
Abstract
Study Design:
Systematic literature review with meta-analysis.
Objective:
Osteoporosis is common in elderly patients, who frequently suffer from spinal fractures or degenerative diseases and often require surgical treatment with spinal instrumentation. Diminished bone quality impairs primary screw purchase, which may lead to loosening and its sequelae, in the worst case, revision surgery. Information about the incidence of spinal instrumentation-related complications in osteoporotic patients is currently limited to individual reports. We conducted a systematic literature review with the aim of quantifying the incidence of screw loosening in osteoporotic spines.
Methods:
Publications on spinal instrumentation of osteoporotic patients reporting screw-related complications were identified in 3 databases. Data on screw loosening and other local complications was collected. Pooled risks of experiencing such complications were estimated with random effects models. Risk of bias in the individual studies was assessed with an adapted McHarm Scale.
Results:
From 1831 initial matches, 32 were eligible and 19 reported screw loosening rates. Studies were heterogeneous concerning procedures performed and risk of bias. Screw loosening incidences were variable with a pooled risk of 22.5% (95% CI 10.8%-36.6%, 95% prediction interval [PI] 0%-81.2%) in reports on nonaugmented screws and 2.2% (95% CI 0.0%-7.2%, 95% PI 0%-25.1%) in reports on augmented screws.
Conclusions:
The findings of this meta-analysis suggest that screw loosening incidences may be considerably higher in osteoporotic spines than with normal bone mineral density. Screw augmentation may reduce loosening rates; however, this requires confirmation through clinical studies. Standardized reporting of prespecified complications should be enforced by publishers.
Keywords
Introduction
Osteoporosis is a common condition in patients of advanced age, especially in women. The most recent comprehensive report on osteoporosis in the European Union describes it as “characterized by reduced bone mass and disruption of bone microarchitecture, resulting in increased bone fragility and increased fracture risk. […] Approximately 6% of men and 21% of women aged 50-84 years have osteoporosis affecting 27.6 million people in the EU in 2010.” 1
Similar figures are reported from the US, with estimates of 15% of women and 4% of men aged 50 years and older having osteoporosis in 2010, affecting a total of 10.2 million people. 2 Because of the general aging of the population, the number of people affected by osteoporosis is expected to rise further. The United Nations’ current report on World Population Prospects states “In Europe, 25% of the population is already aged 60 years or over and that proportion is projected to reach 35% in 2050, while in Northern America it will go from 22 to 28%.” 3
The most important consequence of osteoporosis is an increased risk of fractures, resulting in more than 8.9 million fractures annually worldwide. 1 In instrumented spinal surgery, a decreased bone mineral density (BMD) may also lead to impaired screw fixation. Various biomechanical studies have demonstrated the association of pullout strength, cutout torque and maximum insertional torque with BMD. 4 -8 From a clinical perspective, osteoporosis has been shown to be a significant risk factor for revision surgery 9 and for proximal junctional failure 10 following adult spinal deformity surgery.
