
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Epidemiologic studies suggest that the prevalence of moderate to severe obstructive sleep apnea (OSA) is increasing. OSA has been linked to increased rates of postoperative complications following surgery. Large studies, however, regarding surgical outcomes in this patient population, particularly in the spine literature, are limited. Consequently, the purpose of this study was to assess the prevalence of and postoperative risks conferred by OSA in the elective spine population.
Methods:
Using data from the National Inpatient Sample from 2008 to 2012, an estimated 56 372 (5.1%) patients with OSA undergoing elective cervical and thoracolumbar spine surgery were selected and compared to 1 052 837 patients without OSA undergoing the same procedures. Our primary outcome measures included postoperative complication rates, inpatient mortality, length of stay, and total hospital charges.
Results:
Patients with OSA were, on average 2.6 years older than those without OSA (P < .001) and had a higher comorbidity burden. The prevalence of OSA increased between 2008 and 2012 from 3.5% to 6.8%; P < .001. OSA was associated with a 3-fold increase in major complications (P < .001) and was confirmed as an independent risk factor for major complications based on multivariate analysis (odds ratio [OR] = 2.82; 95% CI = 2.59-2.79; P < .001). Rates of deep venous thrombosis were doubled in patients with OSA. OSA was determined to be an independent predictor of pulmonary complications (OR = 2.69; 95% CI = 2.59-2.79; P < .001). OSA did not increase the risk of postoperative mortality.
Conclusions:
Patients with OSA often have multiple concomitant comorbidities and consequently are at increased risk of experiencing a more difficult postoperative course following elective spine surgery. Specifically, increased risks of pulmonary complications and deep venous thrombosis should be anticipated.
Introduction
Obstructive sleep apnea (OSA) is characterized by periods of airway narrowing or occlusion causing fragmented sleep patterns in patients. It is the most common sleep-breathing disorder and is associated with poor health status. Concomitant hypertension, heart failure, cardiac disease, stroke, diabetes, and psychiatric illnesses are common in patients with severe OSA. 1 -8
Epidemiologic studies suggest that the prevalence of moderate to severe OSA is increasing, with current rates reported at 10% to 20%. 9 -11 It is estimated, however, that up to 80% of patients with moderate to severe OSA may remain undiagnosed and subsequently go untreated. 10 While OSA has been linked to increased rates of postoperative complications following surgery in numerous studies, many of these studies have been limited to small sample sizes and to single institutions. Large studies, regarding surgical outcomes in this patient population, particularly in the spine literature, are limited.
Despite existent guidelines for preoperative screening of this patient population, routine screening for OSA has traditionally been costly and is not common practice. With an increasingly cost-conscious health care environment, it is important to appropriately evaluate the risk of elective spine surgery in this patient population to help determine whether or not screening for OSA would be financially worthwhile.
The purpose of our study was to identify the national prevalence of OSA in the elective spine population and to contrast the outcomes of patients with OSA against outcomes in the normal population. Our hypothesis was that patients with OSA would have higher rates of postoperative complications and in-hospital mortality risk following elective spine surgery.
Materials and Methods
Study Population Selection
A retrospective cohort study was performed using the National Inpatient Sample (NIS) from 2008 to 2012. The NIS is a stratified survey of approximately 20% of all US hospitals that includes inpatient data for more than 7 million annual admissions. Sampling weights are provided to provide estimates of 100% of all US hospital discharges. All numbers presented in this study are national estimates based on NIS sampling weights. Institutional review board approval was not required for this study due to the de-identified nature of this national database.
