
Abstract
Study Design
Retrospective Cohort Study
Objectives
Mid-term Anterior Vertebral Body Tethering (AVBT) results demonstrate an acceptable degree of clinical success, yet the revision rate remains notably higher than fusion. Fulcrum-bending radiographs have previously been shown to more reliably predict radiological outcomes in Adolescent Idiopathic Scoliosis (AIS) as compared to supine-lateral bending radiographs. This study aims to discern how Fulcrum Flexibility Rate (FFR) correlates with Correction Rate (CR) and establish whether this can reliably predict residual deformity following AVBT surgery.
Methods
A review of 38 consecutive AIS patients undergoing thoracic AVBT between 2015 – 2020 was performed. Preoperative (standing and fulcrum-bending) and postoperative (first-erect) radiographs were evaluated for curve magnitude using the Cobb-method. The FFR, CR and Fulcrum Bending Correction Index (FBCI) were calculated. Patients were also percentile-ranked according to their FFR and dichotomized into flexible and rigid cohorts for comparison. Student t-test, Pearson correlation and linear stepwise regression was applied.
Results:
AVBT resulted in a significant improvement in the major Cobb angle (Preoperative: 50.9±7.5° vs Postoperative: 19.9±9.4°; P < .0001) with a mean FBCI of 98.0%. Bivariate correlation revealed a moderate relationship between fulcrum-bending and first-erect Cobb angle (r = .5306, P = .0006). Linear regression demonstrated a predictive relationship between fulcrum-bending and first-erect Cobb using the equation ‘Postoperative Cobb = 7.5 + .65(Fulcrum-bending Cobb).’
Conclusion:
This is the first study to demonstrate the ability of fulcrum-bending radiographs to predict early radiographic outcomes following AVBT, ‘timepoint-zero’ for the growth modulation process.
Keywords
Introduction
Assessing the flexibility of the deformed spine in patients with scoliosis is an important aspect of preoperative surgical planning and can directly influence the surgical technique, approach and selection of instrumented levels.1-5 Even though the surgical treatment of Adolescent Idiopathic Scoliosis (AIS) traditionally involves the rigid fusion of structural curves, there remains a continued drive to research and develop treatments that may offer the means to predictably correct a spinal deformity whilst preserving motion in the hope that patients may come to avoid sequelae of spinal arthrodesis such as adjacent segment disease, proximal junctional failure and flatback syndrome.6-14
Anterior Vertebral Body Tethering (AVBT) is an emerging technique involving the use of a braided polypropylene cord affixed to the convexity of a scoliotic spine via hydroxyapatite-coated vertebral body screws. It offers skeletally immature patients with AIS a means to apply the Hueter-Volkmann Law which states that growth is slowed when increased mechanical compression is applied and accelerated when load is reduced to the spine, leading to a passive deformity correction through growth modulation over time.14-18 Following regulatory approval by the US Food and Drug Administration (FDA) as a Humanitarian Use Device (HUD) in 2019, several recent North American studies have demonstrated promising mid-term results.18-20 However, the predictability and reliability of spinal growth modulation in-vivo remains unproven and depends on a complex interplay of factors including the expected growth remaining and the response of uninstrumented compensatory curves. To optimize outcomes, a better understanding of the optimal timing for surgery and the ‘desired’ initial correction is necessary.14,15,17,18
The amount of surgical correction achieved with AIS surgery is largely determined by patient factors (e.g. preoperative major Cobb angle, curve flexibility), technical factors (e.g. surgical technique, level selection) and implant choice (e.g. screw vs hook, metal rod vs flexible cord). Focusing on the assessment of curve flexibility, there are several well-described methods, with the supine lateral-bending radiograph being the most frequently encountered in clinical practice due to its relative ease of application.21-26 The supine-bending technique, however, has several notable limitations in that it largely relies on patient effort, which has been demonstrated to underestimate curve flexibility to the detriment of their treatment (e.g. addition of anterior releases; greater number of fused segments). 1 In 1997, Cheung and Luk 1 sought to improve and standardize the assessment of curve flexibility with the fulcrum-bending radiograph, where the awake patient is instructed to assume the lateral decubitus position over a padded radiolucent bolster carefully positioned at the apex of the curve whilst ensuring the ipsilateral shoulder or iliac crest is elevated off the table to increase the corrective force applied to the deformed spine. As such, fulcrum-bending radiographs have been shown to reduce the Cobb angle to a greater degree than supine-lateral bending radiographs and correlate more closely with postoperative radiological outcomes following spinal fusion surgery.1,27 When applied correctly, fulcrum-bending radiographs work particularly well for assessing main thoracic, thoracolumbar and lumbar curves.2,28
If fulcrum-bending radiographs can assist in predicting the initial correction achieved following AVBT (as opposed to fusion), this may improve prognostication of outcomes and facilitate decision making about patient selection and timing of surgery. This study aims to discern whether preoperative fulcrum-bending radiographs can provide a reliable estimate of expected curve size on first-erect radiographs in patients undergoing AVBT surgery for AIS and determine whether curve stiffness influences the magnitude of initial correction possible with this technique (i.e. ‘timepoint zero’ for the growth modulation process).