Numerous attempts have been made to overcome problems with screw fixation in compromised bone quality. These include modified implant designs such as conical screws, special thread geometries, expandable screws, cross-linked constructs, and screw coatings. 11 -13 Alternatively, the surgical technique can be modified. This entails undertapping of screws, the use of alternative screw trajectories such as the cortical bone pedicle screw, accepting a lesser degree of correction, taking special care of where to end the construct, as well as screw augmentation with poly(methyl methacrylate) (PMMA) or more recently calcium phosphate (CaP) cement. 11,12,14 -17 For elective procedures, antiresorptive medical treatment initiated well before the procedure may also be an option, 18 even though this is not commonly done.
Unfortunately, clinical studies specifically dealing with problems of spinal instrumentation in osteoporotic patients are scarce, so getting a clear picture on the true incidence of screw-related problems is challenging. The reasons for this are 2-fold: First, the osteoporosis status is seldomly reported. Second, many publications focus on clinical results and do not provide any information on screw loosening or would even not report screw loosening as a complication as long as it has no clinical consequences. The absence of reliable information and well-established reporting standards for complications following spinal surgery adds to the difficulty of interpreting individual studies, so a comprehensive overview is warranted.
The primary objective of this analysis was to determine the incidence of pedicle screw loosening in osteoporotic patients treated surgically for degenerative conditions or osteoporotic fractures. The secondary objectives were to determine the incidences of further local complications, including implant-related complications, subsequent vertebral fractures, infections, neurological complications, as well as reoperations and fusion rates.
Materials and Methods
Search Strategy
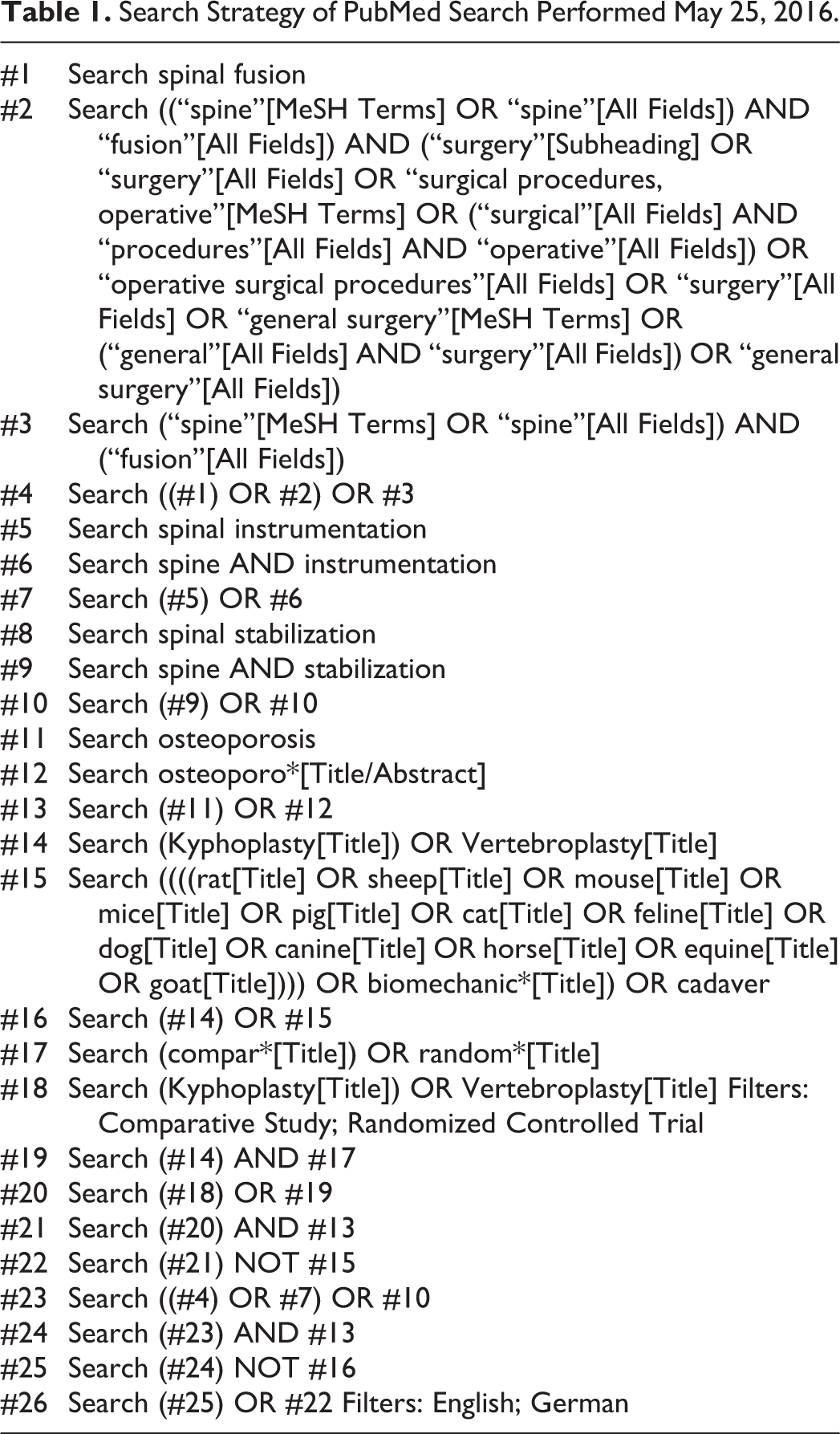
A literature search was performed in PubMed, the Web of Science (Core Collection), and the Cochrane databases on May 25th, 2016. The search strategy used for the PubMed Search is presented in Table 1. Comparable strategies were used in the other databases.
Search Strategy of PubMed Search Performed May 25, 2016.
Study Selection
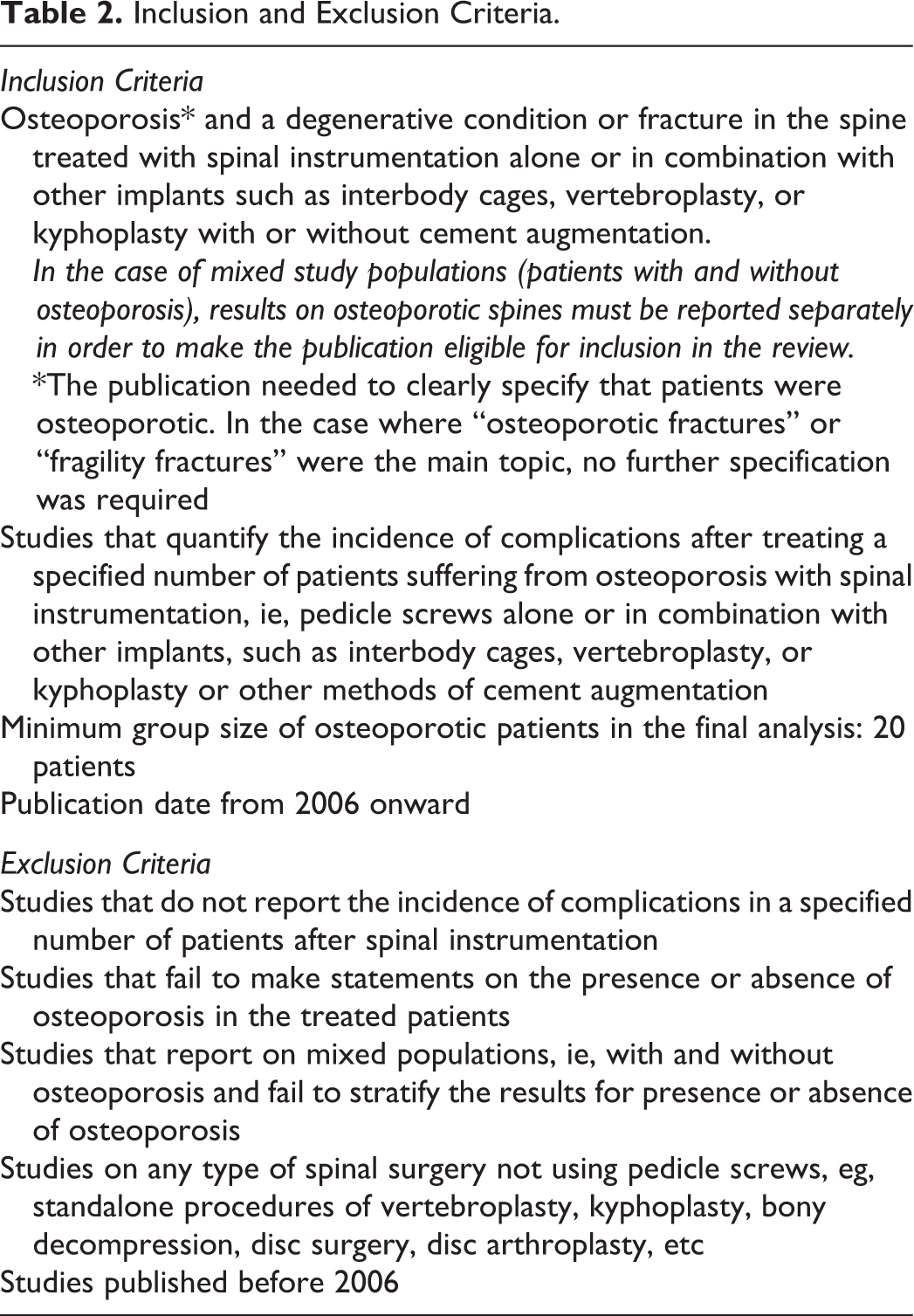
Publications were deemed eligible if they reported on complications of spinal instrumentation in osteoporotic patients who had been operated upon for fractures or degenerative conditions and included at least 20 patients. Further inclusion and exclusion criteria for study selection are described in Table 2. Titles and abstracts of the initial matches were independently screened by 2 reviewers to identify potentially eligible primary studies. In cases where the title or abstract did not allow determination of eligibility, the full text was reviewed in order to make a valid decision. In case of discrepancies, consensus was sought through peer discussion and in case of doubt, a third reviewer was consulted. Additionally, the references of reviews and meta-analyses identified in the search were screened for further potentially eligible primary studies. The eligible studies were further checked for overlapping study populations based on the description of recruitment time, indication, and research location. In case of overlapping study populations, the publication that provided more information on complications was included.
