
Abstract
Study Design:
Retrospective database study.
Objective:
To investigate the impact obstructive sleep apnea (OSA) has on perioperative complications, inpatient mortality, and costs in patients undergoing spinal fusions.
Methods:
Hospitalizations for spinal fusion surgery between the years 2009 and 2011 were identified using the Nationwide Inpatient Sample and grouped into patients with and without OSA. Patient demographic data, comorbidities, hospital characteristics, hospitalization outcomes, and costs were extracted and compared. Multivariable logistic regressions were conducted to compare the in-hospital outcomes of patients undergoing spinal fusion with and without OSA.
Results:
A total of 107 451 (7.7%) OSA patients who underwent spinal fusions were identified from 2009 to 2011. Compared with patients without OSA, OSA patients were significantly older, more likely to be male, and have significantly greater comorbidity burden. Multivariable regression analysis demonstrated that OSA had a significant independent association with slightly increased respiratory (odds ratio [OR] = 1.13, confidence interval [CI] = 1.09-1.16; P < .001), urinary and renal (OR = 1.11, CI = 1.07-1.16; P < .001) or overall inpatient complications (OR = 1.05, CI = 1.02-1.05; P < .001). OSA was also independently associated with significantly lower inpatient mortality (OR = 0.39, CI = 0.33-0.45; P < .001).
Conclusions:
While OSA confers greater comorbidity burden and is associated with slightly higher inpatient complication rates following spinal fusions, diagnosed OSA was not an independent predictor of inpatient mortality. A cautious interpretation of this finding is that on a national level, the current methods of preoperative medical optimization and inpatient management of OSA are satisfactory.
Introduction
Obstructive sleep apnea (OSA) is a sleep breathing disorder that is characterized by repetitive collapse and obstruction of the upper airways during sleep. 1,2 This condition affects up to 10% of the population and is associated with cardiac and respiratory comorbidities. 3,4 OSA has been recognized as a significant risk factor for postoperative mortality and morbidities such as cardiac arrhythmias, respiratory failure, emergent reintubation, and postoperative infections following total joint arthroplasty, cardiac surgery, and general surgery. 5 -8 In turn, medical optimization of OSA has been increasingly recognized as an important aspect of preoperative screening. As the number of spinal fusions increase, the prevalence of patients with OSA who undergo these procedures is likely to increase as well. While the effects of OSA have been evaluated in patients undergoing total joint arthroplasty and general surgery, the impact of recognized OSA on perioperative outcomes in patients undergoing spinal fusions have not been studied.
The purpose of this study is to evaluate the inpatient perioperative outcomes, mortality, as well as the costs in patients with recognized OSA who underwent spinal fusions using the Nationwide Inpatient Sample (NIS) database. We hypothesized that the diagnosis of OSA would increase inpatient mortality, rates of complications, inpatient length of stay, and resource utilization in spinal fusions.
Materials and Methods
The Nationwide Inpatient Sample (NIS) is an administrative dataset maintained by the Healthcare Cost and Utilization Project (HCUP) through sponsorship from the Agency for Healthcare Research and Quality. 9,10 The NIS is the largest all-payer hospital inpatient database in the United States and consists of a 20% stratified sample of all hospital discharges. Each entry in the database corresponds to a single hospitalization record and includes information regarding patient characteristics, hospital characteristics, and hospitalization outcomes. The database utilizes the International Classification of Disease 9th Revision, Clinical Modification (ICD-9-CM) for identification of procedures, diagnoses, and comorbidities.
Sample Selection
Hospitalizations between the years 2009 and 2011 were utilized for this study. The Clinical Classification Software (CCS) for ICD-9-CM is a diagnosis and procedural categorization scheme developed as part of the HCUP to group ICD-9-CM codes into smaller, clinically meaningful groups. 11 Hospitalizations for spinal fusion surgery were identified using ICD-9-CM procedural codes defined by the CCS procedural group for spinal fusion (158). Patients less than 18 years old were excluded. Spinal fusion patients were then divided into those with OSA (327.23 780.57) and those without OSA.