Methods
After obtaining Institutional Review Board (IRB) approval, a consecutive series of AIS patients treated with AVBT by a single surgeon at a single institution between 2015 and 2019 were retrospectively reviewed. To maximize homogeneity, inclusion in this study required the use of a single tether for curve types deemed to only necessitate surgical correction of a thoracic scoliosis in patients with a complete set of preoperative (standing PA and fulcrum-bending) and postoperative (first-erect; collected approximately 6 weeks post-op) radiographs. Exclusion criteria included non-idiopathic scoliosis, utilization of double cords, and patients with lumbar major curves. Fulcrum-bending radiographs were obtained using the technique originally described by Cheung and Luk, 1 as described earlier. A thoracoscopic-assisted mini-open approach, as is the senior author’s (BL) favoured technique, was utilized with tension applied across each motion segment determined using a combination of intraoperative fluoroscopy and a proprietary tensioning device. 29
To determine the effect of curve flexibility on postoperative Cobb angle, patients were percentile-ranked according to their Fulcrum Flexibility Rate (‘FFR’ = (PreOp Cobb – Fulcrum-bending cobb)/PreOp Cobb x 100) and dichotomized into top and bottom quartiles to compare patients with rigid (low FFR) and flexible (high FFR) deformities against their Correction Rate (‘CR’ = (PreOp Cobb – PostOp Cobb)/PreOp Cobb x 100). The Fulcrum-Bending Correction Index (‘FBCI’ = CR/FFR x 100) was then calculated to determine the corrective power of AVBT to treat coronal plane deformities, whilst accounting for preoperative curve magnitude and stiffness (Figure 1).1,2 Radiographic formulas.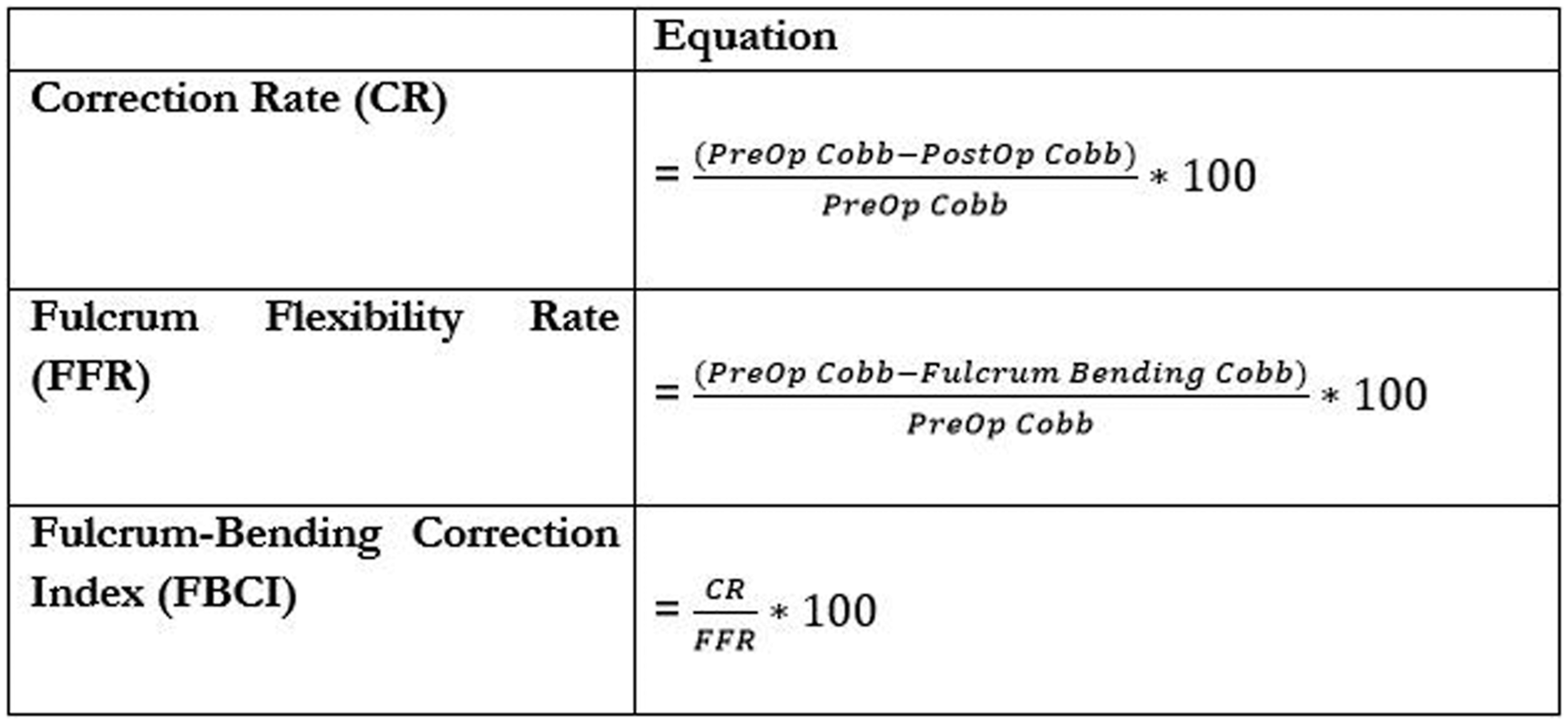