Inclusion and Exclusion Criteria.
Data Extraction
Information was collected on a standardized data extraction form and included the inclusion and exclusion criteria for the study population of the respective study, demographic and spinal disease characteristics, treatment details, complications, and whether implant-related complications and their definitions were specified in the methods section. The categorization of complications was adapted from Audigé et al 19 as presented in Table 3.
Categorization of Complications.a
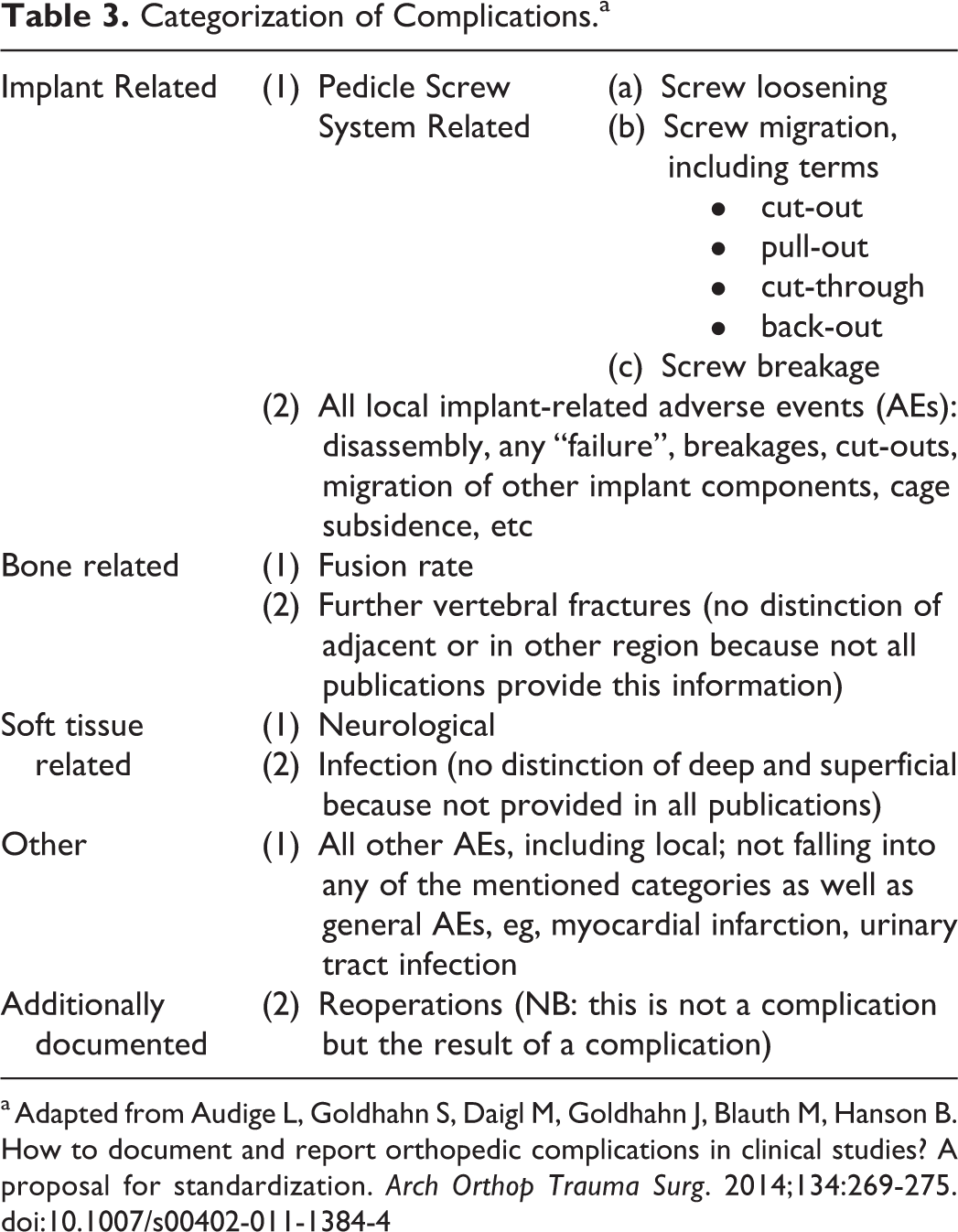
a Adapted from Audige L, Goldhahn S, Daigl M, Goldhahn J, Blauth M, Hanson B. How to document and report orthopedic complications in clinical studies? A proposal for standardization. Arch Orthop Trauma Surg. 2014;134:269-275. doi:10.1007/s00402-011-1384-4
For publications presenting results of several subgroups, only data of the subgroups that complied with our eligibility criteria concerning osteoporosis, indications, and treatment were captured. Data included in the quantitative assessment was extracted independently by 2 reviewers.
In case of missing or irreproducible information in the parameters of interest, authors of the respective publications were contacted and requested to provide the missing information.
Data Synthesis
A quantitative analysis of complications, reoperations, and fusion rates was performed separately for augmented and nonaugmented screws. This was done because cement augmentation was suspected to have a significant effect on our target outcome and thus could have acted as a confounder. Screws were regarded as augmented when any kind of cement (eg, PMMA or CaP) had been applied around the screws or parts of the screws so that it interfaced directly with the metal.
Since a first inspection of the forest plots showed no substantial differences in the results depending on the pathologies treated, no analysis stratified for pathology was performed.
The majority of eligible studies reported results of more than one study group, which were based on different treatment regimens and/or different baseline characteristics, therefore these individual groups were always analyzed as separate groups. Consequently, in the quantitative analysis, the number of included groups exceeds the number of included studies.
The absolute risks of experiencing local complications such as (a) screw loosening, (b) screw breakage, or (c) screw migration (including cutout/pullout), (d) further vertebral fractures, (e) infections, (f) neurological complications, (g) reoperations, as well as (h) fusion rates were calculated for each of the study groups within each study and synthesized. Figures that were not reported on a patient level or that were irreproducible were excluded from the quantitative analysis.
Whenever screw-related parameters were not clearly documented in the primary studies, they were not included in the calculation unless parameters of lesser severity were unambiguously documented. We then assumed that more severe parameters would have been stated had they occurred. We applied the following hierarchy of severity: screw loosening < screw migration < screw breakage/other implant breakage or disassembly. In other words, if the incidence of screw migration was documented but no statement about screw breakage was made, we assumed that no screw breakage occurred. On the other hand, if no statements about screw loosening or migration were made, we did not make any assumptions for the incidence of screw breakage and excluded the respective publication from the quantitative analysis of screw breakage.
