
Abstract
Study Design
Clinical and basic study.
Objectives
This study aimed to investigate whether transforaminal lumbar interbody fusion (TLIF) using 2 banana-shaped cages leads to good clinical outcomes.
Methods
First, we conducted a clinical study to compare outcomes among patients who underwent TLIF using different types or numbers of cages. Propensity matched patients in each group were reviewed. Thirty-four patients who underwent surgery with 2 bullet-shaped cages (group A), 34 with a banana-shaped cage (group B), and 34 with 2 banana-shaped cages (group C) were compared. Twelve months after the surgery, bony fusion and cage subsidence were evaluated.
Results
The mean amount of cage subsidence was 14.9% in group A, 19.9% in group B, and 11.8% in group C. Subsidence in group B was significantly greater than that in group C (P < .01). Radiological bony fusion was not achieved in 2 cases in group B. Second, we performed a finite element model (FEM) analysis to determine the biomechanical stress of the vertebral endplate by comparing the single-banana cage construct with a double banana-shaped cage construct. FEM analysis showed that the maximum stress of the endplate in the single-cage model was 1.72-times greater than the maximum stress in the double-cage model. Furthermore, the maximal stress in the single-cage model was significantly higher than in the double-cage model during lumbar extension and side bending.
Conclusion
This study showed that TLIF with double banana-shaped cages led to good clinical outcomes with less cage subsidence, probably because of decreased mechanical stress on the vertebral endplate.
Introduction
The transforaminal lumbar interbody fusion (TLIF) is one of the most popular techniques for spinal fusion and is performed for various lumbar spinal disorders such as low back pain, radicular pain, and cauda equina symptoms. 1 In recent years, lateral lumbar interbody fusion (LLIF) has been used frequently, as it offers indirect decompression of the spinal canal and neural foramen. Extreme lateral interbody fusion (XLIF) and oblique lumbar interbody fusion (OLIF) are safe and effective procedures that result in at least equivalent clinical improvements with lower procedural morbidity compared to conventional open TLIF techniques.2,3 However, for lower levels of the lumbar spine, L4/5 and L5/S1, LLIF is not always indicated because of the anatomical difficulty in the surgical approach. Therefore, TLIF remains the primary strategy for interbody fusion of the lower lumbar spine.
The goal of TLIF is to achieve stability between the 2 vertebral segments and restore disc height and physiological spinal alignment. 4 Achieving solid fusion is essential for good postoperative outcomes after fusion surgery in the lumbar spine. Subsidence of the interbody cage, on the other hand, is a potential complication of spinal interbody fusion that might have a severe impact on postoperative outcomes. Cage subsidence can lead to progressive spinal deformities, recurrence of neural foraminal stenosis and spondylolisthesis.5,6 The use of large cages is one of the solutions to prevent cage subsidence in the TLIF technique. The large cages significantly restore stiffness of the spine after interbody fusion. 7 According to a previous report, the cage size may influence lateral bending and rotational stability. 8 TLIF with 2 banana-shaped cages is 1 option to make the cage contact area larger than that of the other cage constructs for TLIF. The results of TLIF with double banana-shaped cages are unknown at this time. Here, we performed a study to investigate whether TLIF using 2 banana-shaped cages leads to good clinical outcomes. First, we conducted a clinical study to compare outcomes among patients who underwent TLIF using different types or numbers of cages. Second, we performed a finite element model (FEM) analysis to demonstrate the mechanisms of superiority and to prevent postoperative subsidence in double banana-shaped cage constructs.