Outcome Measures
Patient demographic data for age, gender and race, hospital teaching status, hospital size, and primary payer were analyzed. Comorbidities were determined utilizing the categories identified by the Elixhauser Comorbidity Index as it has been well validated and is commonly used in administrative database studies. 12,13 In-hospital complications were determined on the basis of the following ICD-9-CM codes: neurologic complications (997.00-997.09), respiratory complications (518.4, 518.5, 518.81-518.84 997.3), cardiac complications (410 997.1), gastrointestinal complications (535.0 570 575.0, 577.0, 997.4), renal and urinary complications (584 997.5), pulmonary embolism (415.1), and wound-related complications (998.1, 998.3, 998.5, 998.83 999.3). Additionally, charges, costs, and length of stay were also extracted.
Data Analysis
To calculate national estimates, the dataset was weighted using the discharge weights supplied with the NIS. Multivariable logistic regressions were conducted to determine the contribution of OSA to postoperative complications while controlling for age, sex, race, Elixhauser Comorbidity Index, hospital size, hospital teaching status, hospital region, primary payer type, and complications. Continuous data between OSA and non-OSA groups was compared with t tests, and categorical variables were compared with χ2 tests. Statistical analysis was conducted in SPSS Version 21 (IBM Corp, Armonk, NY), and statistical significance was set at P < .05.
Results
