by Wong et al 2 (0.7% after MIS-TLIF and 1.9% after open-TLIF) and Lee et al 10 (6.0% after MIS-TLIF and 8.8% after open-TLIF.
Return to operation room (OR) was compared in 3 articles. 2,4,8 Parker et al 8 showed no difference in returning to the OR for revision (P = .1); Two (5%) patients required a return to the OR after MIS-TLIF for malpositioned hardware, and 3 (8%) patients returned to the OR after open-TLIF for incision and drainage of a wound infection in 2 patients and malpositioned hardware in 1 patient. 8 Wong et al 2 showed that return to OR was required for screw malposition in 2, cage migration in 1, vascular injury in 1 after MIS-TLIF (2.7%, 4/144), and screw malposition in 2, cage migration in 1, and infection in 3 after open-TLIF (11.1%, 6/54). 2 Tian et al 4 showed that 1 patient in each group returned to the OR because of hematoma after MIS-TLIF (3.3%, 1/30) and deep injection after open-TLIF (3.3%, 1/31). 4 Parker et al 8 reported readmission during the postoperative 90-day global health period, and no patient required a readmission after MIS-TLIF, whereas 3 (6%) patients were readmitted for reoperation after open-TLIF. 8 Mummaneni et al 21 showed a 90-day readmission rate of 3.2% (3/91) after MIS-TLIF and 0.1% (2/254) after open-TLIF (P = .09).
Longer-term Outcomes
Longer-term Patient-Reported Outcomes
