
Abstract
Study Design:
This is a broad, narrative review of the literature.
Objective:
In this review, we describe recent biomechanics studies on cement-augmented pedicle screws for osteoporotic spines to determine which factors influence the effect of cement augmentation.
Methods:
A search of Medline was performed, combining the search terms “pedicle screw” and (“augmentation” OR “cement”). Articles published in the past 5 years dealing with biomechanical testing were included.
Results:
Several factors have been identified to impact the effect of cement augmentation in osteoporotic spines. These include the type of augmentation material, the volume of injected cement, the timing of augmentation, the severity of osteoporosis, the design of the pedicle screw, and the specific augmenting technique, among others.
Conclusions:
This review elaborates the biomechanics of cement-augmented pedicle screws, determines which factors influence the augmentation effect, and identifies the risk factors of cement leakage in osteoporotic bone, which might offer some guidance when using this technique in clinical practice. Further, we provide information about newly designed screws and recently developed augmentation materials that provide higher screw stability as well as fewer cement-related complications.
Introduction
The transpedicular screw system has gained popularity during the past 2 decades to stabilize the posterior spine for the treatment of degenerative disorders, unstable fractures, deformities, and spine tumors.1-3 However, the pedicle screw fixation system is more heavily impacted by decreased bone mineral density (BMD) than other fixation systems like the lamina hook. 4 BMD usually plays a much more important role than other factors affecting the fixation strength, such as the insertion angle, insertion depth, and reinsertion of pedicle screws.5,6 Various studies have found that the stability of pedicle screws is highly correlated to BMD.4,7,8 Weiser et al 9 concluded that there was a highly significant correlation between BMD and pedicle screw stability (r2 = 0.839). Spines with BMD below 80 mg/cm3 reached only 60% of the stability compared with those with adequate bone quality (>120 mg/cm3). Furthermore, osteoporotic patients are predisposed to screw loosening, displacement, or even pulling out, with larger posterior internal fixation failure rates.10-12
Augmentation of pedicle screws with bone cement is recommended as an effective method to enhance the stability of posterior fixation in patients with osteoporosis. 13 A number of recent biomechanical studies are available to help optimize the clinical implementation of this technique. In this review, we give an overview of the current spectrum of screw augmentation techniques to provide some information for clinical practice.
Methods
A search of MEDLINE was performed, combining search terms “pedicle screw” and (“augmentation” OR “cement” OR “PMMA”) from January 1, 2015 to February 15, 2020. The initial search identified 168 potential articles, which were screened for eligibility based on the abstracts. Studies dealing with biomechanical testing of cement-augmented pedicle screws both in cadaveric spines and synthetic bone blocks were included. Articles with only clinical data, case reports, review papers, letters to the editor, Non- English language articles, were excluded. 45 studies in total were eventually included in this review.
Factors Influencing the Effect of Cement Augmentation
Several factors have been identified to impact the effect of cement augmentation in osteoporotic spines. These include the type of augmentation materials, the volume of the injected cement, the timing of augmentation, the severity of osteoporosis, the design of pedicle screw, and the specific augmenting technique, among others. None of the factors should be regarded as independent when we try to increase the augmentation effect by considering these influential factors.
Different Augmentation Materials
The distinct effect of augmentation using different materials may be attributed to the diversity in cement properties. The most widely used material, polymethylmethacrylate (PMMA), is characterized by stability, high curing strength, and rapid solidification, and it tends to provide greater strength than many other augmentation materials,14,15 although these materials are equipped with osteoconductivity, osteoinductivity, and biodegradability.