Student t-tests were used to compare radiographic outcomes of rigid and flexible deformities. Pearson correlation coefficients was used to assess the relationship between preoperative radiographic parameters (major and fulcrum-bending Cobb) and first-erect Cobb. A linear stepwise regression model was developed to provide a predictive model of first-erect Cobb angle following AVBT. The first-erect postoperative Cobb angle was set as the dependent variable with the patient’s age, fulcrum-bending Cobb and preoperative Cobb as independent variables. Statistical significance was set at P < .05.
Results
A total of 38 patients with a median age of 13.3 years met the inclusion and exclusion criteria for this study, 29 (76.3%) of whom were female. Patients varied in skeletal maturity, 28 (74%) were Risser grade <3. The majority had Lenke type 1 curves (n = 37; 98.1%), with only 1 (1.9%) classified as a type 2 deformity.
Improvements in Radiographic and Clinical Parameters Following AVBT.

ATR: anterior trunk rotation
A significant improvement in Angle of Trunk Rotation (ATR) was observed (Preoperative: 15.3 ± 3.9° vs Postoperative: 6.0 ± 2.9°; P < .0001) in addition to a significant reduction in the compensatory lumbar curve (Preoperative: 32.1 ± 7.5° vs Postoperative: 13.2 ± 7.7°; P < .0001).
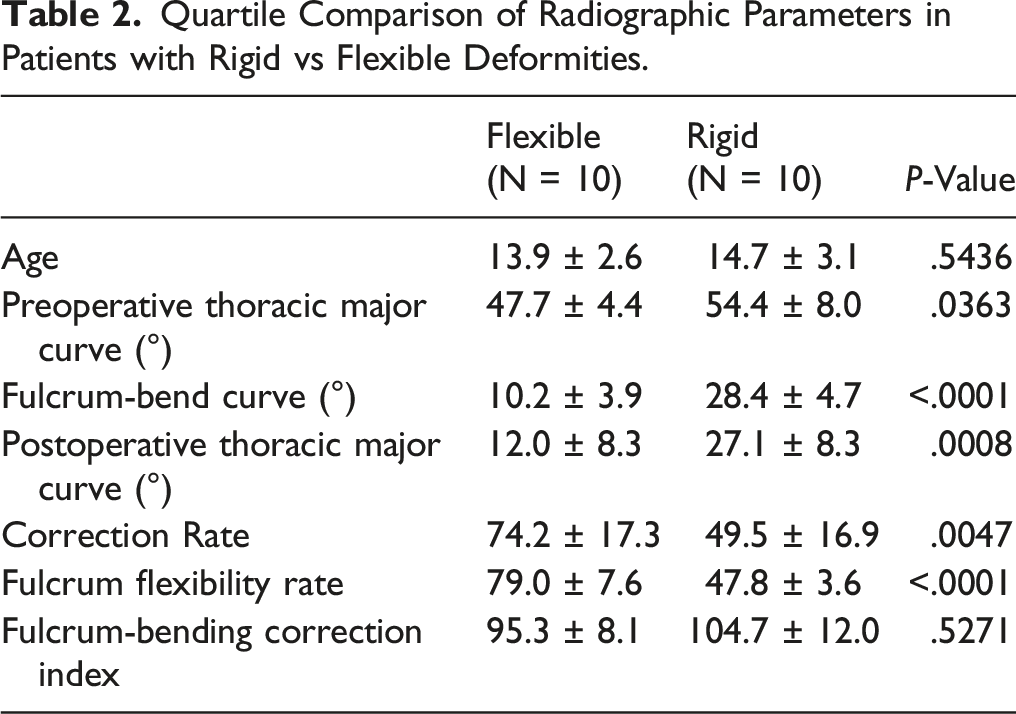
Quartile Comparison of Radiographic Parameters in Patients with Rigid vs Flexible Deformities.