For this review, we analyzed 18 studies reporting outcomes more than 12 months to be longer-term outcomes; 4 studies reported outcomes at 1 year, 6,17,19,21 8 studies at 2 years, 1,3,4,7 -10,12 3 studies at 3 years, 11,18,20 1 study at 4 years, 2 and 2 studies at 5 years. 5,20 All studies showed significant improvement of ODI, VAS-B, and VAS-L compared with preoperative scores with both MIS-TLIF and open-TLIF. Forest plots were generated for studies with available data of means and SDs (Figure 2). The improvement was not different between groups in all parameters, except for better ODI with MIS-TLIF than with open-TLIF at 4 years postoperatively in a report by Wong et al 2 and better VAS-B with MIS-TLIF than with open-TLIF by Mummaneni et al 21 and Wong et al. 2 We included studies with more than 2 years of follow-up data, and the results were pooled in forest plots; MIS-TLIF in comparison to open-TLIF had lower ODI by 1.59 (95% CI, 0.34-2.85), VAS-B by 0.35 (95% CI, 0.07-0.76), and VAS-L by 0.14 (95% CI, 0.20-0.48; Figure 1). 4 -7,9,10,12,18,19
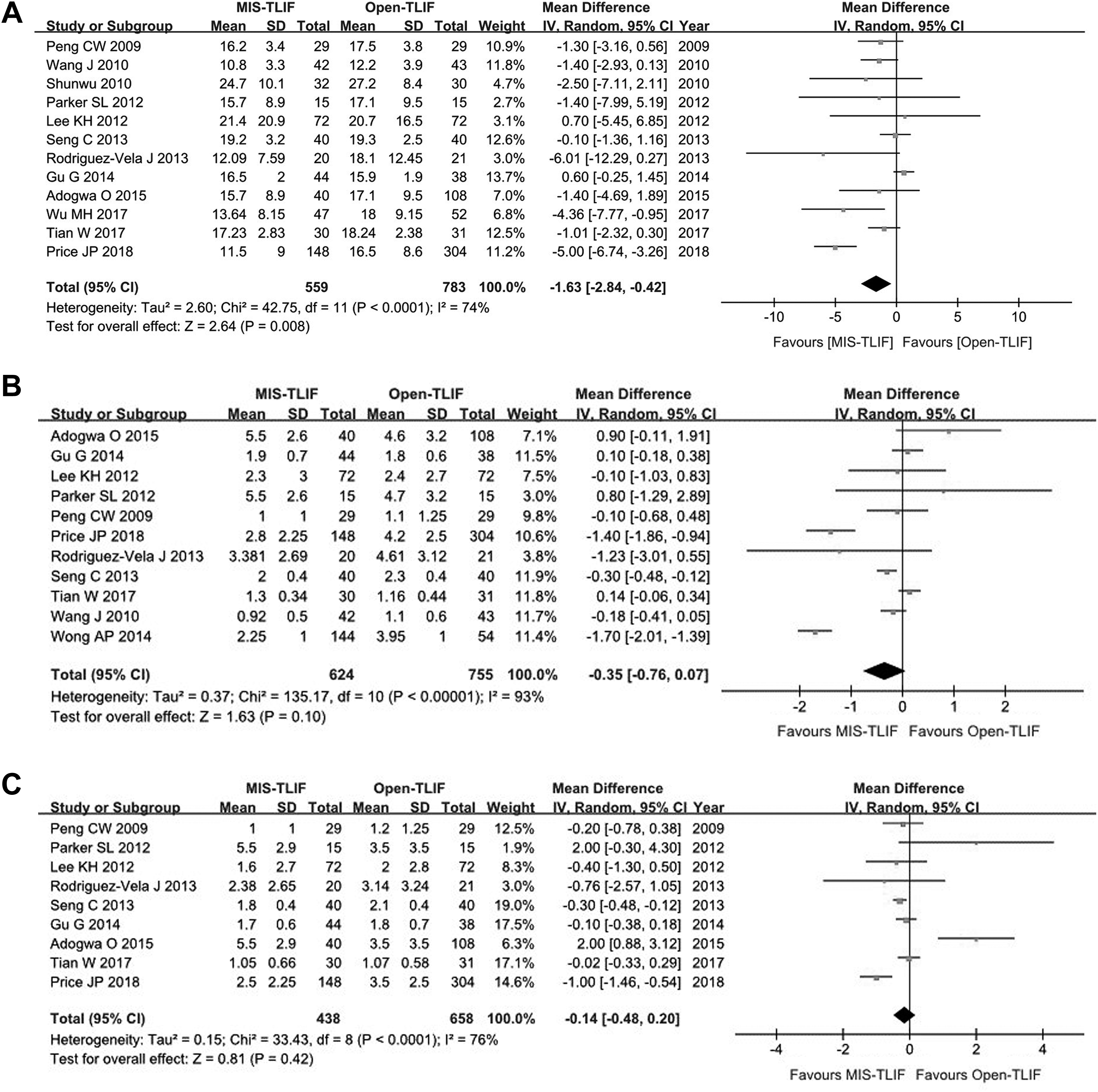
Forest plots for long-term clinical outcomes. Studies with more than 2-year follow-up periods are included in the analysis. Figure 1A showed the Oswestry Disability Index (ODI), Figure 1B showed Visual Analogue Score for Back pain (VAS-B), and 1C showed Visual Analogue Score for Leg pain (VAS-L). The graph shows odds ratios and 95% CIs of each study. The pooled data show means and odds ratios of each parameter. A. ODI. B. VAS-B. C. VAS-L.