However, concerns have already been raised about the high exothermic polymerization temperature, toxicity of the monomer, and lack of osteoconductivity of PMMA, which is neither osteoinductive nor biodegradable. 16 Calcium phosphate cement (CPC) and calcium sulfate cement (CSC) equipped with osteoconductivity and osteoinductivity used to act as 2 potential alternatives, but both of them are unable to offer an adequate short-term period of stability which is essential to bone remodeling.17-19
As a consequence, the drawbacks of conventional cement prompt the development of not only robust but also bioactive and absorbable augmentation materials. The goals for such materials are to play a similar or even greater biomechanical role compared with PMMA as well as to be safe and biocompatible. A novel calcium phosphate-based nanocomposite (CPN) introduced by Sun et al20-22 showed satisfying biodegradability, osteoinductivity in vivo, and exhibited equal even marginally higher maximal pullout force than PMMA. The dispersion pattern of the cement within cancellous bone is crucial to the effect of augmentation. Although the mechanical strength of CPN is weaker than that of PMMA, CPN has a more regular and symmetrical dispersion, which is conducive to achieving biomechanical stability similar to that of cannulated pedicle screws augmented by PMMA. 22 In addition, silicone was found to be osteoconductive and nonhazardous to surrounding tissue and shown to exhibit nonexothermic curing, which was in contrast to PMMA. 23 Schmoelz et al 24 inserted 3 mL of self-curing elastomer (silicone) into a balloon cavity prior to cannulated pedicle screw insertion, and the elastomer group underwent significantly more mean cycles until loosening under cyclic cranio-caudal loading than the PMMA during in situ augmentation (9824 ± 1982 N vs. 7401 ± 1644 N). Recently, Spicher et al 25 introduced a novel ultrasound-melted polymer sleeve to improve pedicle screw anchorage. Biomechanical tests revealed it resisted a significantly higher number of load cycles than the nonaugmented controls, and the number of load cycles until failure was not different from PMMA-augmented screws. The thermoplastic polymer consisting of poly(L-lactide-co-D, L-lactide) copolymer has a biocompatible and biodegradable material structure with an approximate resorption time of 2 to 3 years and does not interfere with bone remodeling. 26 More recently, poly-dicalcium phosphate dihydrate (P-DCPD) cement, which has attractive safety characteristics such as nonexothermic curing and drug-eluting capacity, was demonstrated to significantly increase the pullout load of pedicle screws after augmentation to achieve the similar biomechanical property to PMMA. 27 The characteristics of different cements for pedicle screw augmentation are summarized in Table 1.
Characteristics of Materials for Pedicle Screw Augmentation.
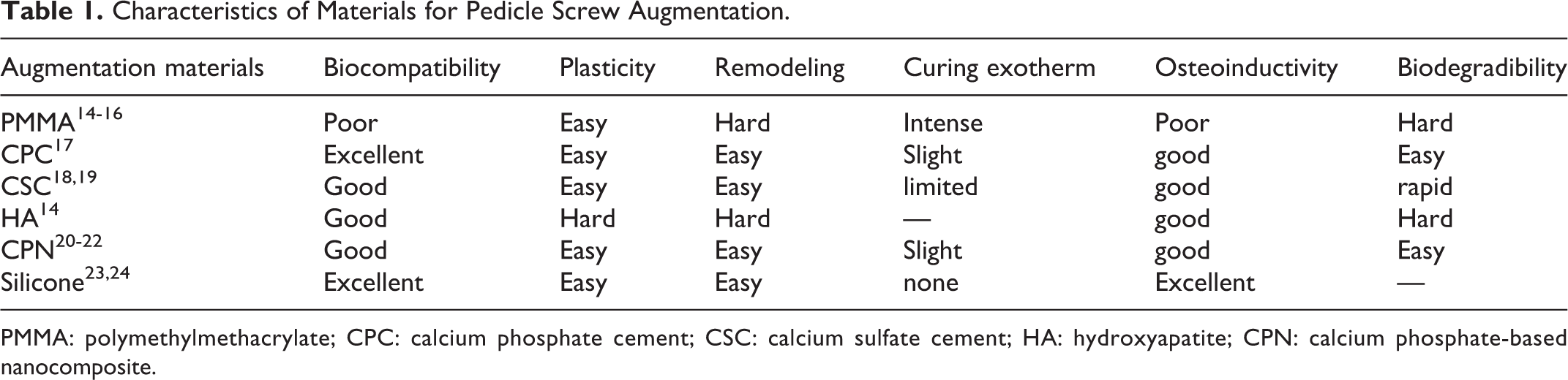
PMMA: polymethylmethacrylate; CPC: calcium phosphate cement; CSC: calcium sulfate cement; HA: hydroxyapatite; CPN: calcium phosphate-based nanocomposite.
