
Abstract
Study Design:
Retrospective cohort study.
Objectives:
This study aims to determine the preoperative predictors of postoperative satisfaction in transforaminal lumbar interbody fusion (TLIF) surgery in order to improve management of patient groups at high risk of dissatisfaction. We retrospectively reviewed prospectively collected data on patients who underwent open TLIF in a tertiary hospital between 2008 and 2012 with 2-year follow-up and performed multivariate analysis for their preoperative variables.
Methods:
A multivariate regression analysis was performed for the 217 patients to identify preoperative predictors of postoperative satisfaction. Clinical outcomes were evaluated using Oswestry Disability Index (ODI), North American Spine Society (NASS) Neurogenic Symptom Score (NSS), 36-item Short-Form Survey (SF-36; mean Physical and Mental Health scores), numerical pain rating scale (NPRS) for pain, and NASS Questionnaire.
Results:
Significant improvements were seen in the postoperative ODI, NSS, SF-36, and NPRS scores at 2 years (P < .05). Eighty-six percent of the patients had their expectations of surgery met, and 94.7% of the patients were satisfied with the results of treatment at 2 years. From the multivariate regression model, patients with higher preoperative NPRS pain score (odds ratio = 1.323; 95% confidence interval = 1.071-1.633; P = .009) was more likely to be satisfied at 2 years.
Conclusions:
TLIF surgery provided significant health-related quality-of-life scores and symptom improvement in terms of SF-36, ODI, NSS, and NPRS, with a high proportion of patients being satisfied with the results of surgery. Patients with higher preoperative NPRS leg pain were more likely to be satisfied at 2 years. Patient-reported satisfaction may be largely influenced by the improvement of radicular leg pain.
Introduction
Transforaminal lumbar interbody fusion (TLIF) is a safe and effective treatment of degenerative lumbar spine conditions and helps reduce pain and improve function, which is particularly important as the prevalence of lumbar degenerative cases increases. 1 –3 A patient’s satisfaction and perception of benefit from surgery are important measures of the success and effectiveness of lumbar spine surgery and are more likely to be associated with an improvement in the quality of life. 4 –6 The relationship between patients’ expectations and satisfaction and the impact on postoperative outcome is complex with conflicting results. Some patients are dissatisfied with their results of surgery even when their expectations were met by the surgery 7 and when they have achieved functional improvement. 4 Patient satisfaction has been reported to correlate most strongly with the postoperative subjective difficulty in walking. 4
The study of preoperative predictors of postoperative patient satisfaction is important for better management of patient groups at high risk of dissatisfaction and improves the outcome measures of patients undergoing TLIF surgery. Their perception of the success of their spinal surgery will determine if they will avail themselves of further health care resources. 8 Our study aims to determine if postoperative satisfaction is influenced by preoperative variables such as clinical scores, age, body mass index (BMI), number of levels of TLIF, or revision TLIF, and we aim to uncover the possible interrelations between them.
Methods
Study Design
Centralized Institutional Review Board approval was obtained for this study (CIRB 2015/2626). We retrospectively reviewed prospectively collected data on patients who underwent open TLIF from the database of a tertiary hospital by a single senior surgeon over a 5-year study period between January 2008 and December 2012, with a minimum of 2-year follow-up. All the patients included in the study underwent open TLIF due to significant symptoms of both back pain and leg pain of more than 6 months duration and have failed conservative management. Instrumentations used were posterior pedicle screws, rods and interbody fusion cages with autologous bone graft obtained from the spinous process, and laminar bone removed during the TLIF procedure. Patients were placed on a standardized postoperative clinical pathway for spine surgery and underwent supervised physical therapy postoperatively by trained physiotherapists.
Patient Metrics
Patient demographics such as age, gender, BMI, preoperative baseline clinical scores, number of levels operated, and revision TLIF surgery were analyzed in this study. Information was obtained from medical records, intraoperative notes, and radiographs. Clinical outcome was evaluated using the Oswestry Disability Index (ODI), North American Spine Society (NASS) Neurogenic Symptom Score (NSS), Short-Form SF-36 (physical component scores [PCS] and mental component scores [MCS]), and numerical pain rating scale (NPRS), graded from “0” for no pain to “10” points for maximum pain. We evaluated patients’ opinions as to whether the surgery met their expectations and whether they were satisfied with the results of their surgery, using 2 questions adopted from the validated NASS Questionnaire. The 2 questions were the following: (1) “Has the surgery met your expectations so far?” and (2) “How would you rate the overall results of surgery?” For Question 1, patients had the choice of selecting from the following answers: (1) yes, totally; (2) yes, almost totally; (3) yes, quite a bit; (4) more or less; (5) no, not quite; (6) no, far from it; or (7) no, not at all. For Question 2, patients had the choice of selecting from the following answers: (1) excellent, (2) very good, (3) good, (4) fair, (5) poor, or (6) terrible. Patients were defined as either having had their expectations met by their surgeries (responses to Question 1 = 1-4) or not having had their expectations met by their surgeries (responses to Question 1 = 5-7). Patients were defined as being either satisfied (responses to Question 2 = 1-3) or dissatisfied (responses to Question 2 = 4-6).