Materials and Methods
Clinical Study
Patients and Surgical Procedures
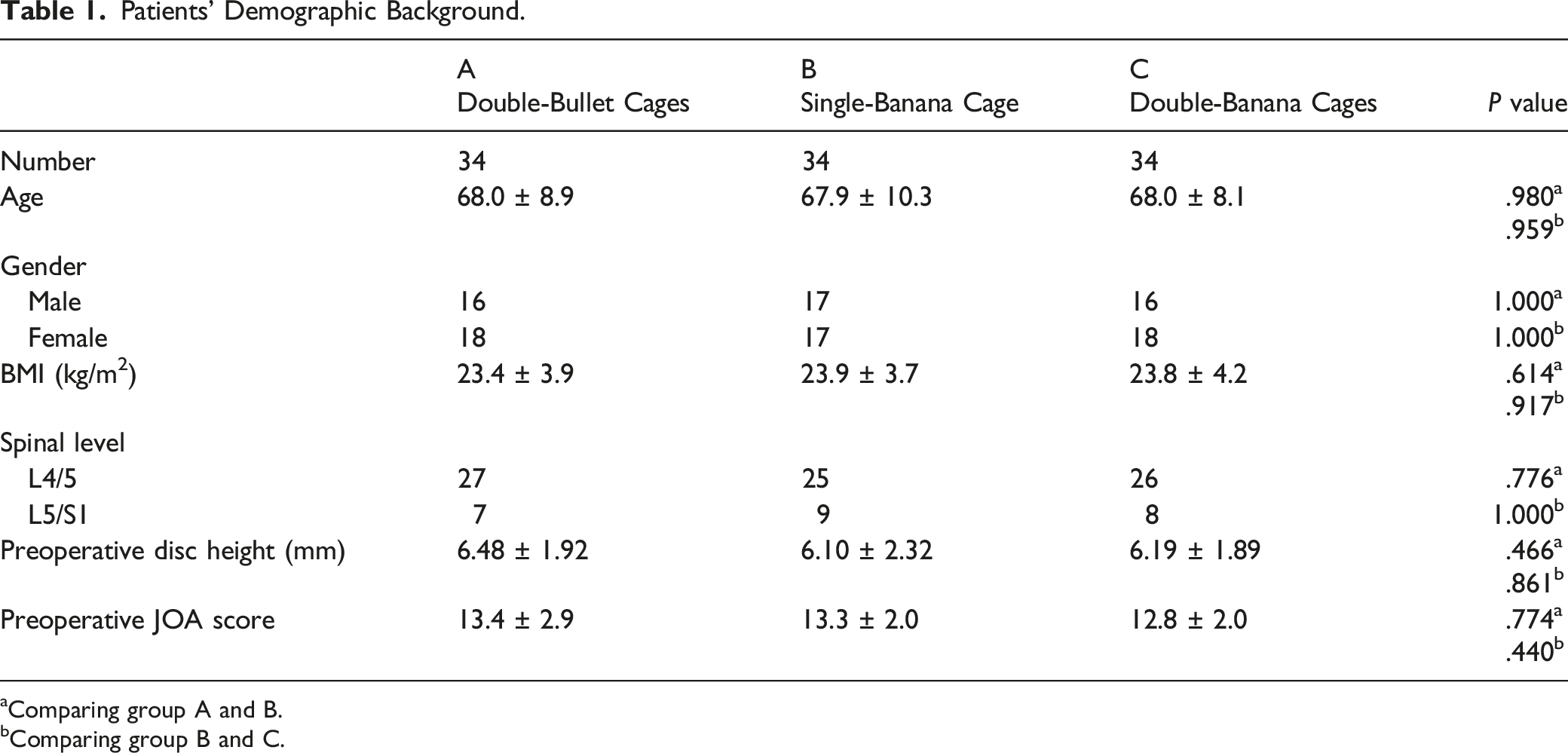
There were 191 consecutive patients who underwent single-level TLIF of the lower lumbar spine (L4/5 or L5/S1), from 2013 to 2021. This study was performed after an approval from the institutional review board (IRB)/ethics committee of Gifu Prefectural General Medical Center (IRB No. 379-4), and an informed consent was obtained from all participants. The patients were divided into 3 groups depending on the type and number of interbody cages. Of those, 34 propensity matched patients (estimated with some variables including age, gender, body mass index, preoperative disc height, and preoperative JOA score) in each group, total 102 patients, were retrospectively reviewed. Thirty-four patients who underwent surgery with 2 bullet-type cages (group A), 34 with 1 banana-shaped cage (group B), and 34 with 2 banana-shaped cages (group C) were compared (Figure 1). Three senior surgeons chose the type or number of cage(s). Post-match analysis found no differences among the 3 groups for age (68.0 ± 8.9, 67.9 ± 10.3, and 68.0 ± 8.1), gender (16 male, 17 male, and 16 male), body mass index (BMI) (23.4 ± 3.9, 23.9 ± 3.7, and 23.8 ± 4.2) and preoperative disc height (6.48 ± 1.92, 6.10 ± 2.32, and 6.19 ± 1.89). Patient demographic information, including affected spinal level, and preoperative Japanese Orthopaedic Association (JOA) score, were also similar among the 3 groups (Tables 1 and 2). Patients with a history of spinal trauma, tumors, surgical intervention, and infectious diseases were excluded from the study. Additionally, patients with inappropriate interbody cage position were also excluded from the study. Intervertebral cage construct of 3 groups. Position and number of the cage(s) are shown. Patients’ Demographic Background. aComparing group A and B. bComparing group B and C. Radiographic and Clinical Evaluations of the Patients. aComparing group A and B bComparing group B and C cComparing the data at 12 months postoperatively.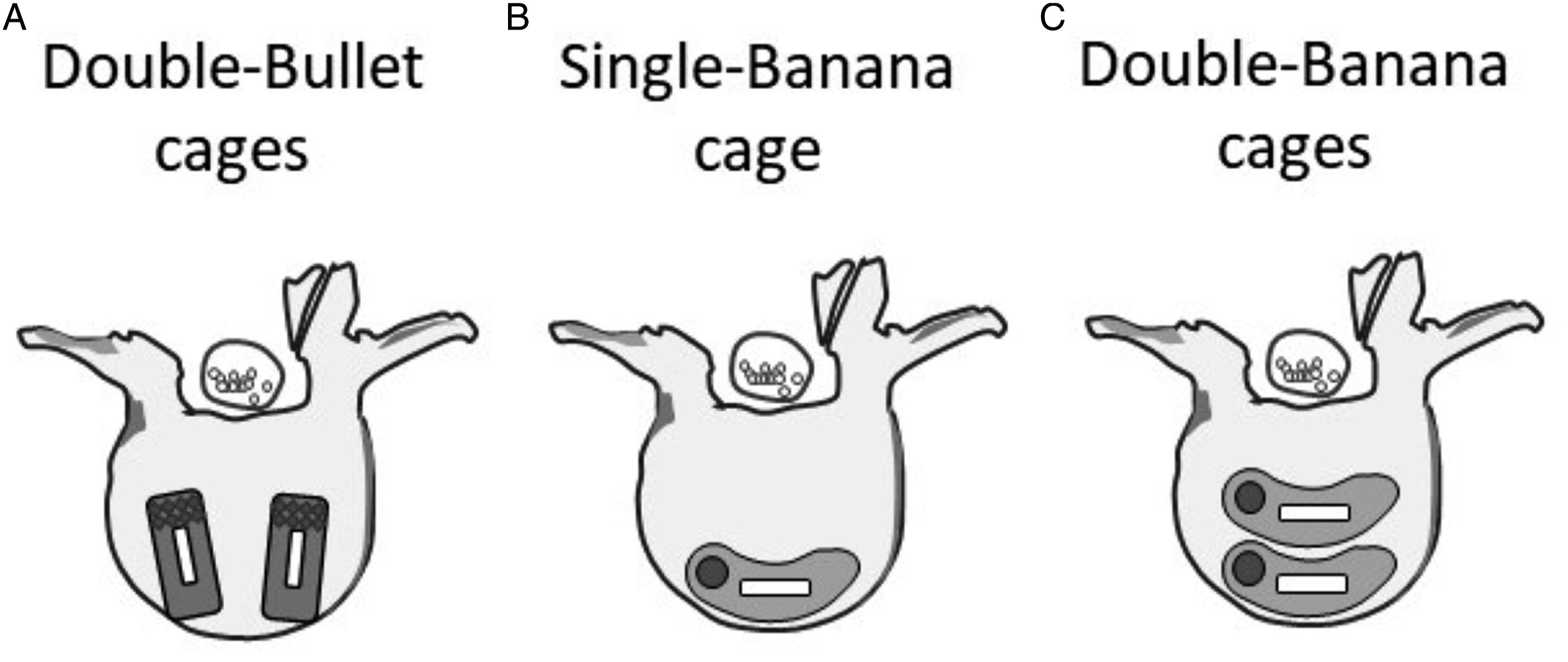
A unilateral transforaminal approach was used in this surgical technique. A unilateral complete facetectomy was performed using a chisel or a high-speed drill. Based on the patient’s neurological symptoms, decompression of the central canal and lateral recess was performed. The intervertebral disc and endplate cartilage were removed, and a cage was inserted through a monoportal trajectory. Three senior surgeons performed the surgery, with a similar career as the spine surgeon, and had equal surgical skills. The type and number of cages used were based on the surgeon’s choice. The obtained autogenous local bone was crushed and used to fill the cage and intervertebral spaces. Finally, the vertebrae were stabilized using pedicle screws. In group C, height of posteriorly placed cage was shorter than anteriorly placed cage (usually shorter height by 1 mm). And then, intervertebral compressive force was applied at final rods fixation. Those procedures made it possible to keep segmental lumbar lordosis.
The bullet-shaped cage was approximately 10 mm wide, 23-25 mm long, and 8-11 mm in height (contact surface area was 230-250 mm2), and the banana-shaped cage was approximately 11 mm wide, 23-28 mm long, and 8-11 mm in height (contact surface area was 253-308 mm2). The material used for each cage was polyether ether ketone (PEEK). Bullet-shaped cage mainly used was Novel SD (Alphatech Spine, CA) or MectaLIF Posterior (Madacta International, Switzerland). And banana-shaped cage mainly used was Novel Tapered TL, (Alphatech Spine, CA) or T-PAL Interbody Spacer (Depuy Synthes, CO). All patients were kept in a rigid orthosis for 3 months after surgery and then mobilized without an external orthosis.