A total of 1 396 501 patients who underwent spinal fusions were identified. From this population, 107 451 (7.7%) had a diagnosis of OSA. Patients with OSA were older (58.2 vs 55.8, P < .001) and significantly more likely to be male (59.6% vs 45.5%, P < .001; Table 1). In the OSA patient population, there was a significantly greater prevalence of congestive heart failure, chronic pulmonary disease, liver disease, neurological disorders, renal disease, obesity, and depression (Table 2). The mean Elixhauser index was also significantly greater in OSA patients. Rates of complications other than inpatient mortality were significantly greater in the group with OSA (P ≤ .001; Table 3). After controlling for patient and hospital characteristics, multivariate regression analysis demonstrated that recognized OSA was independently associated with slightly increased overall inpatient complications (OR = 1.05, CI = 1.02-1.05; P < .001). Specifically, OSA was found to be independently associated with slightly increased respiratory (OR = 1.13, CI = 1.09-1.16; P < .001) and urinary and renal complications (OR = 1.11, CI = 1.07-1.16; P < .001). OSA was also found to be independently associated with slightly reduced cardiac complications (OR = 0.87, CI = 0.82-0.93; P < .001), gastrointestinal complications (OR = 0.93, CI = 0.88-0.98; P = .005), pulmonary embolism (OR = 0.87, CI = 0.78-0.96; P = .009), and wound complications (OR = 0.86, CI = 0.82-0.90; P < .001). Interestingly, OSA was found to be an independent predictor of significantly reduced inpatient mortality (OR = 0.39, CI = 0.33-0.45; P < .001; Table 4).
Demographic Information for Patients Undergoing Spine Fusion.
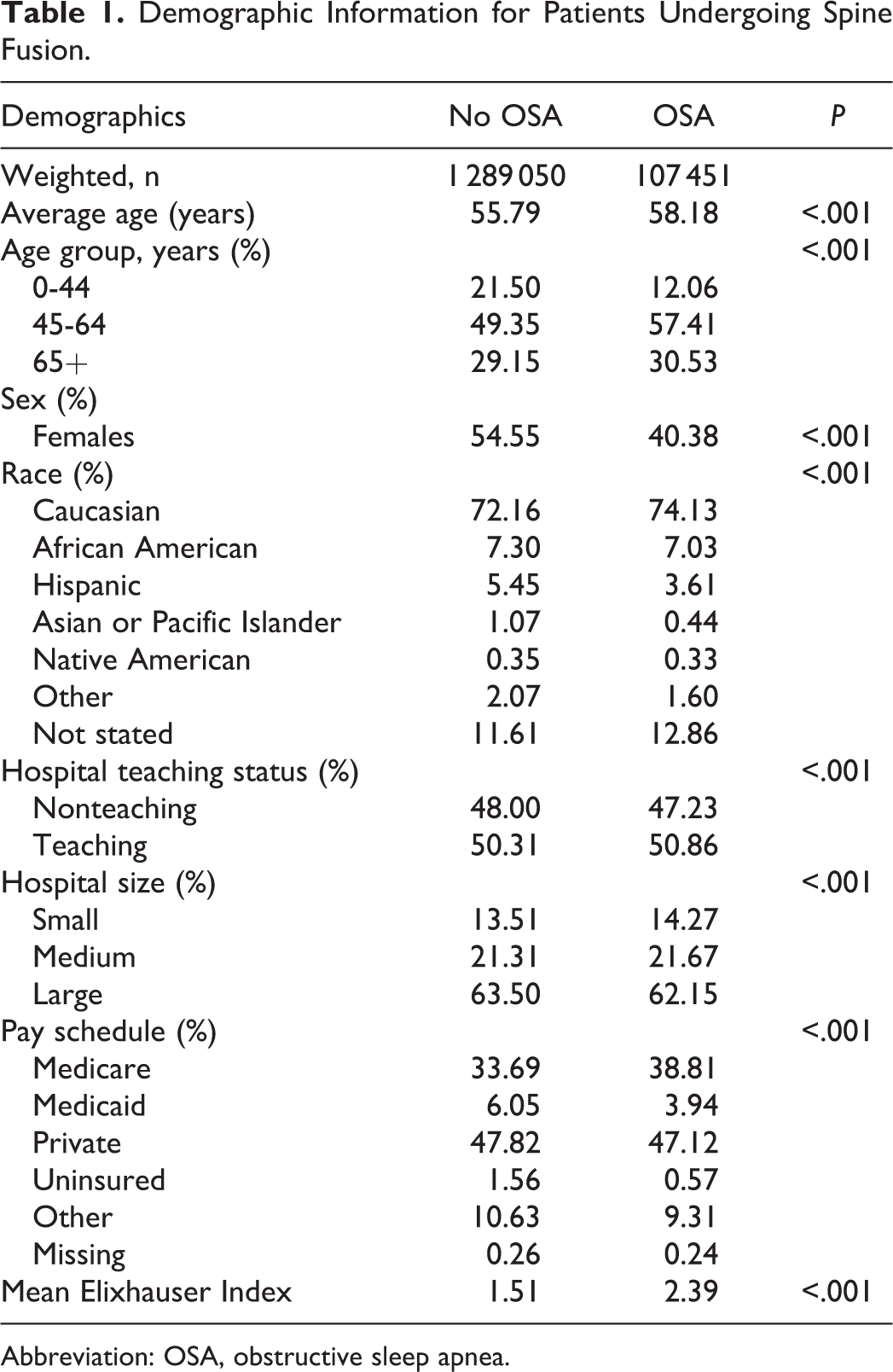
Abbreviation: OSA, obstructive sleep apnea.
Prevalence of Comorbidities in Patients Undergoing Spinal Fusion With and Without OSA.
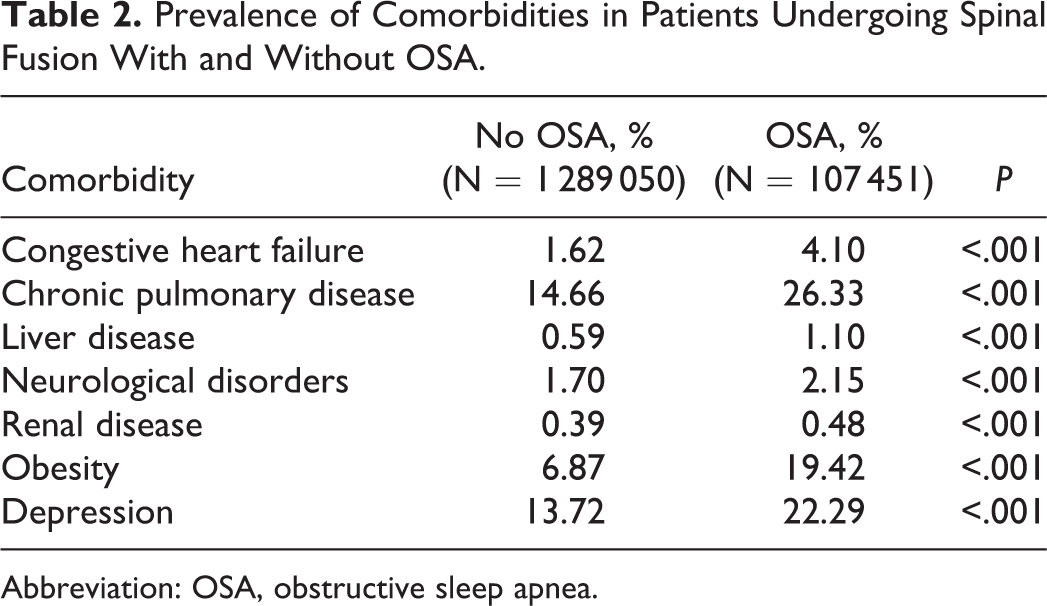
Abbreviation: OSA, obstructive sleep apnea.