Statistical Analysis
All statistical analyses were performed using SPSS version 21 (SPSS, Inc, Chicago, IL) with consultation from biostatisticians. A paired t test was used to analyze the improvement in the preoperative versus postoperative 2-year outcome scores. Univariate and multivariate analyses were conducted to determine significant preoperative predictors of patient satisfaction at 2 years. Univariate associations between independent variables and postoperative satisfaction were calculated using the Wilcoxon rank test for categorical variables and Pearson’s correlation test for continuous variables. Multivariate analysis was performed for significant univariate variables of P < .2 with Kruskal-Wallis post hoc testing. Odds ratios and their 95% confidence intervals were calculated. Statistical significance was defined as P < .05.
Results
A total of 217 patients underwent TLIF by a single surgeon during the 5-year study period. Preoperative demographics of the patients are shown in Table 1. There were 84 male patients and 133 female patients. Eighty-eight patients had stable spinal stenosis without spondylolisthesis on erect flexion and extension radiological views of the lumbar spine and 129 patients had spondylolisthesis. The mean age was 61 years, and the mean BMI was 25.9. A total of 182 and 35 patients underwent primary TLIF and revision TLIF, respectively. One hundred and forty, 68, and 9 patients underwent single-level, 2-level, and 3-level TLIF, respectively. The mean length of operation was 3.5 hours, and the mean length of postoperative stay was 7.2 days. At 2-year follow-up, 191 patients had clinical outcome scores, while a total of 26 patients were lost to follow-up in our study.
Preoperative Demographics of Patients.
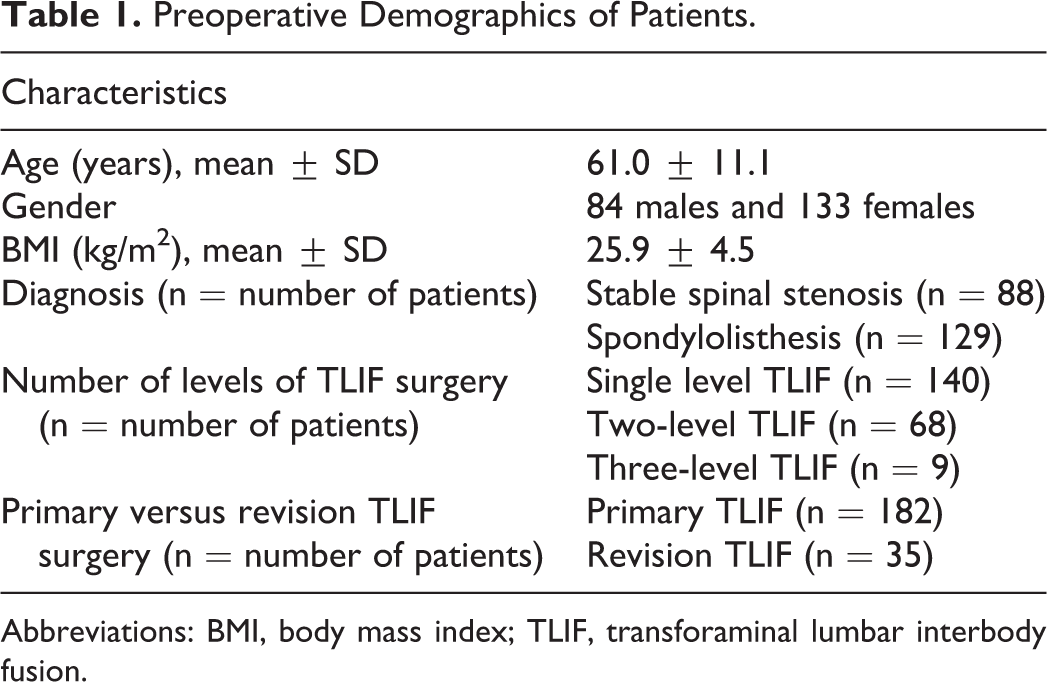
Abbreviations: BMI, body mass index; TLIF, transforaminal lumbar interbody fusion.
