
Abstract
Objective
Obstructive sleep apnea is an independent risk factor for cardiovascular diseases, particularly resistant hypertension. For patients who are noncompliant or unable to tolerate continuous positive airway pressure therapy, surgical treatment may serve as a viable alternative. In this study, we evaluated the impact of multilevel sleep surgery on blood pressure levels in patients with resistant hypertension.
Methods
This is a bicentric retrospective observational study of 50 patients with severe obstructive sleep apnea and resistant hypertension who underwent multilevel targeted sleep surgery.
Results
Clinical improvement was objectively confirmed by polygraphy performed 6 months after surgery, demonstrating a significant reduction in the mean Apnea–Hypopnea Index from 44.98 ± 14.94 to 22.16 ± 7.30 (P < 0.005). Furthermore, the adjusted mean preoperative systolic blood pressure decreased from 150 ± 14.77 to 124 ± 17.14 mmHg (P < 0.001), while diastolic blood pressure decreased from 94 ± 5.3 to 80 ± 7.2 mmHg (P < 0.001). Notably, 20 patients (40%) no longer required antihypertensive medication after surgery.
Discussion
To the best of our knowledge, this study is the first clinical trial to evaluate the efficacy of multilevel surgery in improving resistant systemic hypertension in patients with multilevel airway obstruction and severe obstructive sleep apnea syndrome.
Conclusions
This study highlights the potential of multilevel sleep surgery as an effective intervention for improving blood pressure control in patients with resistant hypertension and severe obstructive sleep apnea.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a prevalent sleep disorder characterized by repeated episodes of partial or complete upper airway obstruction during sleep, leading to disrupted sleep and reduced oxygen levels. OSA is a significant global health issue. The prevalence of OSA varies across studies due to differences in diagnostic criteria and study populations. According to recent studies, the prevalence of OSA—defined as an Apnea–Hypopnea Index (AHI) of ≥5 events per hour—ranges from 5% to 24% of the global population. Furthermore, it is estimated that >80% of moderate-to-severe OSA cases remain undiagnosed. 1
Hypertension is one of the most common medical conditions and a major contributor to cardiovascular disease worldwide. 2 Resistant hypertension is defined as blood pressure above the target level (>130/90 mmHg), despite the use of three antihypertensive drugs from different classes or controlled blood pressure requiring four or more medications. 3
The Sleep Heart Health Study and the Wisconsin Sleep Cohort have demonstrated a strong association between OSA and hypertension.4,5 Numerous studies have also established OSA as a significant risk factor for resistant hypertension, with evidence of a dose–response relationship between OSA severity and the degree of high blood pressure. 6 Experimental and clinical studies suggest that the pathogenesis of OSA-related hypertension is multifactorial, involving disruptions in several regulatory systems. These include autonomic cardiovascular modulation, activation of the sympathetic nervous system, activation of the renin–angiotensin–aldosterone system, systemic and vascular inflammation, endothelial dysfunction, oxidative stress, arterial stiffness, metabolic abnormalities, and alterations in cardiac function and structure. 7
When treating patients with OSA, the primary therapeutic goal should not only be to reduce the AHI but also to improve objective and subjective outcomes such as wakefulness, quality of life, and systemic complications such as hypertension. 8
Since its introduction in the 1980s, continuous positive airway pressure (CPAP) therapy has been widely regarded as the gold standard treatment for OSA.9,10 Numerous systematic reviews and meta-analyses have confirmed the beneficial effects of CPAP therapy on systemic hypertension. 11 However, the benefits of CPAP in reducing blood pressure depend on nocturnal use, the severity of OSA, and patient compliance with the device.9–13 Despite its proven efficacy in treating OSA and reducing cardiovascular complications, compliance with CPAP therapy remains low. 14
For patients who cannot tolerate or do not adhere to CPAP use, surgical treatment may serve as an important alternative.2–15 To be effective, surgical treatment must be carefully tailored to address the specific sites of obstruction and collapse in the upper airway. Therefore, identifying the locations and patterns of upper airway collapse is critical for determining the appropriate surgical approach and ensuring its effectiveness. In patients with multilevel upper airway obstruction who are unable to tolerate CPAP, multilevel surgery can be a viable option, yielding favorable postoperative respiratory outcomes.16–23
To date, only a few studies have focused on the efficacy of multilevel surgery in improving resistant hypertension by reducing blood pressure levels. This study aimed to evaluate the impact of targeted multilevel sleep surgery on blood pressure control in patients with severe sleep apnea and resistant hypertension.
