
Abstract
Study Design:
A retrospective study.
Objectives:
Curve flexibility in patients with adolescent idiopathic scoliosis (AIS) can be evaluated using different techniques. This study aimed to determine whether the combination of side-bending (SB) and traction (TX) radiographs influences preoperative planning for AIS than either radiograph alone.
Methods:
Thirty-two spine surgeons were asked to review 30 AIS Lenke type 1 cases and select an upper instrumented vertebra (UIV) and lower instrumented vertebra (LIV) for the posterior spinal instrumentation of each case. Each rater reviewed the cases 3 times in each round. The raters were provided with the full-length posteroanterior (PA) and lateral standing and SB radiographs for round 1; PA, lateral, and TX radiographs for round 2; and PA, lateral, SB, and TX radiographs for round 3. Intra- and inter-rater reliabilities were evaluated using Kappa statistics.
Results:
The intra-rater reliability for UIV and LIV was 0.657 and 0.612 between rounds 1 and 2, 0.634 and 0.692 between rounds 1 and 3, and 0.659 and 0.638 between rounds 2 and 3, respectively, which indicated substantial agreement between rounds. The inter-rater kappa reliabilities for UIV and LIV selection were 0.103 and 0.412 for round 1, 0.121 and 0.380 for round 2, and 0.125 and 0.368 for round 3, indicating slight to moderate agreement between raters.
Conclusions:
Whether raters used either SB or TX radiography, or both in addition to PA and lateral standing radiographs, did not influence the decision making for UIV or LIV of AIS Lenke type 1 surgery.
Keywords
Introduction
Curve progression after skeletal maturity is expected in patients with adolescent idiopathic scoliosis (AIS) with curves >30°. 1 Currently, the treatment recommendation for correcting the curve and preventing progression is surgical intervention. 2 The factors generally agreed upon as indications for surgical decision making include coronal curve magnitude, skeletal maturity, the progression of deformity, global alignment, and the presence of neurologic pathology.3,4 In addition, pelvic obliquity, shoulder balance, and neck tilt are also considered.5-8
In patients with Lenke type 1 AIS, preoperative planning includes evaluation of the flexibility of the main thoracic curve as well as the lumbar and proximal thoracic compensatory curves. The flexibility of the curve will help determine the type of surgical procedure to be performed, whether an anterior release is necessary, as well as the appropriate levels of instrumentation and fusion. 9 Side-bending (SB) radiographs have been widely used to evaluate flexibility, while traction (TX) radiographs have been reported to be more effective in larger curves.3,10,11 Although some surgeons use both SB and TX to determine curve flexibility, some surgeons use either one or the other. It would be beneficial to patients in terms of radiation exposure and health economics if the number of required radiographs were reduced without influencing or reducing the comprehensive capacity to assess the curve. The expert consensus is that most surgeons prefer SB to TX radiography for relatively mild curves with a Cobb angle between 40° and 70°, while TX radiography is preferred over SB for rigid or stiffer curves with a Cobb angle between 70° and 90°. 12 This expert opinion is consistent with previous reports on the usefulness of TX radiographs for large curves.3,10,11 The purpose of this study was to determine whether the combination of SB and TX radiographs is more informative for preoperative planning for AIS than either SB or TX radiographs alone.
Materials and Methods
After receiving institutional review board (IRB) approval, a retrospective review of medical records and radiographs of consecutive patients diagnosed with AIS, who were managed surgically at a single institution from 2009 to 2015, was performed. The IRB approval was for the retrospective evaluation of medical data and radiographic information of patients with AIS. Thirty AIS patients with Lenke type 1A, 1 B, and 1C curves, with preoperative supine SB radiograph and maximum TX radiograph, were included in this study. Patients diagnosed with non-idiopathic scoliosis were excluded from the study. For each case, information regarding age, sex, as well as comprehensive radiographic evaluation consisting of posteroanterior (PA) and lateral standing radiographs, and/or SB radiograph and/or TX radiograph was extracted. From September 2016 to February 2017, an email survey was sent to experienced spine deformity surgeons in Japan and the United States who were known to the authors. Surgeons were asked to decide on the upper instrumented vertebra (UIV), lower instrumented vertebra (LIV) level, and whether they would perform an anterior release. In the first round, they were asked to evaluate the cases with PA, lateral standing radiographs, and SB radiographs. We also provided data regarding age and sex to the surgeons. Two weeks later, for the second round, the cases were randomly reordered, and surgeons were asked to evaluate the cases with PA and lateral standing radiographs, and the TX radiograph. Two weeks later, for the third round, cases were randomly reordered again, and the surgeons were asked to evaluate the cases with PA and lateral standing radiographs, SB, and TX radiographs. The number of AIS patients to be evaluated by surgeons was set at 30, a number based on past literature, which also took into account the exclusion of cases during the analysis. 13 The number of surgeons to be evaluated was similarly determined based on previous literature. 13 To account for missing responses, 37 spine surgeons were asked to complete the survey.