Radiographic Evaluations
The local lordotic angle of the operated segment was measured using Cobb’s method between the upper endplate of the upper vertebra and the lower endplate of the lower vertebra on the lateral-view radiogram. The disc height was measured and calculated according to the methods reported by Allaire et al. A midline drawn from the posterior midpoint to the anterior midpoint of the vertebral disc space. The sum of the perpendicular distances from both the cranial and caudal corner morphometry points of the vertebral body to the disc midline was measured and calculated. Then, the individual anterior, mid, and posterior disc heights were averaged, and mean value was defined as the estimated disc height. 9 Subsidence of the cage was evaluated by comparing the disc height in lateral radiographs immediately after the surgery and a year after the surgery. The amount of cage subsidence into the vertebral endplates was measured and classified according to previously reported manner: Grade 0, 0%-24%; Grade I, 25%-49%; Grade II, 50%-74%; and Grade III, 75%-100%. 10
Interbody bony fusion was assessed by analyzing lumbar flexion and extension lateral radiographs and computed tomography (CT) images. Fusion was defined as the presence of continuous trabecular bone formation through or outside the cages and less than 3° of movement on lateral flexion and extension radiographs. 11
Clinical Evaluations
The clinical outcomes were based on recovery rates, which were calculated according to the criteria proposed by the JOA score. The recovery rate was calculated as follows: recovery rate = 100 × (postoperative JOA score − preoperative JOA score)/(29 − preoperative JOA score). Radiographic and clinical evaluations were performed preoperatively, immediately and a year after surgery.
Statistical Evaluations
Data was entered into a Microsoft Excel spreadsheet (Version 2111, Microsoft Office 2019, Microsoft Redmond, WA., USA). All statistical analyses were performed using EZR, version 4.1.2., a modified version of R Commander designed to add statistical functions frequently used in biostatistics. 12 Statistical analyses were performed using the unpaired t-test or Fisher’s exact test. Data are presented as mean ± standard error of the mean. Statistical significance was set at a P value less than .05.
Basic Study
Finite Element Models
CT images of the L4 and L5 vertebrae were obtained from a healthy young man (age, 25 years; height, 173 cm; and weight, 65 kg). FE models of the vertebrae were generated from the digital CT images using Mechanical Finder (MF) software version 11.0 (Research Centre of Computational Mechanics, Inc, Tokyo, Japan). This created an FE model that indicated the shape of the individual bone and the distribution of its density.
13
Within this software, FE mesh models were generated using ANSYS ICEM CFD version 19.0 (Ansys Inc, Canonsburg, Pennsylvania) and modelled as a .5-2.0 mm tetrahedral element for cancellous and cortical bone. Regions of interest (ROI) models were semi-automatically constructed in the 3D-planning software Zed View (version 12.0; LEXI, Tokyo, Japan). The pedicle screws, rods, and interbody cage computer-aided design (CAD) data were precisely placed in the vertebral ROI model by perfectly matching the CT in the Zed View software. Subsequently, a composite ROI of the vertebrae and spinal instruments was imported into the MF software for analysis.