Whilst bivariate correlation revealed a weak relationship between initial standing preoperative Cobb angle and first-erect postoperative Cobb angle (r = .2965, P = .0707), a moderate relationship was observed between fulcrum bending Cobb angle and first-erect postoperative Cobb angle (r = .5306, P = .0006). Linear stepwise regression analysis demonstrated a predictive relationship between fulcrum bending Cobb angle and the first-erect Cobb angle using the equation Postoperative Cobb = 7.5 + .65(Fulcrum bending Cobb), with R2 = .261 (P = .0006). The remainder of the independent baseline variables were excluded from the final predictive model as they did not reach statistical significance (P > .05).
Discussion
To our knowledge, this study is the first to extend the use of flexibility radiographs in AVBT beyond their usual application in curve classification by resurrecting a simple and well-described methodology to establish curve flexibility (FFR) and response to treatment (CR), which were originally used to assess and predict radiological outcomes among scoliosis patients undergoing posterior-based fusion surgery.1,2 With specific reference to the fulcrum-bending technique, several studies have demonstrated this to be more effective than standard supine bending radiographs as well as its ability to provide additional information such as segmental flexiblity.1,2,4,30,31 This conclusion was shared by Hay et al who applied this technique of evaluation to scoliosis patients undergoing anterior thoracoscopic fusion, 32 a surgical technique that ABVT has largely evolved from. Similar studies exploring the predictive ability of other radiographic methods (e.g. supine lateral bend) to assess curve flexibility may also be helpful as practices vary between institutions performing AVBT.
The results of this study demonstrate a moderate correlation between fulcrum-bending Cobb angle before surgery and first-erect Cobb angle following AVBT. This provides the context for a simple predictive algorithm clinicians may find helpful to inform discussions with patients and their parents about what 1 might expect, at least initially, following AVBT surgery and perhaps which patients will benefit least if they have a deformity that is ‘too rigid’ to permit a satisfactory initial correction. Whilst we were able to demonstrate that the accuracy of such a model may be improved with the inclusion of additional parameters such as standing preoperative Cobb angle, age, skeletal maturity and Fulcrum Flexibility Rate (FFR), the marginal gain in R2 achieved by increasing the required input variables into such a formula is likely to be of limited clinical value in day-to-day practice and was felt to overcomplicate its use.
This study is particularly relevant due to the large variation in outcomes reported following AVBT in early series.15,17,18,33 In 2020, Hoernschemeyer, Newton, and Miyanji et al separately published their institutions’ 2 to 5 year results demonstrating a revision rate between 15.8% and 41%.19,20,33 Clinical success, as defined by a residual curve at skeletal maturity of ≤ 30° in the first study and ≤ 35° in the latter 2, was found to be 74%, 59% and 77%, respectively. By comparing the baseline patient characteristics of the 3 studies, less favorable results were noted in younger, more skeletally immature patients.
