
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To determine whether there is an association between insurance status and curve magnitude in idiopathic scoliosis pediatric patients in mainland China.
Methods:
Medical records of patients with adolescent idiopathic scoliosis in 4 tertiary spine centers across China from January 2013 to December 2017 were analyzed. Data was extracted on insurance status, curve magnitude, recommended treatment at presentation, source of referral, and treatment initiated. Additional information was collected for patients requiring corrective surgery, including time from recommendation for surgery to surgery and clinically relevant parameters such as, postoperative complications, and pre-/postoperative Scoliosis Research Society–22 scores were also collected for patients requiring corrective surgery.
Results:
Of the 1785 patients included, 1032 were Urban Resident Basic Medical Insurance Scheme (URBMS) insured and 753 were New Rural Cooperative Medical Scheme (NRCMS) insured. NRCMS patients presented with a larger major curve than URBMS patients (32.9° ± 15.1° vs 29.3° ± 12.6°, P = .028). For patients having surgery recommended, NRCMS patients presented with a larger mean Cobb angle at the first presentation (57.7° vs 50.9°, P < .0001) and at time of surgery (61.3° vs 52.2°, P < .0001), and experienced a significantly longer time from surgery recommendation to decision for surgery. Complication rates were comparable between the 2 groups, except for pulmonary complications (NRCMS 7.3% vs URBMS 2.8%, P = .04). Postoperatively, patients covered by NRCMS insurance experienced greater overall improvement in health-related quality of life and were less satisfied with the treatments.
Conclusions:
This study shows that health insurance may influence the severity of scoliosis on presentation, with implications on early diagnosis and surgery time.
Keywords
Introduction
The prevalence of adolescent idiopathic scoliosis (AIS) is approximately 3% in the general population, and up to 0.1% of people diagnosed with AIS is at risk of surgery. 1 AIS is a progressive disease. Earlier diagnosis may allow for conservative treatment, such as observation or bracing. For patients requiring surgical correction, the ability to access care earlier could potentially result in shorter operation time, fewer vertebral levels instrumented, and preservation of distal motion segments. 2 It is well documented that economic status affects access to and utilization of medical care, treatment decisions, and patient outcomes. 3 -5
In China, many adolescents with scoliosis are deterred from early diagnosis and referral to a specialist, due to economic status. This affects the progression of the curve, causes adverse health effects such as cardiopulmonary compromise, and increases AIS management complexity. With commercial health insurance underdeveloped, China’s government has reforms in the health care system, facilitating access to health care and protecting residents from impoverishment by illness. Today there are 2 basic health insurance schemes for children, including (1) the New Rural Cooperative Medical Scheme (NRCMS) for children from rural areas and (2) the Urban Resident Basic Medical Insurance Scheme (URBMS) for children from urban areas. 6 Yet the reimbursement rate can be of great difference between these 2 schemes. For patients with URBMS seeking help in a scoliosis specialty center, the scheme would cover more than 80% of their bill. However, for those with NRCMS, the scheme would cover only about 30% or less of the bill.
There is still no consensus on how insurance status impacts on the diagnosis and treatment of AIS. 7,8 To date, no study has addressed this issue in China. In this research, we first quantify the relationship between insurance scheme and the curve magnitude at the first presentation to a surgeon. We then evaluate the impact of the 2 different insurance schemes on surgical waiting times, hospitalizations, and health-related quality of life of patients treated with posterior spinal instrumentation and fusion. We hypothesized that patients with NRCMS have limited access to healthcare and therefore would present with larger curves, and the improvement in health-related quality of life would be lower in patients with URBMS.
Materials and Methods
We retrospectively reviewed the medical records of AIS patients in 4 tertiary spine centers across China from January 2013 to December 2017.
