
Abstract
Study Design:
Biomechanical study.
Objectives:
Failure of pedicle screws is a major problem in spinal surgery not only postoperatively, but also intraoperatively. The aim of this study was to evaluate whether cement augmentation may restore mounting of initially loosened pedicle screws.
Methods:
A total of 14 osteoporotic or osteopenic human cadaveric vertebral bodies (L2)—according to quantitative computed tomography (QCT)—were instrumented on both sides by conventional pedicle screws and cement augmented on 1 side. In vitro fatigue loading (cranial-caudal sinusoidal, 0.5 Hz) with increasing peak force (100 N + 0.1 N/cycles) was applied until a screw head displacement of 5.4 mm (∼20°) was reached. After loosening, the nonaugmented screw was rescue augmented, and fatigue testing was repeated.
Results:
The fatigue load reached 207.3 N for the nonaugmented screws and was significantly (P = .009) exceeded because of initial cement augmentation (300.6 N). The rescue augmentation after screw loosening showed a fatigue load of 370.1 N which was significantly higher (P < .001) compared with the nonaugmented screws. The impact of bone density on fatigue strength decreased from the nonaugmented to the augmented to the rescue-augmented screws and shows the greatest effect of cement augmentation on fatigue strength at low bone density.
Conclusions:
Rescue augmentation leads to similar or higher fatigue strengths compared with those of the initially augmented screws. Therefore, the cement augmentation of initially loosened pedicle screws is a promising option to restore adequate screw stability.
Keywords
Introduction
Treatment of degenerative spinal diseases, spinal deformity, trauma, and tumors often requires dorsal stabilization using pedicle screws. 1 Such surgical interventions are predominantly required by elderly people. Accordingly, the bone quality of the patients is poor, which represents a great challenge in the intraoperative course, 2 especially because a linear correlation between the bone mineral density (BMD) and screw stability has been described. 3 -5 Consequently, loosening of pedicle screws represents the main cause of failure in the postoperative course of dorsal instrumentations. 3,6 -8 However, loosening is not only a problem postoperatively, but also intraoperatively. The implanted pedicle screws are already subjected to a significant load during surgery—for example, during repositioning, during compression and distraction, or during insertion of the rod. Thus, pedicle screw loosening may already occur intraoperatively.
In case of intraoperative screw loosening, there are different techniques of revision. Probably a thicker pedicle screw is the most common choice, but this technique has a limited effect and is not always possible, depending on the anatomical conditions. 9 Another technique is the subsequent cement augmentation of the screw. Augmentation of pedicle screws with cement is widely used in dorsal instrumentation. 10 -12 Biomechanical studies have shown an approximately 2-fold increase of pull-out force and significantly increased fatigue strength of initially augmented screws over nonaugmented screws, 10,13 -15 but there are few studies that investigated the subsequent cement augmentation of loosened pedicle screws. 16,17 However, only nonphysiological pull-out testing was applied, and the bone density of the vertebrae was above the problematic range from the clinical praxis.
This study focuses on cement augmentation of initially loosened pedicle screws. The aim was to investigate whether the stability after rescue cementation is greater than that of uncemented screws and to determine how they compare with primarily cemented screws. A fatigue testing setup aiming to simulate in vivo loading conditions instead of nonphysiological pull-out testing was used.
Materials and Methods
Human cadaveric lumbar vertebral bodies (L2) with osteopenic or osteoporotic bone mass were collected from donors aged between 46 and 96 years, sealed in plastic bags and stored below −20°C. Computed tomography (CT) images of the specimens were recorded using a 16-row CT scanner (Brilliance 16 CT; Philips Healthcare, Hamburg, Germany). Prior fractures or other pathologies could herby be excluded, leading to a sample size of 14 specimens. A solid calibration phantom (Bone Density Calibration Phantom, QRM, Moehrendorf, Germany) was present in every scan, so that the apparent volumetric BMD could be determined by linearly converting the specimen’s Hounsfield unit value to the phantom’s reference densities (Avizo 5.1, VSG Inc, Burlington, MA). A specimen’s individual BMD was derived from a defined voxel cube in the center of each vertebral body.
The specimens were defrosted the night before testing and all soft tissue was dissected from the vertebrae. Throughout preparation, the specimens were sprayed with Ringer solution and, when possible, wrapped in moist tissue in order to preserve tissue constitution. Both pedicles of each vertebral body were instrumented using commercially available self-tapping, cannulated, augmentable, polyaxial screws (5.5 mm × 45 mm, Mantis augmentable, Stryker Inc, Kalamazoo, MI). Screw insertion occurred parallel to the vertebral end plate under fluoroscopic guidance. Initially, 1 screw was cement augmented (Spineplex bone cement, Stryker Inc, Kalamazoo, MI), likewise under fluoroscopic guidance. Depending on the radiological appearance, screws were augmented with a volume of 2 to 3 mL of cement. Care was taken to ensure that the cement did not cross the midline (Figure 1). After instrumentation, the specimens were embedded in a spherical metal fixture using polyurethane resin (RenCast FC 52/53, Huntsman Inc, Salt Lake City, UT). The vertebrae were embedded from the anterior up to the posterior border of the vertebral body. The posterior arch and the pedicle remained completely free from embedding material (Figure 2).