14
In the model, pedicle screws (6.0 mm in diameter, 50 mm in length) inserted through every pedicle were connected by 2 rods (5.5 mm in diameter, 50 mm in length). A banana-shaped cage was placed between the vertebral bodies. Two surgical constructs were modelled and analyzed. In the first single-banana cage model, a banana-shaped cage was placed within the anterior one-third of the disc space. In the double-banana cage model, the anterior cage was placed within one-third of the disc space, and the second cage was placed just behind the anterior cage (Figure 2). Finite element models of the L4 and L5 vertebrae with cage(s), screws, and rods, showing a single-banana shaped cage construct (left) and double-banana shaped cage (right).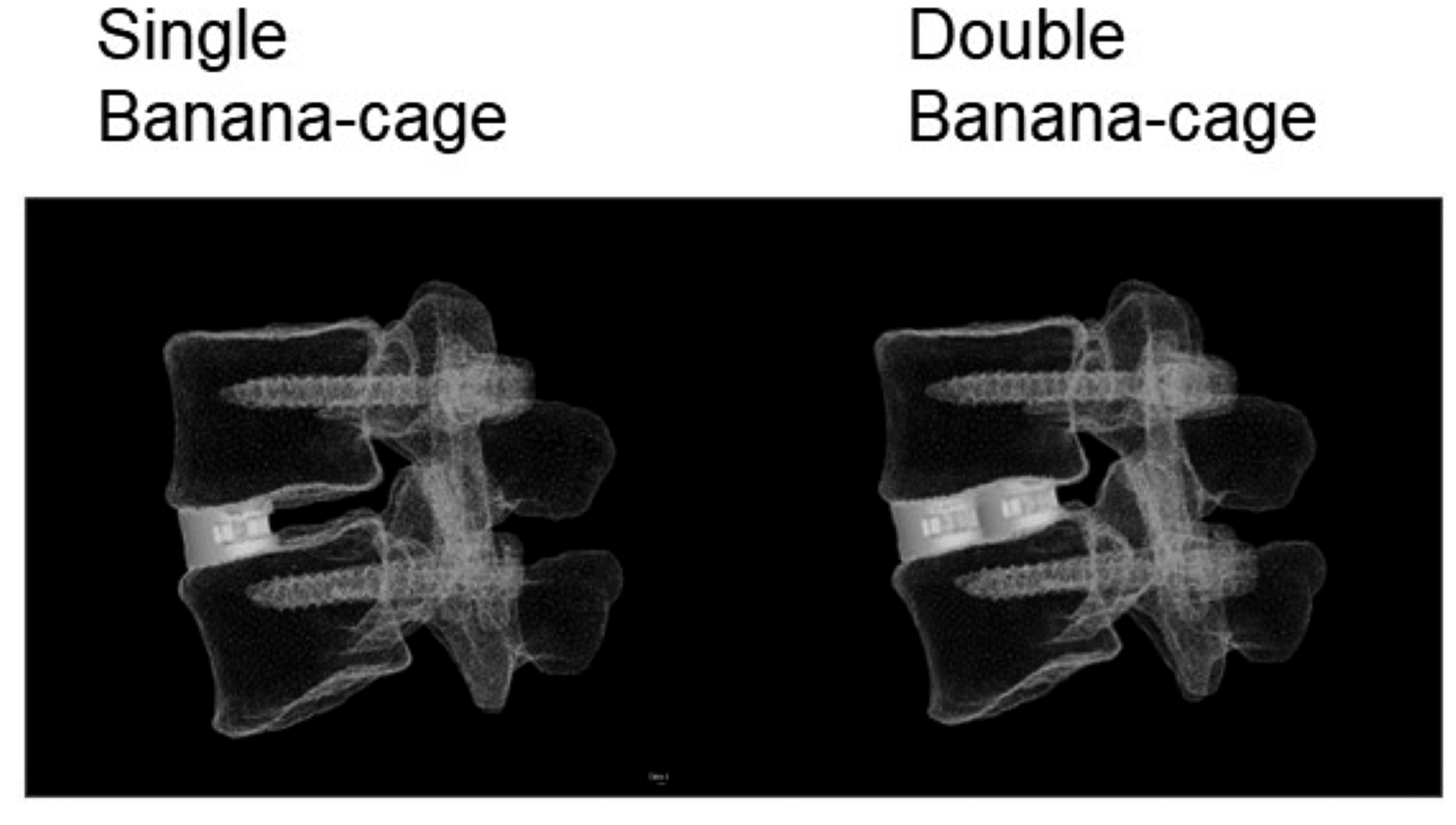
The elastic modulus of the bone was based on CT density values using the equations proposed by Keyak et al. 15 The Poisson’s ratio of the bone was .40. The element types and material properties used in the FE model were defined in accordance with previous literature.16-18 The screws and rods were defined to have the material properties of a titanium alloy with a Young’s modulus of 110,000 MPa and a Poisson’s ratio of .28. The interbody cage was defined to have PEEK properties, with a Young’s modulus of 3600 MPa and a Poisson’s ratio of .25.
Loading Conditions
The lower surface of the L5 vertebra was also constrained. An axial loading of 400 N was imposed on the superior surface of L4 to simulate the physiological weight loading conditions. Another 8 Nm was then applied to the L4 vertebra to simulate flexion, extension, side bending, and axial rotation motions between L4 and 5 in the same manner as previously reported.18,19 The maximum von Mises stress of the cortical endplate was measured and compared among the different constructs. Then, the maximum von Mises stress at the anterior area of the cortical endplate, which is in contact with the anterior cage, was measured and compared between the 2 surgical constructs.