Inclusion criteria were (1) age 10 to 18 years at the time of diagnosis of idiopathic scoliosis and (2) first visit to the spine specialty center due to scoliosis. Patients were excluded from the study if they had received prior treatment (bracing or surgery), or they were diagnosed with congenital, neuromuscular, or syndromic scoliosis. Treatment strategy of AIS was based on curve magnitude and Risser sign. Observation was recommended for patients with mild curves of less than 25° and patients with curves over 25° who had reached skeletal maturity. Bracing was recommended for patients with Risser 0 to 2 and curves 25° to 40°. Surgery was considered for patients with curve reaching 50° or curves between 40° and 50°, for patients with skeletal immaturity. Data extracted from medical records included age at presentation, sex, menarche status for girls, insurance type, and treatment recommendations at the first visit. Radiographic data was also collected, including curve magnitude, levels involved, and Risser stage. For patients underdoing posterior spinal fusion, time from recommendation for surgery to decision for surgery, length of stay, implant density, patient-reported Scoliosis Research Society–22 instrument (SRS-22) score 9 at baseline and 1-year follow-up, and information on adverse events were collected. The study received approval from the institutional review board and was registered with the Chinese Clinical Trial Registry (Protocol ChiCTR1800018687).
Results
A total of 1785 consecutive patients newly diagnosed with AIS were identified between January 2015 and December 2017. A total of 1032 patients (57.8%) were URBMS insured and 753 patients (42.2%) were NRCMS insured. There was no difference in terms of age, gender distribution, and geographic region (Table 1). At the time of presentation, patients with NRCMS insurance presented with a larger major curve than those with URBMS (P = .028). URBMS insured patients were significantly more likely to complete the recommended follow-up (65.2% vs 59.4%, P = .012).
Characteristics of Patients With Adolescent Idiopathic Scoliosis by Insurance Type.
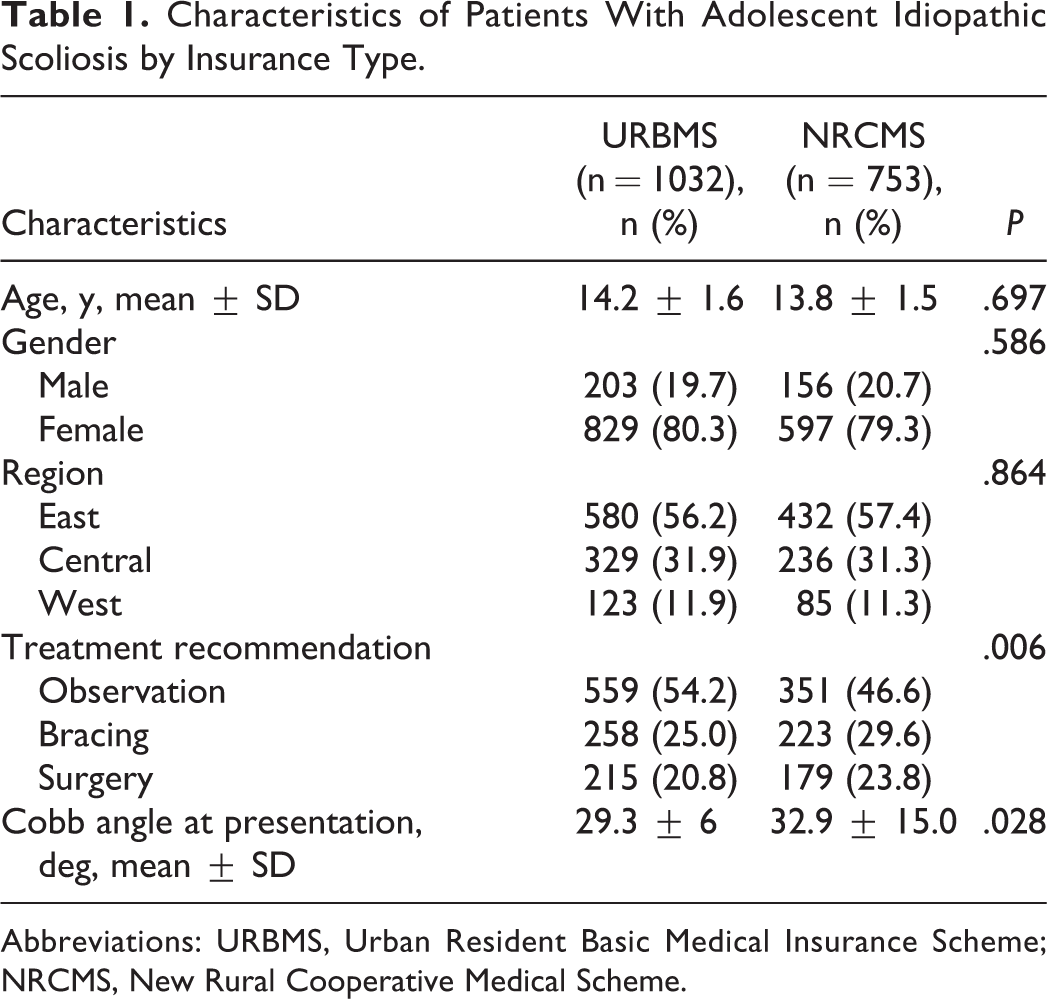
Abbreviations: URBMS, Urban Resident Basic Medical Insurance Scheme; NRCMS, New Rural Cooperative Medical Scheme.