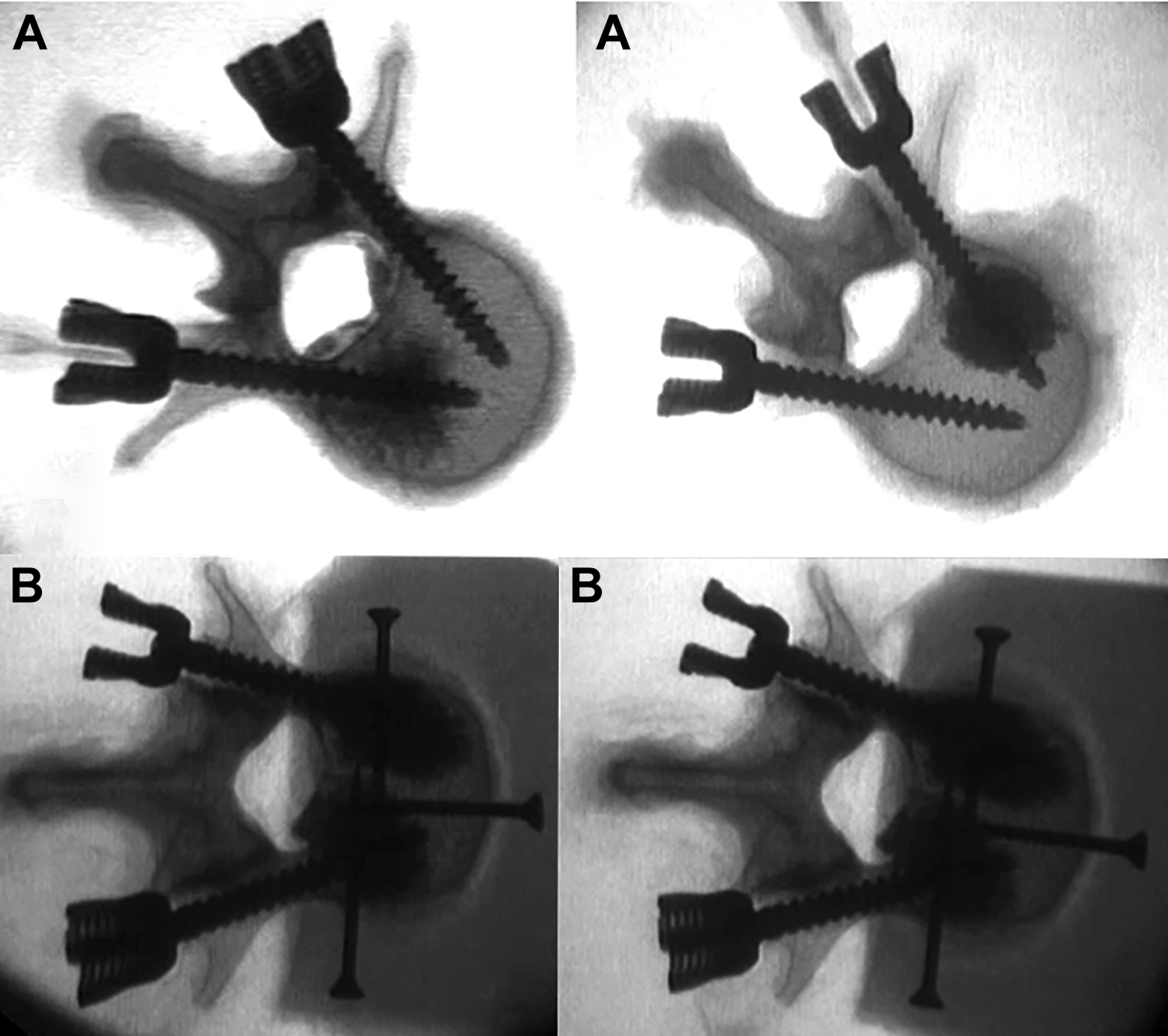
Axial X-rays showing exemplary vertebral bodies after instrumentation with pedicle screws and cement augmentation on one side (A) and rescue augmentation of the other side (B).
