
Abstract
Study Design:
Retrospective Cohort Study.
Objectives:
Spinal surgery site infection and chronic implant infection are possible causes for ongoing pain, implant loosening, and failed back surgery syndrome. Evidence of chronic infection was found in 29.1% of revision cases but is also found in a considerable number of degenerative cases without prior surgery. Infection mechanisms and possible clinical correlations are unclear.
Methods:
Retrospective analysis of standardized surgery site screening (swab, tissue samples, implant sonication) in 181 cases without clinical evidence of preoperative surgery site infection.
Results:
Screening results of cases without prior spinal surgery (n = 49, 10.2% positive) were compared to cases with prior spine surgery without implant placement (e.g. micro discectomy) (n = 21, 23.8% positive), revision cases following singular spinal fusion (n = 73, 23.2% positive), and cases with multiple revisions (n = 38, 50.0% positive). Propionibacterium spp. detection rate increased to 80% in positive cases with multiple revisions. Implants in place during revision surgery had a significantly higher infection rate (32.4%) compared to no implant (14.2%, p = 0.007). Positive cases had a significantly higher pain level prior to surgery compared to negative cases (p = 0.019). Laboratory parameters had no predictive value. Logistic regression revealed that previous spinal surgeries (odds ratio [OR] 1.38 per operation, p < 0.001) and male sex (OR 1.15, p = 0.028) were independent predictive factors for infection.
Conclusions:
Previous spinal surgery is a risk factor for chronic surgery site infection, leading to chronic pain, implant loosening, and revision. The presence of Propionibacterium spp. was correlated with chronic implant loosening and was more likely with cumulative surgeries.
Introduction
Pedicle screw loosening after spinal fusion occurs in up to 63% of cases; it compromises the intended osseous fusion and permanent stabilization of a segment, causes ongoing pain, and often eventually necessitates revision surgery. 1 Pedicle screw loosening, ongoing pain, and consequent spinal fusion failure seem to be correlated with a considerable but unknown prevalence of chronic low-grade surgery site and implant infection.2,3 Chronic inflammatory reactions induced by biofilm formation on the infected implant ultimately led to bone resorption and orthopaedic implant loosening. 4 The number of prior spinal surgeries seems to be a significant risk factor for the high rate of chronic low-grade surgery site infections (29.1%), predominantly caused by Propionibacterium spp and staphylococci in spinal fusion revision cases. 3 However, both bacteria species were also detected in herniated disc cases, with radiologically confirmed degenerative inflammatory changes and no history of previous surgical intervention. 5 Both Propionibacterium and Staphylococcus are commonly found in hair follicles and on the skin 6 ; so intraoperative contamination seems likely. There is a lack of clinical evidence on mechanisms of spinal surgery site infection and possible clinical correlations; it is unclear whether the high prevalence of surgery site infection in revision cases is caused by preexisting infection, correlated with degeneration, or by contamination during or following spinal surgery.
The study objectives were to investigate (1) the impact of prior spinal surgeries and implant placement on chronic surgery site infection risk and (2) potential clinical and laboratory parameters indicative of chronic surgery site infection prior to surgery.
Materials and Methods
Study Population and Data Collection
This study was approved by the Institutional Ethical Review Board of the Medical University of Graz (28-210 ex 15/16). It was performed in accordance with relevant guidelines and regulations, and informed consent was obtained from all participants.
For this retrospective study, intraoperative infection screening results in 70 patients undergoing primary open spinal fusion of at least 1 lumbar segment between 2015 and 2019 were compared with infection screenings from 111 revision cases following spinal fusion between 2013 and 2018 at our institution. We previously published a detailed analysis of 110 revision cases following spinal fusion 3 ; for the present study, 5 cases were excluded for lack of history of prior spinal surgeries, and 6 new cases were added. The main indications for revision were degeneration of the adjacent segment (44.5%), followed by pain only (30.9%), screw loosening (14.5%), and others (broken implant, fracture of an adjacent segment, cage dislocation) as characterized in our original study. 3
To outline prior spinal surgeries and/or implant placement as risk factors for chronic surgery site infection, cases were divided according to their surgical history: (a) cases without prior spinal surgery without prior implant placement, (b) cases with prior spinal surgery without implant placement (eg, microdiscectomy), (c) cases with prior spinal surgery with implant in situ, and (d) cases with multiple revisions (>1) following spinal fusion.
