
Abstract
Background
This study was performed to compare different surgical approaches in the treatment of spinal tuberculosis.
Methods
We conducted a literature search to identify and analyze papers published from January 1966 to April 2018 relevant to comparison of the anterior, posterior, and anterior combined with posterior approaches in the treatment of spinal tuberculosis of the thoracic and lumbar regions.
Results
Twenty-five studies involving 2295 patients were identified in this systematic review. The operative time was significantly longer in the anterior combined with posterior approach than in the other two approaches. Blood loss was significantly greater in the anterior combined with posterior approach (1125.0 ± 275.5 mL) than in the posterior approach (710.4 ± 192.4 mL). The difference in correction of the kyphosis angle among the three procedures was not significant. The overall surgical and transthoracic complications were significantly lower in the posterior approach. The clinical outcome of all patients improved, but there was no significant difference among the three procedures.
Conclusions
Blood loss, overall surgical and transthoracic complications, and the operative time are different among the three approaches. Therefore, different factors must be carefully assessed in deciding among the three procedures.
Keywords
Summarized findings and limitations of this study
The anterior combined with posterior approach had a longer operative time than either the anterior or posterior approach. The blood loss volume was smaller in the posterior approach than in the anterior combined with posterior approach. The posterior approach had lower overall surgical complications and transthoracic complications than the other two approaches. In deciding among the three approaches, specific features of spinal tuberculosis, surgical experience, risks of surgical complications ranging from neurological to structural, and radiologic and clinical outcomes must be carefully assessed. One limitation of this study was that the surgical procedure was not uniform; anterior or posterior or combined approaches were used in a one- or two-stage procedure with different instrumentations. Another limitation of this study was that we only included retrospective studies in the review; thus, the indications for the surgical procedures were probably different.
Background
Tuberculosis is one of the leading infectious causes of death in the developing world. Approximately 1% to 3% of affected patients have involvement of the skeletal system, and up to 50% have spinal involvement, especially in the thoracic and lumbar segments.1,2 Management of spinal tuberculosis involves clearance of the spinal pathology, correction of spinal deformities, prevention of neurological compromise, and achievement of unrestricted mobilization of the patient. The classic “Hong Kong operation” involves direct removal of the anterior spinal pathology followed by careful reduction of stress on the spinal cord and reconstruction of the area by anterior instrumentation.3–5
However, several potential adverse events may influence the choice of the anterior surgical approach as the main treatment option, such as prolonged immobilization, progressive kyphosis, and graft failure. Because of advancements in diagnostic techniques such as computed tomography-guided biopsy and magnetic resonance imaging as well as more effective treatments such as anti-tuberculous chemotherapy, spinal tuberculosis is now diagnosed at an earlier stage and the number of severe cases has decreased.6,7 Additionally, posterior instrumentation techniques for the correction and stabilization of spinal deformities have become very well developed. As a result, the treatment for spinal tuberculosis tends to be more diverse and less destructive.8–10
Whether the anterior, posterior, or anterior combined with posterior surgical approach most effectively eradicates spinal tuberculosis remains controversial. Different surgical methods for spinal tuberculosis of the thoracic and lumbar region have rarely been reported in systematic reviews.
We performed a systematic review of surgical procedures for spinal tuberculosis and analyzed the radiologic data and patient-related outcomes, including complications. The findings of this review will help physicians choose the most effective management techniques for patients with tuberculosis in the thoracic or lumbar region.
Methods
This study was approved by the Ethics Committee of Renji Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. Written informed consent was not needed because of the study design (systematic review).
Based on patient safety and the efficacy of the procedures, we raised three clinically crucial questions to determine the optimal surgical procedure in treating thoracic and lumbar tuberculosis. The primary data used as evidence to answer these questions were obtained from the treatment results, such as the radiologic data and patient-related outcomes. These three questions were as follows:
Among the anterior, posterior, or anterior combined with posterior approach for thoracic or lumbar spinal tuberculosis, which surgical procedure provides the best radiologic outcome? Among the anterior, posterior, or anterior combined with posterior approach for thoracic or lumbar spinal tuberculosis, which surgical procedure most effectively reduces complications? Based on clinical results, is it possible to choose among the anterior, posterior, or anterior combined with posterior approach for patients with thoracic or lumbar spinal tuberculosis?
Inclusion criteria
The four inclusion criteria for studies in this systematic review were as follows.