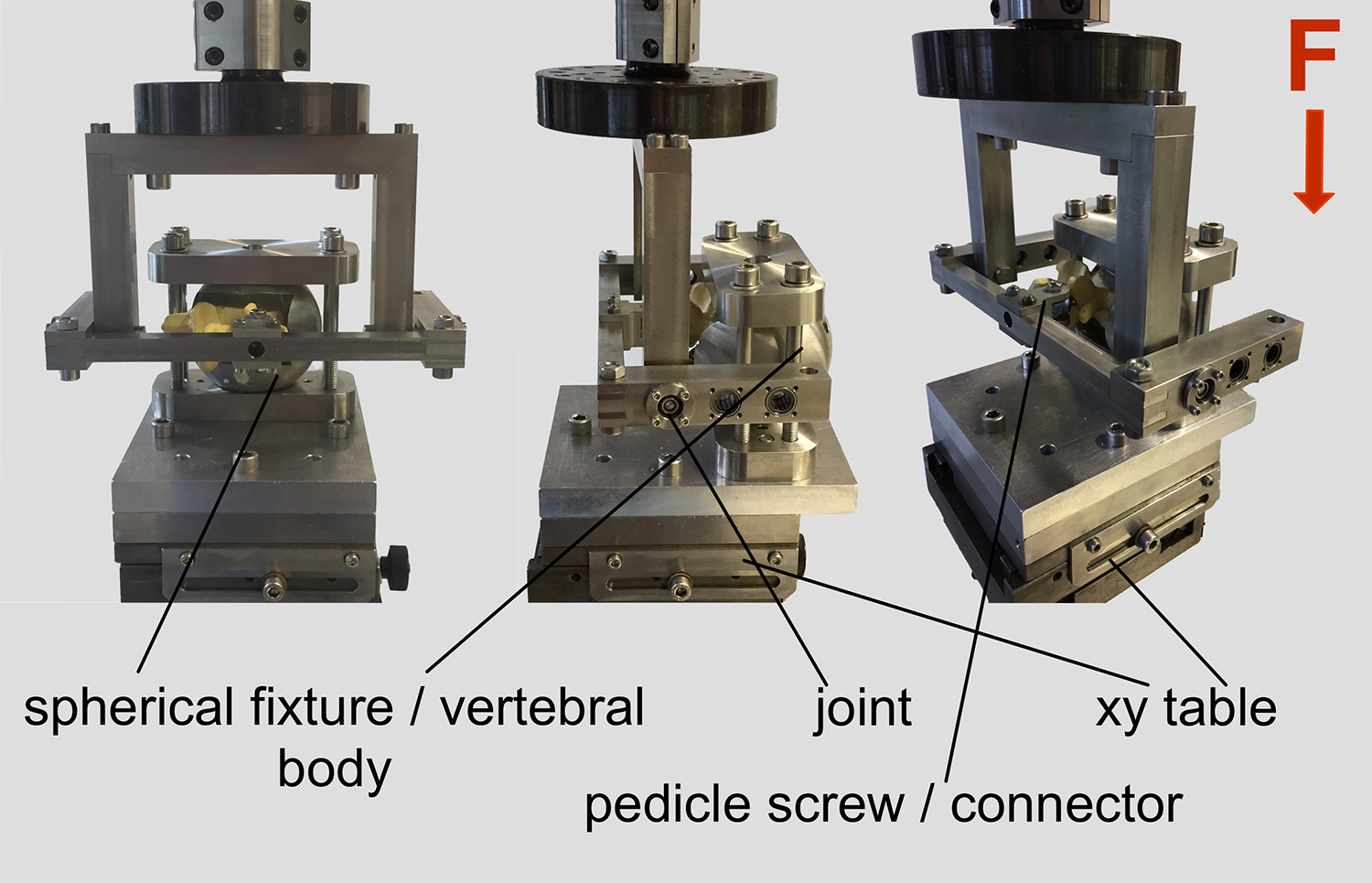
Specimens were mounted on an x-y table on a servohydraulic testing machine. Pedicle screws were positioned exactly horizontally by aligning the spherical fixture. Screws were linked to the connecting frame using a short rod, and the frame was linked to the material tested by a joint. Load was applied from the cephalad direction right through the head of the screw.
The fixtures with the enclosed specimens were mounted on a x-y table located at the bases of a servo-hydraulic testing machine (MTS 858.2, MTS Systems, Eden Prairie, MN). This was done in a way such that the relevant pedicle screw was positioned horizontally. Subsequently, the screw head was linked to the connecting frame using a short rod 2 cm in length (XIA titanium, Stryker Inc, Kalamazoo, MI) fixed with a blocker screw (Mantis Redux, Stryker Inc, Kalamazoo, MI). The connecting frame was linked to the actuator of the testing machine by a rotational axis, which was oriented perpendicular to the screw crossing the center of the screw head (Figure 2). With the rotational axis of the test setup also crossing the sphere of the screw head, no moment was introduced to the screw head, and consequently, no tilting between head and screw occurred.
A sinusoidal, cyclic fatigue force (0.5 Hz) was applied. For the initial cycle, it ranged from 50 to 100 N, which represents the load range during physiological walking. 18 To prevent effects of degeneration during testing, the testing was accelerated stepwise, increasing the peak force by 0.1 N every cycle (Locati test design). 13 Failure was defined as 5.4 mm of displacement of the screw heads (approximately 20° tilting). Testing was consecutively carried out for both sides (augmented or nonaugmented), but the testing order between augmented and nonaugmented sides was alternated.
After loosening of both screws, the nonaugmented screw was removed. A Jamshidi needle was introduced into the cavity that had been created as a result of screw loosening. The cavity was filled with bone cement (Spineplex bone cement, Stryker Inc, Kalamazoo, MI) under radiological control. Subsequently, the pedicle screw was screwed into the yet uncured cement. The volume of cement differed between 2 and 5 mL of cement depending on the radiological assessment of the distribution. Another fatigue test of the rescue-augmented screw followed. For the 2 groups with cement augmentation, CT scans were done after the mechanical testing to evaluate loosening by visual inspection. However, no unified scoring system or quantification was used.
Measured Parameters
The fatigue force at failure (5.4 mm, ∼20° tilting) was recorded. Stiffness of the constructs was determined at the beginning, at 50% of cycles, and at the end of testing—the 2 latter despite different loading cycles and failure load, respectively. The raw data was evaluated in a standardized manner (MATLAB, The MathWorks Inc, Natick, MA).
Statistical Analysis
For statistical analysis (SPSS, Version 21, IBM, Armonk, NY), the type I error probability was set to α =.05. Normal distribution was investigated using the Shapiro-Wilk test. Homogeneity of variances was tested by Levene’s test. Parametric (1-way analysis of variance) and nonparametric (Mann-Whitney U test) analyses were performed to compare the fatigue load as well as the stiffnesses.