For parameters that leave room for interpretation, that is, screw loosening and fusion, we assumed that reporting would be stricter in the presence of clear definitions. Therefore, we performed a sensitivity analysis excluding all studies that had not given a clear definition of the respective parameter. Additionally, based on the high heterogeneity of results for screw loosening, a second sensitivity analysis was performed where outliers were excluded. This was done by screening the groups in the analysis for extreme results and then excluding the respective publication from the analysis based on the assumption of a nonrepresentative patient population.
Statistical analyses were performed using STATA version 14 (STATA Corp, College Station, TX, USA). The incidences from different studies and different treatment groups were pooled using the metaprop command, which has been developed to pool proportions. 20 The Freeman-Tukey double arcsine transformation was used to stabilize the variances and the transformed estimates were pooled using weights derived from a random effects model (DerSimonian-Laird method). As it was expected that augmentation would influence the outcomes, results were pooled separately for patients treated with and without screw augmentation. Heterogeneity was assessed using I 2 statistics and Cochran’s Q test with a P value <.1 considered indicative for heterogeneity, that is, the variation of the respective outcome that can be explained by the variation of the true underlying risks in contrast to the variation caused by sampling error. Usually, an I 2 value ≥50% signifies moderate heterogeneity whereas a value ≥75% signifies high heterogeneity. 21 Additionally, we calculated 95% prediction intervals (PIs) because this has been suggested as a more concise measure for heterogeneity than I 2 in the recent statistical literature. 22 The 95% PI provides an estimate of where the incidence from 95% of similar trials would fall under the assumption that the between-study variability within the included trials also holds for new trials.
Risk of Bias Assessment
The assessment of risk of bias in individual studies focused solely on our outcomes of interest and was based on the McMaster Quality Assessment Scale of Harms for primary studies (McHarm Scale). 23 The McHarm Scale was developed from quality rating items generated by a review of the literature on harms and from previous quality assessment instruments. 23 We selected and adapted elements based on their relevance to implant-related complications as depicted in Table 7 (Supplementary Material).
To determine the risk of bias across studies, papers were assessed regarding the extent of missing information for each of the documented parameters. 24
Ethical Aspects
The protocol of this meta-analysis was registered at PROSPERO with the number CRD42016046958. No institutional review board approval is needed for systematic literature reviews and meta-analyses.
Results
Eligible Literature
The searches in PubMed, the Web of Science and the Cochrane databases resulted in a total of 1831 matches (Figure 1).
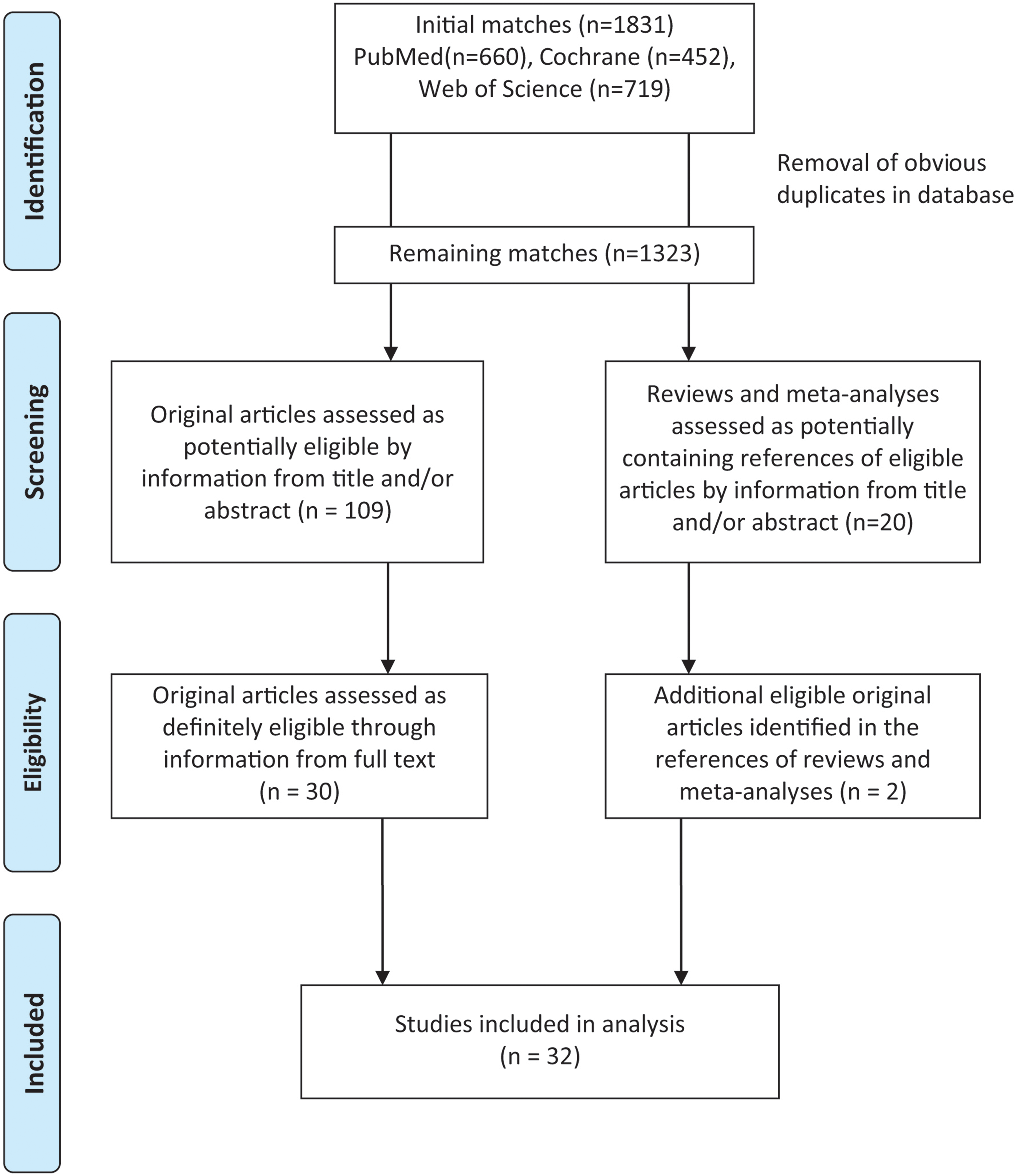
Study inclusion flow diagram.