Target population: Adult patients with spinal tuberculosis in the thoracic and lumbar regions.
Type of study: Clinical study.
Interventions: Anterior, posterior, or anterior combined with posterior approach in the surgical treatment of spinal tuberculosis in the thoracic and lumbar regions.
Measurement of outcomes: We based the outcome of this review on surgical outcomes (radiographic outcomes and complications) and patient-related outcomes (visual analogue scale score, Oswestry Disability Index, and similar measurements).
Exclusion criteria
We excluded case reports, studies published only in abstract form, studies adopting novel and nonconventional techniques, and studies with a follow-up duration of <1 year.
Identification of studies
We searched the Medline and Embase databases for publications comparing the anterior, posterior, or anterior combined with posterior approach for the treatment of thoracic and lumbar tuberculosis from January 1966 to April 2018 using the following keywords in the PubMed search engine: “tuberculosis” or “thoracic tuberculosis,” “lumbar tuberculosis,” and “spinal tuberculosis” or “anterior approach” or “posterior approach” or “surgical treatment” or “decompression” or “debridement” or “bone graft” or “instrumentation.” Two authors independently read the titles and abstracts of each paper and selected those that fit the inclusion criteria. Two reviewers extracted the data used in the review (Figure 1). The overall incidence of surgical complications associated with a procedure was defined as the ratio of the overall number of complications that occurred to the total number of patients who underwent the procedure. The incidence of a specific complication associated with a procedure was defined as the ratio of the number of occurrences of the specific complication to the number of patients in the articles reporting that complication using the surgical procedure.
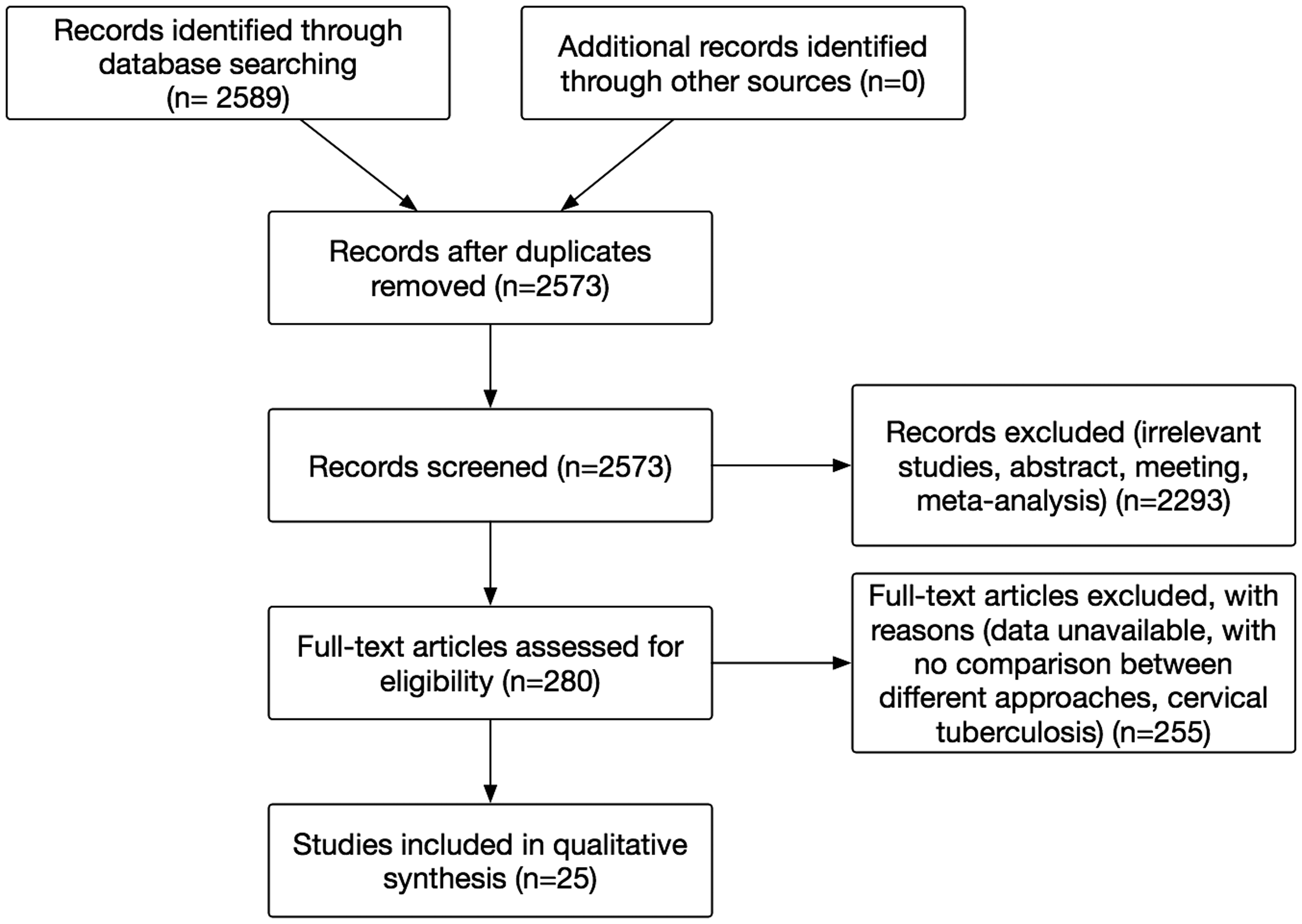
Flow diagram for selection of studies and specific reasons for exclusion.