Results
The individuals from whom specimens for this study were obtained were between 46 and 96 years old (mean = 75 years; SD = 14 years). Because reduced BMD was a selection criterion, each vertebral body exhibited a BMD <120 mg/cm3 (mean = 72 mg/cm3; SD = 22 mg/cm3).
Failure was detected in each screw tested, and the visual screening showed a loosening, whereas there was no tilting of the screw heads with respect to the screw axes. Signs of loosening were qualitatively exhibited in the posttesting CT scans of each augmented screw—in detail, a more pronounced widening in the area of the pedicle and a slightly higher enlargement of the entry point in rescue-augmented screws (Figure 3).
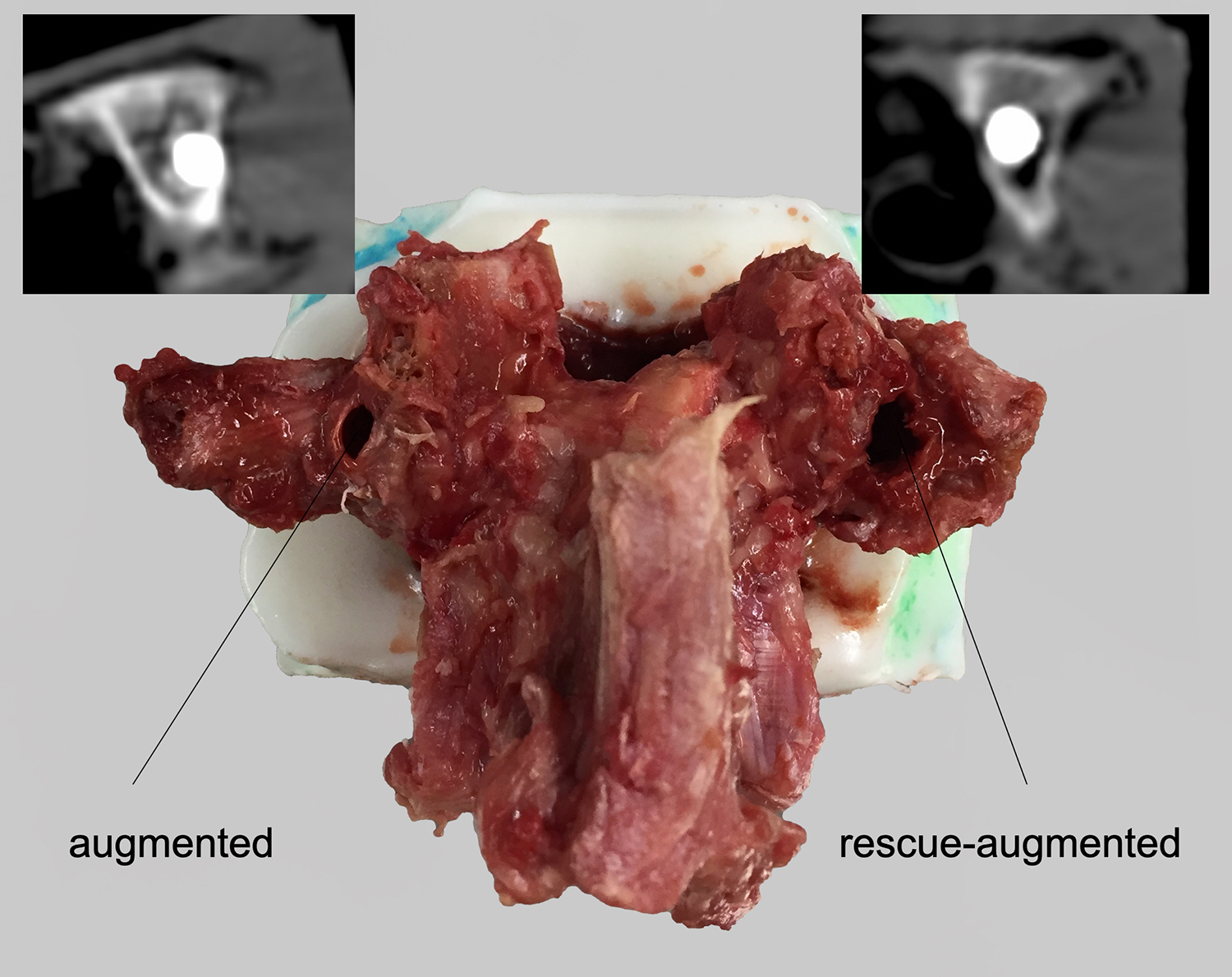
After testing, the specimens showed a more pronounced loosening in the area of the pedicle and a slightly more widened entry point on the rescue-augmented side.
The construct stiffness at the beginning of testing did not significantly differ between nonaugmented, augmented, and rescue-augmented screws (P = .714). In each of these groups, stiffness decreased significantly during testing (Table 1). Although the stiffnesses did not differ significantly after completion of 50% of the cycles, the course of the individual groups was different. Whereas the nonaugmented and augmented screws initially had a relatively persisting stiffness at the beginning that decreased significantly in the second half of the test, the stiffness in the group of rescue-augmented screws decreased steadily from the beginning onward (Figure 4). At the end of the test, the nonaugmented screws showed a significantly higher stiffness compared with the augmented and rescue-augmented screws (P = .014; Table 1). However, it has to be kept in mind that the applied cycles to failure and, consequently, the applied load to failure differs among groups.