There was a significant difference between the 2 groups regarding the overall treatment recommendations. For patients with observation recommended, mean major Cobb angles were similar between the 2 groups (20.9 ± 2.4 for NRCMS and 20.1 ± 2.6 for URBMS, P = .051). For patients with bracing recommended, mean Cobb angle was 31.7° for the URBMS group and 32.6° for the NRCMS group (P = .393). For patients with surgery recommended, mean curve was 50.9° for the URBMS group and 57.7° for the NRCMS group (P < .0001) (Table 2). At time of surgery, mean Cobb angles were 52.2° and 61.4° for the URBMS and NRCMS groups, respectively (P < .0001). There was a significantly statistical difference (P = .012) in mean time from surgery recommendation to decision for surgery, 60.6 ± 36.9 and 86.6 ± 42.7 days for the URBMS and NRCMS groups, respectively. Implant density (1.83 ± 0.15 for URBMS, and 1.82 ± 0.14 for NRCMS) and mean length of hospital stay (P = .48) were similar between groups. Our analysis showed that postoperative complication rates were similar between the 2 groups except for the development of pulmonary complications (NRCMS 7.3% vs URBMS 2.8%, P = .04). Patients with NRCMS had worse preoperative SRS-22 scores in Pain and Appearance domains and in the SRS-22 total score (Table 3). Preoperative SRS-22 scores in Mental and Activity domains were higher in URBMS group, but the differences were not statistically significant. NRCMS patients had greater improvements in SRS-22 Total and all domain scores compared with URBMS patients. SRS-22 scores at 1-year follow-up were similar in Total score, Mental, and Activity domains between the 2 groups. NRCMS patients had worse Appearance, Pain, and Satisfaction domain scores. Factors influencing the decision making on surgery are summarized in Figure 1. The 2 most frequently cited factors were economic instability (61%) and neurologic deficit (42%) in the NRCMS group, while neurologic deficit (48%) was the biggest concern about surgery in the URBMS group.
Characteristics of Patients With Adolescent Idiopathic Scoliosis Treated With Posterior Spinal Fusion by Insurance Type.