There are 12 studies that reported ODI, VAS-B, and VAS-L at multiple time points. 1 -5,7,8,10,12,15,16,19 Of them, 6 studies showed a better VAS-B with MIS-TLIF during a short-term period, but the long-term outcomes at 2 years postoperatively were not different between MIS-TLIF and open-TLIF, except in the study by Wong et al. 1 -4,7,16 Wong et al 2 showed better outcomes of ODI, VAS-B, and VAS-L with MIS-TLIF at 6 months postoperatively. 2 Those clinical outcomes were not different at 24 and 36 months postoperatively, but ODI and VAS-B were better with MIS-TLIF than with open-TLIF at 4 years postoperatively. 2
Fusion Rate
A concomitant posterior lateral fusion between transverse processes is frequently performed to enhance fusion rate in open-TLIF, but not in MIS-TLIF. 22 Moreover, the interbody space preparation may be better with open-TLIF than MIS-TLIF, and fusion rate may be lower with MIS-TLIF than open-TLIF. Fusion rates were reported in 11 studies. 2 -7,9 -10,17,19 Two studies used computed tomography (CT) scans to define bony fusion. 2,17 In 7 studies, dynamic X-rays were utilized to define bony fusion, 3 -7,9 -11 and in 2 studies, CT scans were referenced for ambiguous fusion in dynamic X-rays. 4,19 The fusion rates were not significantly different between MIS-TLIF and open-TLIF, and the fusion rates ranged from 85% to 100% during the 1- to 5-year follow-up period based on dynamic X-rays (Figure 3). 3 -7,9 -11,17 Gu et al 19 and Tian et al 4 showed fusion rates of 92.5% to 96.7% after MIS-TLIF and 92.1% to 93.5% after open-TLIF based on dynamic X-rays in conjunction with CT scan (P > .05). 4,19 Wong et al 2 showed that fusion rates were 92.5% after MIS-TLIF and 93.5% after open-TLIF with CT scan analysis. 2 Serban et al 17 also showed a similar fusion rate of 90% after both MIS-TLIF and open-TLIF with CT scan analysis.
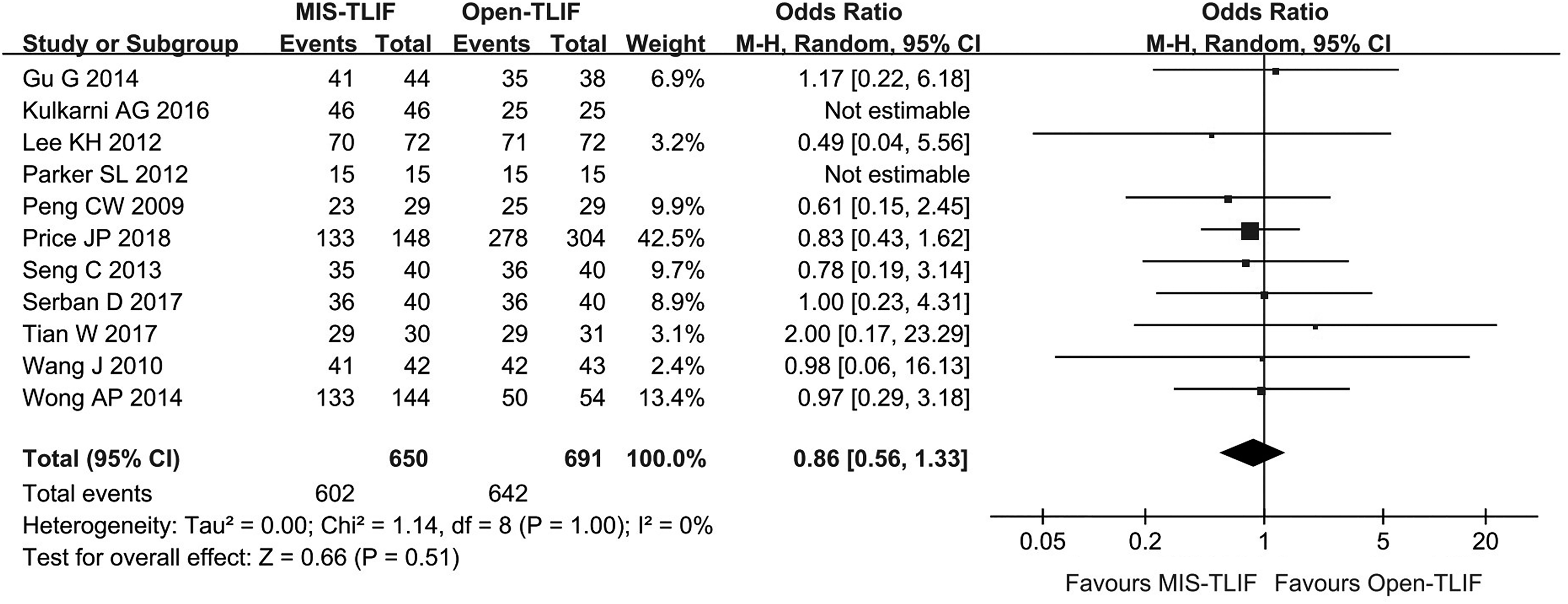
Forest plot for spinal fusion. The graph shows event, number of patients, odds ratios (ORs) and 95% CIs of each study. The pooled data show that the OR of spinal fusion after open-TLIF was not statistically different from that for MIS-TLIF (OR, 0.86; 95% CI, 0.56-1.33).