Stiffness of Nonaugmented, Augmented, and Rescue-Augmented Screws At the Start and At the End of Testing (Mean and SD).a
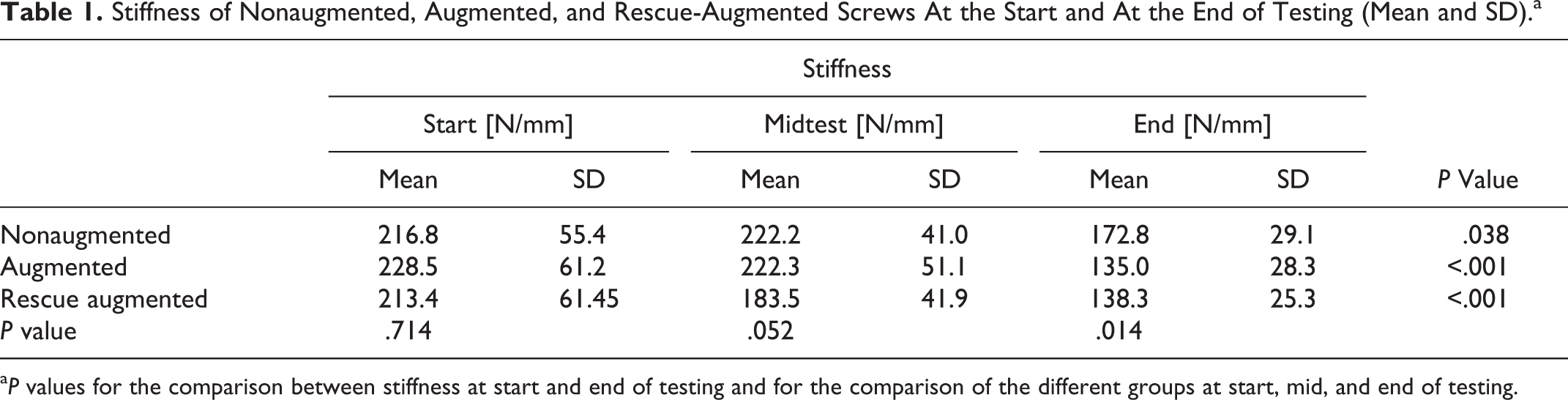
aP values for the comparison between stiffness at start and end of testing and for the comparison of the different groups at start, mid, and end of testing.
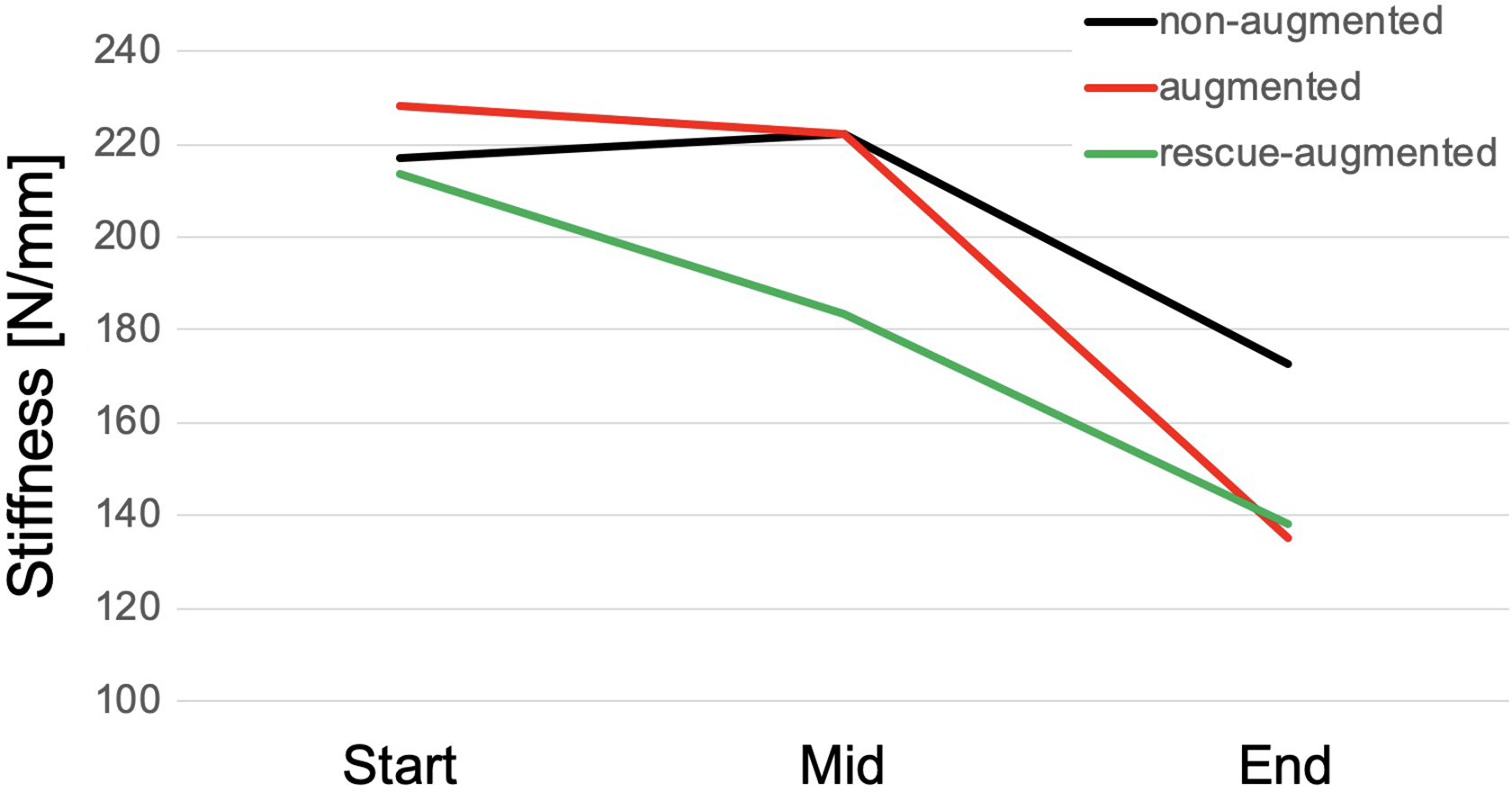
Line chart showing the stiffness of nonaugmented, augmented, and rescue-augmented screws at the beginning, after 50% cycles, and at the end of testing. It is noteworthy that the applied numbers of loading cycles and the peak load at the end of the testing was significantly higher for augmented screws and again higher for the recue-augmented specimens.