Results
Clinical Study
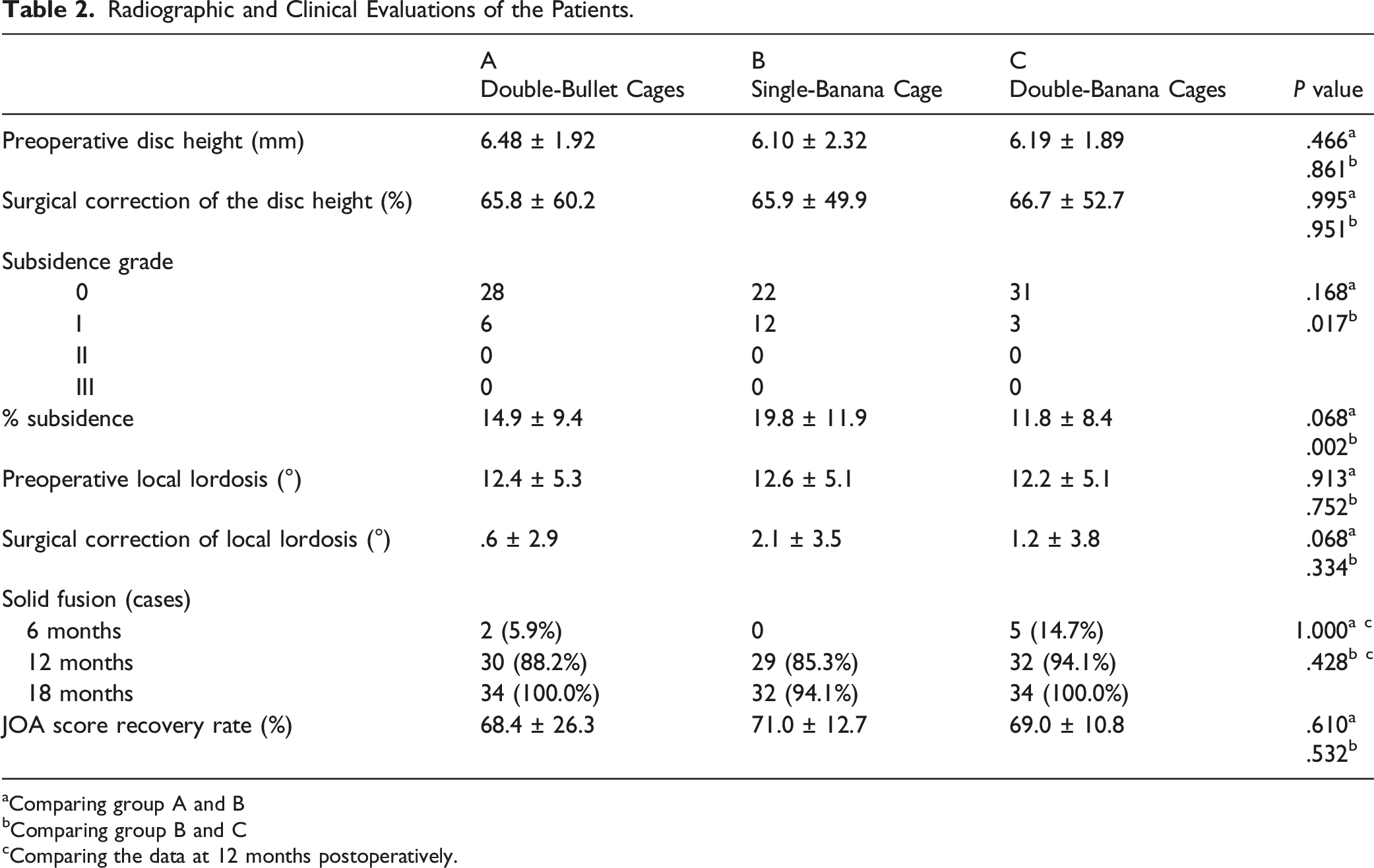
The preoperative mean disc height in group A was 6.48 mm, 6.10 mm in group B, and 6.19 mm in group C (Table 2). There were no statistically significant differences between the groups. Furthermore, surgical correction of the disc height (an increase in the disc height during surgery) was not different among the 3 groups (65.8% in group A, 65.9% in group B, and 66.7% in group C). In contrast, the amount of cage subsidence was 14.9% in group A, 19.9% in group B, and 11.8% in group C. Subsidence in group C was significantly less than that in group B (P < .01). No significant difference in subsidence was observed between Groups A and B (P = .064) or Group A and C (P = .681). Number of the patients with subsidence grade Ⅰ in Group A, B and C was 6, 12 and 3, respectively (Table 2). On the other hand, the preoperative mean local lordosis in group A was 12.4°, 12.6° in group B, and 12.2° in group C (Table 2). Surgical correction of the local lordosis (an increase of lordotic angle after surgery) was not significantly different among the 3 groups (.6° in group A, 2.1° in group B, and 1.2° in group C).
Four patients in group A were regarded as non-union a year after the surgery, as were 5 cases in group B, and 2 cases in group C. Of those, all cases in groups A and C, and 3 cases in group B were finally regarded as complete union 18 months after the surgery. In contrast, complete fusion was not obtained in 2 patients in group B 18 months postoperatively. Regarding the evaluation of bony fusion, the Kappa coefficient of interobserver agreement was .958, the reliability of the classification was excellent. Good recovery of the JOA score was obtained in every group, and the recovery rate of the JOA score a year after surgery did not differ among the 3 groups (68.4% in group A, 71.0% in group B, and 69.0% in group C) (Table 2).