The graft materials used were autologous bone in 8 studies, 2 -5,7,11,17,19 autologous bone plus demineralized bone matrix in 2 studies, 9,10 and autologous bone plus recombinant bone morphogenic protein (rhBMP) in 1 study. 6 Price et al 6 showed that rhBMP was used in 93% of MIS-TLIF and in 71% of open-TLIF (P < .01), but the fusion rates were 90% and 91%, respectively (P = .19). 6 In summary, the studies showed fusion rates of more than 90%; however, there was a higher use of rhBMP in the MIS-TLIF cases. 2 -7,9 -11,17,19
Radiographic Outcomes
Segmental and lumbar lordosis, subsidence rate, and adjacent segment disease are also important outcomes. These outcomes were described in 2 studies. 2,5 Wong et al 2 reported that segmental correction of lordosis was 5.7° with MIS-TLIF and 4.1° with open-TLIF (P > .05). 2 In the same article, subsidence rate of interbody graft was 11.8% with MIS-TLIF and 11.8% with open-TLIF (P > .05). 2 Adjacent segment disease was reported by Seng et al 5 in 10% of patients after MIS-TLIF and in 10% of patients after open-TLIF during 2 to 4 years postoperatively. Other studies did not describe these radiological outcomes. 1,3,4,6 -12,15 -19 Thus, in the 2 studies that reported these imaging outcomes, there were no significant differences between open and MIS-TLIF.
Cost-effectiveness
Of the studies included, 2 studies compared direct costs 2,16 and 2 studies compared both direct and indirect cost 8,9 between MIS-TLIF and open-TLIF. Cost-effectiveness was evaluated by the incremental cost-effectiveness ratio (ICER) in 2 studies by Parker et al. 8,9 Bone graft may influence the cost, and rhBMP was used with open-TLIF in a study by Singh et al, 16 autologous bone with bone extender was used in 2 studies by Parker et al, 8,9 and only autologous bone was used in a study by Wong et al. 2 The direct costs during admission were US$19 925 with MIS-TLIF and US$23 479 with open-TLIF (P < .01) in the study by Wong et al. 2 Singh et al 16 also showed significantly less cost with MIS-TLIF (mean US$19 512) compared with open-TLIF (mean US$23 550; P < .01), 16 whereas Parker et al 8 showed no difference in direct cost between MIS-TLIF (US$27 621) and open-TLIF ((US$28 442; P = .5). 8 ICERs were calculated by Parker et al 8,9 in 2 studies. Parker et al 9 in 2012 showed no cost-effectiveness of MIS-TLIF over open-TLIF 9 : The total cost (direct + indirect) during 2 years postoperatively were US$35 996 with MIS-TLIF and US$44 727 with open-TLIF (P = .18), whereas mean quality-adjusted life years (QALYs) gained was 0.5 for MIS-TLIF and 0.41 for open-TLIF (P > .05). 9 Because of similar cost and QALYs gained, neither TLIF technique was more cost-effective. 9 However, ICER analysis by Parker et al 8 in 2014 showed contradictory results 8 ; MIS-TLIF was more cost-effective than open-TLIF during 2 years postoperatively. 8 MIS-TLIF cost significantly less total cost (direct + indirect cost; US$38 563) than open-TLIF did (US47 858; P = .03). 8 Short hospital stay reduced direct hospital cost by US$1758 with MIS-TLIF and shorter mean time to return to work cut indirect cost by US$8474 with MIS-TLIF. 8 Patients undergoing MIS-TLIF experienced a cumulative 2-year gain of 0.771 QALYs, and patients undergoing open-TLIF had a cumulative 2-year gain of 0.695 QALYs (P > .05). 8
Discussion
The Definition of MIS-TLIF