Complications in Patients Undergoing Spinal Fusions With and Without OSA.
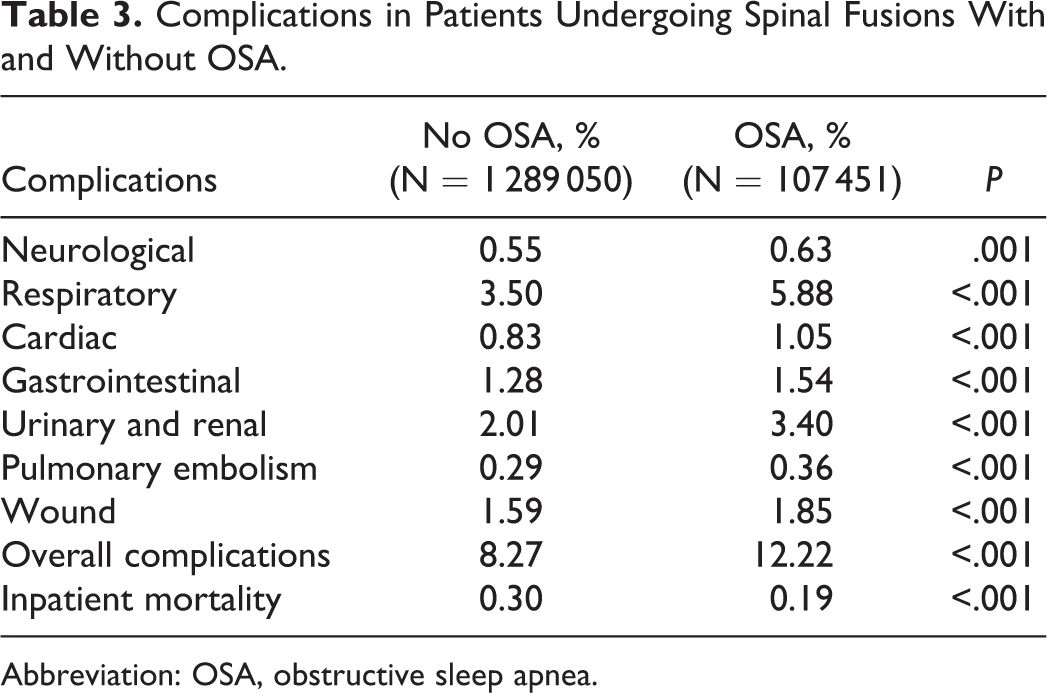
Abbreviation: OSA, obstructive sleep apnea.
Regression Modeling Predicting Influence of OSA on Inpatient Complications.
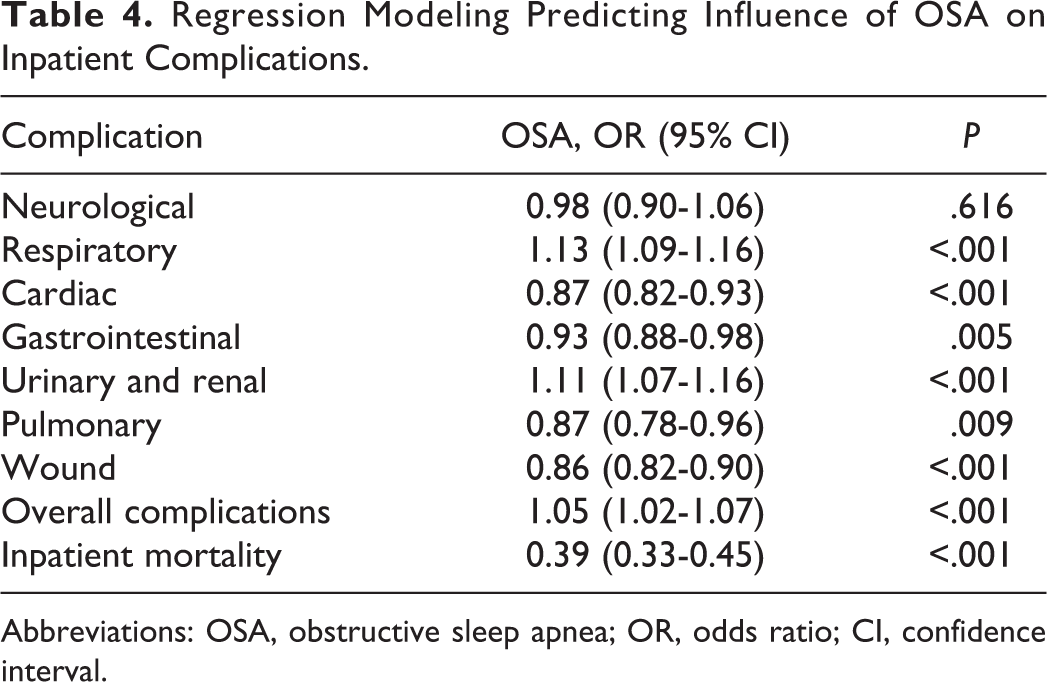
Abbreviations: OSA, obstructive sleep apnea; OR, odds ratio; CI, confidence interval.