Statistical analysis
The statistical analysis was performed using the unpaired t-test, Fisher’s exact test, and the chi-square test. Statistical significance was confirmed when the P-value was <0.05. Variables were calculated using SPSS software version 25 (IBM Corp., Armonk, NY, USA).
Results
Twenty-five studies comparing the anterior, posterior, or anterior combined with posterior approach in treating spinal tuberculosis in the thoracic and lumbar regions were identified.11–35 Table 1 summarizes the characteristics of the included studies. Among the 25 studies, the anterior surgical approach mainly referred to anterior debridement, decompression, and bone grafting with different fixations in a one- or two-stage procedure; the posterior surgical approach mainly referred to posterior debridement, decompression, and bone grafting with different fixations in a one- or two-stage procedure; and the anterior combined with posterior surgical approach referred to anterior and posterior (or posterior and anterior) debridement, decompression, and bone grafting with different fixations in a one- or two-stage procedure.
Previous reports of surgical treatment of thoracic and lumbar spinal tuberculosis.

A, anterior approach; P, posterior approach; AP, anterior combined with posterior approach; T, thoracic; TL, thoracolumbar; L, lumbar; LS, lumbosacral; preop, preoperative; postop, postoperative; INH: isoniazid; RFP: rifampicin; EMB: ethambutol; PYZ: pyrizinamide; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; ODI: Oswestry Disability Index; VAS: visual analogue scale; ASIA: American Spinal Injury Association; N/A: not available.
Operative time and estimated blood loss
The operative time and estimated blood loss of different procedures for tuberculosis in the thoracic and lumbar spinal regions were reported in 20 studies14–18,20,22–35 (Table 2).
Operative time and blood loss of different procedures for thoracic and lumbar spinal tuberculosis.