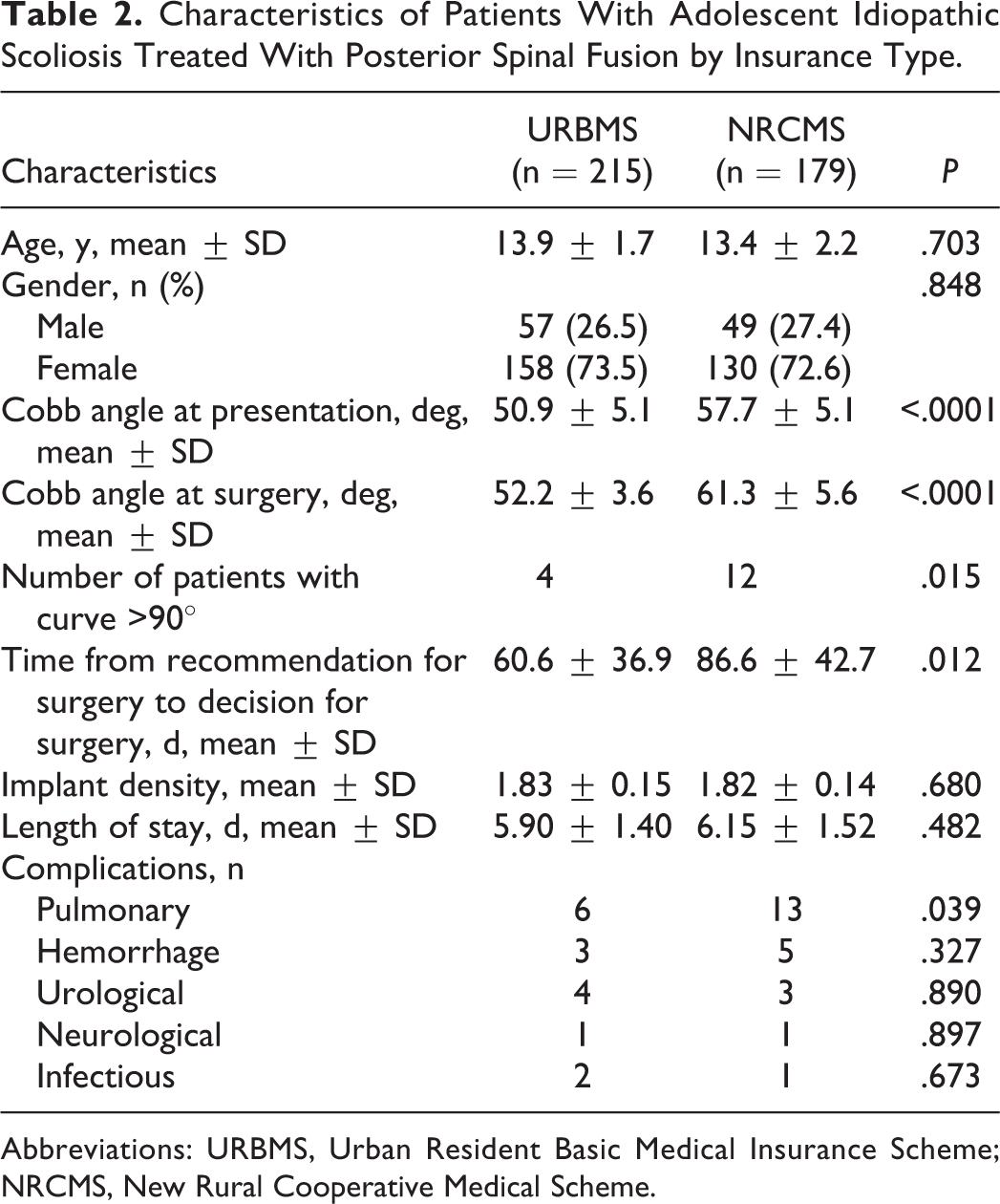
Abbreviations: URBMS, Urban Resident Basic Medical Insurance Scheme; NRCMS, New Rural Cooperative Medical Scheme.
Scoliosis Research Society–22 Scores of Patients Treated With Posterior Spinal Fusion by Insurance Type.
