
Abstract
Study Design:
Retrospective radiographic review.
Objectives:
Our objectives were to (1) compare the ability of fulcrum bend radiographs and traction radiographs under general anesthesia to predict correction of adolescent idiopathic scoliosis (AIS) using pedicle screw only constructs and (2) compare the fulcrum bend correction index (FBCI) with a new measurement: the traction correction index (TCI).
Methods:
This is a retrospective radiographic review of 80 AIS patients (62 female and 18 male), who underwent scoliosis correction with pedicle screw only constructs. The mean age at surgery was 14 years (range 9-20 years). Radiographic analysis was carried out on the preoperative and immediate postoperative posteroanterior standing radiographs and the preoperative fulcrum bend radiographs and traction radiographs under general anesthesia. FBCI is calculated by dividing the correction rate by the fulcrum flexibility and TCI is calculated by dividing the correction rate by the traction flexibility.
Results:
Preoperative mean Cobb angle of 63.9° was corrected to 25.8° postoperatively. The mean fulcrum bending Cobb angle was 37.6° and traction Cobb angle was 26.6°. The mean fulcrum flexibility was 41.1%, traction flexibility 58.4%, and correction rate 59.6%. The median FBCI was 137% and TCI was 104.3%.
Conclusions:
When comparing fulcrum bend and traction radiographs, we found the traction radiographs to be more predictive of curve correction in AIS using pedicle screw constructs. TCI takes into account the curve flexibility better than FBCI.
Keywords
Introduction
Traditionally, correction rate has been used to describe radiographic correction in scoliosis surgery. This does not take into account the flexibility of the curve. Hence a method based on fulcrum bend radiographs to assess scoliosis correction taking flexibility of the curve into account was proposed, called the fulcrum bend correction index (FBCI). 1
FBCI is calculated by dividing the correction rate by the fulcrum flexibility (based on fulcrum bending radiographs) and is expressed as a percentage. FBCI close to 100% suggests that the instrumentation has taken up all the flexibility revealed by the fulcrum bending radiographs. 1 It has been suggested that fulcrum bend radiographs predict curve correction in adolescent idiopathic scoliosis (AIS). 2,3
However, it has been shown that traction radiographs taken under general anesthesia (GA) are better at predicting flexibility of the scoliosis curve than the fulcrum bending radiographs. 4
Our objectives were to (1) compare the ability of fulcrum bend radiographs and traction radiographs under GA to predict correction of AIS using pedicle screw only constructs and (2) compare the FBCI with a new measurement: the traction correction index (TCI). TCI is calculated by dividing the correction rate by the Traction flexibility (based on Traction radiographs taken under GA) and is expressed as a percentage.
Materials and Methods
This is a retrospective radiographic study of 80 patients, who underwent posterior correction of scoliosis using pedicle screw only construct between 2005 and 2012. The mean age at surgery was 14 years (range 9-20 years). All patients had idiopathic scoliosis (62 female and 18 male). Two senior authors (IWN, MJH) performed all operations using pedicle screw only constructs (Depuy, Raynham, MA, USA).
Institutional review board approval was not sought because of the retrospective radiographic nature of the study.
Traction radiographs were performed, according to the method described by Davis et al. 5 On the day of the operation, under GA, with patient in supine position, one assistant applied longitudinal traction holding the ankles, another person applied counter traction holding the patient under the axilla, while the surgeon applied translatory pressure with a lead gloved hand over the apex of the curve and a anteroposterior radiograph was taken.
Fulcrum bending radiographs were performed, according to the method described by Luk et al. 1 The patient was asked to lie sideways over the fulcrum (radiolucent padded cylinder). For the thoracic spine, fulcrum is placed under the rib corresponding to the apex of the curve, assessed on the posteroanterior (PA) scoliosis radiographs and ribs counted from the lowest rib upward. For the lumbar spine, the fulcrum is placed directly under the apex of the curve. Sand bags are used to hold the patient in true lateral position and perpendicular to the x-ray beam while the radiographs are taken.