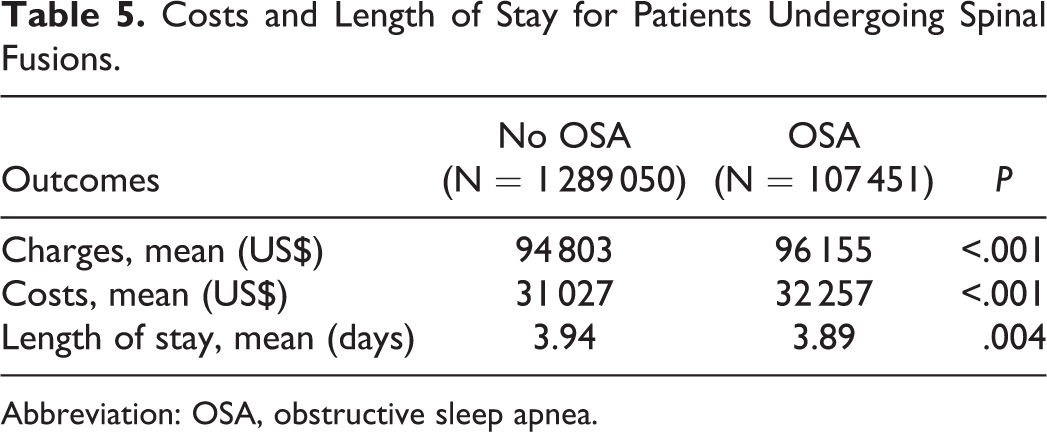
For resource utilization, patients with OSA demonstrated significantly greater inpatient costs ($32 257 vs $31 027; P < .001) but statistically significantly shorter length of stay (3.89 vs 3.94 days; P = .004; Table 5).
Costs and Length of Stay for Patients Undergoing Spinal Fusions.
Abbreviation: OSA, obstructive sleep apnea.
Discussion
Identification of modifiable risk factors is an important aspect of the preoperative evaluation and is critical for reducing inpatient morbidity and mortality. Previous studies have suggested that OSA represents an important surgical risk factor for adverse perioperative outcomes, inpatient mortality, and health care resource utilization. 14 In this study, we performed a large-scale analysis to evaluate the impact of OSA on perioperative outcomes and resource utilization following spinal fusion.