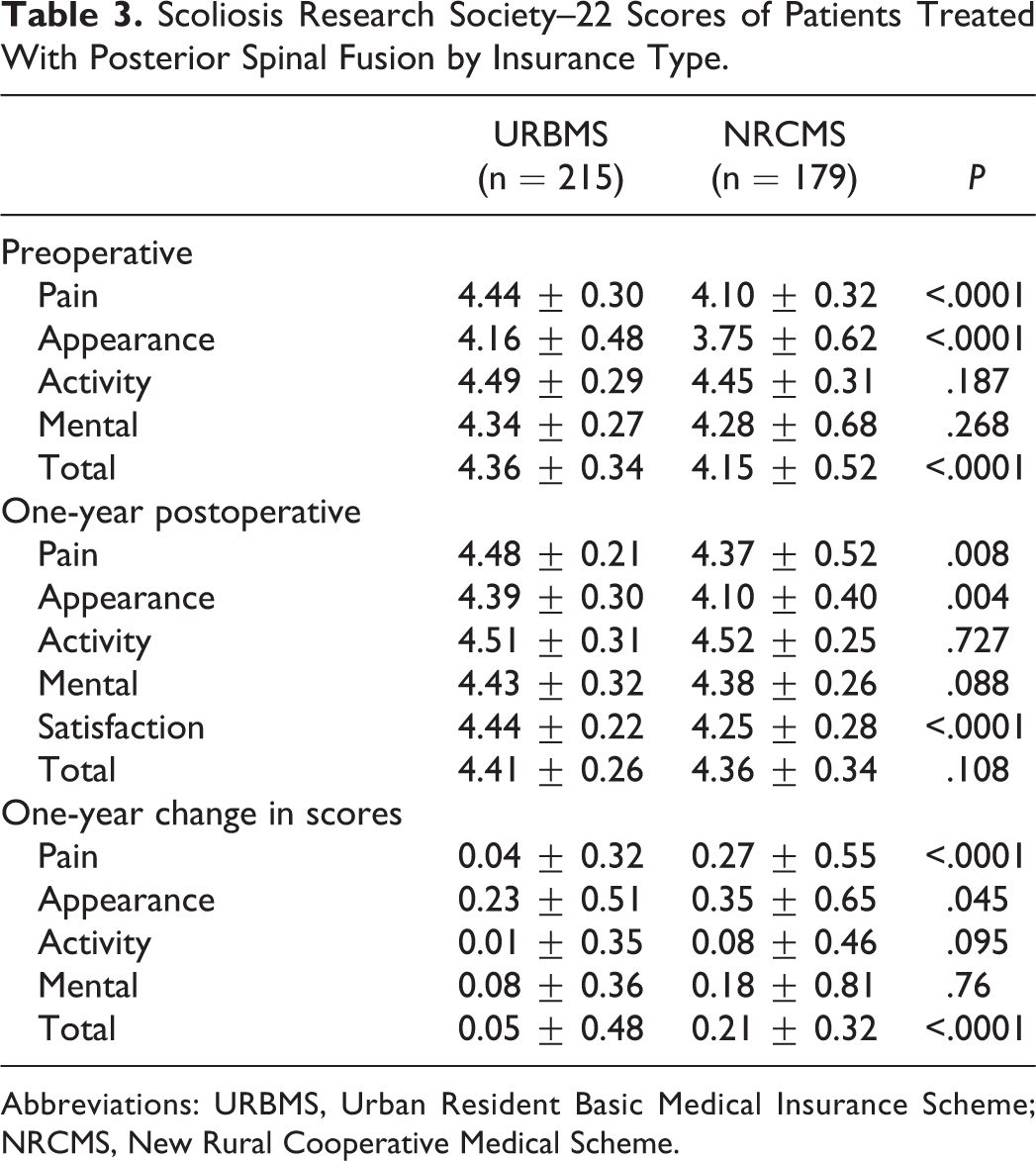
Abbreviations: URBMS, Urban Resident Basic Medical Insurance Scheme; NRCMS, New Rural Cooperative Medical Scheme.