Radiographic analysis was carried out on the preoperative and immediate postoperative PA radiographs and the preoperative fulcrum bend and traction radiographs. Cobb angle was measured and correction rate, fulcrum flexibility, traction flexibility, FBCI, and TCI were calculated as follows (Formulas 1 -5):




Statistical Analysis
This was performed using IBM SPSS version 20 (IBM Corp, Armonk, NY) and StatsDirect version 3.0.150 (StatsDirect Ltd, Altrincham, UK). A power calculation was undertaken and to be 80% sure of detecting a 10 percentage points difference between fulcrum flexibility (%) and traction flexibility (%) measurements, with a standard deviation of 2.0, at the 5% significance level, 34 pairs of measurements would be required. Data was plotted and tested for normality. Where data was normally distributed, paired comparisons were made using paired t tests. The difference between the traction and the fulcrum-bend flexibility rate was evaluated using Wilcoxon’s matched pairs signed ranks test. Correlation between the traction and the fulcrum-bend flexibility rate was tested using Spearman’s rank correlation. Agreement of the fulcrum bend angle, the traction angle, and the postoperative angle was assessed using Bland-Altman analysis (Figure 1). 6
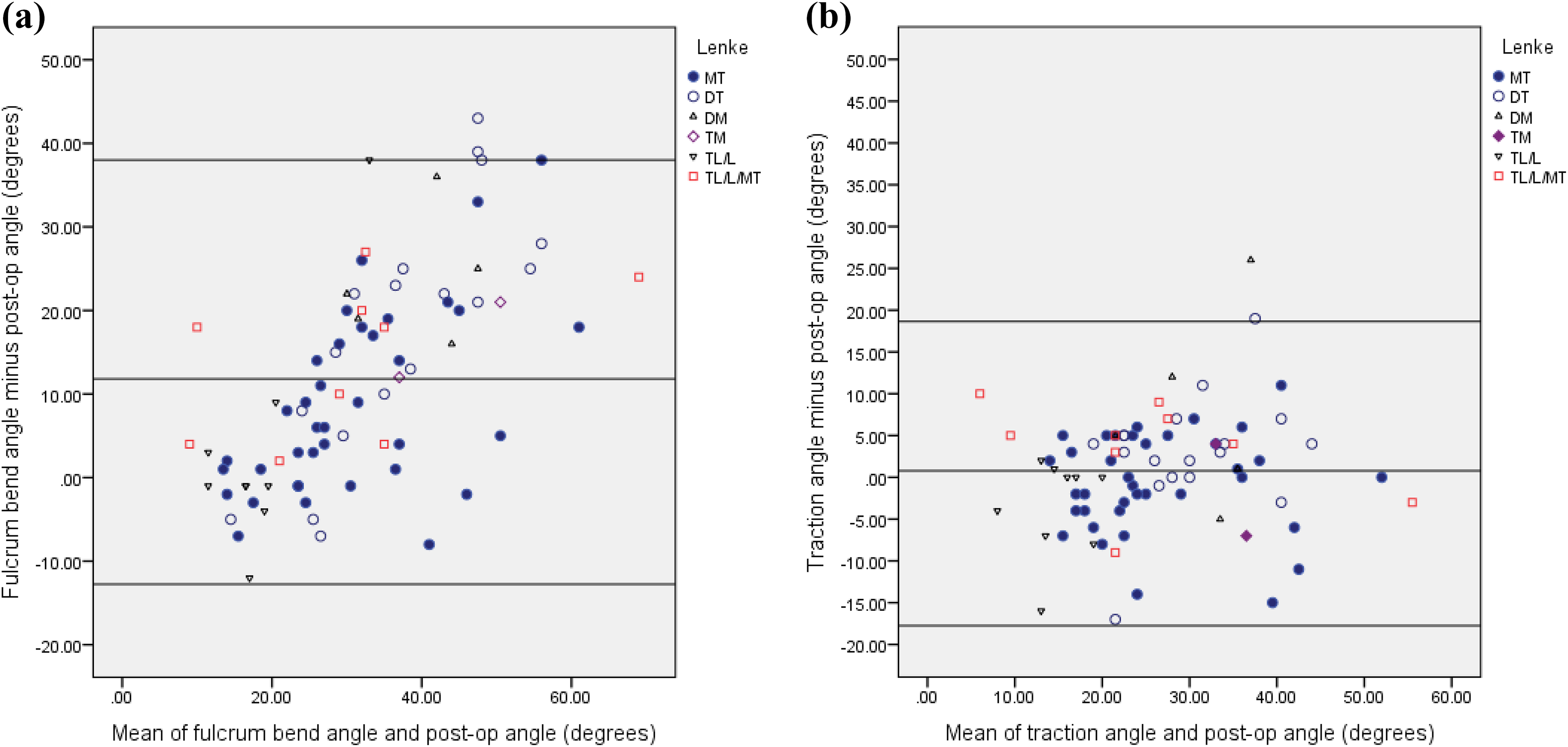
(a) Bland-Altman analysis graph to show the mean of the fulcrum bend angle and the postoperative Cobb angle (x-axis) plotted against the difference between these two measurements (y-axis: postoperative angle subtracted from the fulcrum bend angle). This shows a wide range of differences across the range of possible angles measured, indicating that the angle achieved postoperatively is often very different from the initial fulcrum bend angle. Mean difference = 11.84°, SD = ±12.87°, 95% limits of agreement were −12° to +38°. The sloping nature of the fulcrum bend /postoperative scatter indicates undercorrection at the lower end of the scale around 10° to 30° (where the postoperative angle is more than the fulcrum bend angle) and overcorrection at the other end, around 30° to 60° (where the postoperative angle is less than the fulcrum bend angle). In the majority of cases, the postoperative angle is less than the fulcrum bend angle, giving a positive difference (overall mean 11.84°). This was noticeably the case with Lenke main thoracic (MT), double thoracic (DT), and double major (DM) curves. The best results (with the smallest differences in angle) occurred among those with Lenke thoracolumbar/lumbar (TL/L) and some MT curves. (b) The equivalent graph for traction shows a much smaller range of differences between the initial and postoperative angles, indicating that the mean difference of all the cases is close to zero (0.79°, SD = ±7.07°); 95% limits of agreement were −18° to +19°. This was regardless of where on the spine the curvature was across the range of Lenke subgroups. There is also no obvious statistically significant under- and overcorrection that was found with the fulcrum bend angles.