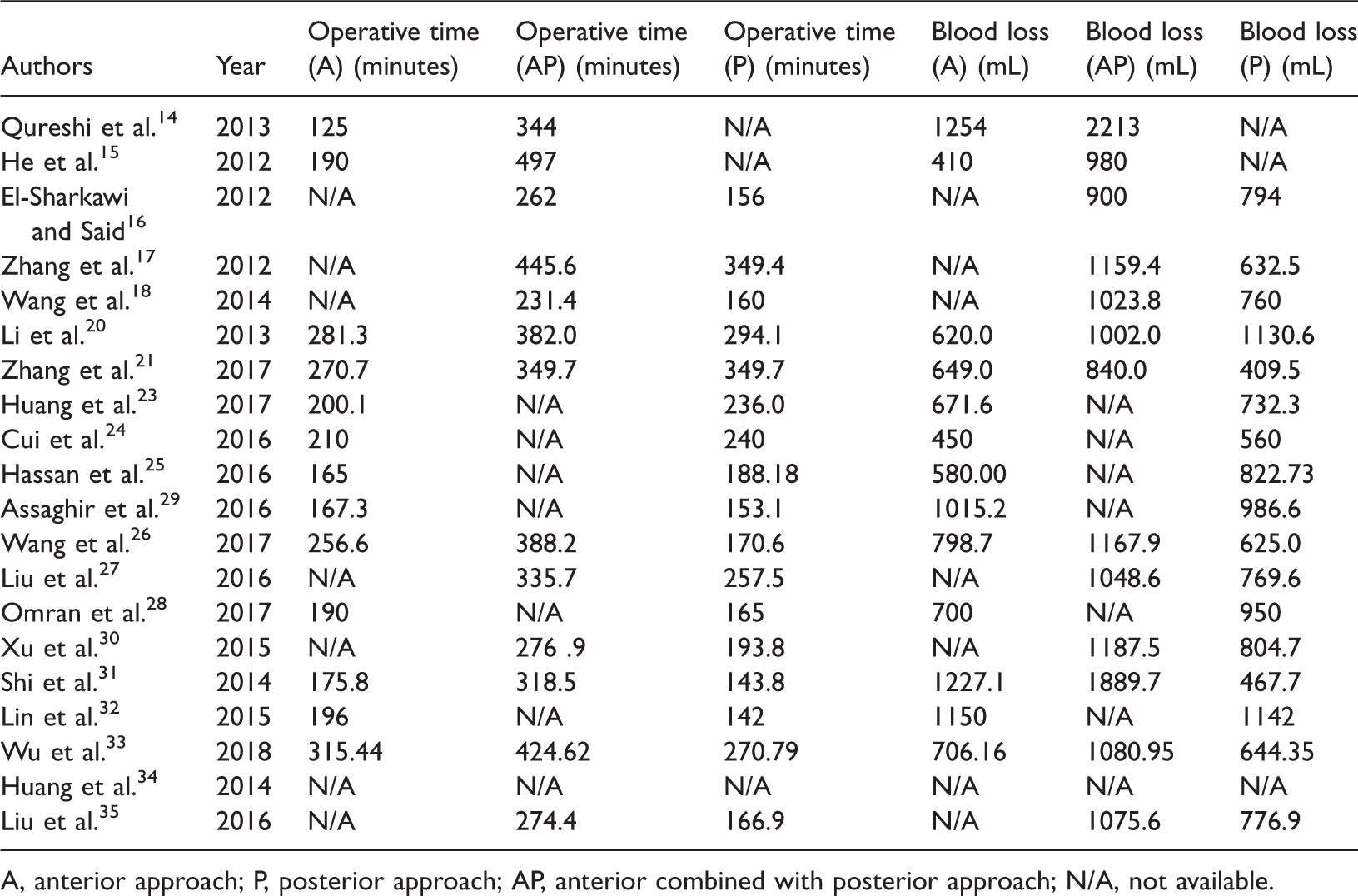
A, anterior approach; P, posterior approach; AP, anterior combined with posterior approach; N/A, not available.
Of the 20 studies, 7 studies14,15,20,21,26,31,33 compared the operative time for the anterior approach (230.7 ± 68.1 minutes) versus the anterior combined with posterior approach (386.3 ± 59.8 min), and a statistically significant difference was detected (t = −4.540, P = 0.001). Among the 20 studies, 11 studies16–18,20,21,26,27,30,31,33,35 compared the operative time for anterior combined with posterior approach (335.4 ± 69.9 minutes) versus the posterior approach (228.4 ± 78.6 minutes), and a statistically significant difference was detected (t = 3.373, P = 0.003). Among the 20 studies, 11 studies16–18,20,21,26,27,30,31,33,35 compared the operative time for the anterior approach (220.8 ± 51.5 minutes) versus posterior approach (213.9 ± 69.3 minutes), and no statistically significant difference was detected (t = 0.262).
Of the 20 studies, 11 studies16–18,20,21,26,27,30,31,33,35 compared the blood loss for the anterior approach (809.3 ± 317.3 mL) versus the anterior combined with posterior approach (1310.5 ± 524.2 mL), and no statistically significant difference was detected (t = −2.164). Among the 20 studies, 11 studies16–18,20,21,26,27,30,31,33,35 compared the blood loss for the anterior combined with posterior approach (1125.0 ± 275.5 mL) versus the posterior approach (710.4 ± 192.4 mL), and a statistically significant difference was detected (t = 4.092, P = 0.001). Among the 19 studies, 11 studies16–18,20,21,26,27,30,31,33,35 compared the blood loss for the anterior approach (778.9 ± 246.5 mL) versus the posterior approach (770.1 ± 255.8 mL), and the difference was not statistically significant (t = 0.082).
Radiographic outcome
Twenty studies11,12,14,16–18,20,22–26,28–35 reported the preoperative kyphosis angle and correction of the kyphosis angle in patients with thoracic and lumbar spinal tuberculosis (Table 3).