Significant improvements were seen in all of the clinical outcome scores at 2-year follow-up when compared to preoperatively (Table 2). As compared to the 2-year outcome scores, preoperative ODI (59.4 vs 16.2; P < .001), NSS (52.8 vs 11.1; P < .001), SF-36 PCS (36.0 vs 65.3; P < .001), SF-36 MCS (60.7 vs 79.8; P < .001), NPRS back pain scores (6.6 vs 1.2; P < .001), and NPRS leg pain scores (6.6 vs 0.7; P < .001) had statistically significant improvement. From the NASS questionnaire, 86.8% of the patients had their expectations of surgery met and 94.7% of the patients were satisfied with the overall results of treatment at 2 years. There were 10 patients who were dissatisfied with the results of their surgery. One patient underwent epidural steroid injection 1 year postoperatively. One patient had a removal of pedicle screw and rods 1 year postoperatively due to pedicle screw cut-out. One of the patients also had adjacent segment disease and underwent revision TLIF at 1 year postoperatively.
Comparison of Preoperative and Postoperative Clinical Outcome Scoresa.
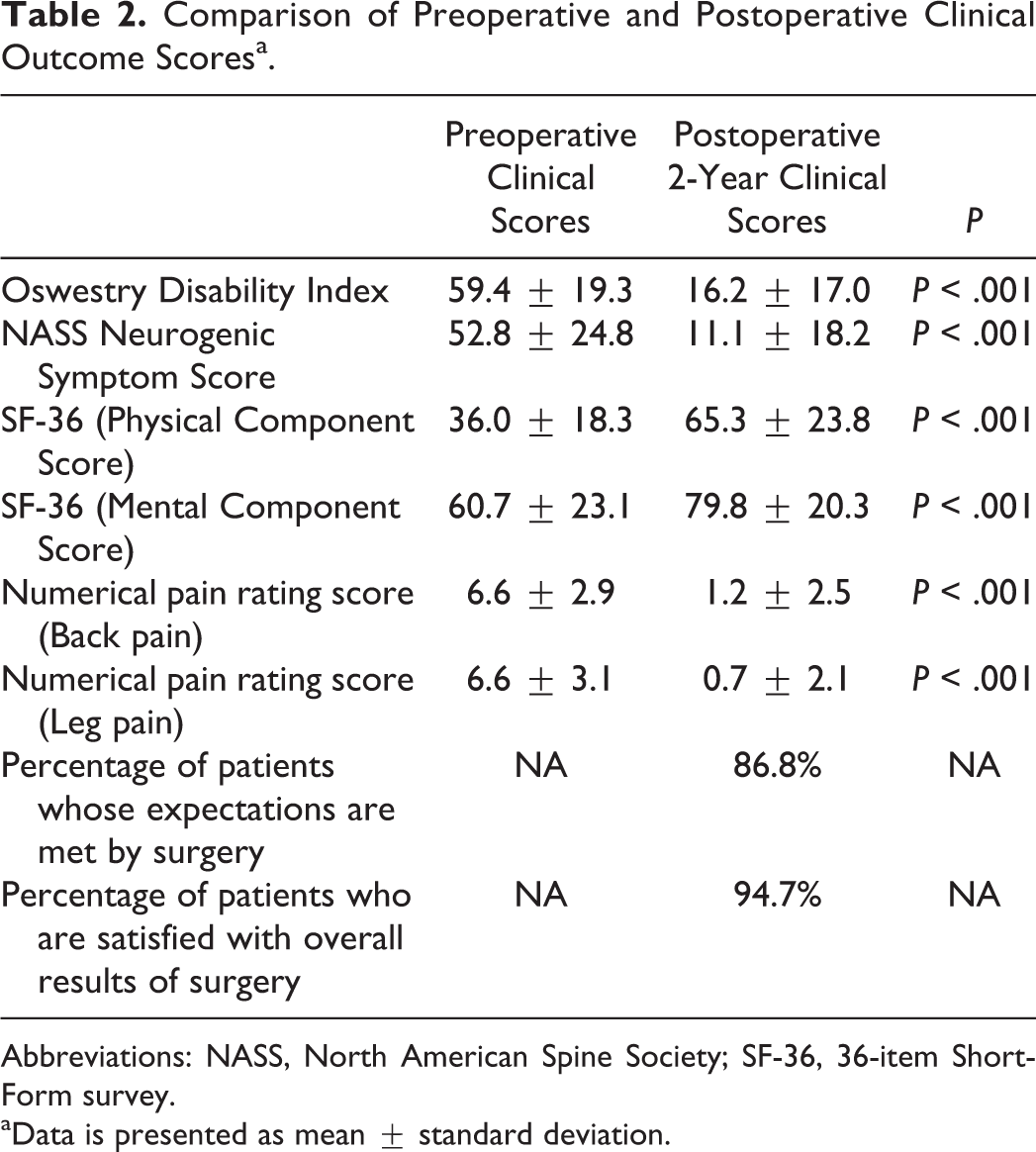
Abbreviations: NASS, North American Spine Society; SF-36, 36-item Short-Form survey.
aData is presented as mean ± standard deviation.