Results
The mean preoperative Cobb angle of 63.9° (range 33°-106°) was corrected to 25.8° postoperatively (range 1°-57°). The mean fulcrum bending Cobb angle was 37.6° (range 11°-81°) and traction Cobb angle 26.6° (range 5°-54°) (Figures 2 –4). The mean fulcrum flexibility was 41.1% (range 4%-82%), traction flexibility 58.4% (range 34%-90%) (Figure 5), and correction rate 59.6% (range 30%-98%). The median FBCI was 137% (range 45%-2000%) and TCI was 104.3% (range 56%-196%) (Figure 6).
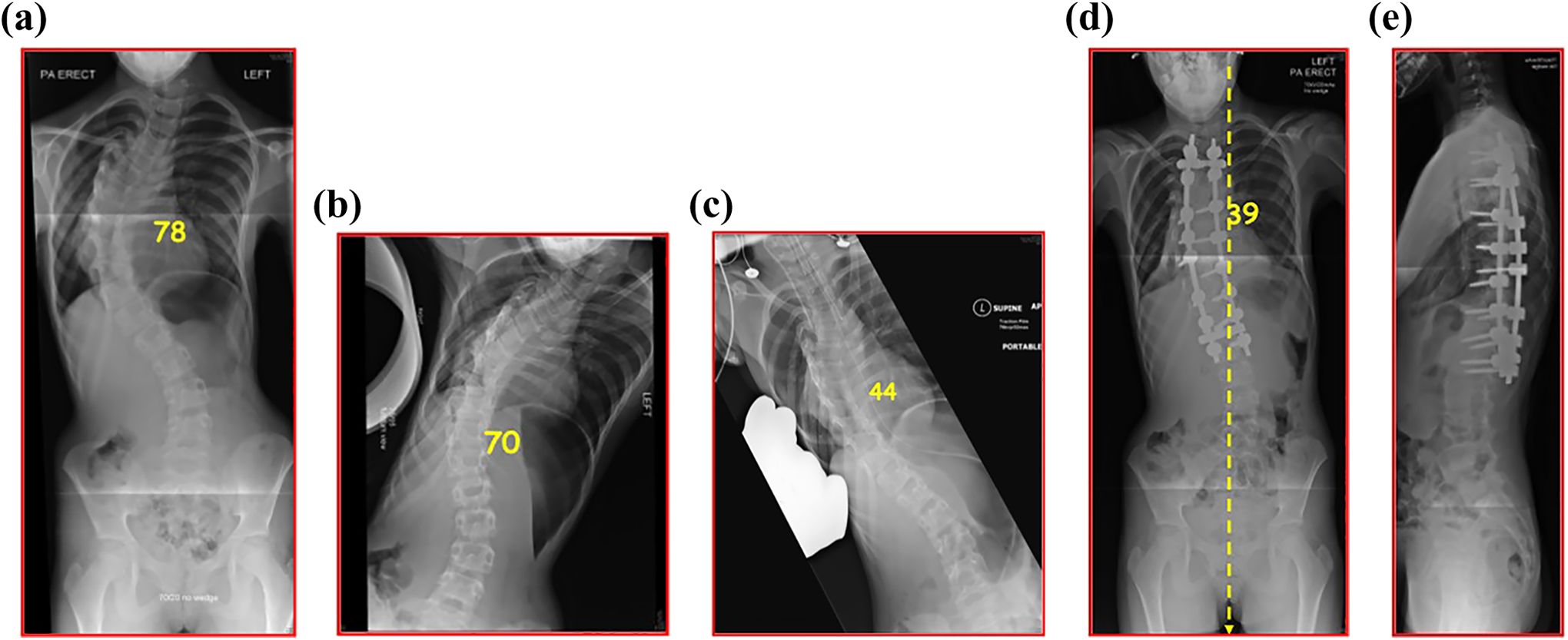
(a) Preoperative posteroanterior (PA) plain radiograph of 11-year-old girl with adolescent idiopathic scoliosis (AIS) showing right thoracic curve of 78°. (b) Fulcrum bend radiograph showing Cobb angle of 70° and (c) traction radiograph showing Cobb angle of 44°. Postoperative (d) PA and (e) lateral radiographs showing cobb angle corrected to 39°.