Preoperative kyphosis angle and correction of kyphosis angle in different procedures for thoracic and lumbar spinal tuberculosis.
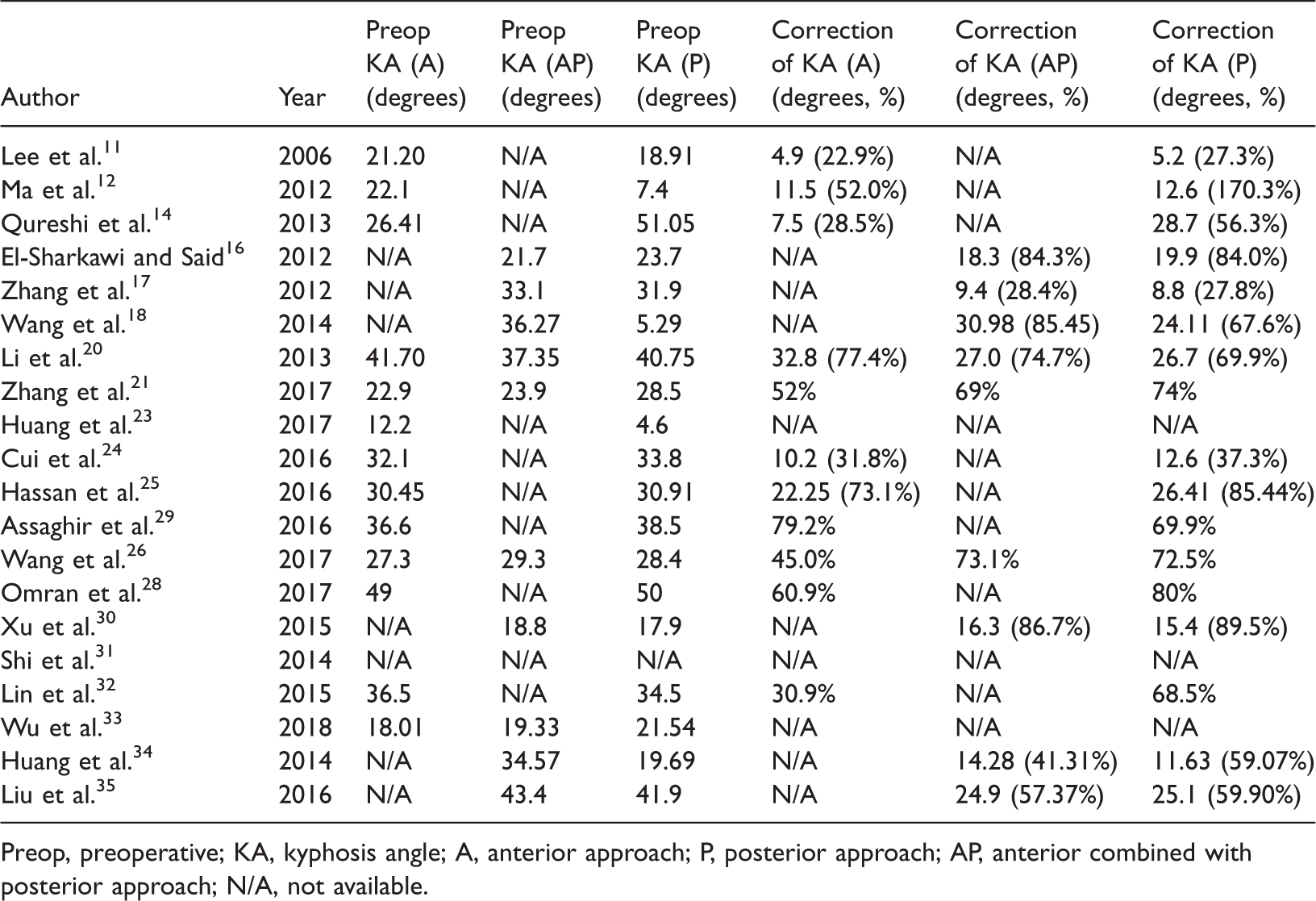
Preop, preoperative; KA, kyphosis angle; A, anterior approach; P, posterior approach; AP, anterior combined with posterior approach; N/A, not available.