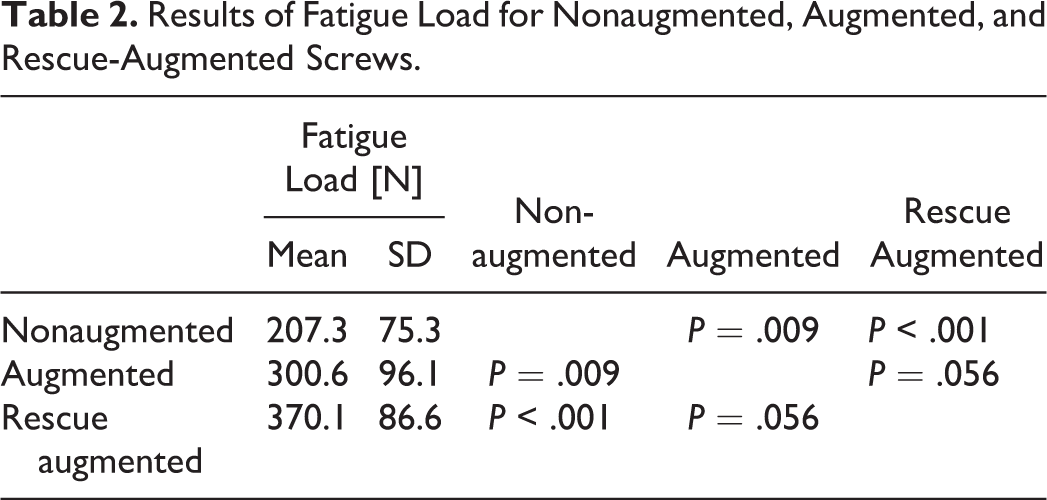
The fatigue load was 207 N (SD = 75 N) for the nonaugmented screws, whereas the augmented screws endured a significantly higher load of 301 N (SD = 96 N; P = .009). After rescue augmentation, the initially loosened screws showed a fatigue load of 370 N (SD = 87 N), which was significantly higher compared with the nonaugmented screws (P < .001). There was a trend showing a higher fatigue load in the rescue-augmented screws compared with the augmented screws (P = .056; Figure 5; Table 2).
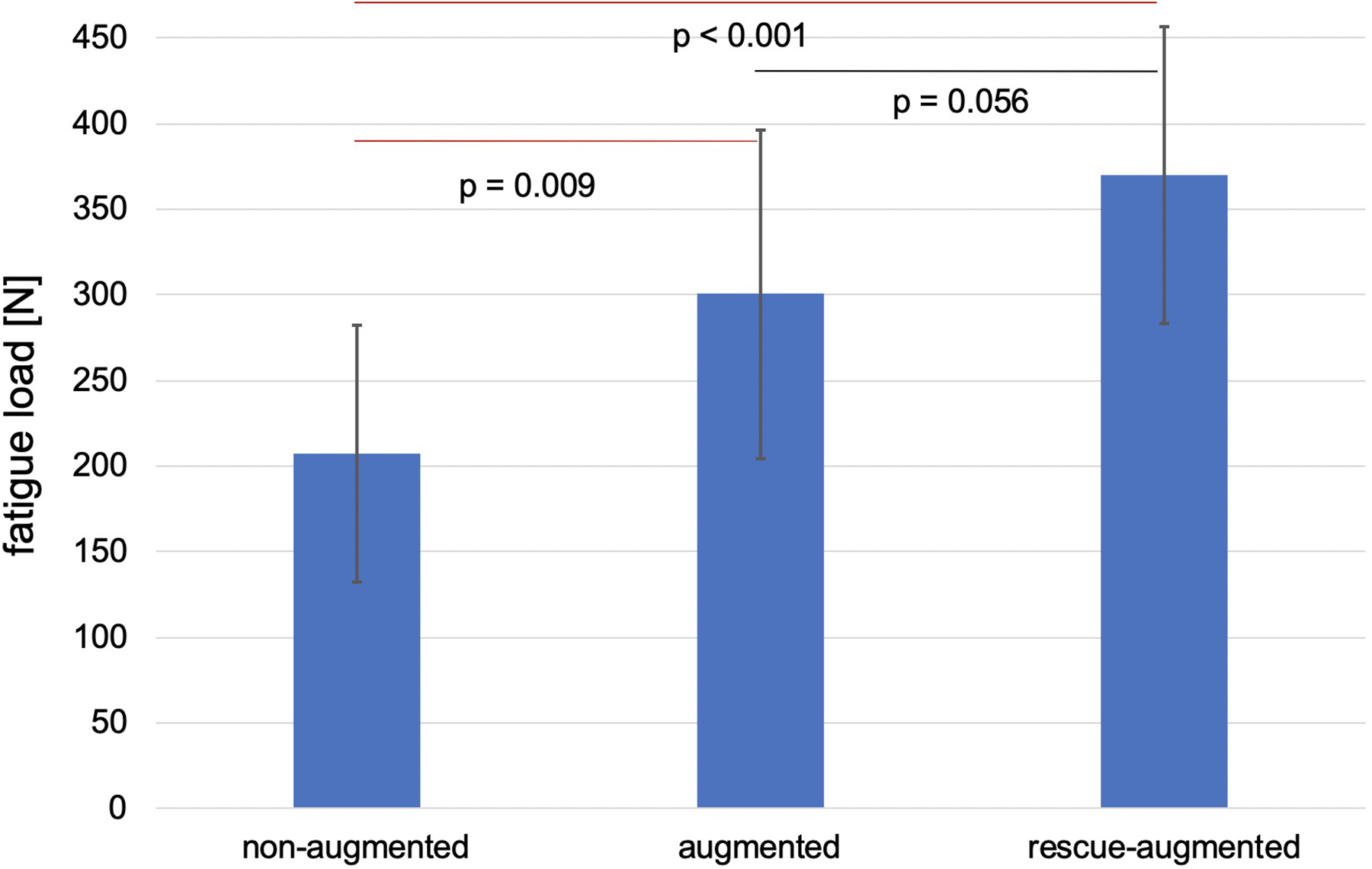
Failure load of nonaugmented, augmented, and rescue-augmented screws at the end of the fatigue testing. The achieved cycles were similar.
Results of Fatigue Load for Nonaugmented, Augmented, and Rescue-Augmented Screws.