Radiographic Evaluation
SB radiographs were taken with the patients voluntarily bending maximally while in the supine position. The surgeon or one of the spine fellows performed the supine TX with the patient’s arms or neck and with the legs pulled to stretch out the spine. Cobb angles in preoperative standing, preoperative SB and preoperative maximum TX radiographs, and thoracic kyphosis (T5-12) were measured and labeled on radiographs.
Statistical Analysis
All values are expressed as the mean ± standard deviation (SD). Intra-rater reliabilities for the presence of UIV or LIV selection were calculated using kappa statistics between round 1 (PA and lateral standing, and SB radiograph) and round 2 (PA and lateral standing, and TX radiograph), round 1 (PA and lateral standing, and SB radiograph) and round 3 (PA and lateral standing, SB, and TX radiograph), as well as between round 2 (PA and lateral standing, and TX radiograph) and round 3 (PA and lateral standing, SB, and TX radiograph). Kappa statistics for UIV or LIV selection were calculated with quadratic weights to give importance to disagreements closer together at the vertebral level. Inter-rater reliabilities for UIV or LIV selection in each round were calculated using the intra-class correlation coefficient (ICC). Only a single evaluation in each round was used to determine inter-rater ICC. As the raters had not been randomly selected, ICC case 3 was used. Kappa or ICC of 0 to 0.2 represent slight agreement, 0.21 to 0.4 fair agreement, 0.41 to 0.6 moderate agreement, 0.61 to 0.8 substantial agreement, and 0.81 to 1 excellent agreement. 14 The statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 24.0; SPSS, Chicago, IL, USA).
Results
Cases
The mean age of the 30 AIS cases was 13.9 years, with 4 males and 26 females. The curve type included Lenke type 1A (n = 12, 40.0%), type 1 B (n = 5, 16.7%), and type 1C (n = 13, 43.3%). The mean Cobb angle of the main thoracic curve on the preoperative PA standing, SB, and TX radiographs were 57.9 ± 10.7°, 31.1 ± 10.6°, and 34.2 ± 9.0°, respectively. The mean thoracic kyphosis (T5-12) was 28.0 ± 10.0°. The intra-observer ICCs for the Cobb angle of the main thoracic curve on the PA standing, SB, and TX radiographs, and thoracic kyphosis were 0.923, 0.965, 0.919, and 0.867, respectively.
Reviewers
Responses were received from 32 of the 37 (86%) experienced spine deformity surgeons who were invited to complete the questionnaire. They included 16 American spine surgeons from 11 institutions and 16 Japanese spine surgeons from 8 institutions. All 32 attending spine surgeons practice at academic institutions and routinely care for patients with AIS. Thus, the complete evaluation of this case series yielded a total of 960 discrete UIV, LIV, and anterior release for each round. The intra-rater kappa reliability for UIV and LIV selection of the 30 AIS patients was as follows: round 1 (PA and lateral standing, and SB radiograph) versus round 2 (PA and lateral standing, and TX radiograph) reliability was 0.657 and 0.612; round 1 (PA and lateral standing, and SB radiograph) versus round 3 (PA and lateral standing, SB, and TX radiograph) reliability was 0.634, and 0.692 respectively; round 2 (PA and lateral standing, and TX radiograph) versus round 3 (PA and lateral standing, SB, and TX radiograph) were 0.659 and 0.638, respectively, indicating substantial agreement between rounds (Table 1). Of a total of 960 responses, only 39 (4.1%) in the first round, 19 (2.0%) in the second round, and 21 (2.2%) in the third round responded that they would perform an anterior release.
Intra-Rater Weighted Kappa Coefficients in all Patients.

PA, posteroanterior; SB, side-bending radiograph; TX, traction radiograph; UIV, upper instrumented vertebrae; LIV, lower instrumented vertebrae.