Continuous variables identified by univariate analysis to be significant indicators of postoperative patient satisfaction (P < .2) are SF-36 PCS, ODI, and NPRS leg pain score. For categorical variables, revision TLIF surgery was identified to be a significant indicator of postoperative patient satisfaction (Table 3). However, subsequent Kruskal-Wallis post hoc testing and multivariate analysis found that only preoperative NPRS leg pain score was a significant predictor for postoperative patient satisfaction (Table 3). Patients with higher preoperative NPRS leg pain scores (odds ratio = 1.331; 95% confidence interval = 1.074-1.649; P = .009) were more likely to be satisfied at 2 years. For each 1-point increase in preoperative NPRS leg pain score, the patient will be 1.33 times more likely to be satisfied postoperatively.
Univariate and Multivariate Logistic Regression Variables That Are Predictive of Patient Satisfaction 2 Years After Transforaminal Lumbar Interbody Fusion Surgery.
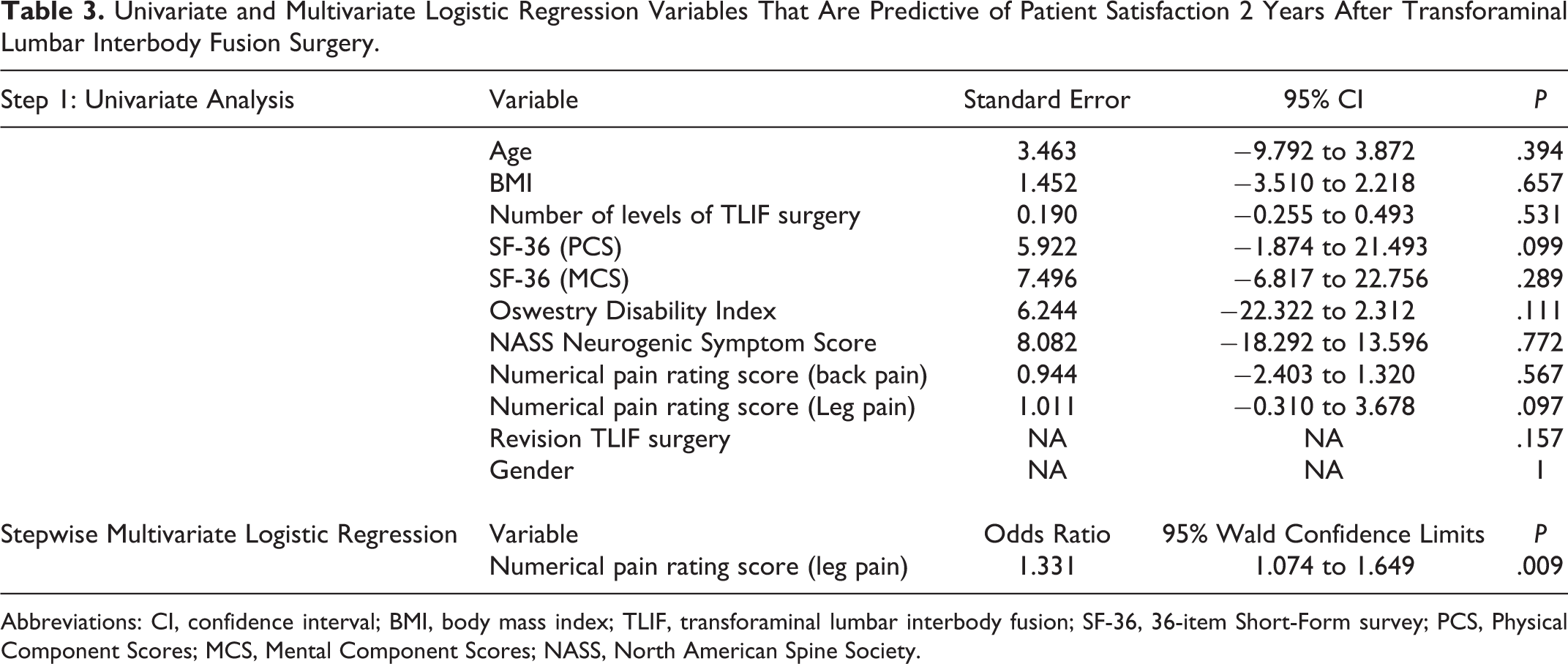
Abbreviations: CI, confidence interval; BMI, body mass index; TLIF, transforaminal lumbar interbody fusion; SF-36, 36-item Short-Form survey; PCS, Physical Component Scores; MCS, Mental Component Scores; NASS, North American Spine Society.