Demographic characteristics (age, sex, body mass index), laboratory parameters indicating acute bacterial infection (leucocyte blood count, C-reactive protein [CRP]), and rest/active pain level (expressed as Visual Analogue Scale [VAS]) were evaluated 1 day prior to surgery.
All included patients were considered as aseptic before surgery. Exclusion criteria were stabilization for infectious spondylodiscitis as the primary intervention, acute deep implant infection as the indication for revision, and/or long-term antibiotic therapy prior to surgery. Local vancomycin application was not performed in any case included in this study.
In all cases, intraoperative infection screening was performed by the surgeons according to our standardized protocol. 3 Intraoperative swabs and tissue samples for microbiological cultures and histology were immediately collected from degenerative lumbar disc material or surrounding tissue in case of implants in situ (disc material was not available in most revision cases). Sonication with consecutive cultures was performed for cases with any explanted metal.
Statistical Methods
Screening results, demographic characteristics, surgical history, and comorbidities were compared among patients with primary spinal surgery, prior surgery, and revision cases. Statistical analysis was performed using the χ2 test to compare categorical parameters, t-test for continuous normally distributed parameters, and Spearman correlation coefficient for correlation calculations. Multivariate logistic regression analysis was performed to identify independent factors predicting screw loosening as described by Hart et al. 7 Differences were considered significant at P <.05.
Results
This retrospective study included 181 patients with intraoperative infection screening of material from spinal surgery. Bacterial infection was identified in 46 (25.4%); the most commonly identified species were Propionibacterium acnes (also known as Cutibacterium acnes, n = 20) and Staphylococcus epidermidis (n = 13; Table 1).
Specification of Germs Isolated in 46 Patients With Positive Infection Screening.
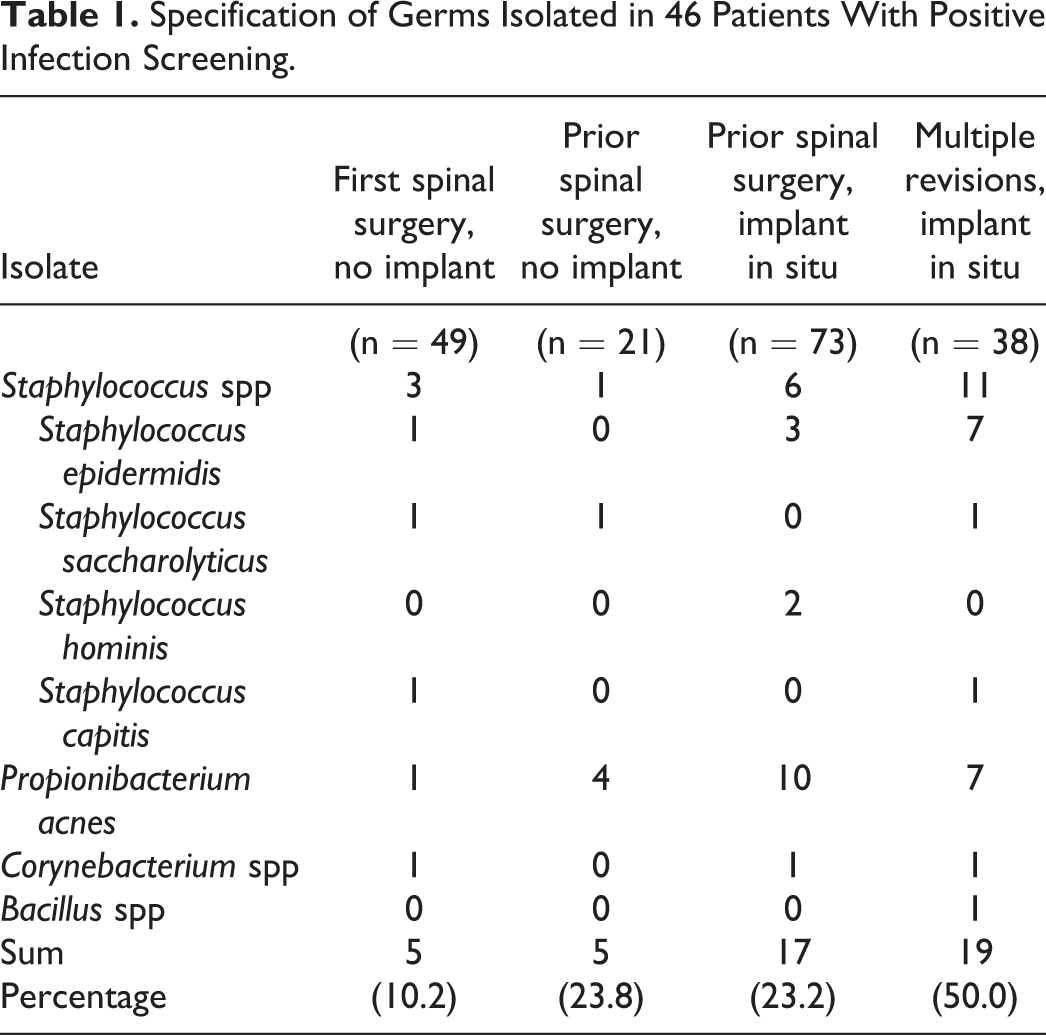