Inclusion and Exclusion Criteria
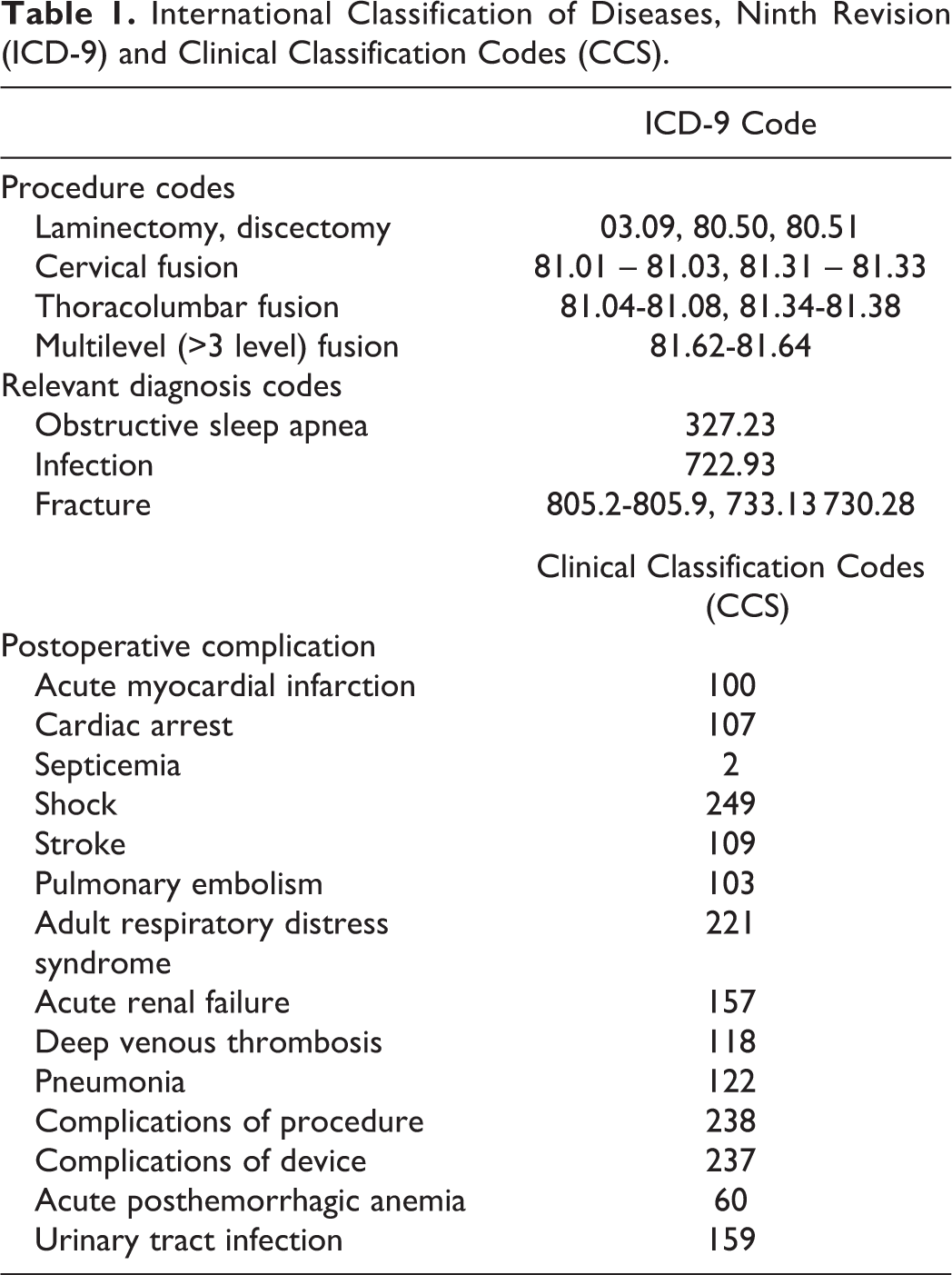
All patients undergoing elective spine surgeries were selected using International Classification of Disease, Ninth Revision, Clinical Modification procedure codes (ICD-9-CM) codes. 12 All emergency admissions, transfers from outside facilities, infections, tumors, and fractures were excluded to isolate the typical elective population. Two cohorts were created based on the diagnosis of OSA. All ICD-9 codes used are presented in Table 1. Our finalized study group contained a total of 220 036 patients without OSA and 11 503 patients with OSA, representing a national estimate of 1 052 837 patients without OSA and 56 372 patients with OSA. All numbers presented in this study from hereafter are national estimates based on NIS sampling weights.
International Classification of Diseases, Ninth Revision (ICD-9) and Clinical Classification Codes (CCS).