Materials and methods
Patient selection
This was a bicentric retrospective observational study conducted at the sleep surgery centers of Alexandria University and Sapienza University of Rome. Patients with OSA and resistant hypertension who consecutively underwent multilevel surgery for sleep apnea were selected for inclusion in the study. All enrolled patients had severe OSA (AHI > 30) accompanied with high blood pressure (systolic blood pressure (SBP) > 130 mmHg and diastolic blood pressure (DBP) > 90 mmHg). These patients either refused CPAP therapy or demonstrated poor compliance with its use. Despite the concurrent use of three antihypertensive agents from different drug classes—including a long-acting calcium channel blocker, a renin–angiotensin system inhibitor (angiotensin-converting enzyme inhibitor or angiotensin receptor blocker), and a diuretic—their blood pressure remained uncontrolled.
Patients were excluded from the study if they had severe cardiorespiratory comorbidities, dyslipidemia, diabetes, or severe obesity (body mass index (BMI) > 40 kg/m2). Patients with mild-to-moderate OSA (AHI < 30), sleep disturbances other than OSA, severe OSA with normal blood pressure, or incomplete postoperative records were also excluded. Additionally, individuals who had previously undergone any type of upper airway surgery—including pharyngoplasty, radiofrequency ablation, septoplasty, or endoscopic sinus surgery—were not eligible for inclusion.
Data collected for all enrolled patients included age, sex, BMI, preoperative and postoperative polysomnography (PSG) results, and preoperative and postoperative blood pressure (SBP and DBP).
Polysomnography
Level III polygraphy, a home sleep apnea test (HASAT) using the SOMNOtouch™ RESP device (Randersacker, Germany), was performed for all patients during the baseline preoperative evaluation and 6 months after surgery. The AHI was defined as the total number of apneas plus hypopneas per hour of sleep. According to the American Academy of Sleep Medicine guidelines, an apnea was defined as a drop in the peak thermal sensor excursion by at least 90% of baseline for at least 10 seconds. Hypopnea was defined as a reduction of at least 30% in nasal pressure signal excursions for at least 10 seconds, accompanied with a desaturation of 3% or more from the pre-event baseline.17–19 Preoperative and postoperative PSG data focused on the AHI.
Blood pressure measurement
Blood pressure was measured using a precision manual sphygmomanometer. Two readings were taken at 5-min intervals to ensure accuracy. Measurements were performed in a comfortable, resting environment to minimize external factors that could influence the results. The same settings and methods were applied for preoperative and follow-up measurements at all clinical visits.
Surgical procedure
All patients underwent multilevel targeted sleep surgery for the management of OSA. Drug-induced sleep endoscopy 18 was performed preoperatively to identify the sites and patterns of upper airway obstruction or collapse. Patients with nasal obstruction, velopharyngeal collapse, and base-of-tongue collapse were deemed suitable candidates for multilevel surgery.
The surgical approach involved a combination of nasal surgery (septoplasty and turbinoplasty), barbed reposition pharyngoplasty, 19 and coblation tongue base ablation/resection.20,21 This approach is well-documented in the literature as an effective method for treating severe cases of OSA with multilevel obstruction (nose, velopharyngeal, and base of tongue), resulting in improved respiratory outcomes.19–23
Postoperative care
Postoperative care included a 3-day hospital stay with the head of the bed elevated to 45° during the night. Continuous pulse oximetry was used during the first postoperative night. The postoperative treatment regimen included 24-h corticosteroids, prophylactic antibiotics, and pain management with intravenous ketorolac (30 mg every 6 h). Preoperative tracheostomy and postoperative intensive care unit admission were not routine procedures for this patient cohort.