Cases with screening performed from degenerative spine with no prior surgeries had the lowest rate of bacterial identification (n = 49; 10.2% positive). There were higher rates of positive screening results in patients with prior surgical intervention without implant placement (eg, microdiscectomy) of the spine (n = 21; 23.8% positive; P = .136) and from revision cases following singular prior spinal fusion with implant placement (n = 73; 23.2% positive; P = .065). The bacterial contamination rate was significantly higher in cases with metal implants in place that had undergone repeated revision after spinal fusion (n = 38; 50.0% positive; P < .001; Figure 1).
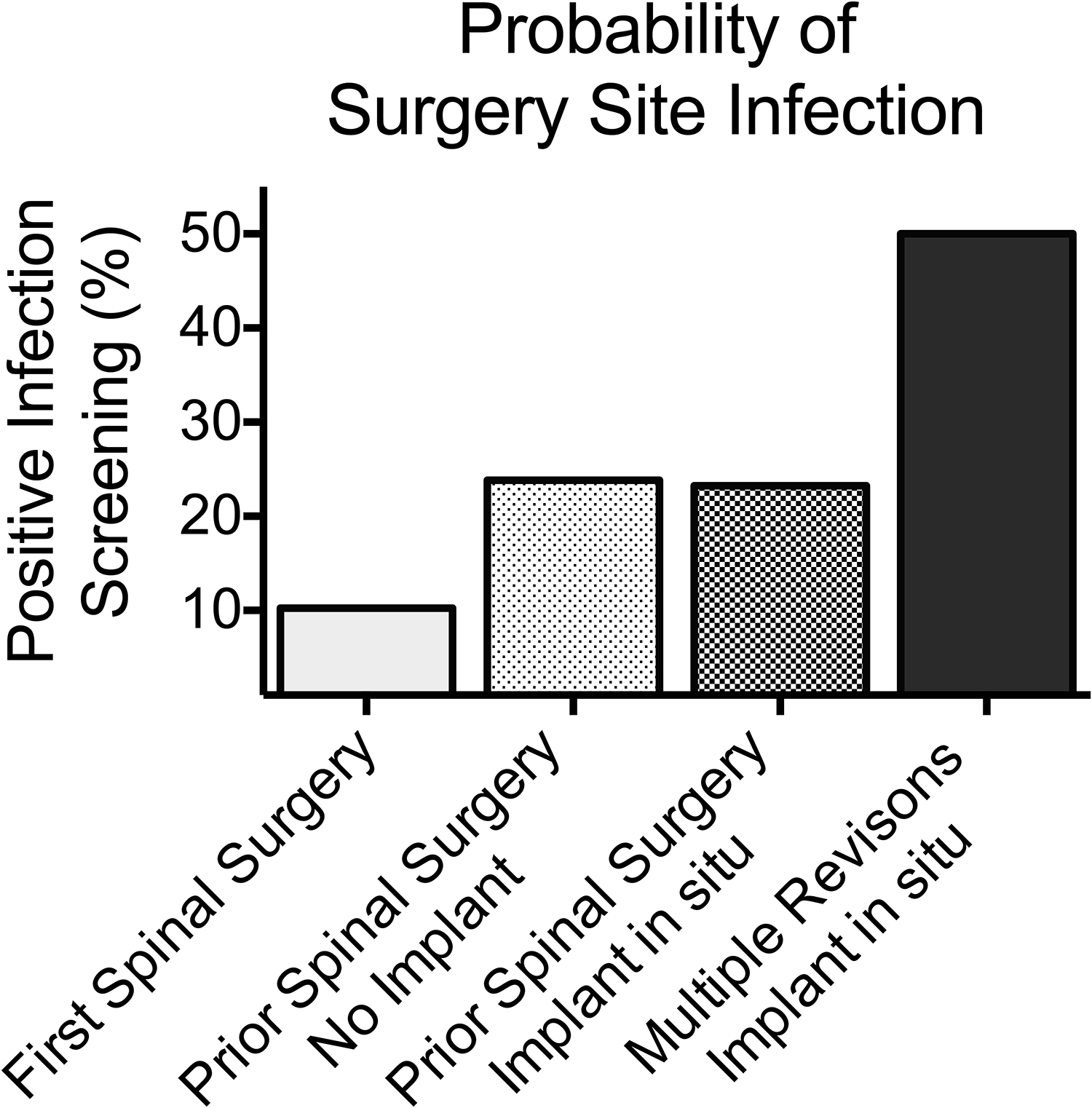
Probability of positive surgery site infection screening, according to our collective: first spinal surgery (n = 49; 10.2% positive); prior surgery, no implant (eg, microdiscectomy; n = 21; 23.8% positive); prior surgery, implant in place (n = 73; 23.2% positive); multiple revisions after spinal fusion, implant in place (n = 38; 50.0% positive).
Cases with preexisting metal implants in place during surgery (n = 111) had a significantly higher number of previous operations (1.6 vs 0.4; P < .001) and a significantly higher rate