Volume of the Injected Cement
Various volumes of injected cement tend to provide different screw stabilities, and many recent studies have tried to determine the ideal injection volume for the cement augmentation technique, but it is quite difficult to acquire homogeneous results to use in clinical practice. Firstly, most studies are focused on biomechanical testing, using testing materials such as artificial bones or cadaveric specimens that differ somewhat from physiological conditions. Secondly, the heterogeneity of design in testing pedicle screws and augmentation techniques is not suitable for direct clinical applicability of the conclusions. Thirdly, the optimal volume of cement varies among different spinal locations along with changes of anatomical structures and mechanical properties. Moreover, bone stock is also a factor for determining the ideal cement volume. As a consequence, further studies should focus on clinical trials that take mainstream pedicle screws as the subject and find out which volume could acquire little fixation failure and cement-related complications for different conditions. Fortunately, we can still get some insights from current biomechanical studies.
To a certain degree, there is a positive correlation between the fixation strength and the volume of cement. 28 Leichtle et al 29 found that 3 mL of cement significantly improved failure load compared to 1 mL regardless of the tested spinal regions. But Liu et al 28 contended that a volume increase of 0.5 mL did not lead to a significantly increased pullout strength. However, a volume increment of 1 mL played a significant role in the increment of pedicle screw stability. 30 As a result, it is logical to raise the cement quantity to increase screw anchorage in poorer bone stock as long as no cement leakage takes place. However, excessive cement volume should be avoided. Past a certain threshold, extra cement provides little additional benefit to screw holding power, and it may be bad for stability after long-term physiological load and carry with it a greater potential to cause cement-related complications such as cement leakage or even bone necrosis. Pishnamaz et al 31 found that a volume of 4.0 mL achieved little advantage over a volume of 1.5 mL regarding the immediate pullout strength without cyclic preloading, and the higher volume also suffered a larger reduction in screw holding power after cyclic loading. Fan et al 32 contended the optimal filling volume of cement was 75% of the pedicle screw trajectory (about 1.03 mL) for conventional pedicle screw (CPS) augmentation, and the use of excessive bone cement did not increase the fixation stability but increased the risk of leakage. This result is opposite to the study of Jia et al, 33 which found that full (100%) trajectory augmentation increased the pullout strength by 39%, cycles to failure by 18%, and failure loads by 12% compared with half (50%) trajectory augmentation using allograft bone particles. Perhaps the reason is that the full-trajectory allograft bone particles could increase the contact area of screw and augmentation materials, a factor that is less important when the injectable bone cement quantity reaches 75% of the full tractor volume.
With respect to spinal segments, it is common to use more cement for the larger size of the lumbar spine than the thoracic spine. Leichtle et al 29 found that 1 mL of cement could significantly enhance the pedicle screw holding power in the lower thoracic region, whereas in the lumbar regions this effect was only found in the 3 mL cement-augmented groups. Hence, they advised the use of at least 1 mL cement in the thoracic spine and 3 mL in the lumbar spine.
In addition to the volume of cement injected, the distribution of bone cement after augmentation is also an important factor determining screw stability. Another nonnegligible factor which limits the cement volume is the cement leakage. When the vertebrae are subjected to cement leakage, a smaller quantity of cement might be reasonable. But keeping the enhancement of screw strength in mind, it would be best to focus on identifying the cement distribution most favorable to the augmentation effect. Liu et al 34 showed that 2.0 mL of cement for cannulated screws with 4 lateral holes and 1.0 or 1.5 mL for screws with 6 holes could increase screw stability to the same extent as 1.5 mL in the traditional augmentation method. To decrease cement leakage, they suggested 1.0 mL of cement for screws with 6 lateral holes. If we worry about the potential rise of cement leakage, trying to lengthen the cement distribution along the screw stem would be a useful method to reduce the cement quantity but not the augmentation strength. 35 For severely osteoporotic vertebrae, it is difficult to maintain the cement augmentation effect, but we can increase the cement volume and optimize the cement distribution at the same time. Liu et al 30 showed that a higher cement volume (3 mL) coupled with a design of fenestrated pedicle screws (FPS) with 2 pairs of holes (which made the injected cement distribute around the pedicle region containing more cortical bone compared to the design with 6 holes) offered the best biomechanical augmentation effect in severely osteoporotic vertebrae. Their result, however, should be carefully evaluated before clinical adoption, because a large injected cement volume and a cement cloud more proximal to the spinal canal would carry higher potential of cement leakage in severely osteoporotic spines. The effects of cement volume on screw biomechanics are summarized in Table 2.
The Effects of Cement Volume on Screw Biomechanics.