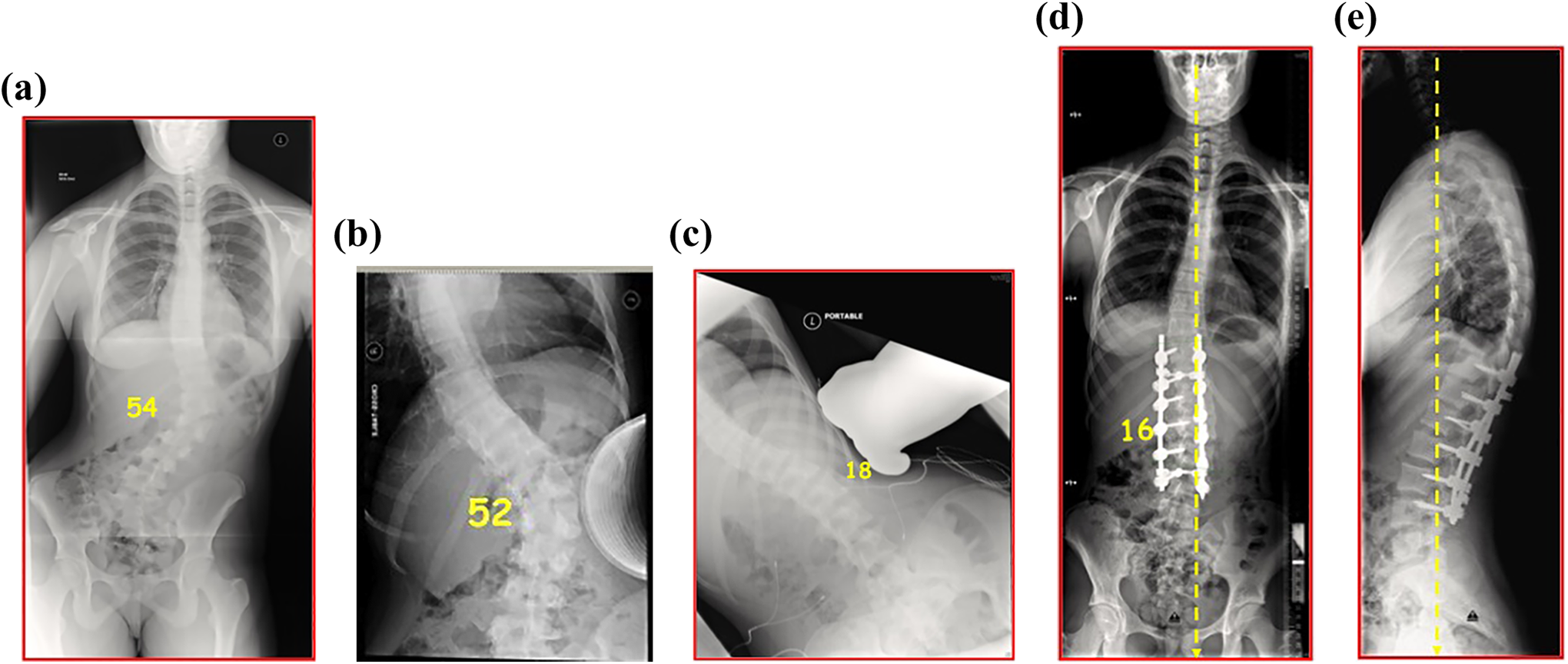
(a) Preoperative posteroanterior (PA) plain radiograph of 15-year old girl with adolescent idiopathic scoliosis (AIS) showing left lumbar curve of 54°. (b) Fulcrum bend radiograph showing Cobb angle of 52° and (c) traction radiograph showing cobb angle of 18°. Postoperative (d) PA and (e) lateral radiographs showing Cobb angle corrected to 16°.