Patient Characteristics
Basic demographic information including age, sex, and race as well as payer status were extracted from the NIS database. Preoperative comorbidities were identified using ICD-9 and DRG (Diagnosis-related Group) coding with the use of the Healthcare Cost and Utilization Project (HCUP) Comorbidity Software. This software package identifies 29 patient comorbidities based off of an Elixhauser Comorbidity Index. A Charlson Comorbidity Index (CCI) score was then created with higher cumulative scores representing a higher comorbidity burden. 13 -17
Outcomes
Primary outcomes assessed included postoperative complications, inpatient mortality, and length of stay. Complications were identified using the clinical classifications software (CCS) provided by HCUP. The clinical classifications software groups together related ICD-9 coded postoperative complications to facilitate statistical analysis. These codes are provided in Table 1. Complications were classified as major or minor similar to previously published work. 14,18,19 Major complications included cardiac complications (acute myocardial infarction and cardiac arrest), septicemia, septic shock, stroke, respiratory failure, need for reintubation or mechanical ventilation, and pulmonary embolism. Minor complications included deep venous thrombosis, pneumonia, surgical complications, postoperative anemia, and urinary tract infections. Pulmonary complications were separately defined any of the following: postoperative respiratory failure, pneumonia, or need for reintubation or mechanical ventilation. Finally, a comparison of total hospital charges between the 2 cohorts was made.