FEM Analysis
The maximum von Mises stress of the L4-5 vertebrae is shown in Figure 3. Under axial loading in the neutral position, the maximum stress on the anterior aspect of the vertebral body was significantly greater in the single-cage model than in the double-cage model (Figure 3). With extension, the maximum stress at the pedicles of L4 and 5 seemed to be greater in the single-cage model. Finite element models of the L5 vertebra. An axial loading of 400 N was imposed on the superior surface of L4 to simulate the physiological weight loading conditions. Another 8 Nm was then applied to the L4 vertebra to simulate flexion, extension, side bending, and axial rotation motions between L4 and 5. Figures show the maximum von Mises stress of the upper cortical endplate of the L5.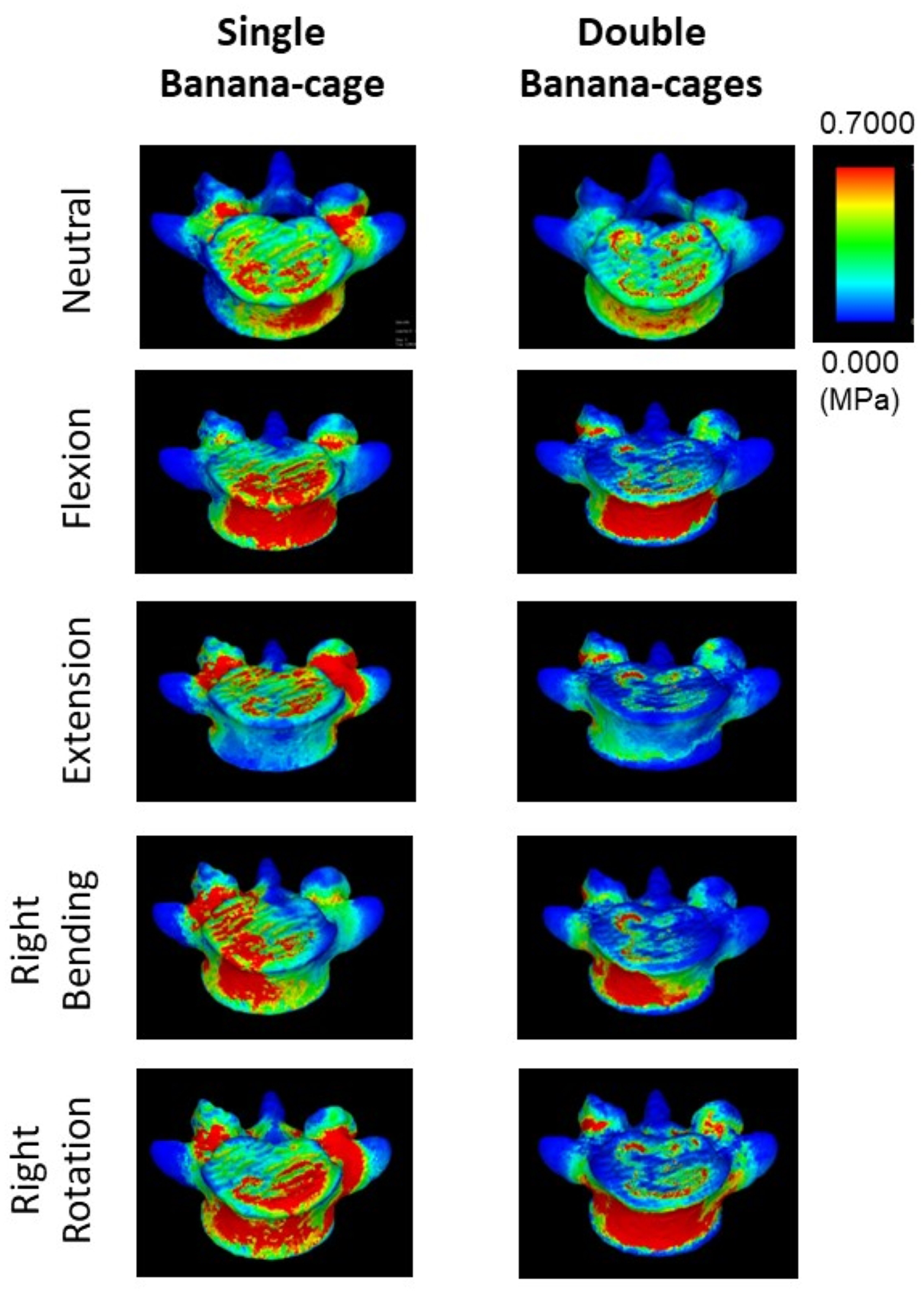
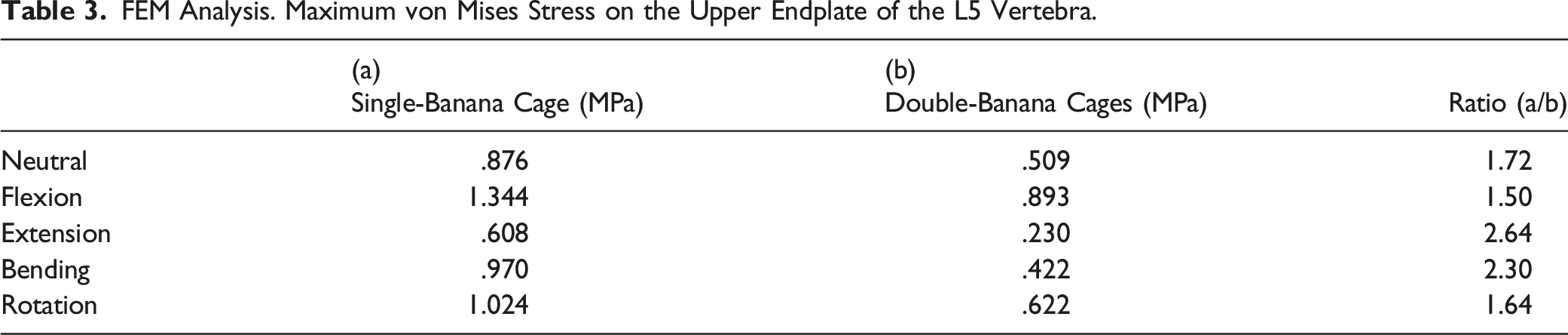
The maximum von Mises stress on the upper endplate of L5 was also evaluated and quantified, as shown in Figure 4 and Table 3. The maximum stress of the endplate in the single-cage model (.876 MPa) was 1.72-times greater than the maximum stress in the double-cage model (.509 MPa) (Figure 4, Table 3). Under additional motion stress (flexion, extension, right bending, and right rotation), the maximum stress was greater in the single-cage model than in the double-cage model (1.344 MPa vs .893 MPa in flexion, .608 MPa vs .230 MPa in extension, .970 MPa vs .422 MPa in bending, and 1.024 MPa vs .622 MPa in rotation). In particular, with extension or side bending, the maximum stress was more