Of the 20 studies, 13 studies11,12,14,20,21,23–26,28,29,32,33 compared the preoperative kyphosis angle for the anterior approach (29.0 ± 10.19 degrees) versus the posterior approach (29.9 ± 14.2 degrees), and no statistically significant difference was detected (t = −0.197). Among the 20 studies, 10 studies16–18,20,22,26,30,33–35 compared the preoperative kyphosis angle for the anterior combined with posterior approach (29.8 ± 8.5 degrees) versus the posterior approach (26.0 ± 10.9 degrees), and no statistically significant difference was detected (t = 0.871). Among the 20 studies, 4 studies20,21,26,33 compared the preoperative kyphosis angle for the anterior approach (27.5 ± 10.2 degrees) versus the anterior combined with posterior approach (27.5 ± 7.7 degrees), and no statistically significant difference was detected (t = 0.001).
Of the 20 studies, 10 studies11,12,14,20,24–26,28,29,32 compared the correction of the kyphosis angle for the anterior approach (16.7 degrees, 50.3% ± 20.4%) versus posterior approach (22.2 degrees, 73.8% ± 36.5%), and no statistically significant difference was detected (t = −1.342). Among the 20 studies, 9 studies16–18,20,22,26,30,34,35 compared the correction of the kyphosis angle for the anterior combined with posterior approach (19.9 degrees, 66.8% ± 22.8%) versus the posterior approach (19.3 degrees, 74.2% ± 23.5%), and the difference was not statistically significant (t = 0.208). Among the 20 studies, 3 studies20,21,26 compared the correction of the kyphosis angle for the anterior approach (19.0 degrees, 58.1% ± 17.0%) versus the anterior combined with posterior approach (21.6 degrees, 72.3% ± 2.9%), and the difference was not statistically significant (t = −0.349).
Surgical complications
Twenty studies11–14,16–18,20–22,24–31,33,35 reported various surgical complications in the treatment of thoracic and lumbar spinal tuberculosis (Table 4). Overall, the incidence of surgical complications was as follows: anterior approach, 103/1879 (5.48%); anterior combined with posterior approach, 126/1904 (6.62%); and posterior approach, 67/2262 (2.96%). The difference in the incidence of overall surgical complications between the anterior approach and anterior combined with posterior approach was not statistically significant (χ2 = 2.146), but that between the anterior and posterior approaches (χ2 = 16.552, P = 0.000) and that between the anterior combined with posterior approach and posterior approach (χ2 = 31.271, P = 0.000) were statistically significant.
Surgical complications of different procedures for thoracic and lumbar spinal tuberculosis.

Anti-TB, anti-tuberculous; ARDS, acute respiratory distress syndrome; CSF, cerebrospinal fluid; DVT, deep vein thrombosis; PE, pulmonary embolism; N/A, not available.
*P < 0.05, the incidence of overall surgical complication was significantly different between the anterior and anterior + posterior procedures.
Transthoracic complications included pleural effusion, pneumonia, pneumothorax, hemopneumothorax, and injury to the intercostal nerves, pleura, and lung parenchyma. The incidence of transthoracic complications was 25/294 (8.50%) in the anterior approach, 30/338 (8.88%) in the anterior combined with posterior approach, and 8/322 (2.48%) in the posterior approach. Statistically significant differences were found between the anterior and posterior approaches (χ2 = 10.531, P = 0.001) and between the anterior combined with posterior approach and posterior approach (χ2 = 12.414, P = 0.000). However, there was no statistically significant difference between the anterior approach and anterior combined with posterior approach (χ2 = 0.052).
Hardware failure was found in 14 of 249 patients (5.62%) treated with the anterior approach, in 1 of 83 patients (1.20%) treated with the anterior combined with posterior approach, and in 4 of 151 patients (2.65%) threated with the posterior approach. The incidence of hardware failure was not significantly different among the three surgical approaches.
The incidence of revision surgery was 7/57 (12.28%) in the anterior approach, 1/25 (4.0%) in the anterior combined with posterior approach, and 1/18 (5.56%) in the posterior approach. The incidence of revision surgery was not significantly different among the three surgical approaches. Further detail is shown in Figure 2.

Comparison of complications depending on the anterior, anterior combined with posterior, or posterior approach. *Statistical difference in transthoracic complications between anterior and posterior approach and between posterior and anterior combined with posterior approach (P < 0.05).