Outcome measurement
Surgical efficacy was assessed by comparing preoperative and postoperative changes in HASAT parameters. Surgical response was defined according to the Sher criteria: a reduction in AHI of at least 50% and a postoperative AHI of <20 events per hour. 22 Clinical evaluations were conducted at 2 weeks, 1 month, 3 months, and 6 months after surgery. A follow-up PSG was performed at the 6-month visit to evaluate improvements in nocturnal respiratory outcomes, and blood pressure measurements were used as part of the study outcomes.
Statistical analysis
Statistical analysis was performed using the Student’s t-test for continuous data, with Fisher’s correlation used to evaluate differences in preoperative and postoperative results. A P-value <0.05 was considered to indicate statistical significance. All analyses were conducted using STATA 12.1 software (Stata Corp., College Station, Texas, USA).
Due to the retrospective design of the study, local ethics committee approval was not required. We discussed the study with the Ethics Committee of Sapienza University and received their exemption. Due to the retrospective design of the study, signed consent was not required. No patient details have been reported in this study. The study was conducted in accordance with the Declaration of Helsinki.
The reporting of this study complies with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 24
Results
A total of 50 patients met the inclusion criteria and underwent multilevel targeted sleep surgery. Their clinical characteristics are summarized in Table 1.
Clinical characteristics and operative data of 50 patients with severe obstructive sleep apnea who underwent targeted multilevel sleep surgery.

The preoperative AHI was 44.98 ± 14.94, which significantly decreased to a postoperative AHI of 22.16 ± 7.30 at the 6-month follow-up. The surgical success rate was 72%, defined as a 50% reduction in AHI and a postoperative AHI <20 events per hour. A statistically significant reduction in AHI was observed (P = 0.002).
The adjusted mean preoperative SBP decreased from 150 ± 14.77 to 124 ± 17.14 mmHg (P = 0.001), while the DBP decreased from 94 ± 5.3 to 80 ± 7.2 mmHg (P = 0.001) (Table 2 and Figure 1).
AHI value and blood pressure values before and after surgery.

Values are presented as mean ± SD.
AHI: Apnea–Hypopnea Index; DBP: diastolic blood pressure; SBP: systolic blood pressure.

Changes in systolic blood pressure and diastolic blood pressure before and after surgery. DBP: diastolic blood pressure; SBP: systolic blood pressure.
Linear regression analysis revealed a statistically significant correlation between AHI reduction and blood pressure levels, with patients with a lower reduction in AHI showing higher SBP levels (P = 0.04) (Figure 2).