than 2 times greater in the single-cage model than in the double-cage model (Figure 4). Maximum von Mises stress on the upper cortical endplate of the L5. Maximum stresses at the anterior area of the cortical endplate of the L5, which contacts the anterior cage, were measured and compared between the 2 surgical constructs. The bar graph shows maximum stress during neutral position, flexion, extension, right side bending, and right rotation. White bar shows maximal stress in the single-cage model, and gray bar shows that in the double-cage model. FEM Analysis. Maximum von Mises Stress on the Upper Endplate of the L5 Vertebra.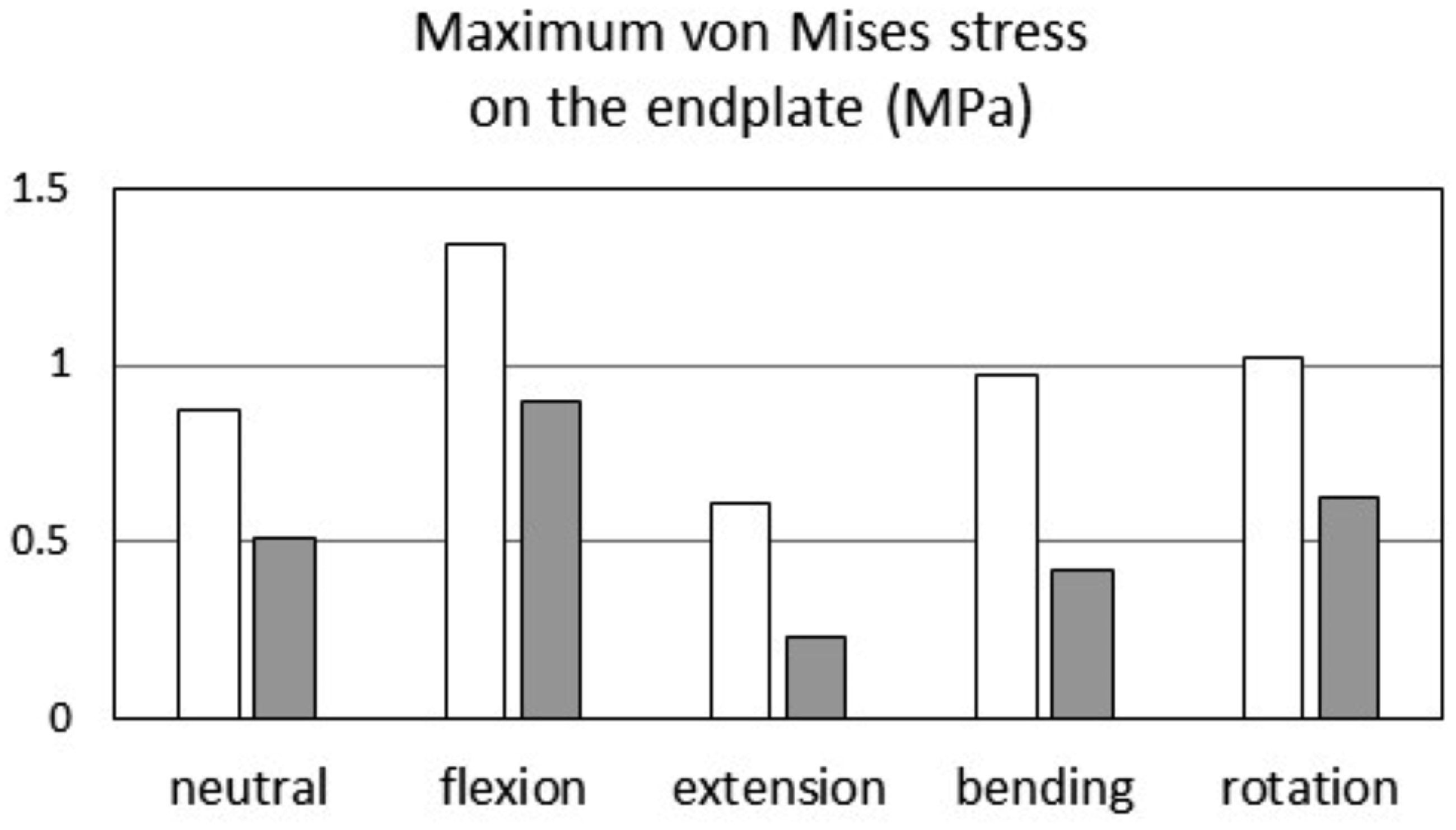
Discussion
Rigid and stable interbody support is essential to obtain solid bony fusion and to prevent cage subsidence during lumbar interbody fusion surgery. Some factors that affect the postoperative stability of the cage have been reported. The shape and material of the cage, cage position, and amount of surgical correction of the disc height may be influencing factors.20-23 In particular, in the case of the posterior-approached lumbar interbody fusion technique, facetectomy is conducted in most cases to access the interbody space as well as to perform our surgical procedure. After facetectomy, the functional stiffness of the spine is significantly reduced compared with that of the intact spine in extension (48% of intact), lateral bending (25%), and rotation (39%). 7 Therefore, constructional vertebral stability using interbody cages is a particularly important consideration.