Discussion
Patient’s expectation is important and can be used to determine functional outcome postsurgery. 9 Expectations of surgery can be independent predictors of postoperative satisfaction, which is not associated with age, gender, marital status, and race. 10,11 A patient’s preoperative pain expectations and SF-36 score can have significant effects on postoperative clinical outcomes. Patients with more optimistic pain expectations and symptomatic relief reported better clinical outcomes following lumbar spine surgery. 8,12 It is interesting to note that although more optimistic patients who expected a complete resolution of pain were more satisfied with the results of their surgery, they have similar postoperative pain scores compared with the patient group that expected some postoperative residual pain. 12
There are complex interrelations existing between patients’ expectations and satisfaction after lumbar spine surgery, which can be influenced by the type of surgery, levels of surgery, sociodemographic factors, associated comorbidities, and also clinical presentation. 12 –19 In a study by Yamashita et al, 4 in their multivariate regression analysis, the only independent correlate for postoperative satisfaction was the subjective difficulty in walking.
In our study, TLIF surgery provided significant health-related quality-of-life scores and symptom improvement in terms of SF-36, ODI, NASS neurogenic symptom score, and NPRS (back pain and leg pain). Patients also reported high satisfaction rates, and their expectations of surgery were met postoperatively. From multivariate logistic regression for preoperative factors, we found that only preoperative NPRS leg pain score was a significant predictor for postoperative patient satisfaction. Patients with higher preoperative NPRS leg pain scores were more likely to be satisfied with their TLIF surgery postoperatively. Thus, this result suggests that the improvement in leg pain after a TLIF surgery may contribute largely to postoperative satisfaction. In our study, we did not find any correlations between a patient’s gender, age, BMI, number of levels of TLIF surgery, or revision surgery and postoperative patient satisfaction.
Regardless, the majority of patients have high postoperative satisfaction rates and also had their expectations met by surgery, which corresponds to the significant improvement in postoperative clinical scores. This could be attributed to the decompression and restoration of intervertebral disc height by their TLIF surgery, which may influence their final clinical scores. However, patient-reported satisfaction is shown to be multifactorial and may also have been largely influenced by their expectations of surgery. This highlights the importance of managing patients’ expectations preoperatively as a means of improving postoperative patient satisfaction and outcomes. 7 –9,12,18,20 Also, optimizing preoperative factors such as mental health, optimism, and avoiding unrealistically high expectations of surgery are important for patients undergoing surgical procedures to achieve patient satisfaction. 12,21 –25
In the Spine Patient Outcomes Research Trial, 26,27 patients who underwent surgical management as compared to nonsurgical management for symptomatic lumbar degenerative spondylolisthesis and lumbar spinal stenosis had substantially greater improvement in pain and function scores, which were maintained at 4-year follow-up. As this is a pilot study in our center evaluating preoperative predictive factors that are associated with patient satisfaction postoperatively, we only utilized the 2-year outcome scores. We plan to continue to follow-up these patients prospectively to evaluate if these factors will be consistent at a longer term follow-up, that is, at 4 years.
There are several limitations to our study. This study is a retrospective review of patients who were operated on by a single surgeon. Nonetheless, all our patients were placed on a standardized postoperative clinical pathway for all spine surgeries and all underwent a similar rehabilitation protocol by trained physiotherapists. Our study did not include confounding factors such as the patients’ comorbidities and also did not evaluate their preoperative expectations of surgery. However, we have employed well-validated outcome scores such as NASS neurogenic symptoms score, ODI, and SF-36, along with the validated postoperative NASS questionnaire to evaluate their satisfaction and expectations of surgery.
Conclusions
TLIF surgery provides significant improvement in health-related quality-of-life scores and symptom improvement in terms of SF-36, ODI, NSS, and NPRS, with a high proportion of patients being satisfied with the results of surgery. Patients with higher preoperative NPRS leg pain scores were more likely to be satisfied at 2 years postoperatively. Preoperative factors that influence patient-reported satisfaction of TLIF surgery may be largely influenced by the improvement in radicular leg pain postoperatively.
Footnotes
Authors’ Note
This study was performed at Singapore General Hospital, Singapore, Republic of Singapore.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.