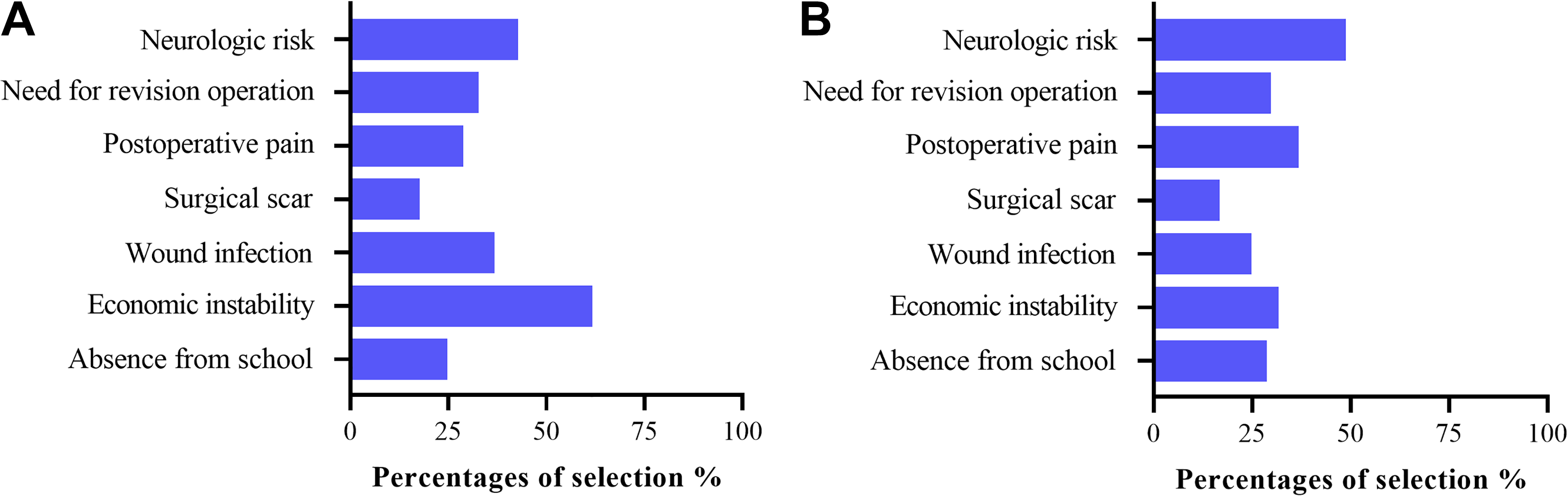
Factors influencing decision on corrective surgery for adolescent idiopathic scoliosis (data obtained from interview of patients’ guardians using a standardized questionnaire). (A) New Rural Cooperative Medical Scheme (NRCMS) group and (B) for Urban Resident Basic Medical Insurance Scheme (URBMS) group.
Discussion
To our knowledge, this is the first study to examine the association between health insurance coverage and curve magnitude of patients with AIS in mainland China. Insurance status has been identified as one of major factors affecting the access to health care for patients. Scoliosis, requiring frequent follow-up or eventual surgery, may lead to significant financial burdens to the patients and their family. Several studies conducted in the United States revealed insurance status was related to waiting times in obtain appropriate treatment, 10 curve magnitudes at presentation, 11 and postoperative outcomes. 12,13
The health insurance system is completely different in China. Since 2009, comprehensive health care reforms have been initiated, including the establishment of basic medical insurance schemes for adolescents and children. The basic medical insurance schemes include the URBMS for urban residents and NRCMS for rural residents.
Our results suggest that insurance status, as a proxy for socioeconomic status, may influence the severity of scoliosis on presentation. NRCMS insured scoliosis patients face significantly greater barriers in access to health care. The mean Cobb angles of major curves were higher in the NRCMS group. More patients in the NRCMS group required bracing or surgery treatment. Both mean Cobb angles and ratio of patients requiring surgery were higher in the present study than in the study by Goldstein et a 7 performed in the United States. One explanation is the prevalence of school screening programs for scoliosis in their area, while they are inexistent in China. The US Preventive Services Task Force changed its grade for the scoliosis screening program from a “D” (discourage the use of screening programs) to an “I” (uncertainty about the balance of benefits and harms of the service) in the latest recommendation statement. 14 No publications included in the task force evaluated the benefits of screening for AIS on severity of curvature compared with no screening. Thomas et al 15 compared the curve magnitude at initial presentation for evaluation of scoliosis for new patients between 1994-2004 (during school screening) and 2004-2014 (after school screening) and found that after school screening was discontinued, mean curve magnitude at presentation statistically increased. Consistent with their results, our study and that by Goldstein et al 7 collectively imply the importance of scoliosis screening for early curves detection.