After removal of obvious duplicate publications in the literature database, 2 reviewers independently screened titles and abstracts and identified 109 primary studies and 20 reviews and meta-analyses as potentially relevant. Two complete studies were excluded due to overlapping study populations 25,26 and 1 of 2 subgroups of a publication 27 was excluded from the quantitative analysis because it substantially overlapped with the population of another study included in this review. 28 Full text assessment of the primary studies and reference checking of review articles identified 32 eligible primary studies that reported on 1518 osteoporotic patients treated with spinal instrumentation. The major reason for exclusion after full text screening was the absence of information on the osteoporosis status.
In 7 studies, screws were augmented, 29 -35 in 21 studies, screws were nonaugmented, 27,28,36 -54 and 4 studies compared outcomes of augmented versus nonaugmented screws. 55 -58 Indications, that is, degenerative disease or fracture, were equally distributed in the studies on augmented and nonaugmented screws (Table 4). In addition to the fusion with posterior instrumentation, vertebroplasty was performed in 12 studies and/or interbody fusion in 14 studies.
Distribution of Indications According to Implantation Technique.
Only 4 of the eligible studies were randomized controlled trials. Of these, 3 analyzed the effect of different anti-osteoporotic drugs on the outcome after spinal fusion procedures 37,46,48 and 1 study compared the effect of expandable and conventional screws on screw loosening and clinical outcomes. 54
Overall, studies presented a high heterogeneity regarding their study population, interventions performed, and the degree of detail in which complications were reported. A summary of study characteristics with focus on baseline parameters is given in Table 8 (Supplementary Material) and with focus on screw-related complications, fusion rates, and subsequent fractures in Table 5.
Study Characteristics: Implant-Related Complications, Further Fractures, and Fusion Rates.
Abbreviations: nd, not documented, pt, patient; pts: patients; CPC, calcium phosphate cement; CT, computed tomography; N/A, not applicable; PMMA, poly(methyl methacrylate); RCT, randomized controlled trial; SSF, short segment fixation; VB, vertebral body; VCR, vertebral column resection; VF, vertebral fracture.
Outcomes
Information about screw loosening rates was provided in 19 publications, 16 of these studies reported loosening rates per patient. Thirteen publications provided information about screw cutout/pullout or migration, while explicit statements about screw breakage rates were made in only 7 studies. The rates of screw-related complications other than loosening were always given per patient. Fusion rates were presented in 21 publications, 20 of these presented data per patient. Information on the number of patients suffering from subsequent vertebral fractures, infections, neurological complications, or requiring a reoperation was provided in 18, 16, 15, and 15 publications, respectively. Three studies reported adjacent segment 39,44 or disc degeneration, 33 and only 1 study reported the kyphosis angle proximal to the index level. 41 Since not a single study reported complete information on all the parameters of interest, we attempted to contact all authors to request further information. A total of 4 authors responded to our mails but only 3 were able to provide additional information.
Eighteen studies reported results stratified for different treatment regimens and/or different diagnoses. 27,32,37,38,42,44 -48,52 -59 The respective study groups were analyzed separately in the quantitative analysis (total number of study groups = 49), and the number of included study groups ranged from 5 to 31, depending on the variable of interest (Table 6).
Pooled Incidence Estimates for Complications, Reoperations, and Fusion Rates (Random Effects Model).
Abbreviations: CI, confidence interval; PI, prediction interval.
a I 2 is a measure of heterogeneity, that is, the proportion of the observed variance that reflects true variation in risks for the respective complication.
b P value refers to test of heterogeneity and was determined by Cochran’s Q test.
c “Migration” includes reports of “cutout,” “pullout,” “cut-through,” and “back-out.”
The pooled incidence estimates for complications, reoperations and fusion rates are shown in Table 6, which also denotes the number of study groups as well as articles included in the respective analysis, and the corresponding number of patients. For a third of the parameters, I 2 was ≥75% indicating high heterogeneity. 21 This high level of heterogeneity is also reflected in the extremely wide PIs of the pooled results. The 95% PI describes the range in which the incidences of 95% of similar trials is expected to lie, whereas the 95% CI describes the range in which the true (pooled) mean is expected to lie.
Heterogeneity slightly decreased in the analysis of screw loosening after removing outliers, but remained significant. In the sensitivity analyses of loosening and fusion, which only included studies that clearly defined how the respective parameters were determined, no decrease of heterogeneity was seen compared with the analysis comprising all eligible studies. Of the 19 publications that reported screw loosening rates, only 10 defined loosening. However, no uniform definition was used. Some studies defined any type of “clear zone” in the implant’s surroundings as loosening, while others defined “radiolucent zones,” “radiolucent lines,” “radiolucent lines of ≥1 mm at the screw-bone interface.” Another 2 publications stated that loosening was evaluated on CT, albeit without being more specific. Likewise, only 12 of the 21 publications that reported fusion rates described the exact parameters used to evaluate fusion.
Several of the analyzed parameters showed a trend to be more favorable in publications on augmented screws than in publications on nonaugmented screws (Table 6).
This was most pronounced in the pooled risk of screw loosening, which was 22.5% (95% CI 10.8%-36.6%, 95% PI 0.0%-81.2%) in publications on nonaugmented screws and 2.2% (95% CI 0.0%-7.2%, 95% PI 0.0%-25.1%) in publications on augmented screws (Figure 2).
Forest plot of risk of screw loosening.
These pooled results are not based on comparative studies but on individual studies conducted independently from each other, which precludes a direct comparison of the results.
The incidences of several other variables were similar in publications on augmented and nonaugmented screws. For instance, the pooled risk of reoperation was 5.3% (95% CI 1.5%-10.6%, 95% PI 0.0%-32.0%) in publications on nonaugmented screws and 3.9% (95% CI 0.0%-12.4%, 95% PI 0.0%-39.6%) in publications on augmented screws (Figure 3). The pooled risk of further vertebral fractures was 8.4% (95% CI 3.3%-15.0%, 95% PI 0.0%-41.7%) in publications on nonaugmented screws and 6.5% (95% CI 0.4%-17.1%, 95% PI 0.0%-52.4%) in publications on augmented screws (Figure 4).