of positive infection screening (32.4% vs 14.2%; P = .007) compared with cases with no existing implant in the surgery field (n = 70). There were no significant differences between groups in terms of age, sex, rate of diabetes mellitus, smoking, or allergy status, which were considered as possible risk factors for chronic surgery site infection (Table 2).
Comparison of Patients With and Without a Spinal Implant In Situ During Surgery Site Infection Screening.a
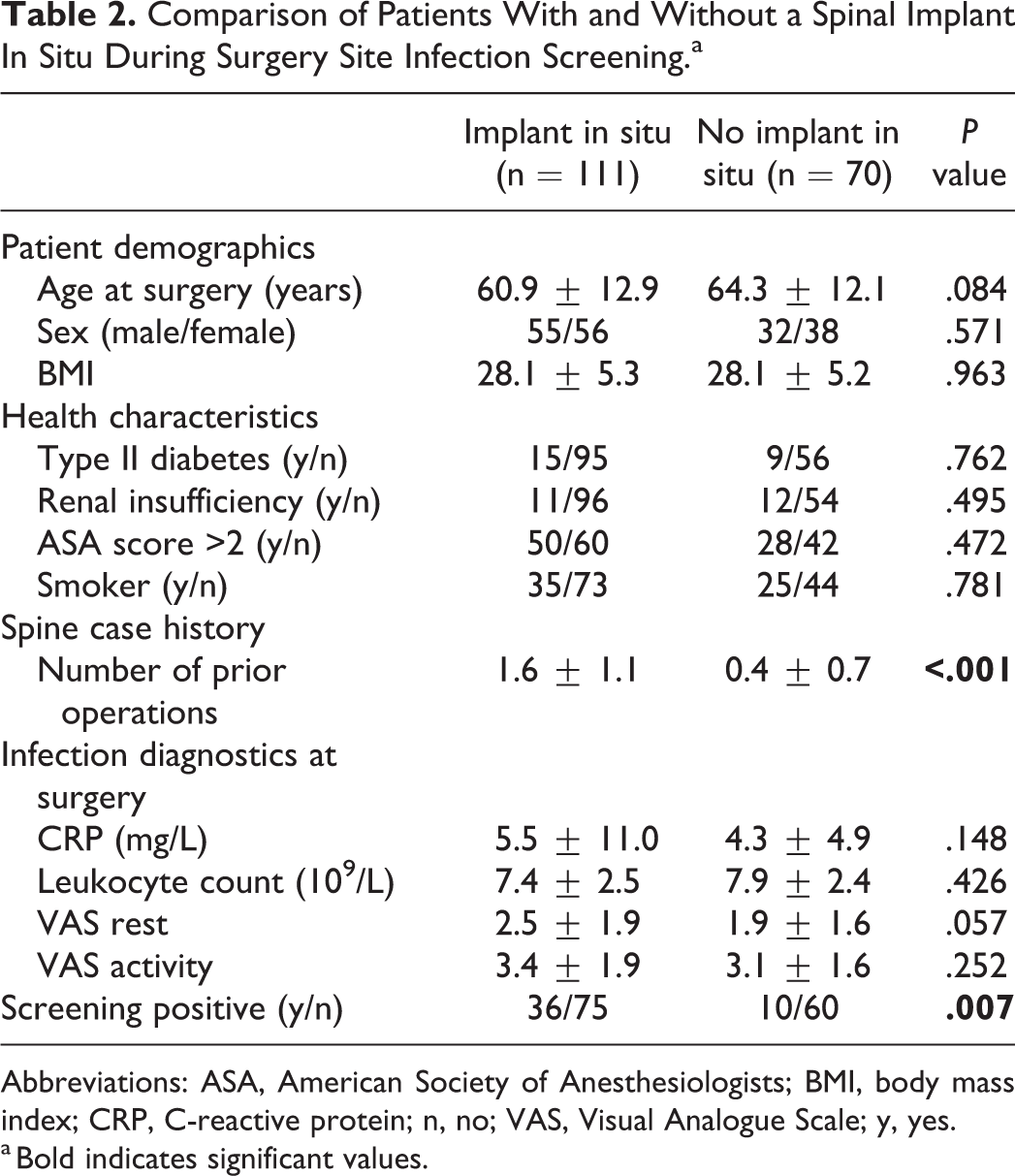
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; n, no; VAS, Visual Analogue Scale; y, yes.
a Bold indicates significant values.
Cases with positive surgery site infection screening had significantly higher preoperative activity pain levels (VAS: 3.93 ± 1.78) than negative screening cases (VAS: 3.09 ± 1.73; P = .019). There was no difference in resting pain levels (VAS: 2.54 ± 1.78 vs 2.19 ± 1.88; P = .33; Table 3). Among cases with existing implants, the difference in preoperative activity pain levels was more pronounced in positive screening cases (VAS: 4.29 ± 1.90 [positive] vs 3.11 ± 1.82 [negative]; P = .013).