Other surgical complications included anti-tuberculosis drug-induced liver dysfunction, acute respiratory distress syndrome, chest and back pain, cerebrospinal fluid leakage, donor site problems, dural tear, deep vein thrombosis, fistula, intercostal neuralgia, intraoperative excessive bleeding, local abscess, neural effusion, nonunion, paralytic ileus, pulmonary embolism, persistent injury, postoperative paralysis, pressure ulcer, pseudarthrosis, psoas abscess, recurrence, residual neurological defects, root injury, segmental artery injury, sinus formation, superficial infection, urinary infection, vascular injury, water–electrolyte imbalance, wound dehiscence, and wound infection (Table 4).
Only one study 29 reported the recurrence rate in the anterior approach (2/57, 3.51%) and anterior combined with posterior approach (2/65, 3.08%), and the difference was not statistically significant.
Clinical outcome
All 25 studies reported the clinical outcomes of the different procedures for spinal tuberculosis in the thoracic and lumbar regions. There were no uniform criteria for the assessment of these clinical outcomes. Clinical outcomes were evaluated using the American Spinal Injury Association impairment score, Oswestry Disability Index, visual analogue scale score, Frankel grade, Denis scale, erythrocyte sedimentation rate, and C-reactive protein concentration. The 25 studies involved a total of 2295 patients: 702 who underwent the anterior approach, 1095 who underwent the posterior approach, and 498 who underwent the anterior combined with posterior approach. Overall, the clinical outcomes of all patients improved, but there was no significant difference among the three different approaches (Table 1).
Discussion
The choice of the optimal surgical method for spinal tuberculosis remains controversial and challenging. The anterior, posterior, and combined surgical approaches are the three most commonly used techniques in the surgical treatment of spinal tuberculosis. The anterior part of the vertebra and intervertebral disc is the most commonly affected area in spinal tuberculosis; therefore, the classic “Hong Kong operation” involves direct removal of the anterior spinal pathology followed by careful reduction of stress on the spinal cord and reconstruction of the area by anterior instrumentation.3–5 However, several potential adverse effects may influence the choice of the anterior surgical approach as the main treatment option: progressive kyphosis, prolonged immobilization, and graft failure. These complications are major concerns among surgeons and historically required a second-stage posterior surgical treatment 36 ; however, this treatment was subsequently developed into a one-stage operation.37–39 Several parameters are used to evaluate the management of spinal tuberculosis in the thoracic and lumbar regions, including estimated blood loss during the operation, radiographic results and others, and these parameters were compared in this systematic review to help surgeons choose the most effective surgical procedure.
The traditional operation is carried out anteriorly and therefore allows access to the spinal pathology and direct release of the obstruction. The traditional approach, which includes debridement and strut graft fusion, has therefore been widely and effectively adopted to manage spinal tuberculosis in the active state.3,38,40 Moreover, the traditional approach enables complete removal of psoas and paravertebral abscesses and restoration of the normal sagittal alignment through anterior debridement and strut graft fusion, especially in patients with severe anterior pathology involving multiple levels. In a study by Jin et al., 41 all 23 patients who underwent one-stage anterior debridement, anterior interbody autografting, and instrumentation achieved therapeutically effective outcomes. Likewise, Huang et al. 39 reported that one-stage surgical management using anterior decompression, bone grafting, posterior instrumentation, and fusion was effective for all children with spinal tuberculosis in their study.
In a study involving patients with tuberculous spondylitis, the researchers found that an operation involving posterior fusion may facilitate adequate debridement of the spinal pathology and ensure postoperative spinal stabilization. 42 Because the posterior approach does not involve the establishment of a surgical pathway through thoracotomy and thoracoabdominal access, patients of advanced age who have impaired pulmonary function are spared from further risk.16,19,38 Ma et al. 12 evaluated 217 patients and reported no significant differences in spinal cord decompression, correction of deformity, or pain relief between anterior instrumentation and posterior instrumentation. However, the posterior approach showed a higher potential for maintaining the correction of deformity. 12
The present study showed that the anterior combined with posterior approach had a longer operative time than either the anterior or posterior approach. The blood loss volume was smaller in the posterior approach than in the anterior combined with posterior approach. The posterior approach had a lower overall surgical complication rate and transthoracic complication rate than the other two approaches. The correction of the kyphosis angle and hardware failure were not significantly different among the three procedures. However, some studies have indicated that posterior instrumentation can achieve better correction of kyphosis because the anterior part of the vertebra is more commonly involved and does not allow for firm fixation.43,44 Furthermore, when using the anterior approach only, more consideration must be given to stabilization to prevent graft-associated complications, particularly when the surgery involves longer segments of the spine. 45 In this review, differences were noted in the severity of abscesses and vertebral destruction among the patients with spinal tuberculosis undergoing surgery as well as in the surgical conditions and experiences among the spine centers; this was likely to reflect the trends and characteristics of the different surgical procedures.