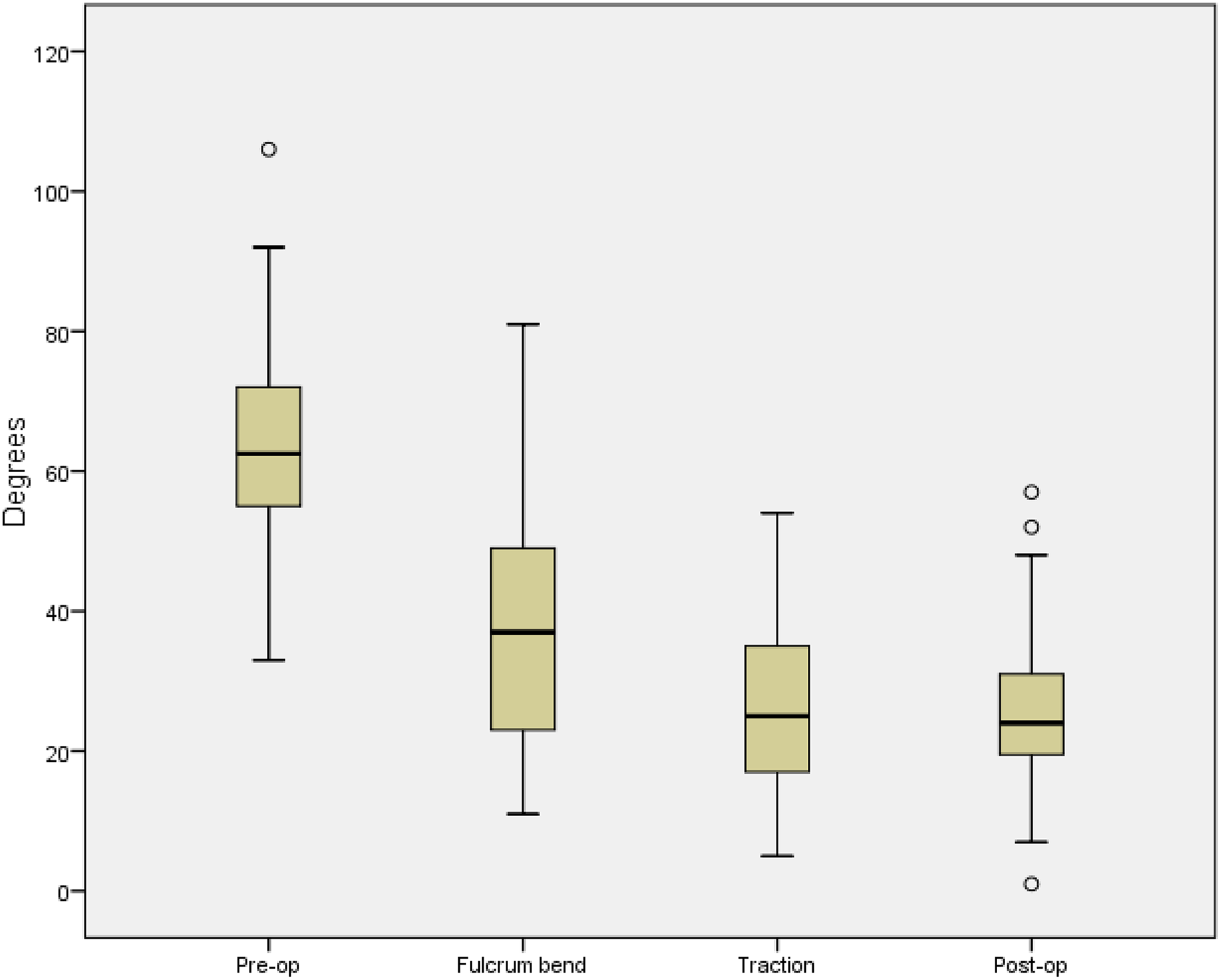
Box-and-whisker plot illustrating the median values and ranges of preoperative Cobb angle, fulcrum bend Cobb angle, traction Cobb angle, and postoperative Cobb angles.