Comparison of Patients With and Without Positive Surgery Site Infection Screening.a
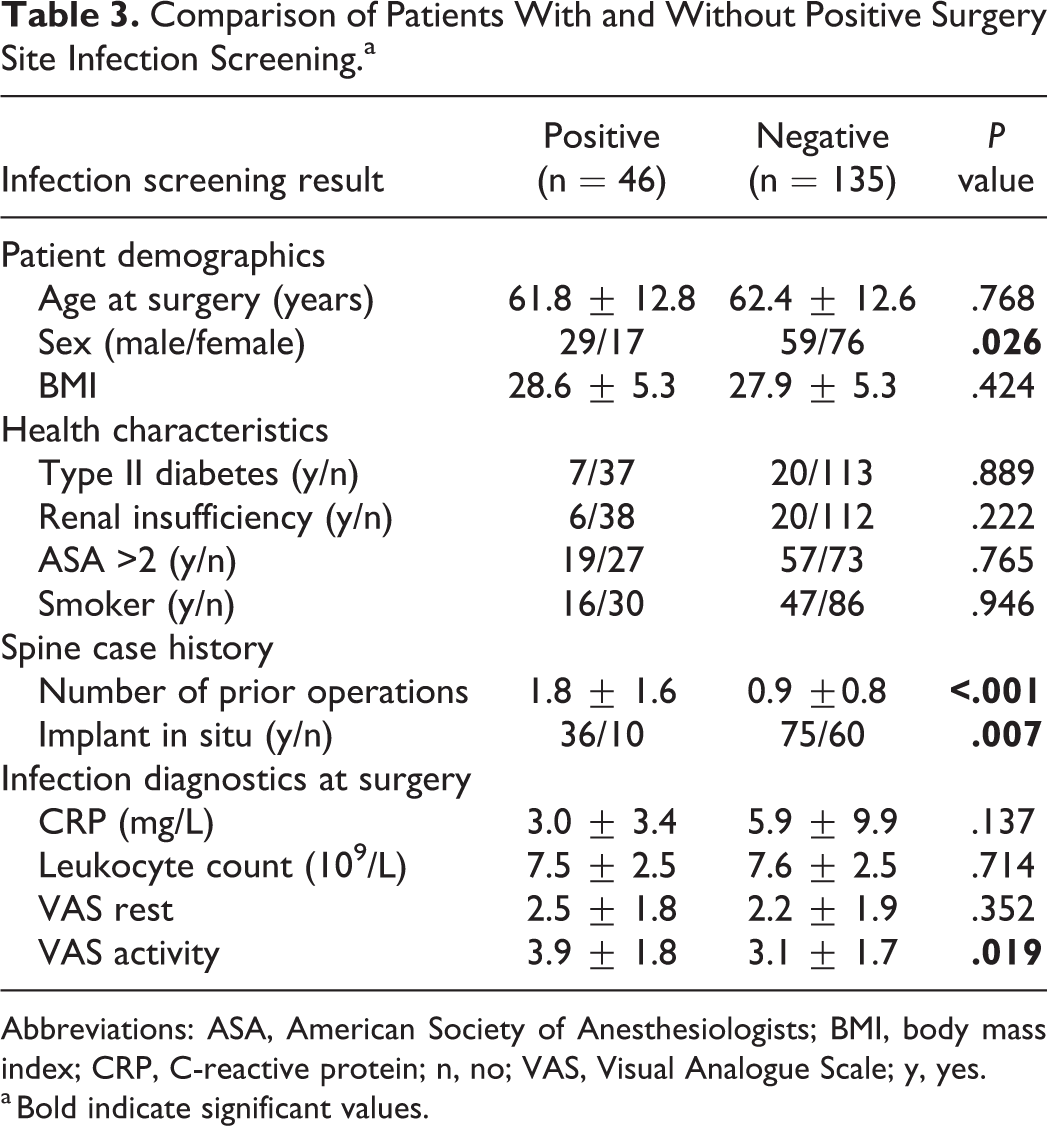
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CRP, C-reactive protein; n, no; VAS, Visual Analogue Scale; y, yes.
a Bold indicate significant values.
Preoperative inflammatory laboratory parameters had no predictive value for positive intraoperative infection screening. Leucocyte blood count (7.51 ± 2.6 vs 7.69 ± 2.5 G/μL) and CRP serum level (3.04 ± 3.4 vs 5.65 ± 7.9 mg/dL) were similar in positive and negative screening cases (Table 3).
Interestingly, the Propionibacterium spp detection rate was 20% among positively screened cases without prior spinal surgery and increased to 80% in cases with prior surgery; this difference was not significant, because of the low number of positive screening cases (Table 1).