In this study, we also focused on patients who required surgical intervention, evaluating the potential effects of insurance status on curve magnitudes and surgical outcomes. Fletcher et al 11 reviewed 135 AIS patients treated with posterior spinal fusion and found that insurance status had an impact on presenting Cobb angles and Cobb angles at time of surgery. Our data suggests a 7° difference in presenting curves between patients with URBMS and with NRCMS. The difference increased to 9° at the time of surgery. NRCMS-insured patients experienced a much longer time from recommendation for surgery to decision for surgery. Ahn et al 16 found that a prolonged wait for surgery increased the risk of additional surgery compared with the original plan at the time that surgery was first indicated. Our study did not suggest any difference between insurance groups in clinically relevant parameters such as fusion levels and hospitalization duration. As all surgical procedures in our study were scheduled on a first-come first-served basis without preference for insurance status, we surveyed the patients’ guardians for factors influencing their decision making on surgery and found that economic instability was the most frequently cited factor in the NRCMS group, while neurologic deficit was the biggest concern about the surgery in the URBMS group.
Several reports have demonstrated insurance status is related to postoperative outcomes. 13,17 -20 In our research, NRCMS-insured patients demonstrated inferior preoperative domain scores across pain and appearance domains. Postoperatively, patients covered by NRCMS experienced greater overall improvement in health-related quality of life and were less satisfied with the treatments. We did not find any significant difference in complication rates, except for pulmonary complications. This may be partially explained by more severe scoliosis (Cobb angle >90°) patients with preoperatively compromised pulmonary function in the NRCMS group than in the URBMS group.
The differences between URBMS and NRCMS groups reflect the fact that although the launch of new medical insurance schemes in China has improved access to health care, inequality in health care utilization remains a serious social problem. According to the data of National Bureau of Statistics of China, by 2016, health care expenditures per capita was 1630.8 CNY for urban residents, but only 929.2 CNY for rural residents. 21 It is worth noting that health insurance in rural and urban areas may affect health inequalities. Sun et al 22 found that the NRCMS had limited effects on reducing household health spending. Similar findings were reported by Yu et al. 23 A major reason was the lower reimbursement rates for NRCMS compared with URBMS. Li et al 24 explored the influence of medical insurance policy on the regular prophylaxis treatment in Chinese children with severe hemophilia A and found groups receiving higher reimbursement proportion were more likely to have higher medication consumption. Similarly occurs for corrective surgery, which costs have increased substantially with the application of advanced technology such as pedicle screw constructs, blood salvage techniques, and intraoperative cord monitoring. 25 Unlike fractures requiring emergent attention, AIS is an essentially asymptomatic condition and can be treated surgically on an elective basis. Some patients experienced a long waiting time before surgery, during which they found ways to raise enough money for the surgery. Some patients even refused the doctors’ recommendation for surgery due to economic reasons.
There are several design limitations in our study. First, this study was retrospectively designed. However, the results encourage further hypothesis-driven prospective data analysis. Second, as commercial health insurance is underdeveloped in China and public medical insurance covers over 95% of the total population, we could not compare the quality of health care between public and private insurances due to the small sample size. Third, there might be other potential factors affecting the access to health care, such as few charity assistances projects that occasionally assist in the treatment of scoliosis for children from underprivileged families, which we were unable to evaluate. Finally, all centers from this study were located in economically developed areas, in which the medical insurance policies and personal income are relatively superior. Therefore, our results may not represent country wide status.
In conclusion, despite its design limitations, this study shows differences between NRCMS and URBMS insured patients. It also points out the potential benefits of improved medical insurance for children with AIS in China, especially for those living in rural areas. Given the outstanding progress of the health care reform in China, it would be necessary to implement a more comprehensive insurance package to effectively target the rural residents with better financial protection.
Footnotes
Acknowledgments
The authors thank Ms Huixian Jiang and Hong Qin at the Center of Spinal Surgery, Department of Orthopedics, Shanghai Changzheng Hospital, Shanghai, for statistical consultation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.