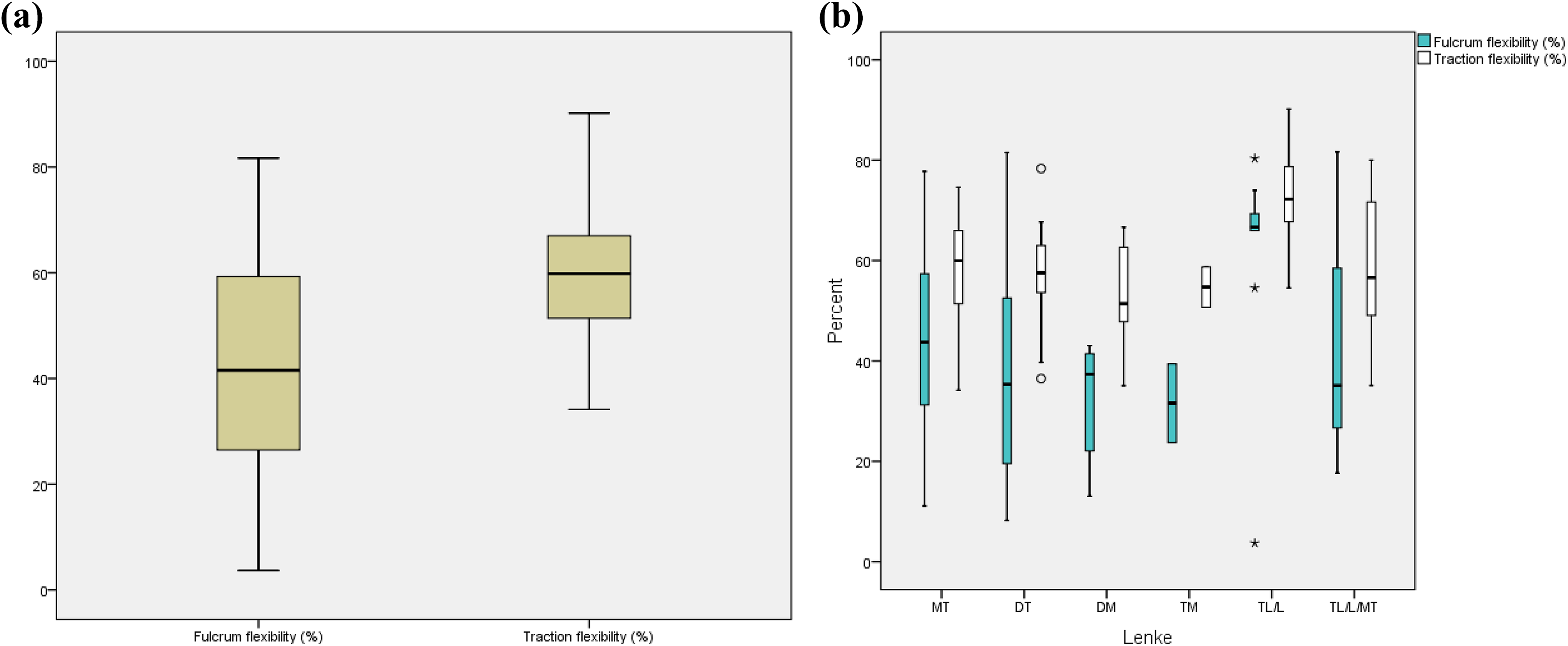
(a and b) Box-and-whisker plot illustrating the median values and ranges of fulcrum flexibility and traction flexibility.
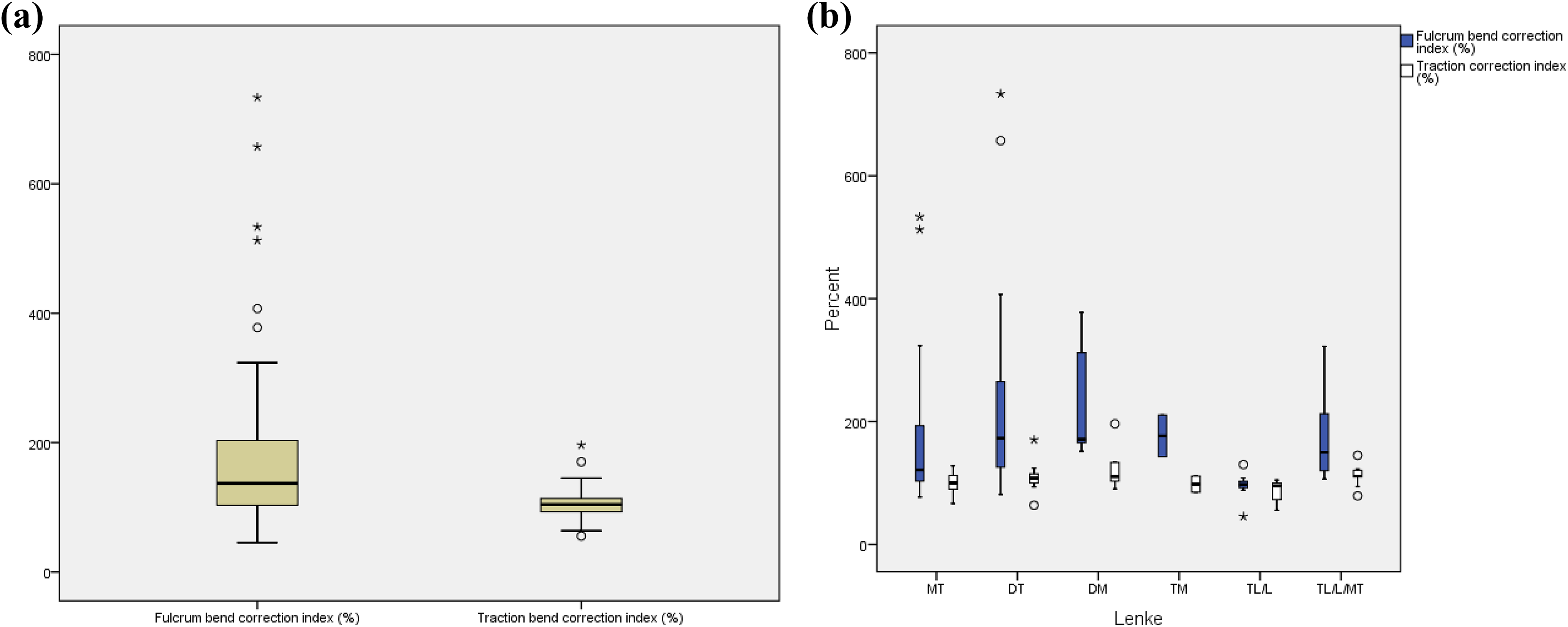
(a and b) Box-and-whisker plot illustrating the median values and ranges of fulcrum bend correction index (FBCI) and traction correction index (TCI).