In conjunction with several other factors, it is widely accepted that preoperative curve size and stiffness may influence level selection, approach and surgical technique.4,34 Our results demonstrate that patients with large and/or rigid deformities may not respond as well to the tethering technique, at least initially. In this study, ‘rigid’ curves were found to be preoperatively larger (54° vs 48°) and have a lower FFR (48% vs 79%) compared to flexible curves. We also observed a significant difference in the CR (50% vs 74%) between these groups, which may be an important consideration for determining a patient’s suitability for this technique as surgical techniques thought to improve correction of stiffer curves such as apical disc releases are still being explored and require further evidence to support their use.
To better compare the radiological outcomes of patients who differ in terms of their underlying curve magnitude and rigidity, the Fulcrum Bending Correction Index (FBCI) is used instead as CR alone fails to account for curve stiffness. It does so by expressing the difference between CR and FFR as a percentage (Figure 1). 2 Several studies have demonstrated FBCI is a reliable method of assessing and comparing the performance of an implant, technique or a surgeon in their ability to correct coronal plane spinal deformities.1,4,35 In this study, an overall FBCI of 98% was found, with no significant difference observed between rigid and flexible curves, suggesting that AVBT may, at best, produce a Cobb angle equivalent to that observed on a fulcrum bending radiograph. Whilst the ‘rigid’ cohort all achieved a first-erect Cobb angle below the surgical threshold for a fusion (Table 2), longer-term follow up is required to determine how this group perform with respect to patient reported outcome measures (PROMS), revision rates and their response to growth modulation.
Limitations of the study relate to the overall sample size, yet the strict inclusion criteria serve to limit the effect of confounding factors. A larger sample size would both permit a more robust stepwise regression analysis to improve upon the predictability of our model and make it permissible to stratify patients according to their skeletal maturity. If the correlation between fulcrum-bending radiographs, postoperative Cobb and correction achieved at final follow-up can be understood with greater granularity in respect to skeletal maturity, the uncertainty associated with the procedure’s longer-term outcomes may be reduced. As such, a longer-term study is warranted to determine if there is a relationship between curve flexibility, tether breakage, revision rates and the extent of growth modulation possible following AVBT. Another limitation of the study is the inability to compare the predictive ability of fulcrum flexibility radiographs to supine side bending radiographs which are also commonly used for pre-operative flexibility assessment. Future study comparing the predictive ability of the 2 imaging techniques to determine if 1 is superior to another is warranted.
Conclusion
In conclusion, this is the first study to demonstrate the predictive ability of fulcrum-bending radiograph to determine early radiographic outcomes following AVBT. Our data not only suggests that the initial correction observed following AVBT is likely to match the correction observed on the preoperative fulcrum-bending radiograph, it also highlights that large and more rigid curves are less amenable to initial correction using a single-cord AVBT technique.
The predictive algorithm described in this study may not only enhance patient selection by screening for cases with a lower likelihood of initial success, it may also be used to better inform patients (and their parents) about the size of the residual curve initially expected following AVBT surgery.
Although further study to explore the relationship between preoperative radiographic parameters (e.g. preoperative Cobb, FFR and skeletal maturity) and longer-term outcomes (e.g. radiographic correction, implant failure rate, return to theatre and patient reported outcomes) is warranted, an assessment of the likely initial correction achievable is an important first, as this represents ‘timepoint-zero’ for the growth modulation process.
Footnotes
Author Contribution
ZS, JT, LE, and BL-Conception and design, Acquisition and data, Analysis and interpretation of data, Drafting of the manuscript, Revision for important intellectual content, Statistical Analysis, Administrative, technical or material support, Supervision, and Approval final version of paper.
Declaration of Conflicting interest
Dr Lonner reports personal fees and royalty fees from Zimmer Biomet for The Tether—Vertebral Body Tethering System implant.Dr Lonner also reports personal fees, non-financial support and other from Depuy Synthes, personal fees and non-financial support from OrthoPediatrics, other from Paradigm Spine, non-financial support and other from Spine Search, other from Setting Scoliosis Straight Foundation, outside the submitted work. Dr. Lonner also reports royalities from Depuy Synthes; the Pradigm Spine COI is no longer relevant.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Material
The datasets analyzed during the current study are not publicly available due to Institutional Review Board guidelines but will be maintained for this study for up to 7 years post-publication as required by our institution’s review board and can be made available from the corresponding author.
Ethics Approval
This work was approved by the Institutional Review Board at Mount Sinai Hospital. IRB approved Study 19-00322
Consent to Participate
N/A- This work was approved as a retrospective chart review with a waiver of consent.