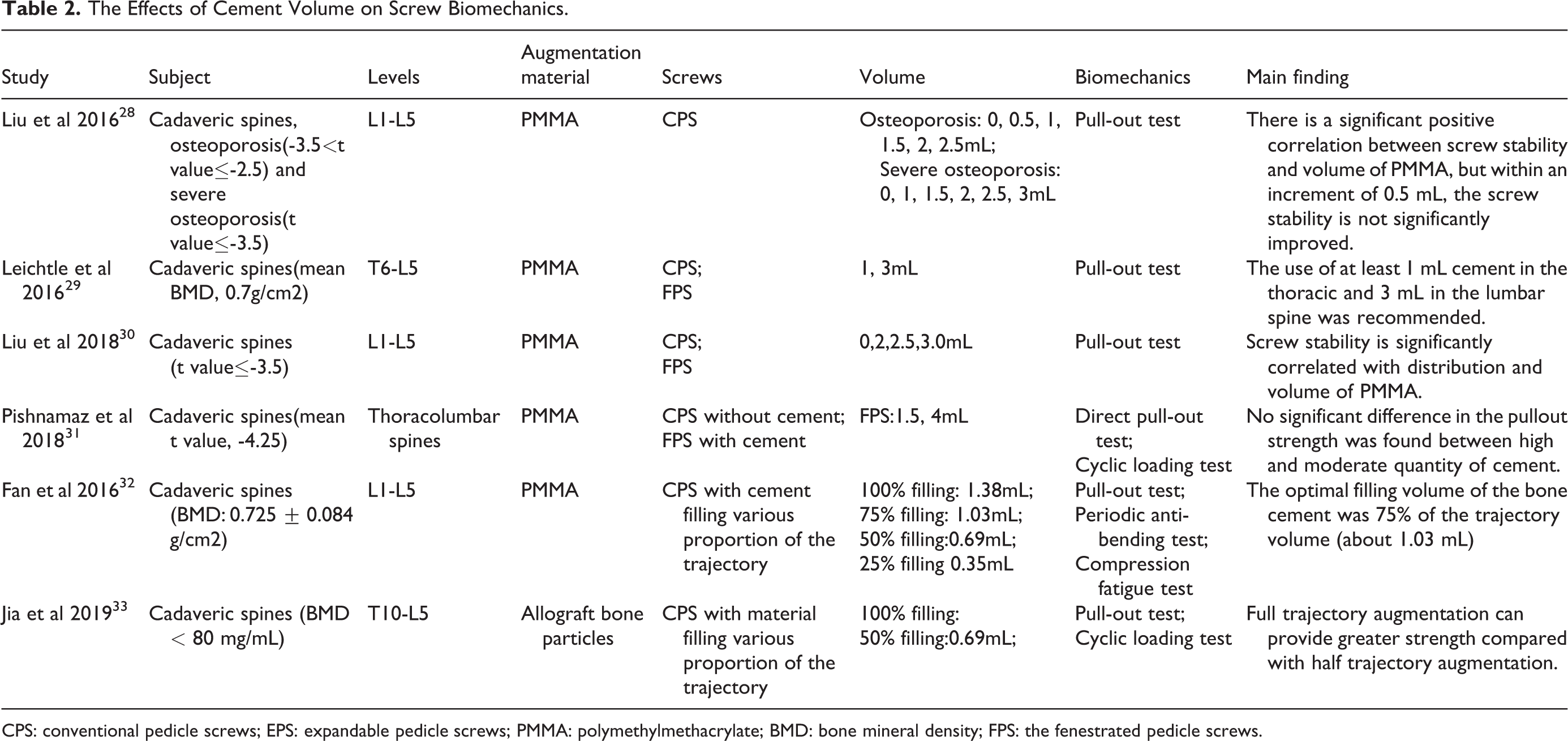
CPS: conventional pedicle screws; EPS: expandable pedicle screws; PMMA: polymethylmethacrylate; BMD: bone mineral density; FPS: the fenestrated pedicle screws.
Timing of Cement Injection
It is recommended that screws need to be inserted before the initiation of cement hardening. Masaki et al 36 found that screws inserted 10 minutes after cement mixing showed the lowest pullout strength in comparison to 2-minute and 5-minute groups, and cross sectional observations also revealed that CPC diffused deeper into the trabecular bone in the 5-minute group than in the 10-minute group. Similarly, Cho et al 11 reported that augmentation power tended to increase up to 4 minutes after CPC injection but decreased after 6 minutes. Consequently, 4 or 5 minutes after cement mixing might be optimal timing for the screws augmented by CPC.