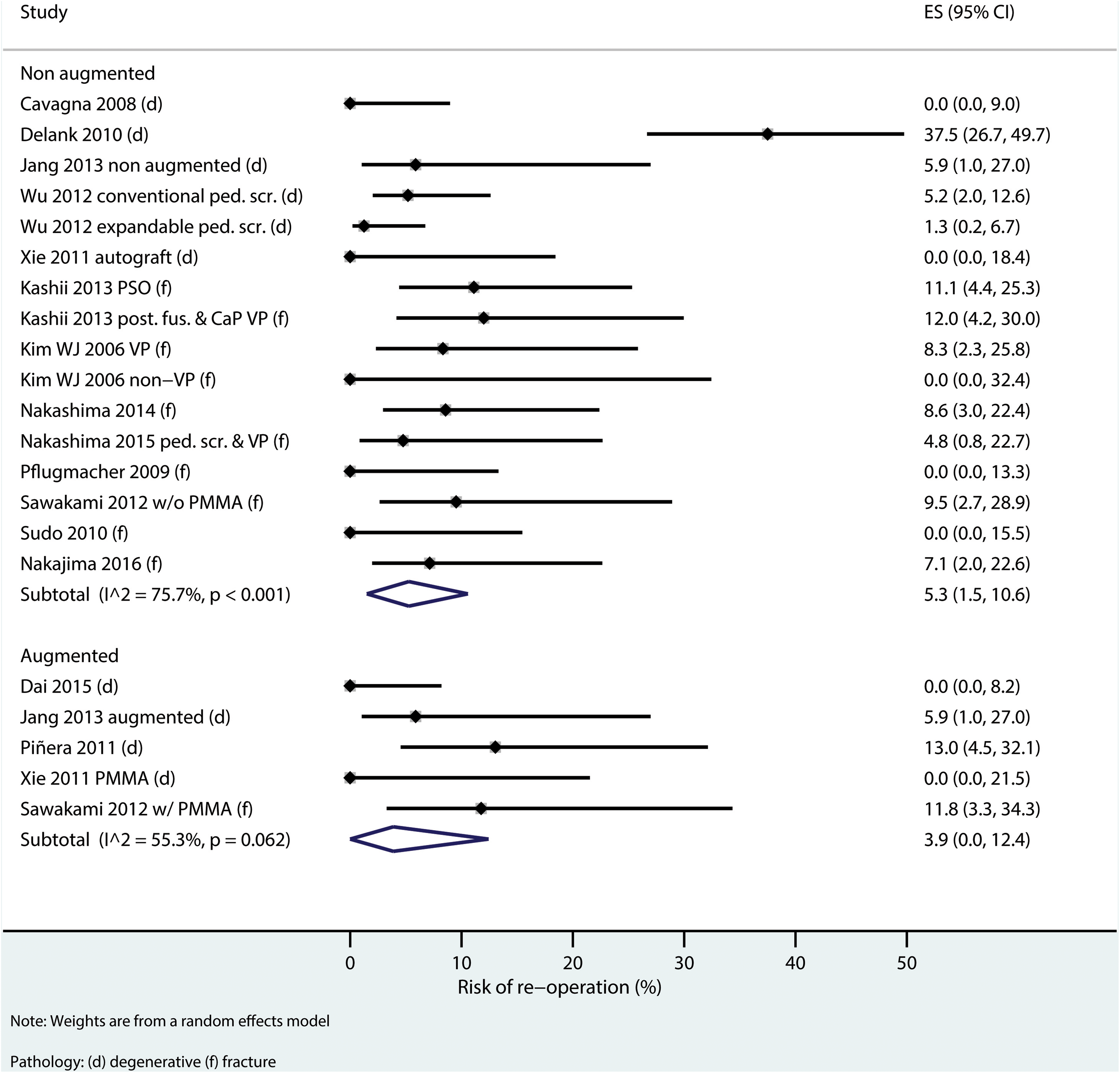
Forest plot of risk of reoperation.
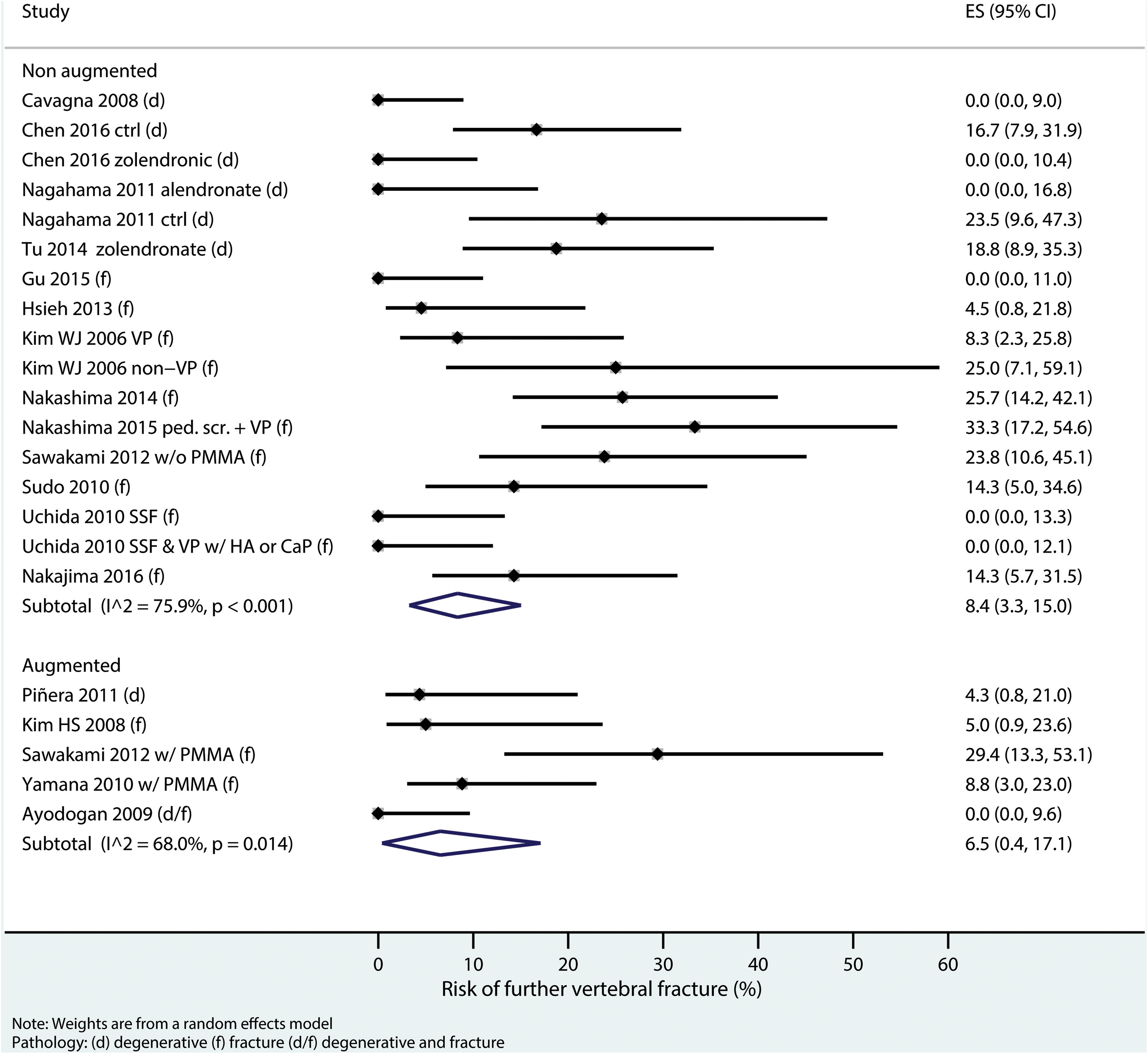
Forest plot of risk of further vertebral fracture.