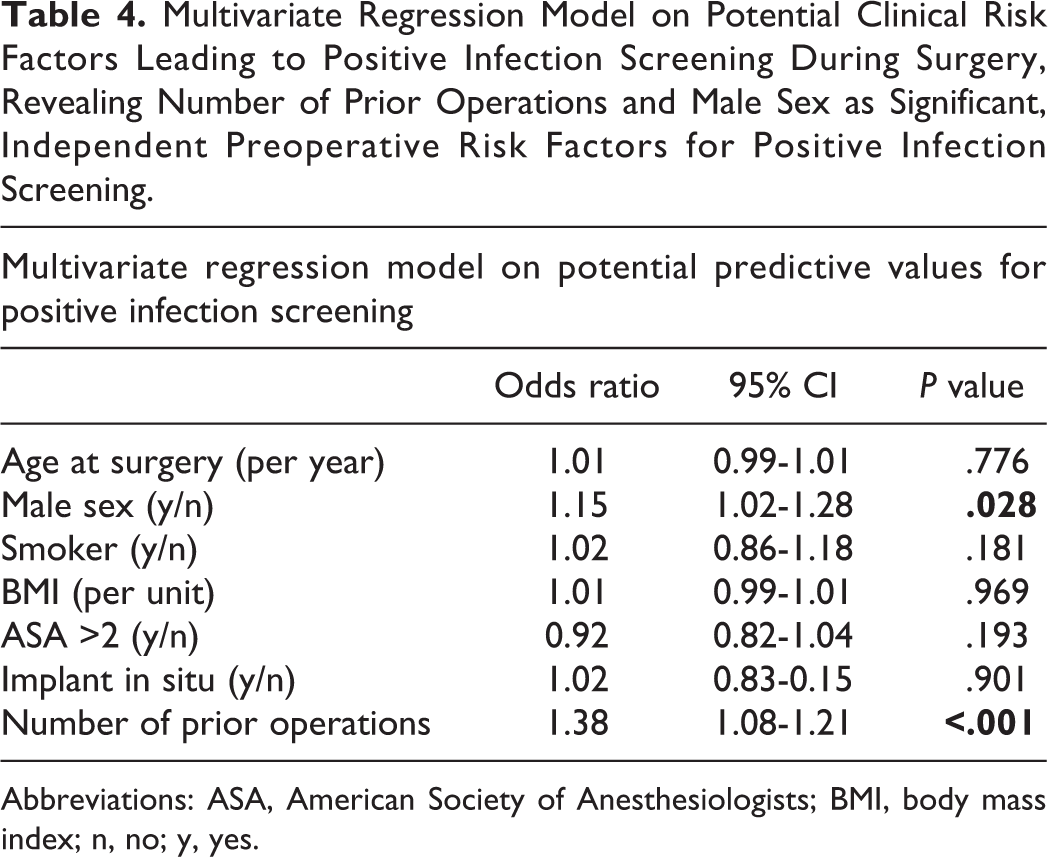
The subsequent multivariate logistic regression analysis was performed to identify independent, preoperative factors predicting positive infection screening. The number of previous spinal operations (odds ratio [OR] = 1.38 per additional operation; P < .001) and male sex (OR = 1.15; P = .028) were significant, independent factors indicating positive infection screening. Other factors, including presence of implants at surgery site at the time of the operation, were not significant in this model (Table 4).
Multivariate Regression Model on Potential Clinical Risk Factors Leading to Positive Infection Screening During Surgery, Revealing Number of Prior Operations and Male Sex as Significant, Independent Preoperative Risk Factors for Positive Infection Screening.
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; n, no; y, yes.
Discussion
Earlier observations suggested a correlation between signs of degeneration and evidence of chronic low-grade bacterial infection in patients without prior spinal operations, 5 represented by our study group (a: cases without prior spinal surgery without prior implant placement). On the other hand, chronic subclinical bacterial infection by staphylococci and Propionibacterium spp seems to cause implant failure by contributing to loosening and ultimately leading to revision surgery after spinal fusion. 3
It was unclear whether the surprisingly high incidence of germ detection during spinal surgeries in both scenarios is a result of preexisting colonization or contamination during or following spinal surgery. The number of revision surgeries, presence of foreign material, and patient-associated health factors were evaluated to determine if they promoted spinal bacterial colonization.
The first aim of this study was to clarify the impacts of several risk factors for bacterial contamination of the spine via comparison of standardized surgery site infection screenings in a large cohort of primary degenerative spinal surgery cases and miscellaneous revision cases.