Statistical Analysis
Patient characteristics and inpatient outcomes for both groups were analyzed with the use of chi-square and Student t tests. A chi-square test was used for categorical variables, and an independent Student t test was used to assess continuous variables. Only more commonly occurring comorbidities (occurring in >1% of our sample population) were found to have statistically significant associations with the outcome of interest based on univariate analyses and were consequently included in our multivariate analyses. Multivariate logistic regression analysis was then used to identify independent predictors of postoperative complications and inpatient mortality and to control for potential confounders including age, sex, race, hospital size, and hospital type. These calculated associations were reported as multivariate odds ratios (OR) with 95% confidence intervals (CIs). P < .05 was set as our measure of statistical significance.
Results
Patient Characteristics and National Prevalence of OSA
A total of 1 052 837 patients without OSA, and 56 372 (5.1%) patients with OSA underwent elective spine surgery from 2008 to 2012 (P < .001). The prevalence of OSA increased from 3.5% in 2008 to 6.8% in 2012 (P < .001). Patients with OSA were slightly older; 60.3 years (SD = 11.9), compared with mean age of 57.6 years (SD = 15.0) in patients without OSA (P < .001). Patients with OSA were more likely to be male (65.5% with OSA compared with 50.1% without OSA; P < .001). Overall, 22% of the patient population underwent elective cervical procedures while the remaining 78% underwent thoracolumbar surgeries (P < .001). These and additional figures are presented in Table 2.
Patient Characteristics by Obstructive Sleep Apnea (OSA) Status.
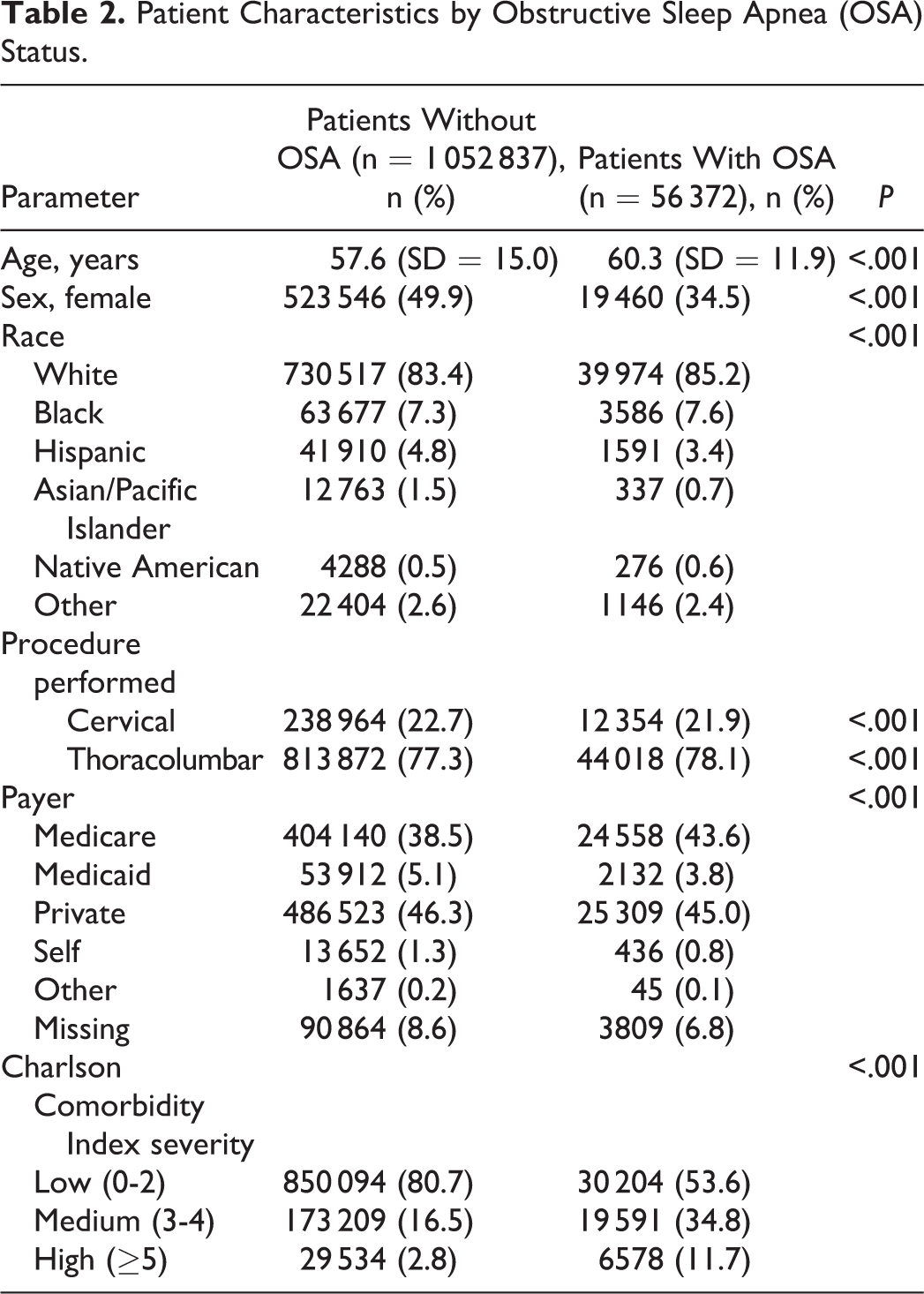
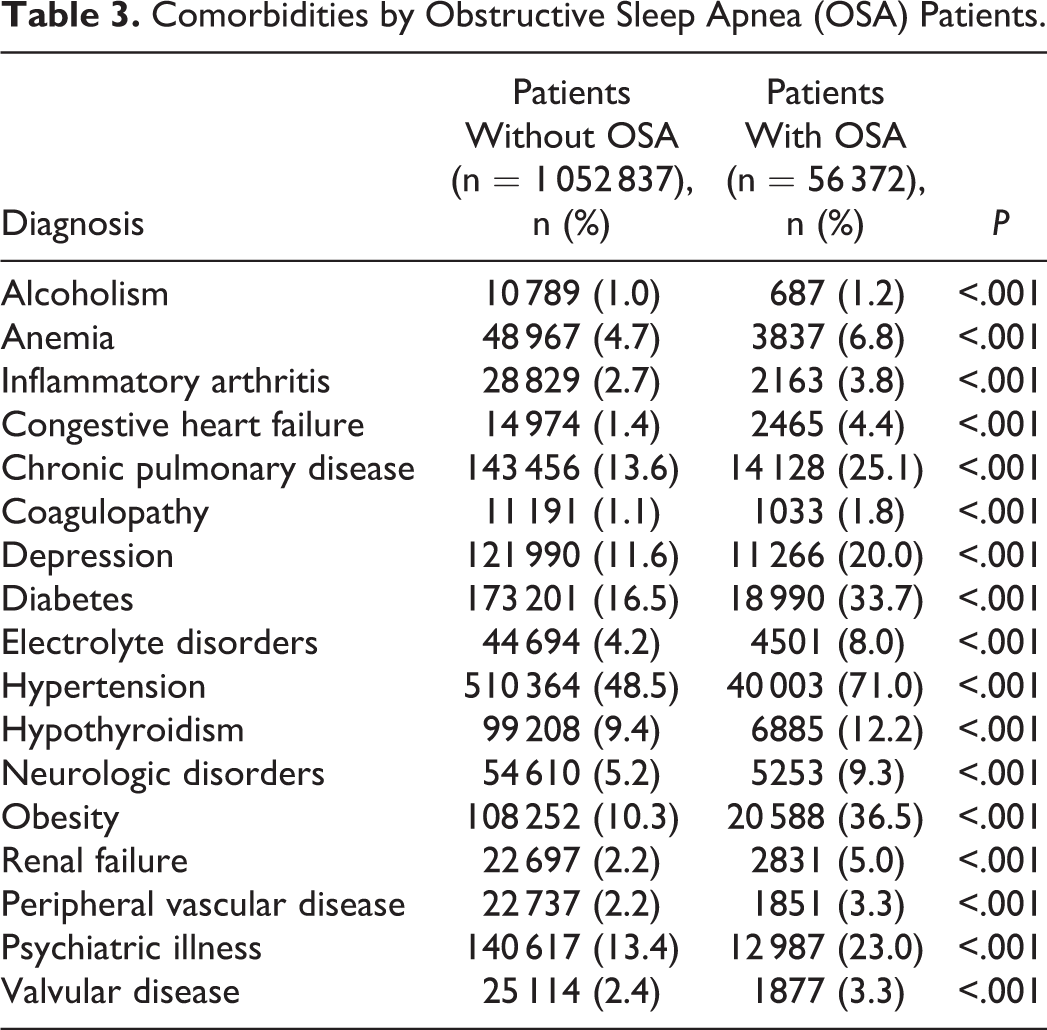
As expected, OSA was associated with a higher CCI severity score (Table 2; P < .001). A significantly higher proportion of patients with OSA carried the following diagnoses when compared to patients without OSA: hypertension (71% compared with 48.5%; P < .001), obesity (36.5% compared with 10.3%; P < .001), diabetes (33.7% compared with 16.5%; P < .001), chronic obstructive pulmonary disease (COPD) (25.1% compared with 13.6%; P < .001), psychiatric illnesses (23% compared with 13.4%; P < .001), and congestive heart failure (4.4% compared with 1.4%; P < .001). The remaining comorbidities and their associations are shown in Table 3.
Comorbidities by Obstructive Sleep Apnea (OSA) Patients.
Postoperative Morbidity and Mortality