MIS-TLIF has been developed to reduce the morbidity of the exposure of open surgery while still preserving the hallmark features of the TLIF procedure such as posterior approach interbody fusion, decompression, and instrumentation. However, there is currently no unanimous definition for MIS-TLIF. 22,23 During open posterior lumbar surgery, the paraspinal muscles are detached from their origin/insertion causing more severe injury to the muscles. In contrast, MIS-TLIF seeks to minimize muscle injury by using paraspinal exposure that seeks to split or dilate the muscles to reduce damage to the muscles. 23,24 Therefore, we suggest the following definition: MIS-TLIF is a posterior lumbar interbody fusion surgery accessed by muscle dilation or splitting with paramedian skin incision, and the access route is maintained with either a tube, cylindrical retractor blades, or sleeves. 23
Short-term Outcomes
Comparison of early outcomes are important in open-TLIF versus MIS-TLIF because much of the potential benefits of MIS-TLIF might be present in the early recovery period after surgery. The results were not unanimous throughout all studies, but the following results could be summarized. The majority of studies showed shorter operative times, lower intraoperative bleeding, shorter hospital stay, and lower rate of use of narcotics. 1 -12,16,17,19 Clinical outcomes were not greatly different between MIS-TLIF and open-TLIF, but forest plots favored outcomes for MIS-TLIF in ODI, VAS-B, and VAS-L. However, the total mean differences between the 2 groups were within minimal clinically important difference (MCID), and clinical significance may be minimal (Figure 1). Complication rates seemed to be similar between both groups. 1 -3,5,6,8 -10,15,17 -19 Return to OR or readmission during 90 days postoperatively did not occur more often with MIS-TLIF than open-TLIF. 2,4,8 In summary, it is difficult to discern a significant difference in complication rates between MIS and open TLIF because these parameters were not the primary outcome that the study was powered to measure. One of the major concerns about MIS-TLIF is inevitable increased radiation exposure. 2,3,5,7,10,11,15,19 With the use of navigation, the exposure to radiation may be decreased. 25 -27
Long-term Outcomes
Clinical outcomes were similar between MIS-TLIF and open-TLIF, but forest plots showed a trend for favored outcomes with MIS-TLIF in ODI, VAS-B, and VAS-L (Figure 2). However, the total mean differences between the 2 groups were within MCID, and clinical significance may not be meaningful (Figure 2). Fusion rates were similar between open-TLIF and MIS-TLIF, 2 -7,9 -11,17,19 but there was a higher rate of rhBMP use in MIS-TLIF. 6 The changes in radiological parameters between MIS-TLIF and open-TLIF were similar, but this issue was not sufficiently studied. 2,5
Cost-effectiveness
Comparing the cost-effectiveness between MIS-TLIF and open-TLIF is important in the current economic climate. 2,8,9,16 Parker et al 8,9 showed that QALYs gained were similar with both open-TLIF and MIS-TLIF. Parker et al 8,9 calculated ICERs considering both direct and indirect cost but showed contradictory results in 2 articles in 2012 and 2014. In summary, cost-effectiveness between 2 surgical techniques could not be judged based on previous studies.
Conclusion
The potential benefits of MIS-TLIF might be present in the early recovery period after surgery, whereas long-term outcomes were not different between MIS-TLIF and open-TLIF. MIS-TLIF reduced direct costs mostly by reducing hospital stay and indirect cost by expediting return to work. However, cost-effectiveness of MIS-TLIF over open-TLIF seemed to be controversial based on ICER analysis. Although there have been many prospective studies, statistical power needs to be considered in accepting the results. In the future, studies with significantly larger power are necessary to better delineate the differences between MIS and open-TLIF outcomes and costs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from the Carl Zeiss Meditec Group.