Details on the complications of interest, including those that could not be pooled because they were reported too rarely or not on a patient level, are presented in Table 5 and Table 10 (Supplementary Material).
Risk of Bias Assessment
The risk of bias assessment done according to an adapted McHarm Scale customized for implant-related complications is shown in Table 9 (Supplementary Material). Of the 32 studies included in this review, 24 reported the number of specific implant-related complications for each study group separately (item 9). Twelve publications clearly specified the number of reoperations for each study group (item 2). Fourteen publications prespecified in the methods section which complications would be collected (items 3 and 4), but only 6 predefined implant-related complications using standardized or precise definitions (item 1).
Risk of bias across studies was determined by assessing the extent of missing information. Most studies did not report all of the complications we would have liked to analyze. The different number of study groups that were included in the respective quantitative analysis as shown in Table 6 indicates the degree of missing information for each outcome.
Discussion
The primary objective of this analysis was to determine the incidence of pedicle screw loosening reported for osteoporotic patients.
The pooled risk of screw loosening for nonaugmented screws in our analysis was 22.5% (95% CI 10.8%-36.6%), with a 95% PI of 0.0%-81.2% and I 2 of 90.4%. For augmented screws, the pooled risk was 2.2% (95% CI 0.0%-7.2%), with a 95% PI of 0.0%-25.1% and I 2 of 73.4%. On the other hand, the pooled risks for subsequent vertebral fractures were similar in augmented and nonaugmented screws with reported values of 6.5% (95% CI 0.4%-17.1%; 95% PI of 0.0%-52.4%, I 2 of 75.9%) and 8.4% (95% CI 3.3%-15.0%; 95% PI of 0.0%-41.7%, I 2 of 68.0%) respectively.
Notwithstanding, and beyond the high heterogeneity alone, given the noncomparative nature of most of the studies included, no scientifically valid comparison statement on how the different procedures compare with each other can be made as this would require prospective comparative studies.
Even though it was beyond the scope of this work to formally compare screw loosening rates in osteoporotic patients to patients with normal bone density, our results suggest that pedicle screw loosening rates may be twice as high as in patients with uncompromised bone quality, at least if screws are implanted in a nonaugmented fashion. However, the highly variable rates provide a low level of clinical evidence, even though this is in line with reports on non-osteoporotic patients in which screw loosening rates range between 0% and 20%, with most studies reporting less than 10%. 60 -67
The high variability of results both in our analysis and in the literature on non-osteoporotic patients can be explained by several reasons. First, most studies reporting on elderly populations have typically used age as an inclusion criterion and do not include a proper assessment of the patients’ BMD. This most likely results in study populations that contain a mixture of osteoporotic and non-osteoporotic patients, which increases their heterogeneity. Second, a wide range of treatment modalities is available for the conditions eligible for our review. Including all these treatment options may be another reason for the diverse results, in particular for observational studies. The same mechanism takes effect with the wide range of indications included in our review. Third, the focus of the publications was usually clinical outcome and not complications. Therefore, the quality of complication reporting is hampered by a lack of operational definitions and of standardized methods of data collection, as well as inconsistent recording and reporting. For instance, only 10 of 19 publications provided an unequivocal definition of screw loosening and the definitions varied slightly amongst the individual studies. Consequently, a given screw could have in theory been rated as loose in one study but rated as firm in another study.
All the above reasons result in a high heterogeneity and make proper comparisons amongst studies challenging if not impossible. This is reflected very clearly in the wide PIs and high I 2 seen in our results.
The pooled risks for reoperations in our analysis were 5.3% with a 95% CI of 1.5% to 10.6% and a 95% PI of 0.0% to 32.0% in publications on nonaugmented screws and 3.9% with a 95% CI of 0.0% to 12.4%, and a 95% PI of 0.0% to 39.6% in publications on augmented screws. These rates are similar to reports of comparable procedures in patients with a mean age of less than 50 years, which range from 0% to 18.5%. 68 -72 It appears that despite an apparent increased screw loosening rate, the reoperation rate remains the same. There are several possible explanations for this observation. Most likely, screw loosening is frequently reported as a radiographic phenomenon with no clinical consequence, especially in the light of the limited follow-up times. In symptomatic patients, the classic telltale of implant loosening is pain, yet pain remains subjective and the relative severity of the discomfort or pain may not be significant enough to warrant additional surgery. In elderly patients, the threshold for the decision to perform another surgery may be higher than in younger patients due to their lower lifestyle demands and potential increased comorbidities. In younger patients, a more active lifestyle could lead to increased stresses on the implants which in turn may lead to higher clinical failure rates.
Limitations
Reporting of Complications
The major limitation of our analysis results from the incomplete and non-standardized reporting in the included publications. Many of the complications we regarded as relevant in the context of osteoporosis were hardly ever documented. Of the 32 eligible publications, 18 mentioned subsequent vertebral fractures, and only 12 specified whether these fractures occurred in adjacent segments. Likewise, adjacent segment degeneration was only documented in 3 publications. While variables targeting kyphosis were reported, none of the publications reported specifically on proximal junctional kyphosis. Therefore, we cannot provide an overview about the incidence of some complications specifically relevant in the context of osteoporosis.
Additionally, the reporting of “zero” complications was the exception rather than the rule. In many instances it remained unclear whether information on complications was omitted, not available, or whether the respective complication did not occur. Such reporting practices bear the risk of misinterpretation and pave the way to underreporting. We tried to address this by developing an algorithm that allowed us to assume a zero incidence of certain complications if the remainder of the report provided sufficient detail to justify our assumption. In all other instances, we rigorously excluded parameters from the quantitative analysis if no unequivocal statements about their incidences were provided. Under the assumption that “zero” incidences were omitted unintentionally, our conservative approach could potentially have overestimated the respective incidences.