OSA was associated with a 3-fold increase in major postoperative complications (7.9% compared with 2.0%; P < .001). Please refer to Table 4 for rates of specific complications. Multivariate analysis identified OSA as an independent predictor for major complications (OR = 2.82; 95% CI = 2.59-2.79; P < .001). Minor postoperative complication rates were also increased in patients with OSA (Table 4). Notably, the rate of deep venous thrombosis was higher in patients with OSA when compared with those without OSA (4.0% compared with 2.2%; P < .001).
Univariate Analysis: Outcomes by Obstructive Sleep Apnea (OSA) Status.
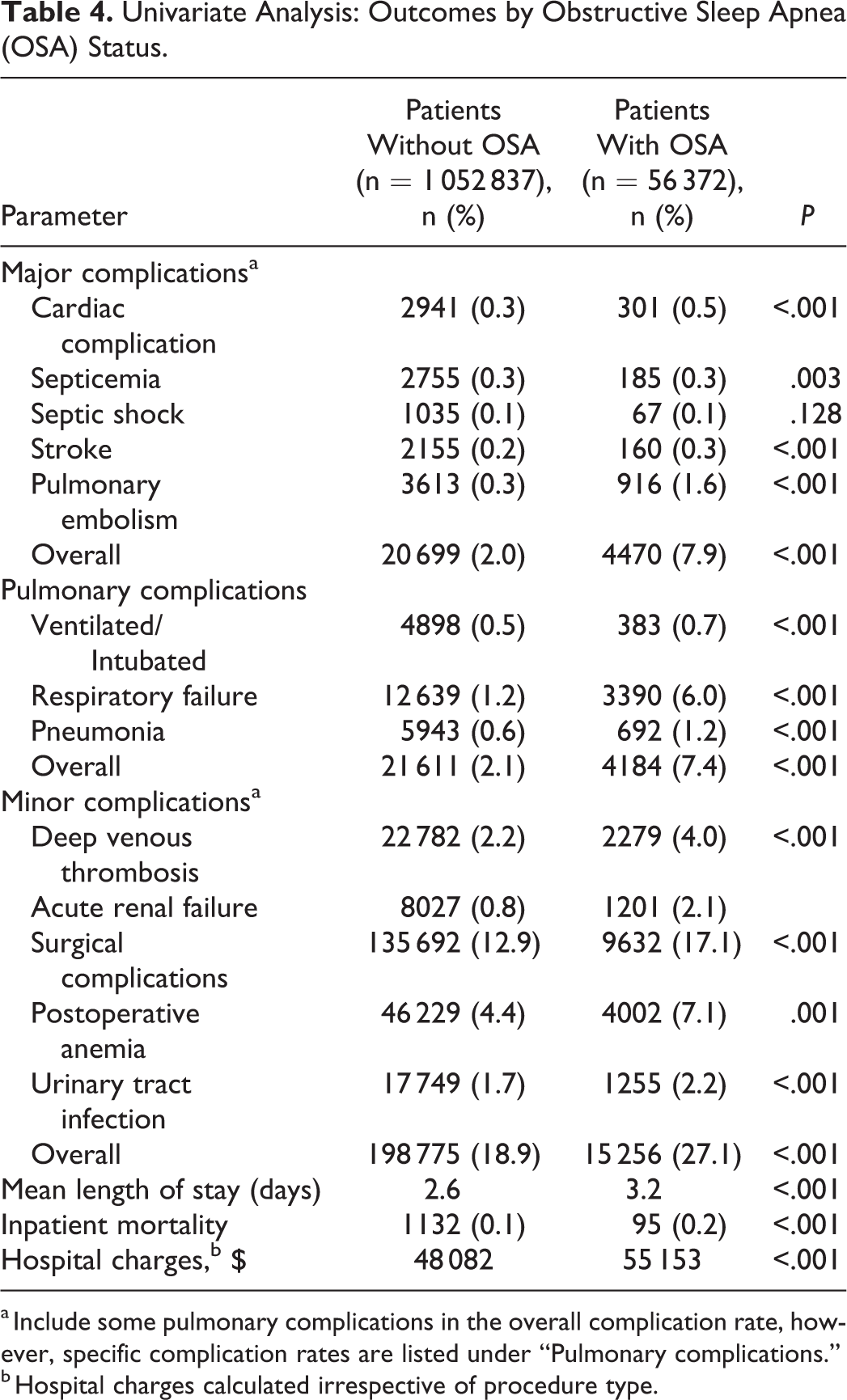
a Include some pulmonary complications in the overall complication rate, however, specific complication rates are listed under “Pulmonary complications.”
b Hospital charges calculated irrespective of procedure type.
Pulmonary complications were also higher in patients with OSA (7.4% compared with 2.1%; P < .001). There was a 5-fold increase in risk of postoperative respiratory failure in patients with OSA (6.0% compared with 1.2%; Table 4). OSA was identified as an independent predictor of pulmonary complications based on multivariate logistic regression (OR = 2.69; 95% CI 2.59-2.79; P < .001; Table 5).
Logistic Regression Analysis of Comorbidities and Outcomes.
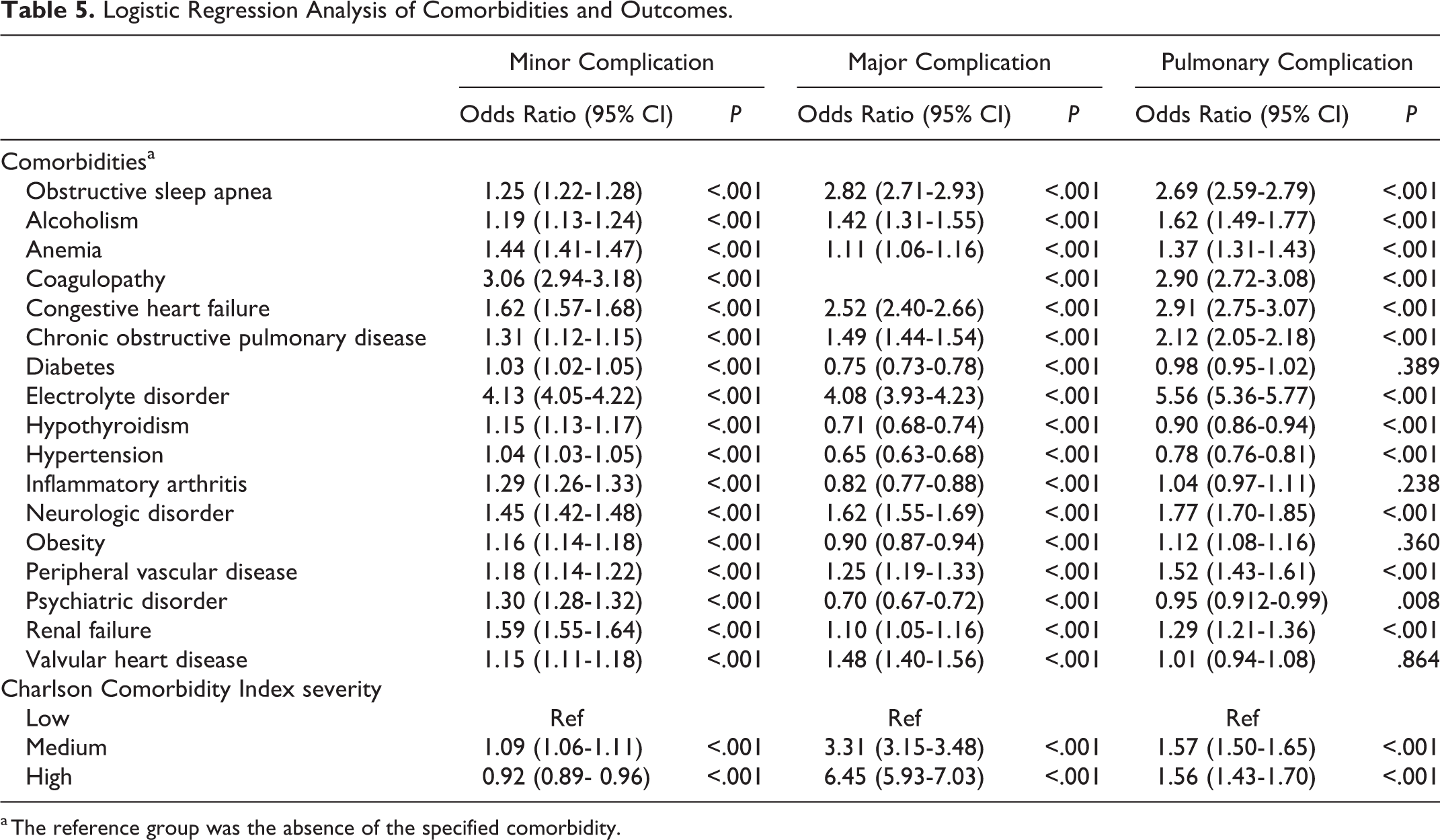
a The reference group was the absence of the specified comorbidity.
While univariate analysis determined that mortality rates were doubled in the OSA group (0.2% compared with 0.1%; P < .001), multivariate analysis did not identify OSA as an independent predictor of inpatient mortality (Table 5).
Length of Stay and Hospital Charges
Average length of stay was slightly longer for patients with OSA (3.2 days compared with 2.6 days; P < .001), and there was a moderate increase in overall hospital charges in the OSA cohort when compared with patients without OSA ($55 153 compared with $48 082; P < .001; Table 4).
Discussion
OSA is characterized by episodic upper airway obstruction and consequent hypoxia that leads to fragmented sleep patterns. While OSA is most commonly associated with obesity, there are a multitude of conditions that are inherently associated with decreased airway size and consequently increase the risk of OSA. These include connective tissue disorders, advanced age, alcohol consumption, and various congenital craniofacial deformities. Consequences of OSA include but are not limited to an increased risk of: cerebrovascular events, myocardial infarction, cardiac arrhythmias, congestive heart failure, insulin resistance, and psychiatric illness. 20
Epidemiologic data suggests that the prevalence of moderate to severe OSA is increasing, with current rates reported at 10% to 20%. 9 -11 Additionally, it is estimated that approximately 80% of patients with severe OSA may go undiagnosed. 10 While our data suggests that the prevalence of OSA increased from 2008 to 2012, the overall prevalence was less (5.1%) than rates published in the literature. This may be due to limited screening for the disease on a national level. Ultimately, the epidemiology of OSA still remains to be fully clarified.