That the anchorage of screws varies with the timing of bonding of screws and cement could be explained by the mechanism of pedicle screw loosening. Cemented screw loosening might be divided into 2 types: one is due to displacement occurring at the cement−bone interface, whereas the other is due to displacement occurring at the screw−cement interface. Linhardt et al 37 found a more pronounced increase in pullout strength for screws inserted immediately after soft cement injection than screws placed into cured cement 60 minutes after injection. For the soft cement group, the failure occurred at the cement−bone interface, whereas for the cured cement group, the failure occurred at the screw−cement interface. Indeed, Schmoelz et al 38 revealed that pedicle screws augmented after a reposition maneuver showed a significantly higher number of load cycles until screw loosening and had a smaller per cycle motion during loading test in comparison to screws cemented prior to the reposition maneuver. The stress x-rays illustrated that pedicle screws cemented after a reposition maneuver showed the same loosening mechanism as the cement-bone type, whereas the screws repositioned after augmentation showed the screw-cement loosening mechanism. The soft cement could help to form much closer contact in the screw−cement interface after screw insertion if no other disturbance exists before cement solidification. But when screws are inserted into cured cement or the contact between screws and cement is subjected to outside shaking interference during cement curing, it might lead to some potential cracks in an otherwise tight screw−cement interface.
Severity of Osteoporosis
As is well known, decreased BMD exerts a negative impact on pedicle screw fixation. The holding power of screws is also higher with the larger BMD value under the condition of cement augmentation.14,32 Liu et al 28 indicated that the maximum pullout strength for cement-augmented screws in osteoporotic lumbar vertebrae (T score ≤-2.5) was significantly higher than that in severely osteoporotic lumbar vertebrae (T score ≤-3.5) augmented with the same volume of cement. Fan et al 32 demonstrated the positive correlation between the BMD of lumbar vertebrae and the pullout strength of cemented screws, and illustrated that the maximum pullout strength was reduced by about 50 N as the BMD dropped by every 10 mg/mL.
Both the quality of cancellous bone surrounding a screw and the cement mass may affect the screw stability. Because most cemented pedicle screws tend to fail in the cement–bone interface under the axial pulling out force rather than the screw–cement interface 29 —which might be explained by the fact that the strength of the cement–bone interface is weaker than the screw–cement interface 39 —the higher quality of cancellous bone surrounding the cement mass would increase the strength of the screw–cement complex.
The injected cement serves to increase the local density of the screw trajectory to restore the original pedicle screw stability. Accordingly, the vertebrae of lower BMD that take on larger increment in local density after cement injection should derive more benefits from the cement augmentation. In other words, the benefits from cement augmentation decreased with increasing BMD. Weiser et al 40 recently observed that augmented screws exhibited a significant 50% increase in fatigue load compared to nonaugmented screws in osteoporotic specimens (BMD < 80 mg/cm3), whereas the cycles to failure only increased by 36% in the osteopenic BMD group (80–120 mg/cm3). As a result, a preoperative measurement of BMD by a micro-CT scanning or dual energy x-ray absorptiometry is necessary to predict the effect of augmentation, and there is no need to use cement with normal bone mass (BMD > 120 mg/cm3). 40 Of course, the targeted BMD should not be seriously low due to the potential for substantially increasing the risk of early screw loosening and cement leakage. It is found that early screw loosening might occur in sacral cement-augmented fixation if the BMD value is less than 0.6 g/cm2. 41
Different Pedicle Screw Designs
It is undoubted that pedicle screws with cement augmentation possess higher stability than those without cement augmentation for almost every kind of screw design,15,42 but the degree of augmentation effect differs with the various designs of pedicle screws.
Without cement augmentation, the screw parameters conducive to holding power enhancement are also favorable to the cement augmentation condition. For example, thicker screws without cement exhibit higher anchorage under the same circumstances. 43 This rule may still be applicable to the cement augmentation technique. Modifying the thread design is a useful method to enhance screw anchorage. For example, the dual lead dual cored (DLDC) screws could provide higher pullout strength than CPS due to the greater flank overlap area (FOA). Tolunay et al 44 reported that DLDC screws with cement augmentation exhibited the highest pullout strength values among CPS and FPS with or without cement augmentation in both artificial bone and bovine vertebrae. The newly designed screws equipped with higher biomechanical strength merit further biomechanical studies to determine whether the cement augmentation technique could further raise their stability.