There was one outlier, with a fulcrum flexibility of only 3.7%, which was almost 2 standard deviations from the mean. Hence this patient was excluded from the statistical analysis. The distributions of both fulcrum flexibility (%) and traction flexibility (%) were not significantly different from normal distributions (Shapiro-Wilk test, P = .119 and P = .741, respectively). A paired t test was therefore undertaken.
After excluding the aforementioned patient, mean traction flexibility was 59.12% (SD 12.25%), which was significantly greater than the mean fulcrum flexibility of 43.45% (SD 19.92%), t = −9.647, P < .001. The mean difference was 15.68%. This difference was seen between the 2 techniques regardless of the position of the structural curve (Figure 4b).
With regard to FBCI and TCI, these indices were not normally distributed, and comparisons were made using Wilcoxon’s matched pairs signed ranks test. Median TCI was 104.35 (interquartile range [IQR] = 21.85), and median FBCI of 137.04 (IQR = 107.5), z = −6.912, P < .001.
There were significant negative correlations of a number of variables with the age of the patient (all Ps < .005). These included the preoperative angle, the fulcrum bend angle, the traction bend, and the postoperative angle. However, neither FBCI nor TCI was significantly correlated with age.
Discussion
Accurate assessment of the flexibility of scoliosis curve is still necessary when pedicle screw only constructs are used for scoliosis correction. In patients with rigid curves, although anterior release is now seldom performed, in order to achieve better correction of scoliosis curve, posterior osteotomies are performed and increased number of pedicle screws used (increased metal density). 7 –9 Posterior osteotomies are recommended in rigid curves because it has been shown that intraoperative correction exceeding the preoperative bending correction of the curve, can lead to spinal cord injury. 10,11 Furthermore, in flexible curves, use of less number of pedicle screws and avoiding unnecessary osteotomies will decrease operation time, blood loss, cost of operation, and potential morbidity to the patient.
Numerous radiological methods have been used to determine the flexibility of the scoliosis curve preoperatively, including lateral side bending radiographs obtained with the patient in supine or standing position, push-prone radiographs, fulcrum bending radiographs, vertical traction radiographs without GA, 12 and traction radiographs under GA with and without translatory pressure applied over the apex of the curve.
Vedantam et al 13 compared the push-prone with the side bending radiographs and found that the application of pressure over the apex of the curve with push-prone method gave a better prediction of flexibility and correction. Duval-Beaupere et al, 14 suggested that the flexibility of scoliosis consists of 2 different components: collapse as a result of gravity stretching the convex elements and reducibility caused by correctional forces applied over the apex of the curve. Hence the combination of axial loading/traction and translatory force on the curve would be most likely to predict the postoperative correction of the curve. Other advantages of push-prone radiograph are its ability to assess the effect of forceful correction of primary curve on the compensatory curves above and below the level of fusion, and it is one radiograph compared to two radiographs for the lateral bending films. Disadvantages of push-prone radiographs are patient discomfort and standardization of amount of force applied on the apex of the curve. 13
Luk et al 1 compared the fulcrum bending radiographs with lateral bending radiographs and found the former to be more predictive of flexibility and correctability than the latter, when segmental spinal instrumentation using hook constructs were used. Recently Li et al 15 compared newly designed Changai hospital fulcrum bend radiographs (CH-Fulcrum) (20 cm high metal box with a lid, which can be lifted up to 12 cm with a gear and electronic pressure monitor under the lid) with traditional fulcrum bend radiographs (FBRs) and supine side bending radiographs. They found that the CH-FBRs provided significantly more correction than traditional FBRs and supine side-bending radiographs, and CH-FBR values were closer to the postoperative correction achieved using pedicle screw constructs than the traditional FBRs. Li et al 15 suggested that traditional FBRs depend on fulcrum size selection, which determines the corrective force provided by the patient’s body weight against the fulcrum. CH-FBR provided 2 new parameters: (1) variable height and (2) measurable weight, thus standardizing the FBR by optimizing the force applied across the fulcrum. In order to perform the CH-FBRs, special CH-Fulcrums are needed, which are not widely available.