The comparisons of intra-rater weighted kappa statistics stratified by curve type are summarized in Table 2. In Lenke 1A, 1 B, and 1C, the intra-rater kappa reliabilities for UIV or LIV selection showed substantial agreement between round 1 (PA and lateral standing, and SB radiograph) and round 2 (PA and lateral standing, and TX radiograph) except for LIV selection in Lenke 1 B and 1C.
The Comparison of Intra-Rater Weighted Kappa Statistics Stratified by the Lumbar Curve Type.
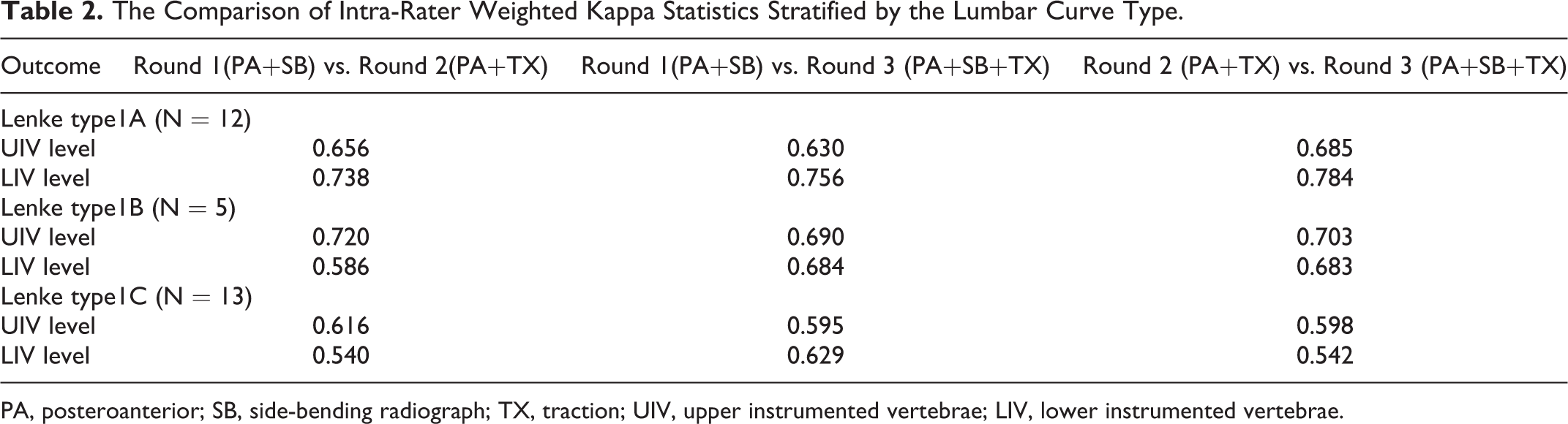
PA, posteroanterior; SB, side-bending radiograph; TX, traction; UIV, upper instrumented vertebrae; LIV, lower instrumented vertebrae.
Across all surgeons, the inter-rater reliability kappa statistics for UIV or LIV selection for each round were as follows (Table 3): round 1 reliabilities (PA standing, lateral standing, and both SB radiograph) were 0.103 and 0.412; round 2 reliabilities (PA standing, lateral standing, and TX radiograph) were 0.121 and 0.385; round 3 reliabilities (PA standing, lateral standing, both SB radiograph, and TX radiograph) were 0.125 and 0.368, indicating slight to moderate agreement between raters.
Inter-Rater Observer Reliability.
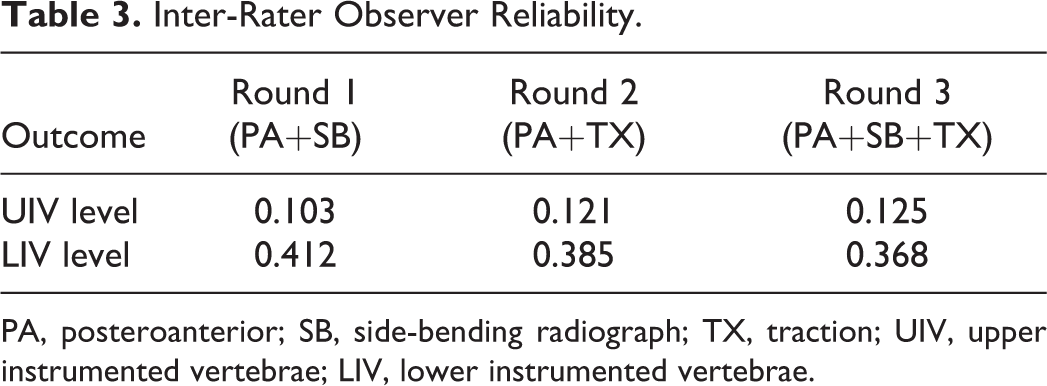
PA, posteroanterior; SB, side-bending radiograph; TX, traction; UIV, upper instrumented vertebrae; LIV, lower instrumented vertebrae.