This appears probable because we did not find any indication that the reason for omitting complications was related to a potentially unfavorable outcome and could thus have led to a differential reporting bias. More likely, due to the different focus of the research, authors were not aware of the importance of such information for readers interested specifically in complications. The low scoring on the McHarm Scale of most of the included studies and the widespread absence of a prespecification of complications is a clear indication for a lack of awareness how complication reporting should optimally be done.
In spite of attempts to address the topic, 19 no standardized guideline has been established that describes how complications should be reported, including specifically that reporting “zero” incidence should be mandatory. 19
Heterogeneity of Results
Moreover, the limited and heterogeneous information available made us refrain from quantitively addressing important potential outcome determinants like sagittal balance or the length of the instrumentation. Drawing meaningful conclusions from our analysis is further complicated by the pronounced heterogeneity of the pooled results. However, wide ranges of results are often reported after spinal fusion procedures with comparable indications. This is usually attributed to the variability of interventions, but there is also a lack of standardized reporting. 73,74
Inclusion Criteria
An additional limitation of our analysis was that only studies that clearly specified the presence of osteoporosis were included. This may have led to the exclusion of publications in which many of the patients were osteoporotic, but the authors did not specifically mention it because a diminished bone quality in frail and elderly patients is taken as a given. Age is widely used as a proxy for osteoporosis even though complete osteoporosis checkups are not routinely performed. 75 At the same time, this inclusion criterion may have limited our selection to studies in which the authors were sufficiently aware of the potential sequels of osteoporosis to address the condition better than in other studies. This could have contributed to the good results reported in these publications and thereby biased our selection.
Publication Bias
This meta-analysis addresses complications, which are reported as incidences. Unfortunately, no established statistical method to determine the presence of publication bias for incidences exist so far. Most other meta-analyses compare different interventions to identify find out whether the differences between treatments are significant. This allows determining the presence of publication bias with a funnel plot with the underlying idea that small studies with nonsignificant results are less likely to be published than studies with significant findings. This would then become visible in the asymmetry of the plot. The present work, however, analyzes incidences, so there are no significant or nonsignificant studies. In this case, a funnel plot could only demonstrate the presence of a “small study effect,” that is, whether the incidences in small studies differ from those in large studies. Additionally, in the case of proportions, the relationship between the estimate itself (incidence) and its variance may lead to asymmetric funnel plots even when no small study effect is present. Most important, an asymmetric funnel plot may just reflect the true differences seen in the individual studies’ estimates, which is then demonstrated by a high heterogeneity, as it is the case with our results.
Conclusion
The findings of this meta-analysis suggest that screw augmentation may be beneficial in osteoporotic spines; however, this needs to be confirmed through further studies. Reoperation rates were not excessively high, indicating that the risks resulting from diminished bone quality may not necessarily lead to revision surgery. Our analysis was hampered by the low quality of complication reporting; therefore, we recommend that publishers and reviewers insist that complication reporting be complete, unequivocal, and follow defined standards.
Supplemental Material
Supplemental Material, CIOS_table_10_other_AEs_reop_SUPPLEMENTARY_single_spaced - Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis
Supplemental Material, CIOS_table_10_other_AEs_reop_SUPPLEMENTARY_single_spaced for Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis by Elke Rometsch, Maarten Spruit, Jack E. Zigler, Venugopal K. Menon, Jean A. Ouellet, Christian Mazel, Roger Härtl, Kathrin Espinoza and Frank Kandziora in Global Spine Journal
Supplemental Material
Supplemental Material, CIOS_table_7_(formerly_4)_adapted_McHarm_items_SUPPLEMENTARY_single_spaced - Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis
Supplemental Material, CIOS_table_7_(formerly_4)_adapted_McHarm_items_SUPPLEMENTARY_single_spaced for Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis by Elke Rometsch, Maarten Spruit, Jack E. Zigler, Venugopal K. Menon, Jean A. Ouellet, Christian Mazel, Roger Härtl, Kathrin Espinoza and Frank Kandziora in Global Spine Journal
Supplemental Material
Supplemental Material, CIOS_table_8_(formerly_6)_baseline_parameters_SUPPLEMENTARY_single_spaced - Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis
Supplemental Material, CIOS_table_8_(formerly_6)_baseline_parameters_SUPPLEMENTARY_single_spaced for Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis by Elke Rometsch, Maarten Spruit, Jack E. Zigler, Venugopal K. Menon, Jean A. Ouellet, Christian Mazel, Roger Härtl, Kathrin Espinoza and Frank Kandziora in Global Spine Journal
Supplemental Material
Supplemental Material, CIOS_table_9_McHarm_outcome_SUPPLEMENTARY_single_spaced - Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis
Supplemental Material, CIOS_table_9_McHarm_outcome_SUPPLEMENTARY_single_spaced for Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis by Elke Rometsch, Maarten Spruit, Jack E. Zigler, Venugopal K. Menon, Jean A. Ouellet, Christian Mazel, Roger Härtl, Kathrin Espinoza and Frank Kandziora in Global Spine Journal
Supplemental Material
Supplemental Material, Prisma_Checklist_CIOS_supplementary_updated_2018_10_15_no_hilite - Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis
Supplemental Material, Prisma_Checklist_CIOS_supplementary_updated_2018_10_15_no_hilite for Screw-Related Complications After Instrumentation of the Osteoporotic Spine: A Systematic Literature Review With Meta-Analysis by Elke Rometsch, Maarten Spruit, Jack E. Zigler, Venugopal K. Menon, Jean A. Ouellet, Christian Mazel, Roger Härtl, Kathrin Espinoza and Frank Kandziora in Global Spine Journal
Footnotes
Acknowledgments
The authors thank the AO Foundation TK System for funding this work and AOCID staff, in particular Anahí Hurtado-Chong, for critical review and helpful discussions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was funded by AO Foundation TK System. Two authors (Elke Rometsch and Kathrin Espinoza) are employees of AO Foundation in the Department of Clinical Investigation and Documentation (AOCID) and have received grants from the AO Foundation TK System during the conduct of the study. Concerning the work under consideration, Frank Kandziora has received travel support and honorary for board meetings by AO Spine and Maarten Spruit is Chairman of the AOSpine Technical Commission. Financial activities outside the submitted work within the preceding 36 months are reported by Frank Kandziora for his activities as a consultant for DePuy-Synthes, Siemens, and Silony, by Roger Härtl for his activities as a consultant for Brainlab, Ulrich, Depuy-Synthes, and Zimmer, and by Jean Ouellet for receiving grants from AO North America and from Omega, whereas the other authors have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by AO Foundation TK System.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.