Zhao et al 12 reported vertical traction without GA in 27 patients treated with hybrid hook screw instrumentation. They found that traction films under predicted postoperative curve correction and attributed this extra correction to GA induced muscle relaxation and muscle dissection during operation. Davis et al 5 compared traction under GA with side bending radiographs and found that the traction radiographs demonstrated significantly greater curve flexibility than supine bending radiographs in curves both above and below 60°. Anterior release was avoided in 11 out of 13 patients after review of traction radiographs. Hamzaoglu et al 16 compared traction under anesthesia, fulcrum bending radiographs, and supine lateral bending radiographs. They found statistically no significant difference between fulcrum bend radiographs and traction radiographs in curves <65°; however, traction radiographs were better in curves >65°. The traction method described in their study was different from that described by Davis et al. 5 Hamzaoglu et al 16 and Zhao et al 12 applied traction to the cervical spine without any apical translatory force. We used the method described by Davis et al 5 with traction under GA, which included additional translatory force applied over the apex of the curve. Ibrahim et al 4 from our institute reported on a mixed group of patients (19 patients with all pedicle screw instrumentation and 14 patients with hybrid pedicle screw laminar hook instrumentation) comparing traction under GA with fulcrum bend radiographs in curves >60° and found that the former were better than latter at predicting the flexibility of the curve and avoided anterior release surgery in 19 out of 22 patients based on criteria of Cheung et al. 2 Traction radiographs taken under GA does not rely on patient compliance and because all the muscles are relaxed, it removes the muscle factors, which affect the flexibility. Traction radiograph technique described by Davis et al 5 incorporates both components suggested by Duval-Beaupere et al 14 regarding the flexibility of the curve. Axial traction forces combined with translatory force at the apex of the curve gives a better picture of flexibility of the curve. Hasler et al, 17 in their functional, radiographic analysis of idiopathic thoracic scoliosis, found significant, homogenous segmental tethering confined to 4 periapical levels. Hence translatory force on the apex of the curve in our view is essential to identify the true flexibility of the curve. It also shows the effects of this force applied on the primary curve on the compensatory curves preoperatively, which may lead to coronal imbalance.
Our objectives of this study were to (1) compare the ability of fulcrum bend radiographs and traction radiographs under GA to predict correction of AIS using pedicle screw only constructs and (2) to compare the FBCI with TCI.
To describe radiographic outcome of scoliosis curve correction, traditionally correction rate has been used. However, this does not take into account flexibility of the curve. Surgical flexibility index (SFI) was used by Wojcik et al. 18 SFI took into account flexibility of the curve and was calculated by dividing the correction rate by the lateral bending film correction, expressed as a percentage. Wojcik et al 18 found mean SFI of 222% after Harrington-Luque instrumentation and 362% after Cotrel-Dubousset instrumentation. This can be misleading, because it conveys that these instrumentations can result in 2 to 3 times more correction than the flexibility of the spine would allow.
Luk et al 1 used FBCI, based on the fulcrum bending radiographs, which accurately predicted postoperative correction of scoliosis when hook constructs were used.
However, when pedicle screw constructs were used for scoliosis correction, it was found that pedicle screw constructs achieved better scoliosis correction compared with fulcrum bend radiographs. 19 In their study, the mean fulcrum bending Cobb angle was 28° and postoperative Cobb angle was 15°. This suggests that there was underprediction of the curve correction with the fulcrum bend radiographs. Furthermore, FBCI was 122% for flexible curves and 203% for rigid curves. If FBCI was an accurate predictor of curve correction, then the figure should approximate 100%, indicating that the fulcrum bend radiographs under predict curve correction obtained using pedicle screw constructs. This under prediction can be misleading to the operating surgeons, causing them to use excessive number of pedicle screws unnecessarily and or to perform unnecessary posterior osteotomies leading to increased operating time, blood loss, cost of operation, and potential morbidity to the patient. In our study, we found that median TCI was 104% while FBCI was 137%. This suggests that traction films performed under GA are better at predicting the curve correction than the fulcrum bend radiographs when pedicle screw only constructs are used. This accurate prediction of curve correction can help the surgeon to use appropriate number of pedicle screws and avoid unnecessary posterior osteotomies.
Conclusion
We found traction radiographs to be more predictive of curve flexibility and curve correctability than the fulcrum bend radiographs in patients who had pedicle screw instrumentation for the correction of scoliosis. TCI takes into account the curve flexibility better than FBCI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.