Discussion
Surgeons use multiple radiographs prior to surgery to determine the flexibility of the spinal curve. In turn, the degree of flexibility helps guide the surgical approach and the selection of fusion levels. Curve flexibility is often evaluated using SB or TX radiographs, but some surgeons utilize both. In the evaluation of curve flexibility between SB and TX, TX is superior in cases with a large Cobb angle of 60° or more in the main thoracic curve, while SB is superior in AIS patients with a relatively small curve. In the thoracolumbar and lumbar curves, SB is generally superior in curve flexibility evaluation. 11 Whether the combination of SB and TX radiographs provides more information for preoperative planning for AIS than either SB or TX radiography alone has not been examined previously. In this study, a total of 3 surveys were conducted with 32 experienced spine surgeons to examine the usefulness of the combination of SB and TX radiographs to evaluate pre-operative curve flexibility in AIS patients. UIV and LIV selection by the individual surgeon showed substantial agreement whether SB or TX alone was used, or both were used as a flexibility evaluation. This means that the use of either SB or TX radiographs in addition to PA and lateral standing radiographs did not influence the decision making for UIV or LIV level of AIS Lenke type 1 surgery. Considering the above results, it is not always necessary to use both SB and TX to assess flexibility, and it may be up to the individual surgeon’s policy to decide whether to use SB or TX radiographs. It would potentially be beneficial to patients in terms of radiation exposure and health economics since the number of radiographs taken can be decreased. The average patient contribution payment for full spine radiography in Ontario (Canada) is reported to be approximately $25 to $75, respectively, depending on the number of views. 15 The entrance surface doses for non-filtered radiography of anteroposterior and lateral images of the whole spine are reported to be 0.31 and 0.93 mGy, respectively. 16 Radiation exposure for AIS patients may increase lifetime cancer risk. 17 However, not all spine surgeons are fully aware of the potential cancer risk in patients associated with radiation exposure.18,19 Therefore, surgeons must consider reducing radiation exposure as much as possible, including during preoperative planning.
Considering the curve type, the intra-rater agreement for UIV and LIV selection was similar. In other words, it would seem that the use of both SB and TX radiographs did not provide more information for preoperative planning compared to either one alone by the lumbar modifier in the Lenke 1 curve.
Remarkably, the inter-rater reliability for LIV selection was fair to moderate. Several studies have been published to guide LIV selection, such as selecting the stable vertebral body, 20 neutral vertebrae, 21 last touch vertebral body, 22 last substantially touching vertebra body, 23 or stable vertebrae in TX radiograph. 24 However, there is still no consensus. In addition, it was reported that radiographic determination of the end vertebrae, neutral vertebrae, and stable vertebrae demonstrated poor interobserver reliability. 25 For this reason, LIV selection differs from surgeon to surgeon, and it may have led to a low inter-rater agreement for LIV selection in this study.
The inter-rater reliability for UIV selection was much worse than that for LIV. This may be because there are no widely accepted guidelines for UIV selection in AIS surgery. Rose et al. suggested extending the fusion to T2 when the left shoulder is high, fusion to T2 or T3 when the shoulder is level, and fusion to T3 when the right shoulder is higher. 26 In recent years, methods using the UIV tilt angle 7 or the line between the center of the spinous process of C7 and that of the spinous process of the LIV 27 have also been reported. Conversely, there are reports that shorter segment fusion is recommended because postoperative shoulder imbalance is corrected spontaneously.28,29 The extremely low inter-rater reliability for selecting the UIV and LIV levels, even if SB or TX alone was used, or both were used as a flexibility evaluation is also problematic. It is important to perform long-term postoperative follow-up and create optimal global guidelines for fusion selection.