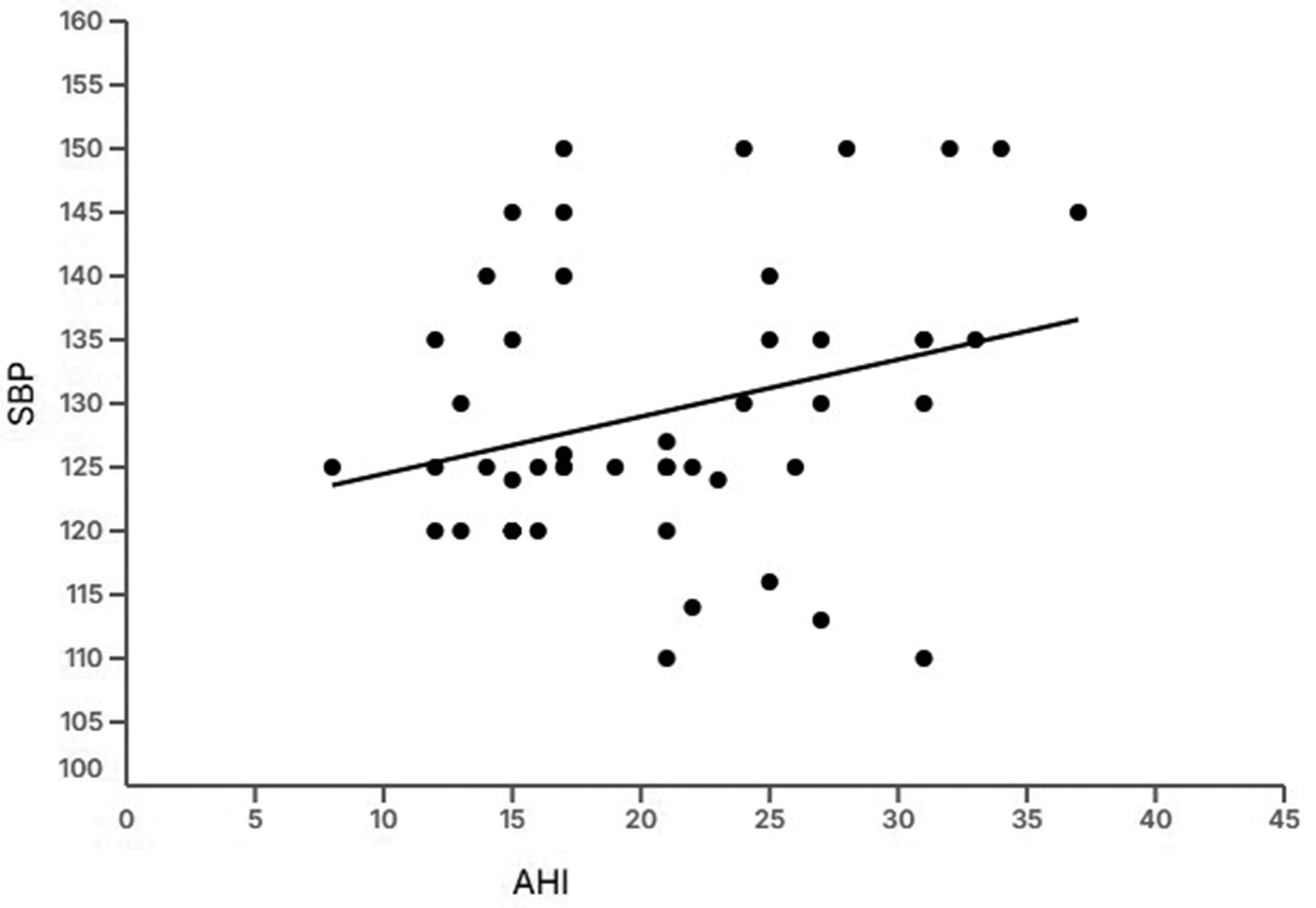
Regression analysis between Apnea–Hypopnea Index (AHI) value and systolic blood pressure (SBP) levels.
There was no significant change in BMI before and after surgery. The mean preoperative BMI was 30.64 ± 2.88 kg/m2, compared with a postoperative BMI of 29.64 ± 2.88 kg/m2.
Twenty patients (40%) no longer required their usual antihypertensive therapy after surgery. Another 20 patients (40%) changed their antihypertensive medications, achieving blood pressure control with two drugs instead of three. However, 10 patients (20%) experienced no change in blood pressure control and continued to have resistant hypertension. These patients also did not meet the success criteria in the postoperative sleep study.
Discussion
OSA significantly increases the risk of cardiovascular diseases through mechanisms such as sympathetic nervous system overactivity, oxidative stress, and endothelial dysfunction. Major cardiovascular comorbidities include hypertension (especially resistant and nocturnal hypertension), coronary artery disease, heart failure, pulmonary hypertension, transient ischemic attacks, atherosclerosis, and arterial stiffness.1–15
Arterial hypertension is the primary comorbidity associated with OSA. In some cases, it manifests as resistant hypertension requiring multiple drugs for treatment.24,25 CPAP remains the gold standard treatment for OSA in the literature. This treatment has been shown to be effective and validated in the management of all OSA-related comorbidities. Patients who use CPAP for at least 4–6 h per night, especially those with severe OSA, demonstrate greatest reductions in blood pressure levels after treatment. Furthermore, CPAP therapy combined with antihypertensives has shown additive effects in reducing blood pressure compared with medical therapy alone. Therefore, as confirmed by several studies, CPAP therapy can be considered a highly effective nonpharmacological intervention to reduce blood pressure in patients with OSA, especially when adherence is high and in patients with severe disease or resistant hypertension.26–33
However, the issue with CPAP therapy lies in its low compliance. Poor compliance with CPAP is often attributed to discomfort, mask-related problems, dry mouth, or lack of perceived benefit. These factors significantly limit its effectiveness in managing OSA and its associated comorbidities. Therefore, in patients with severe OSA and resistant hypertension, alternative treatments should be considered to reduce the risk of adverse cardiovascular events.