As for cemented screws of different designs, it is difficult to decide which kind of pedicle screw is best. Without cement, expansive pedicle screws(EPS) which are referring to the screws with expansive fins at tip offer higher pullout strength than CPS, but Tai et al 42 found there is no statistical difference among CPS and EPS with cement augmentation. They also demonstrated that some design parameters of EPS, such as the number of fins and the extent of expansion, had little influence on screw-anchoring strength with or without cement. But Kiyak et al 15 drew an opposite conclusion that an increase in both fin number and length had a positive effect on the pullout strength of EPS with cement, which might be interpreted to mean that EPS with longer fins and a larger number of fins come into contact with a higher volume of cement and form a more complicated fins−cement structure. But the translation to clinical practice should be approached cautiously because of the use of synthetic bone in the 2 studies. Because screws with diverse designs form different screw-cement shapes, and the design parameters affect the cement volume dispersing into bone, it seems reasonable to believe the screw design could be an important factor influencing cement augmentation.
When it comes to the comparison between cemented CPS and FPS, a number of studies contended the cemented CPS were equipped with better stability than FPS.29,44,45 However, FPS are still frequently used as they are convenient to operate and can help to reduce operating time. Moreover, the design of cannulated screws with holes can control cement spread better than CPS and EPS 15 so as to decrease cement leakage. In addition, surgeons can decide which screws should be augmented according to specific needs. Furthermore, the augmentation of FPS could also be performed percutaneously, which achieves similar stability compared to traditional augmentation methods. 46 There are many types of FPS available, and they provide different amounts of stability after cement injection. The difference mainly originates from the cement mass location, cement distribution in vertebrae, geometrical shape of the cement cloud, and cement volume flowing out of the fenestrations. Firstly, the closer the cement cloud approaches to the pedicle, the higher the purchase of FPS would be, as the pedicle area contains a larger mass of cortical bone.30,34 Secondly, the geometrical shape of the cement cloud is an important factor influencing the stability of FPS. The irregular shape may be favorable to the screw’s purchase,47,48 and the larger maximum length of cement could contribute to the higher holding power. 48 In addition, with the same volume of injected cement, the cylindrical cement mass has better performance than the conical mass, which can be explained by the larger cement-bone interfacial area of the cylindrical cement.39,49
Another purpose of the improved FPS design is to increase intraoperative operability, such as reducing the injection pressure of cement. It is shown that the hollow part of the screw is the bottleneck to reducing perfusion pressure. When the inner diameter of the hollow part doubles, the injection pressure will drop by 59%. 50 To make up for the resulting loss of mechanical strength of the screws, an inner pin can be used to restore the screw strength.50,51 It is also reported that a larger diameter hollow with an inner pin could significantly increase the cement augmentation effect; the reason might be that the lower perfusion allows for a higher volume of cement injection. 51
Different Augmentation Technique
Commonly, the varieties of augmenting techniques rely on different pedicle screw designs. Generally, for solid screws, the cement should be injected into the prepared trajectory prior to the screw insertion, whereas cannulated screws with holes must be augmented by subsequent cement injection through the cannulation.
For pedicle screw loosening, the traditional augmentation is usually through the trajectory technique after the loosened screws are extracted. A modified technique called the expandable anchor bolt screw (EABS) technique is carried out with the following steps 43 : (1) The vacant pedicle hole after loose pedicle screw removal is filled with cement of 1-2 mL. (2) A small pilot screw is inserted into the toothpaste-like cement. (3) The pilot screw is removed after the cement is hardened, leaving a trajectory with inner thread. (4)A thicker permanent screw is inserted in and expand the cement thread to achieve stronger holding power. Kang et al 43 proved the EABS technique could achieve higher strength than original fixation and traditional trajectory augmentation, whereas the traditional trajectory technique got a similar holding power to the original fixation.
Another technique is to apply the cement into a balloon-created cavity prior to screw insertion, which is called vertebroplasty augmentation. The augmentation effect of this method varies with the location of cement in the vertebral bodies. Charles et al 52 found that the cement bolus around the proximal part of screws tend to have higher pullout forces. Cement augmentation via vertebroplasty has been shown to have a better effect than the injection technique. Schmoelz et al 24 compared the balloon cavity creation technique with the in situ augmentation technique with FPS and concluded that the balloon cavity creation technique could withstand more cyclic loads until loosening (9824 ± 1982 vs. 7401 ± 1644). However, the conclusion should be studied more rigorously in the future because the study used 2 different augmentation materials and 2 different pedicle screws when comparing the 2 augmentation techniques. Perhaps the better performance was a result of the combined effect of these variables.