As there were very few raters who replied that they would do anterior release, an analysis of the impact of both the SB and TX and each alone on the decision to perform an anterior release could not be adequately performed. A recent study has shown that even in AIS patients with a rigid thoracic curve, a posterior-only approach with an all-pedicle screw construct could achieve a similar curve correction as posterior spinal fusion with anterior release by increasing the implant density. 30 Almost all raters preferred the procedure with the posterior approach alone for AIS Lenke type 1 in this study.
This study has several limitations. First, the method of determining the fusion segments in AIS surgery varied greatly among surgeons. Second, some surgeons do not use TX radiographs in their routine practice. Third, there may not be evidence that consensus decision-making by experienced international spine surgeons is appropriate. Thus, the results of this study of 32 experienced spine surgeons from Japan and the United States are not necessarily representative of all spine surgeons. However, this study investigated whether there is a consensus of opinion on UIV or LIV selection under different flexibility assessment methods among spine surgeons having varied spine training experiences. There was a selection bias in our choice of surgeons, which may have affected the results. Fourth, the UIV and LIV determination in this study were not related to postoperative outcomes. Fifth, a difference in the choice of 1 or 2 levels of UIV may not affect the clinical outcome. Sixth, the 30 AIS cases had relatively flexible curves and may not have been an appropriate cohort for this study. Future research should also investigate the differences in UIV and LIV selection between different flexibility assessment methods for larger and stiffer curves. Seventh, with regard to inter-rater reliability, round 3, unlike rounds 1 and 2, has been evaluated once before, so the surgeons are not independently evaluating the SB and TX images, and potential bias may exist.
Conclusions
In our study, the use of either SB or TX radiography, or both, in addition to PA standing radiograph, did not influence the preoperative decision making for UIV or LIV level of AIS Lenke type 1 surgery. It is not always necessary to use both SB and TX to assess flexibility, and it may be up to the individual surgeon’s policy to decide whether to use SB or TX. It would potentially be beneficial to patients in terms of radiation exposure and health economics since the number of radiographs taken can be decreased.
Footnotes
Acknowledgment
This study was reviewed and approved by the University of Louisville Institutional Review Board. IRB# 16.0453. The authors would like to express great thanks to Dr. Kamal Ibrahim, Dr. B. Stephens Richards, Dr. Hiroshi Taneichi, Dr. Lawrence Haber, Dr. Jun Takahashi, Dr. Satoshi Inami, Dr. Daisuke Togawa, Dr. Mladen Djurasovic, Dr. Charles Crawford, Dr. Kota Watanabe, Dr. Naobumi Hosogane, Dr.Hiroshi Moridaira, Dr. Tomohiko Hasegawa, Dr. Mitsuru Yagi, Dr.Tetsuro Ohba, Dr. Yu Yamato, Dr. Go Yoshida, Dr. Sho Kobayashi, Dr. Shin Oe, Dr. Tatsuya Yasuda, Dr. Kirk Owens, Dr. Michael Kelly, Dr. Patrick Sugrue, Dr. Betty Norheim, Dr. Calvin Kuo, Dr. Paul Celestre, Dr. Paul Rubery, and Dr. Kathryn McCarthy for their excellent cooperation of this project. The authors would like to express great thanks to Dr. Morio Matsumoto, Dr. Hirotaka Haro, and Dr. Yukihiro Matsuyama for recommending raters. We would like to thank Editage for English language editing.
Authors’ Note
SDG, JRD, JLG and LYC are employees of Norton Healthcare. JRD receives consulting fees, holds patents from and receives royalties from Medtronic; is on the editorial review board of JBJS Highlights, Spine, Spine Deformity, JAAOS and Global Spine; is a member of the SRS Board. SDG holds patents from and receives royalties and consulting fees from Medtronic. JLG receives consulting fees from Medtronic, Acuity, K2M/Stryker, NuVasive and Mazor, and royalties from Acuity and NuVasive. LYC is a Member, Editorial Advisory Board, Spine and Spine Journal, University of Louisville Institutional Review Board, Scoliosis Research Society Research Committee; receives research funds from the Orthopedic Research and Educational Fund, Norton Healthcare, Scoliosis Research Society; received funds for travel from Association for Collaborative Spine Research and the University of Southern Denmark, University of Louisville Institutional Review Board; received consulting fees from Washington University in St. Louis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Relevant financial activities outside the submitted work: board membership, consultancy, employment, grants, payment for lectures, travel/accommodations/meeting expenses, patents, royalties, stocks, and donated fund laboratory.