The effect of mandibular advancement devices (MAD) in reducing blood pressure in patients with OSA has been reported in a recent clinical study. Ou et al. 34 demonstrated that patients using MAD at night showed a greater reduction in all secondary ambulatory blood pressure parameters, with the most pronounced effects observed in sleep blood pressure parameters. Both MAD and CPAP improved daytime sleepiness, with no significant differences between groups (P = 0.384). There were no notable between-group differences in cardiovascular biomarkers between the MAD and CPAP groups.
To the best of our knowledge, this study is the first clinical trial to evaluate the efficacy of multilevel surgery in improving resistant systemic hypertension in patients with multilevel airway obstruction and severe OSA syndrome.
In our study, multilevel sleep surgery involved simultaneous nasal, velopharyngeal, and tongue base surgeries.32,33 The adjusted mean preoperative and postoperative SBP reduced from 150 ± 14.77 to 124 ± 17.14 mmHg (P < 0.001), and DBP reduced from 94 ± 5.3 to 80 ± 7.2 mmHg (P < 0.001). There was no significant decrease in the patients’ BMI before and after surgery (preoperative BMI: 30.64 ± 2.88 kg/m2, postoperative BMI: 29.64 ± 2.88 kg/m2), indicating that the reduction in SBP and DBP was not influenced by BMI changes.
Twenty patients (40%) did not require antihypertensive medications after surgery, while another twenty patients (40%) had their antihypertensive medications adjusted (blood pressure controlled with two drugs instead of three). Ten patients (20%) showed no change in blood pressure control and continued to have resistant hypertension, indicating that they still required three antihypertensive agents. These patients also did not meet the success criteria based on postoperative sleep study results.
Limitations of this study included the small patient sample and the retrospective design. Prospective randomized studies are currently underway to confirm these findings. All patients underwent the same surgery, making it impossible to determine the effect of individual surgical interventions on blood pressure reduction. Additionally, further studies are ongoing to evaluate the effectiveness of different types of single- or multilevel surgeries on hypertension.
Conclusions
In patients with severe OSA, multilevel obstruction, and resistant hypertension, multilevel targeted sleep surgery could be effective in reducing blood pressure to controllable levels, potentially decreasing the use or dosage of oral antihypertensive therapy.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251361484 - Supplemental material for Effect of targeted multilevel sleep surgery on resistant hypertension in patients with severe obstructive sleep apnea
Supplemental material, sj-pdf-1-imr-10.1177_03000605251361484 for Effect of targeted multilevel sleep surgery on resistant hypertension in patients with severe obstructive sleep apnea by Ahmed Bahgat, Mostafa Elwany, Claudio Vicini, Yassin Bahgat, Giuseppe Magliulo, Antonio Greco, Armando De Virgilio, Annalisa Pace, Mario Giuseppe Bellizzi, Enrica Croce, Lodovica Gatti, Antonino Maniaci, Jerome R Lechien, Alberto Caranti, Stéphane Gargula, Luigi A Vaira, Heloisa Dos Santos and Giannicola Iannella in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank Ms Daniela Pastore for her support in drafting the manuscript.
Author contributions
All authors have contributed to the design, analysis, and results of the study and to the writing of the final manuscript.
Data availability statement
Data supporting this study are included within the article.
Declaration of conflicts of interest
The authors declare no conflicts of interest.
Funding
This research received no external funding.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki. Due to the retrospective design of the study, local ethics committee approval was not required. We discussed the study with the Ethics Committee of Sapienza University and received their exemption.
Informed consent statement
Due to the retrospective design of the study, signed consent was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.