The size of the contact surface area of the cage is likely an important factor in preventing cage subsidence. Several previous studies have demonstrated a correlation between the size of the cage contact surface area and vertebral stability after lumbar interbody fusion. Goh et al performed an in vitro biomechanical study comparing cages with various contact surface areas and sizes. They found that the size of the cage contact surface influences lateral bending and rotational stability. Large cages significantly restore spinal stiffness after posterior lumbar interbody fusion. 7 Yuan et al reported that the size of the cage contact surface was strongly correlated with the subsidence of the cage after surgery. They measured the force required for subsidence in an in vitro biomechanical study using mechanical compression devices to compare various sizes of bullet cages and LLIF cages. They found that the LLIF cage, which had the largest contact surface area (810-1210 mm2), showed a significantly higher subsidence resistant potential. 8 Lu et al conducted a FEM analysis comparing various lumbar fusion models, including posterolateral fusion (PLF), TLIF, and LLIF. They measured mechanical stress on the vertebral endplates and found that LLIF with a large contact surface induced fewer stress peaks than TLIF with a single-banana-shaped cage. 18
Thus, a cage with a large contact surface area has a great advantage in preventing cage subsidence and maintaining the stability of the constructs. However, the effect of interbody fusion with double banana-shaped cages is not fully understood. This is the first study to biomechanically evaluate TLIF using double banana-shaped cages. In this study, we investigated clinical outcomes after surgery. The results showed that subsidence in the single-banana cage group was significantly higher than that in the double-banana cage group, with a similar bone union rate and JOA score recovery. Furthermore, a biomechanical study was conducted using FEM analysis to verify the mechanism of the results obtained from our clinical data. Our data showed that TLIF with double banana cages resulted in less vertebral endplate stress than that with a single-banana cage. Under physiological axial loading, the maximum stress of the endplate in the single-cage model was 1.72-times greater than the maximum stress in the double-cage model. Additionally, during lumbar extension and side bending, the maximum stress was more than 2 times greater in the single-cage model than in the double-cage model. These results can explain the mechanisms of the results in our clinical study; cage subsidence in the single-banana cage group was significantly greater than that in the double-banana cage group.
Other potential risk factors also affect cage subsidence. The position of the cage was previously reported to be an important factor related to the surgical technique. According to the literature, posterior positioning of the cage is a potential subsidence risk factor.24,25 Therefore, anterior positioning of the cage is ideal for preventing cage subsidence. In the double-banana cage group, the first anterior cage had to be positioned in the anterior one-third of the disc space to maintain enough space for inserting another posterior cage. This could be another possible reason for the lower incidence of subsidence in the double banana cage construction. Singhatanadgige et al reported that using excessively high cages (>12 mm) is also a risk factor for cage subsidence. 24 In our patients, the operative correction of disc height was not different among the groups. Therefore, this may not have been the main reason in our study.
There are technical knacks in double-banana cages TLIF. Firstly, intervertebral disc material and cartilage endplate should be sufficiently removed. If clearance of the intervertebral space is insufficient, it might be difficult to insert 2 banana cages. Secondly, anterior cage should be positioned at the anterior third of the disc space in order to keep enough space for posterior cage. Finally, posterior cage should be gently inserted into the posterior half of the disc space along posterior aspect of the anterior cage. Surgeon should be careful not to push out the first cage by the second cage. Bone graft can be positioned at both lateral sides of the cages.
We recognize that there are some limitations in this study. Firstly, it was retrospective study with small sample size. Secondly, there may have been a bias in choosing a type of cage(s) which were selected by 3 different surgeons. The type and number of cages used were based on each surgeon’s choice. However, we believe that the bias was minimized by conducting every surgery with the use of standardized surgical procedure and similar spinal implants as stated above. Furthermore, patient with inappropriate interbody cage position was excluded from the study. Thirdly, bone mineral density (BMD) was not evaluated in our patients. Low BMD is known as an important risk factor that contributes to cage subsidence.25,26 Okano et al recently demonstrated that obesity, diabetes, and epidural steroids affect the BMD in the lumbosacral spinal region. 27 We did not evaluate BMD in all our patients, but the age of the patients in every group was almost identical. Therefore, we hypothesized that BMD was similar among the groups. Further prospective study with large sample size and consideration of osteoporosis and other patient-specific risk factors would be required to demonstrate the efficacy of TLIF with double banana-shaped cages.
Conclusions
This study suggested that TLIF with double banana-shaped cages led to good clinical outcomes with less cage subsidence, probably because of the decreased mechanical stress on the vertebral endplate during weight loading and lumbar motion stress, including extension and side bending.
Footnotes
Acknowledgments
This study and the research behind it would not have been possible without exceptional support. We are especially grateful to Medacta International (Switzerland) for kindly providing computer-aided design (CAD) data for pedicle screws, rods, and cages, which are essential for generating finite element models of postoperative constructs.
Author Contributions
Conception and design: Fushimi, Miyagawa. Acquisition of data: Fushimi, Nozawa, Iwai. Analysis and interpretation of data: Fushimi, Nozawa, Iwai. Drafting the article: Fushimi, Miyagawa. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Fushimi. Study super-vision: Miyagawa, Akiyama.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.