Overnight polysomnography remains the gold standard for the diagnosis of OSA. The apnea-hypopnea index (AHI), the calculated number of apneic or hypopneic breathing events per hour, is derived during these sleep studies, with increasing AHI correlating with severity of OSA. This test requires an overnight stay in a specialized facility and as such, appointment availability and consequent high cost are limiting factors in its routine use. More recently, home sleep testing has also been introduced as a validated modality to diagnosis OSA. While cheaper than overnight polysomnography, costs of these home monitors are substantial, nonetheless. Furthermore, although overnight pulse oximetry alone has been suggested as an alternative and cost-effective screening option, its use has not been recommended to diagnose obstructive sleep apnea. To circumvent the high cost of these diagnostic tests, several questionnaires have been developed to screen for OSA. Examples of these questionnaires include the Berlin Questionnaire, Wisconsin Sleep Questionnaire, STOP-BANG questionnaires, and Haraldsson questionnaires. 10,21
The STOP-BANG questionnaire is one screening tool that has more recently been validated. It consists of 8 yes or no questions regarding clinical features of OSA (snoring, tiredness, observed apnea, elevated blood pressure) as well as patient demographic information, including body mass index (BMI), age, neck circumference, and gender. The questionnaire itself takes approximately 1 to 2 minutes to complete. BMI >35 m/kg2, age >50 years, neck circumference >40 cm, and male gender are considered positive responses. A patient with a score of 3 or greater is considered to be at higher risk for having OSA. The STOP-BANG model has been shown to have a sensitivity of 84.1% and specificity of 40.3% in detecting OSA in surgical patients. For moderate to severe OSA, the sensitivity of the STOP questionnaire increases to 92%. For the most severe cases of OSA, the sensitivity is 100% and specificity is 37%. 10 While certainly not perfect, the use of a validated and quick screening tool may be beneficial in the preoperative setting. Ultimately, until a standardized, cost-effective screening protocol is implemented, many patients with OSA will continue to go undiagnosed.
Recent studies have found that OSA imparts significantly higher odds of postoperative complications. Specifically, an increase in pulmonary-related complications such as a need for postoperative reintubation or mechanical ventilation has been demonstrated. 22 -24 This may be secondary to a decrease in the pharyngeal cross-sectional area and a consequent increase in the risk of pharyngeal collapse conferred by general anesthesia and opioids. 25 While we did not appreciate a significant increase in the need for mechanical ventilation or intubation following surgery (a 0.1% increase), there was a noticeable difference in the rates of postoperative respiratory failure between our 2 cohorts (6.0% compared with 1.2%; P < .001). The decrease in more severe pulmonary complications in our study may reflect an increased awareness in appropriate postoperative management of patients with OSA in more recent years.
Interestingly, OSA was associated with an approximate 2-fold increase in the development of a postoperative deep venous thrombosis in our patient population (4.0% compared with 2.2%; P < .001). A recent study by Chou et al 26 similarly showed a 3-fold increase in the incidence of deep venous thromboses in patients with OSA, and an even higher risk of deep venous thromboses in patients with OSA requiring continuous positive airway pressure (hazard ratio 9.58; 95% CI = 3.18-28.82; P < .001). It is thought that the intermittent nocturnal hypoxia and chronic systemic inflammation inherent to OSA ultimately induce endothelial dysfunction and create a physiologic environment that promotes thrombosis. 26
OSA did not appear to be associated with a clinically meaningful increase in inpatient mortality or length of stay despite noticeable increasing complication rates. However, in our study, patients with OSA had more expensive hospital stays. As length of stay did not differ by much between the two cohorts, these increased costs may be secondary to more specific pulmonary monitoring required in this patient population. Furthermore, as patients with OSA tend to have a higher comorbidity burden, concurrent specialist management may also increase resource utilization.
There are several notable limitations to this study. First, data available in the NIS is limited to the duration of a single hospitalization and as such may underestimate the incidences of adverse events. Additionally, analysis of NIS data depends on ICD-9 coding, which does not allow for the discernment of the severity of the OSA. Furthermore, the use of ICD-9 coding does not allow for assessment of intraoperative factors or accurate evaluation of preoperative factors such as laboratory values. Several studies have also shown that ICD-9 coding may additionally lack in sensitivity and specificity. Miscoding and missing data have also been cited as sources of error in large database studies. However, the use of a large database like the NIS is also a major strength of this study, as it allows for the national analysis of rare outcomes in discrete populations such as ours.
Conclusion
In conclusion, OSA is associated with an increased rate of postoperative complications and hospital resource utilization in patients undergoing elective spine surgery. Specifically, special attention should be paid to mitigate the risk of postoperative pulmonary complications as well as deep venous thrombosis. Patients who carry a diagnosis of OSA or who may be at high risk of having OSA should be counseled accordingly regarding the increased risks of surgery. The use of screening questionnaires for OSA in the preoperative setting may be prudent. However, given the limited amount of data regarding OSA and outcomes in spine surgery, prospective studies are warranted to confirm our findings and to evaluate the cost-effectiveness of routine preoperative screening for this disease.
Footnotes
Authors’ Note
Portions of this work were presented in presentation form at the American Academy of Orthopedic Surgeons Annual Meeting on March 17, 2016 in San Diego, California, as well as the 2017 Global Spine Congress Meeting on May 4, 2017 in Milan, Italy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.