Despite the small range of BMDs within the harvested specimens, a significant correlation between BMD and fatigue load of the nonaugmented (P = .012) and augmented screws (P = .043) was observed, whereas the fatigue load of the rescue-augmented screws did not significantly correlate with the BMD (P = .398). The closest correlation was seen in the nonaugmented screws, showing a very low failure load at low bone density, whereas cement augmentation particularly increased failure load with poor bone densities, resulting in a less close correspondence (Figure 6).
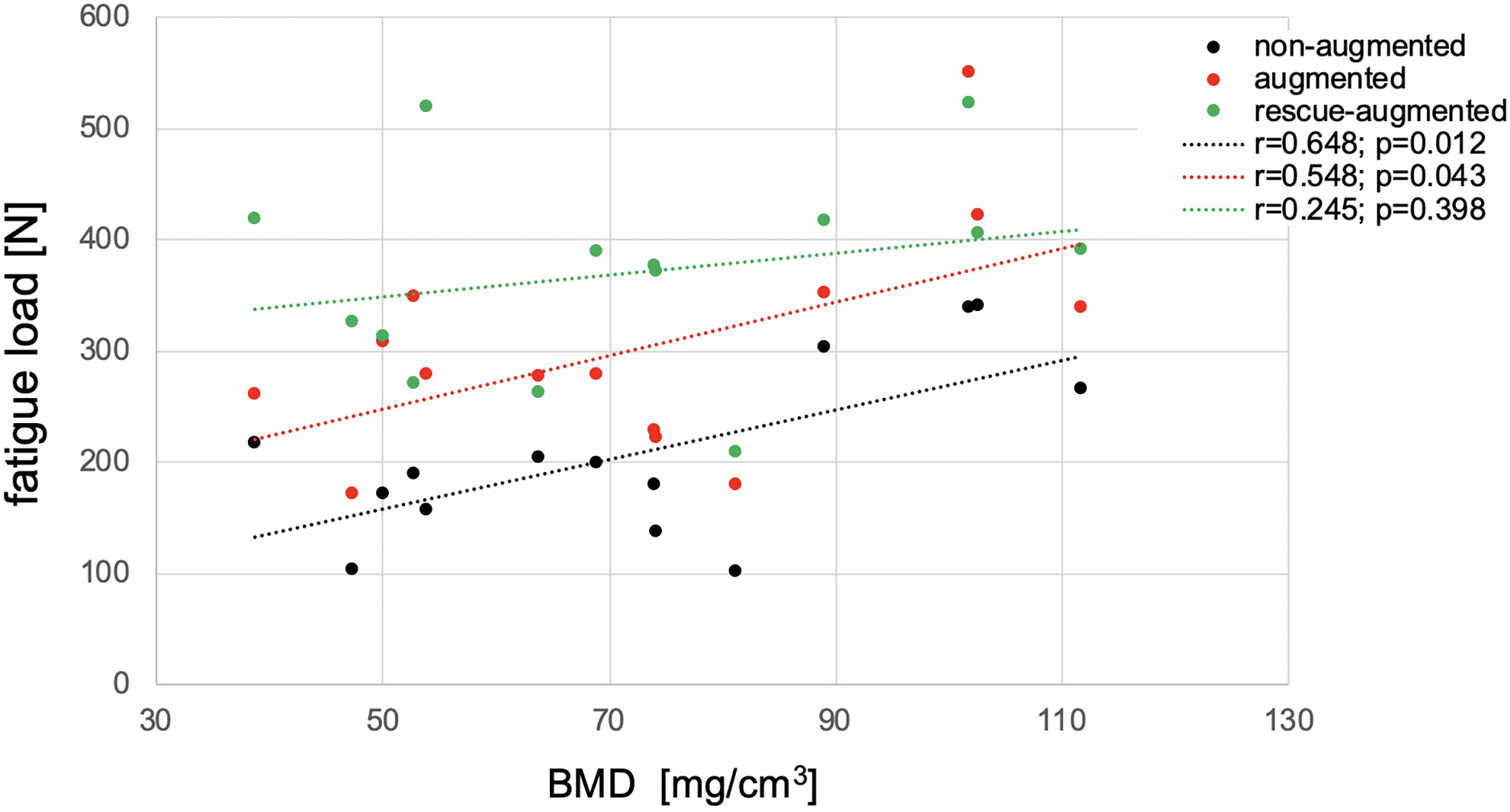
Correlation of fatigue load and bone mineral density (BMD) for the nonaugmented, augmented, and rescue-augmented screws.