The prevalence of OSA in spinal fusion was 7.7%, which closely corresponds to its prevalence in the North American OSA population of 2% to 10%. This highlights the importance of understanding the impact of this risk factor in the spine patient population. Our demographic findings that OSA patients undergoing spinal fusion are older, more likely to be male, and have a greater comorbidity burden compared with those without OSA are consistent with other studies that evaluated OSA as a risk factor in general surgery, orthopedic procedures, and medical patients. 2,15,16
Our findings that OSA was independently associated with slightly increased risk of perioperative complications are also consistent with previous studies that evaluated OSA as a surgical risk factor. 14,15,17 A retrospective analysis found that OSA was independently associated with a high rate of cardiopulmonary complications in patients undergoing ambulatory colonoscopy and bariatric surgery. 16 Similarly, an analysis of OSA as a risk factor in revision joint arthroplasty found that OSA was independently associated with higher rates of pulmonary embolism, hematomas/seromas, and genitourinary complications. 14
Recognized OSA was also found to be independently associated with respiratory complications, which includes pulmonary insufficiency and acute respiratory failure. This was an expected finding as patients with OSA typically experience multiple episodes of upper airway collapse and hypoxemia. 4 Similarly, a prospective study evaluating OSA in vascular and general surgery also found that untreated OSA was independently associated with increased risk of unplanned reintubation. 18 OSA was also identified as an independent risk factor for emergent intubation in bariatric surgery. 16
Our multivariable analysis also demonstrated that OSA was associated with decreased inpatient mortality. This observed decrease in inpatient mortality was consistent with findings from other existing studies suggesting OSA confers a survival benefit during an inpatient stay. 2,16,19 A retrospective analysis evaluating the effect of OSA on inpatient management of pneumonia found that this risk factor was associated with lower inpatient mortality despite having a higher risk of transfer to intensive care and longer hospital stay. 19 Other studies examining the impact of OSA also found that this risk factor was associated with survival benefit during inpatient stays. 2,16
A possible explanation for the observed survival benefit of OSA in spine surgery is ischemic conditioning. One of the key characteristics of OSA is repeated collapse and obstruction of the upper airways, which results in repeated episodes of sublethal intermittent hypoxia and ischemia. This chronic intermittent hypoxemia was hypothesized to provide protection from ischemic insults. 2,16 This phenomenon is supported by an animal study that demonstrated intermittent hypoxia resulted in decreased infarction size after simulated myocardial infarction as well as an observational cohort suggesting that OSA patients may have less severe cardiac injury following myocardial infarction. 20,21 Another possibility is that the patients with recognized OSA in our study may have undergone more rigorous preoperative medical optimization and postoperative inpatient care. This explanation is supported by previous studies suggesting that preoperative treatment of OSA with positive airway pressure is effective in reducing postoperative complications while untreated OSA is independently associated with increased risk of postoperative cardiopulmonary adverse events. 18,22 Moreover, patients with previously diagnosed OSA have significantly lower inpatient complications and mortality rates compared with those with OSA that was detected on day-of-surgery screening, suggesting proper preoperative identification and treatment of OSA are critical for optimal postoperative outcomes. 23
Although our analysis demonstrated that the prevalence of postoperative complications were significantly greater in the OSA patient population, the actual differences in prevalence were small. Similarly, while multivariable regression analysis demonstrated that OSA was a significant predictor of respiratory, urinary and renal as well as overall complications, the calculated odds ratios were relatively low. In fact, the highest odds ratio for complications was respiratory complications with an odds ratio of only 1.13. Therefore, due to the large sample size in our study, we detected statistical differences showing that recognized OSA was associated with increased odds of postoperative complications, but further interpretation of the data suggests that these differences were small and may not be clinically significant.
The implications of this study are that although OSA confers a greater comorbidity burden such as respiratory complications that is similar to what was seen in previous studies, recognized OSA is associated with only a slightly increased risk of postoperative complications that may not be clinically significant in spinal fusions. Moreover, diagnosed OSA was not a significant predictor of inpatient mortality. Diagnosed OSA was also not associated with substantially higher inpatient costs or longer length of stay. An interpretation of our findings is that on a national level, the current preoperative optimization and inpatient management of previously diagnosed and recognized OSA in the spine surgery patient population appear to be satisfactory. This finding can be utilized by both patient and surgeon for risk-benefit considerations for spinal fusions and help guide research into preoperative medical optimization in spinal surgery toward other medical comorbidities.
Our study has several limitations that are inherent to large database analyses. The NIS database does not contain information on preoperative medical management of OSA or long-term postdischarge outcomes including postdischarge mortality or readmission rates. Moreover, the NIS database relies on clinical coding and diagnosis entry and therefore there may be inaccuracy, bias, or lapses in coding for OSA. Last, it is also possible that patients with diagnosed OSA may have better access to health care and preoperative optimization.
The implications of this study are that although OSA confers greater comorbidity burden, greater resource utilization, and is associated with higher overall rate of postoperative complications following spinal fusions, diagnosed OSA does not appear to increase inpatient mortality and is possibly associated with a survival benefit. An interpretation of our findings is that on a national level, the current preoperative optimization and inpatient management of previously diagnosed and recognized OSA in the spine surgery patient population appear to be satisfactory. However, further studies are needed to further clarify the relationship between OSA and outcomes following spinal fusion surgery.
Footnotes
Authors’ Note
Given the de-identified, publicly available nature of this dataset, this study qualifies for IRB exempt status under Section 4 of 45 CFR 46.101(b).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.