As the length of the cement cloud has something to do with the resistance to axial forces, combining techniques could produce a better augmentation effect. Costa et al 35 revealed that cement injection through a fenestrated trocar and retrograde prefilling results in a higher pullout strength than the trajectory method, injection method, and the combination of the trajectory method with the vertebroplasty method.
Other Factors
In addition to the influential factors analyzed above, there are a few other factors affecting the cement augmentation technique. For example, the diversity in the structure of vertebrae is a mentionable factor capable of impacting the comparison results. It has been reported that the strength of cemented FPS is significantly better than that of CPS and even better than that of bicortical screws when it comes to the sacral screw fixation. 53 Its biomechanical stability could be equivalent to that of bicortical screws/sacral alar screws. 53
Complications of Cement Augmenting the Pedicle Screws
Cement leakage, pulmonary cement embolism (PCE), postoperative infection, and difficulty in revision surgery are considered as the main concerns related to cement augmentation technique.
The reported incidence of cement leakage in augmentation techniques was 62.30% to 81.68%, though most patients were clinically asymptomatic.54-60 If the cement leakage causes a PCE, the consequence might be fatal.61,62
Several factors would affect the occurrence of cement leakage and PCE. Firstly, higher cement volume and a larger number of pedicle screws augmented increase the likelihood of cement leakage and even PCE,32,63-65 Secondly, the bone quality and the integrity of the vertebrae play an important role. The patients with severe osteoporosis or spinal metastasis exhibit a higher risk of cement leakage.61,65,66 In addition, the distribution of cement also maters. The closer the cement cloud is to the pedicle, the higher the risk of leakage as there is more cancellous bone around the pedicle.61,66 Another important factor would be the viscosity of cement. It seems that there is a potential advantage of high-viscosity cement in terms of reducing the incidence of cement leakage and enhancing the screw fixation effect. 67 As for spinal level, Janssen et al 61 reported the risk of cement leakage was not affected by which spinal segments are augmented. However, it is found patients received instrumentation of thoracic or thoracolumbar spine had an increased risk to suffer from PCE, whereas the lumbar spine had a lower risk, 59 which might be explained by the thoracic location was more adjacent to the pulmonary artery. Before the cement augmentation technique is performed, these risk factors of cement leakage should be taken into account. Erdem et al 68 recommended cementing the strategic vertebrae alone instead of all segments, which are proved to provide adequate strength for screw attachment and decrease the volume of cement, subsequently reducing the risk of cement leakage and PCE. During the operation, cement injection should be performed under continuous fluoroscopy to avoid high-volume leakage, and be ceased as soon as leakage is noticed or suspected. To deal with systematic cement leakage, a second surgery, or an additional decompression to remove epidural cement might be required.54,69
Since the commonly used PMMA is neither osteoinductive nor biodegradable, the persistent PMMA is likely to give rise to deep and superficial infection. 70 When it comes to the revision surgery due to infection, the instrumentation does not have to be removed if the intravenous anti-infection treatment works well58,70
Another concern is the difficulty in screw extraction during revision surgery may pose a danger to the patient with osteoporosis. But 2 studiesdemonstrated that pedicle screws can be easily and safely removed after augmentation with PMMA58,71 Although a high torque force was needed in the revision of cement-augmented pedicle screws, there was no relationship between the volume of the injected PMMA and the extraction force. 72 When inserted into the pedicle again, the new screws would better to have a larger diameter than the removed, since it is difficult to augment again because of the sclerotic wall of the removed screws. 72
Conclusion
Biomechanical studies have identified several factors that impact the effect of cement augmentation in osteoporotic spines. These include the type of augmentation material, the volume of injected cement, the timing of augmentation, the severity of osteoporosis, the design of pedicle screw, and the specific augmenting technique, among others. But the final effect of cement augmentation is affected by the combination of factors, suggesting that we should comprehensively analyze the combined effects of these influential factors as well as consider the cement leakage risks when we design new pedicle screws or adopt findings from biomechanical studies into clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Natural Science Foundation of Beijing (no. 7212117) to HS.