Discussion
Spinal surgical treatment of especially elderly patients with poor bone quality represents a great challenge for orthopaedic surgeons—in particular, loosening of pedicle screws in the intraoperative and postoperative course. No data on the incidence of intraoperative screw loosening is available, and guidelines concerning handling of screw loosening in this situation are scarce.
Probably the most commonly used technique for revision of an intraoperatively failed screw is choosing a thicker screw, but the appraisal is inadequate and inconclusive. 19 Hirano et al 20 stated that a larger screw would not enhance screw stability and might break the thin cortex in osteoporotic vertebrae. 20 Polly et al 9 showed that an increase in screw diameter led to a better insertional torque compared with revision with the same screw; however, they were not able to restore initial torque with the revision screws. Therefore, alternative methods are needed.
Pfeifer et al 16 showed that reconstruction with bone cement is able to reconstruct 149% of initial pull-out strength. Elsewhere, an increase in pull-out strength after rescue augmentation by 96% was shown. 17 Although both studies exhibited a significantly increased pull-out force by augmentation, it is problematic to draw conclusions for the clinical situation because the force application is nonphysiological.
The results of the present study show that screw cement augmentation can reconstruct and even significantly increase the failure load after loosening. With regard to the correlation between fatigue load and bone density, the regression coefficient for nonaugmented screws was higher than that for augmented screws. In both cases, the correlation was significant even though the BMD of the specimens covered a small range because of restricted inclusion criteria. In contrast, the rescue-augmented cases did not exhibit a significant correlation. This suggests that the success of screw implantation is less dependent on the discovered bone density for screw augmentation and especially for rescue augmentation. This might be explained by the increased anchorage of the screw through the cement in the vertebral body, which makes cancellous bone quality less relevant and by the potentially higher cement volume of rescue augmentation. The latter probably also caused the higher (nonsignificant) failure load of the rescue-augmented screws compared with the initially augmented screws. By loosening the screw in the vertebral body, a cavity is created and unstable spongiosa already broken. This results in a larger cement seal, which anchors the screw more stably in the bone. Furthermore, it explains the differences in the measured stiffness. From previous studies, it is known that the final failure stiffness of cement-augmented screws can be below that of nonaugmented screws (but at higher numbers of loading cycles). This is probably a result of the fact that the pivot point of screw loosening changed. In nonaugmented screws, it is located in the area of the pedicles and moves further into the vertebral body after screw augmentation. This increases the toggling lever arm, resulting in reduced fatigue stiffness. This effect is even more pronounced in rescue augmentation because the main anchoring of the screws is even further anterior in the vertebral body, in the area of the cement seal, and probably also because the cement volume is higher.
One of the major risks of cement augmentation include embolism and leakage. 21,22 Because of the study design, no statements in this regard can be made because the cortical wall of the vertebrae was covered in the potting. However, it is probable that the loosening of the pedicle screw in the vertebral body creates a cavity for the cement. This may lead to similar results as known during kyphoplasty and similar level of risk. Nevertheless, prior to augmentation, it has to be ensured that leaking into the spinal canal is inhibited.
It is worth mentioning the limitations of this study, especially the limited sample size because of the use of human specimens and the absence of in vivo factors such as bony ingrowth and fluid environment. Furthermore, the variation of the dimensions of the human vertebral bodies was not taken into account.
To keep the study design as consistent as possible, the screw diameter was not individually adapted to the specimen’s pedicle width according to clinical routine. In the strict sense, the findings are only valid for the L2 level with its rather thin pedicle, but it is highly relevant in treating fractures in the thoracolumbar transition. Inconsistencies with regard to the screw insertion as well as differences in the amount of cement per screw might have influenced the results, even though this was done based on radiological methods in an order similar to the usual in clinical practice. Factors associated with the testing setup such as subsidence of the specimen fixation, deformation of the setting, and stiffening of the cortical wall as a result of the potting might also have influenced the results. It is occasionally conceivable that loosening of the augmented screw during testing may also have damaged the vertebral body on the other side of the midsagittal plane—the side of the subsequent rescue augmentation. This bears the potential to negatively affect the failure load of the rescue-augmented screw. However, in this case, the test design would have likely underestimated the failure strength of the rescue-augmented screws.
In conclusion, cement augmentation of an initially loosened pedicle screw could adequately reconstruct the screw stability in a clinical failure situation, but attention has to be paid to the risk of leakage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.