The authors of recently published papers have expressed a preference for increasingly more individualized surgical options tailored to different characteristics of patients with spinal tuberculosis. Nussbaum et al. 46 reported different treatment options for patients with different extents of bone involvement. In their study, only patients with high-level bone destruction of the vertebral body were qualified as candidates for aggressive debridement and fusion. Rezai et al. 5 reported that operative management with radical debridement and fusion was needed only when more than 50% of the vertebral body was destroyed. Kato et al. 47 used minimally invasive posterior instrumentation through the anterior and posterior combined approach to treat patients with extensive thoracolumbar spinal tuberculosis as a two-stage surgery. To precisely approach the spinal pathology with accurate screw fixation and avoid vascular and neurological structural damage, intraoperative fluoroscopy with a comparatively large amount of radiation 48 is used in minimally invasive surgery for spinal tuberculosis. A computer-navigated technique was developed to replace repetitive fluoroscopy and thus ensure less radiation exposure, although several studies showed no improvement in outcomes. 49 Before performing the operation, the surgical indication and proper procedure or instrumentation must be carefully considered based on the specific features of the tuberculosis pathology, surgical experience, risks of surgical complications ranging from neurological to structural, and potential radiologic and clinical outcomes.18,20,50–53
Stricter indications for surgical management should be proposed because of the potential for serious outcomes (reconstruction failure, massive bleeding, nerve root lesions, and other major complications directly related to the spinal surgery)54–56 as well as the presence of compromising conditions among different groups of patients. 57 Nene and Bhojraj 58 reported that conservative management achieved a success rate of 98% in a selected group of patients with thoracic spinal tuberculosis. In an effort to guide clinical management, Mehta and Bhojraj 19 devised a classification system based on magnetic resonance imaging results, while Oguz et al. 59 presented another standard based on clinical features and the condition of vertebral involvement. Although surgery is important in the treatment of spinal tuberculosis and significantly influences patients’ quality of life, anti-tuberculous chemotherapy should still be considered the most important factor in determining the treatment options. A proper suggestion is the use of a combination of anti-tuberculous drug therapy for more than 12 months (3HRZE/9HRE) because the recurrence of spinal tuberculosis is always relevant to failure to comply with anti-tuberculous chemotherapy.
This systematic review has three main limitations. First, although we searched the Medline and Embase databases, an incomplete literature search may have biased our analysis because we only included articles written in English; all articles written in other languages were excluded. However, we believe that the articles we included from these two databases constitute a very important part of the field. The second limitation is that the surgical procedure was not uniform; anterior, posterior, or combined approaches were used in one- or two-stage procedures with different instrumentations. Finally, we only included retrospective studies in this systematic review. There were no prospective studies comparing surgical procedures in the literature. Thus, the indications for the surgical procedures were probably different. More randomized controlled prospective studies should be designed in the future to draw a more reliable conclusion about the treatment of spinal tuberculosis in the thoracic and lumbar regions.
Conclusion
In conclusion, no justification of superiority among the three procedures was established in this systematic review. When deciding among the three procedures for treatment of thoracic and lumbar spinal tuberculosis, surgeons must thoroughly consider the patient’s specific features of spinal tuberculosis, the surgeon’s own surgical experience, the risks of surgical complications ranging from neurological to structural, and the different possible outcomes.
Footnotes
Acknowledgment
The authors thank Kevin H. Phan, who assisted with language editing.
Authors’ contributions
ZB, YG, and LL designed the study and wrote the manuscript. FF and HS helped to collect and analyze the data. ZB and YG carried out the review and modified the manuscript. All authors read and approved the final manuscript.
Data sharing statement (availability of data and material)
No additional unpublished data exist, but the prepublication history and original material are available.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by grants from the Shanghai Science and Technology Fund (17411964200), Municipal Human Resources Development Program for Outstanding Young Talents in Medical and Health Sciences in Shanghai (2017YQ030), and Incubating Progam for Clinical Research and Innovation of Renji Hospital (PYXJS16-006, PYZY16-010).