The lowest infection rate was found in patients with no history of prior spinal surgery. Our multivariate regression model revealed that any prior spinal surgery dramatically increased the risk of a positive screening. This finding suggests that the majority of surgery site colonization occurs intraoperatively and is likely influenced by cumulative surgery duration. A similar correlation between primary spinal surgery duration and increased wound infection risk was previously reported. 8 This is in line with published data on repeated revision surgery and increased infection risk following knee arthroplasty. 9 We assume that poorly vascularized and dysfunctional scar tissue, which is often present in a surgery site following multiple spinal revisions, provides a vulnerable niche for chronic low-grade bacterial infection.
According to our multivariate regression model, the presence of spinal implants and concomitant diseases were minor, nonsignificant covariables for infection risk. A correlation between male sex and the probability of revision and/or chronic low-grade spine surgery site infection was described in other studies.3,10
S epidermidis or P acnes were detected in a significant proportion of disc herniation material evacuated via miniopen surgery under stringent sterile conditions from patients without any prior operations or clinical signs of an infection.5,11 Even in these cases, contamination cannot be fully ruled out; a certain false-positive detection rate caused by contamination must be considered with any screening method. 12 The significantly higher rate of germ detection in cases with prior surgery and revision cases still indicates a higher infection rate in these cases because contamination would be equally distributed.
According to a meta-analysis, local vancomycin application during spinal surgery might protect from surgery site infection, especially in high-risk cases; however, this approach is not commonly supported by the scientific community. 13 Local vancomycin application was not performed in any case included in this study. According to our data, cases with a higher number of prior spinal surgeries might benefit from this method because of their higher risk for chronic surgery site infection.
The second aim of this study was to identify potential laboratory or clinical parameters indicating chronic bacterial surgery site infection prior to surgery. This remains challenging because clinical presentation ranges from chronic pain to implant loosening and nonunion of the fused segment. We found that although laboratory parameters usually have high diagnostic specificity for acute infection, they do not add much value in the diagnosis of chronic low-grade spinal infection, as previously published for chronic spinal implant associated infection. 14 Chronic, ongoing pain might have diagnostic value for identifying cases with chronic surgery site infection. 15 Our results suggest that local pain during activity after spinal surgery may be a useful symptom.
Study Limitations
Whereas primary spinal surgery in the control group was performed for degeneration, revision group operations were mainly performed to address implant failure. This would result in overrepresentation of bacterial identification in the revision group because chronic implant infection might lead to more revision surgeries. 5 In any event, the results remain relevant regarding the study aim of identifying risk factors for bacterial surgery site colonization.
Sonication of removed implants is the most sensitive method for detecting implant infection. 12 This could lead to a higher detection rate compared with the group for which this technique could not be used because there was no implant in place. However, we also found a higher infection rate in cases with prior surgical intervention without implant sonication, indicating that the presence of an implant is not the determining factor for persistence of bacteria. We hypothesize that the degree of scar tissue may be a contributing factor.
Spinal injections and prior surgical intervention have been proposed as possible explanations for bacterial contamination in degenerative spine cases. Applying professional standards, we found that spinal injections were an exceptionally low risk factor and furthermore were equally distributed among our patient groups; so it was not included in our analysis.
We do not consider these limitations significant concerning our main finding that the number of prior spinal surgeries is the main risk factor for chronic surgery site infection.
Conclusion
In summary, cases with history of prior spinal surgery and revision cases should be considered as higher risk for chronic surgery site infection when spinal fusion is performed. The number of prior surgeries—rather than the use of implants at the surgery site—seems to be the determining factor for bacterial colonization that may lead to chronic low-grade infection. Increased levels of pain during activity might have a positive prognostic value for chronic surgery site infection, but preoperative laboratory parameters are usually not increased.
Footnotes
Authors’ Note
Authorship requirements have been met, and the final manuscript was approved by all authors. GB, RR, IZ-S, AL, and LL contributed to the conception of the study; GB, LL, PS, and AL wrote the main manuscript text; LL, GB, PP, RR, and IZ-S acquired and analyzed the data; and all authors reviewed and corrected the manuscript. This study was approved by the Institutional Ethical Review Board (Reference Number: 28-210 ex 15/16).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.