
Abstract
Study Design:
Retrospective case series.
Objective:
Short posterior stabilization with vertebroplasty is one treatment option for thoracolumbar burst fractures (AO A3). Whether it avoids progression in segmental kyphosis, especially after implant removal, is unclear. In a retrospective case-control study, its stability and the effect on intervertebral discs with and without implant removal was studied.
Methods:
Fifty-nine consecutive patients were treated with bisegmental short posterior instrumentation and additional vertebroplasty of the fractured vertebra. Twenty-nine patients (male/female 17/12; age: 41.7 ± 15.4 years) underwent implant removal. Changes of segmental kyphosis and disc heights between both groups (with and without implant removal) were compared on lateral X-rays preoperative, postoperative, after 1 year and after implant removal. Risk factors for loss of reduction were analyzed.
Results:
Kyphosis increased up to 12 months after implant removal. The loss of bisegmental correction was 6.0 ± 4.2 (range 0° to 16°) 12 months after implant removal. Risk factors for loss of reduction are younger patient age, fractures of the thoracolumbar junction (Th12), and degree of traumatic kyphosis. Intervertebral discs traversed by the stabilization lose height and don’t recover within 1 year after implant removal. Without implant removal, disc height of the lower adjacent level is reduced after 24 months.
Conclusions:
Short posterior stabilization in combination with vertebroplasty is a treatment alternative for thoracic and lumbar AO A3 fractures. After implant removal kyphosis increases, predominantly in the segment above the augmented vertebra. Risk factors for loss of reduction include younger age, fractures of the thoracolumbar junction (T12), and higher fracture kyphosis.
Introduction
The treatment of thoracolumbar burst fractures (AO/Magerl type A3) is generally based on national and international guidelines. Some of the factors that contribute to the absence of standardized treatment strategies include lack of evidence regarding benefits of one treatment over the other, financial and medical accessibility of resources, medicolegal considerations, traditions of surgeons and departments, different interpretation of biomechanical data and morphological aspects, and patient expectations. 1 –5 Even though posterior stabilization may be an option in the treatment of these fractures, 1 insufficient anterior column support would mandate additional adequate internal fixation and anterior stabilization with cages or iliac bone grafts. 6 These operations are commonly planned as a 2-stage procedure, resulting in prolonged hospital stay, with a subsequent risk increase of surgical complications.
Recent reports have shown that a combination of short-segment pedicle instrumentation with anterior transpedicular augmentation of the fractured vertebral body may provide a reasonable alternative to anterior corpectomy in both osteoporotic and younger patients. 7 –12 Posterior instrumentation can be performed through an open 8,11 or percutaneous 9 approach; vertebral augmentation could further be achieved with either vertebroplasty 7,8,11,13 or kyphoplasty. 10,14,15 Compared to anterior stabilization, the above-mentioned procedure did prove beneficial in reducing operation time, hospitalization days, and complications. The short-term (<1 year) radiological and clinical results were shown to be comparable to anterior stabilization. 14
It is agreed that posterior stabilization of burst fractures alone, without sufficient support of the anterior column, leads to loss of reduction after implant removal. 16 –18 However, it is unknown whether this loss of reduction occurs in the cranial or caudal fracture-adjacent disc, or whether the fractured vertebral body itself loses its height after implant removal, which is likely to explain associated instability. Therefore, the study was designed to measure the potential loss of fracture reduction and the behavior of the adjacent intervertebral discs after implant removal in patients treated with short posterior instrumentation and anterior vertebral augmentation.
Materials and Methods
Patient Sample
Between 2000 and 2013, 59 patients with monosegmental A3 fractures according to the AO/Magerl classification 19 of the thoracolumbar junction between T10 and L3 were treated using open short posterior stabilization in combination with vertebroplasty. Only patients who also received decompression of the injured level were included in the study.
Inclusion criteria for the analysis were a complete radiological assessment including preoperative spine computed tomography (CT), conventional biplanar X-rays of the thoracolumbar spine before implant removal, 2 months after implant removal, and at 12 months follow-up (“implant-removal group”).
The inclusion criteria were met in 29 patients (male/female 17/12; age: 41.7 ± 15.4 years). Fractures were classified as A3.2.1 in 25 patients and A3.1 in 4 patients. The fractures were located at the level of Th12 in 9, L1 in 14, and L2 and L3 in 3 patients each.
Patients who underwent the same primary procedure but without implant removal comprised the control group (“no-implant-removal group”), which included 30 patients (male/female 20/10; age: 43.2 ± 13.2 years), of which 25 patients had A3.2.1 and 5 patients A3.1 fractures initially. The fractures were located at Th12 level in 13 patients, L1 in 11 patients, L2 and in L3 in 3 patients each. Follow-up was performed at 12 and 24 months postoperatively.
Surgical Technique
All 59 patients were treated with an open posterior bisegmental bridging short posterior stabilization in combination with a cross-link (USS II, Synthes, Bettlach, Switzerland).
Influenced by fracture morphology (n = 55) and the presence of neurological symptoms (n = 1, cauda equina syndrome; n = 3, radiculopathy), stabilization was accompanied by decompression in all patients. To achieve fusion for the cranial fracture-adjacent segment, monosegmental posterolateral bone grafting with autologous bone from the laminectomy was performed. After reduction of the fracture, standard bipedicular vertebroplasty using polymethylmethacrylate (PMMA) under constant biplanar radiological control was performed. No clinically relevant complications associated with the PMMA augmentation occurred. In 3 patients, minor leakage into the disc space was seen intraoperatively at the end of the procedure. Radiological signs of venous leakage were seen in 2 patients; leakage into the spinal canal did not occur.
Implant Removal
All patients were offered the option of having the implant removed after the ninth postoperative month to free the nonfused segment. The indication for implant removal was therefore subsequently based on the individual wish of the patients. During implant removal the posterior fusion was confirmed visually. No implants were removed due to infection, failure, adjacent segment degeneration, or re-instrumentation.
The mean time of implant removal was 9.8 ± 4.5 months after the initial procedure.
Radiographic Assessment
A preoperative spinal (trauma) CT as well as postoperative lateral X-ray projections in a standing position were available for all patients. All patients received the same treatment regime during the first year, after which the 2 groups were formed based on either removal or nonremoval of the implant. At this time point, all patients received standing anteroposterior and lateral radiographs (t0).
Patients with implant removal received further radiographic follow-ups 2 months (t2) and 12 months (t12) after implant removal.
Patients without implant removal were also followed up for the same time interval, with t12 corresponding to 24 months after the initial procedure.
To determine the loss of reduction, the monosegmental cranial and caudal (adjacent to the fractured vertebra) as well as the bisegmental Cobb angle were measured. To assess the degree of disc degeneration and disc height change, the disc height was measured according to Frobin et al 20 at the 2 levels within rigid stabilization (adjacent to the fractured vertebra) as well as at the cranial and caudal levels (adjacent to the instrumented vertebrae). Furthermore, the anterior and posterior vertebral body heights (“sagittal index”) were measured during every follow-up (Figure 1). Possible implant failure or screw loosening were assessed with plain radiographs 21 as well as visually during implant removal.
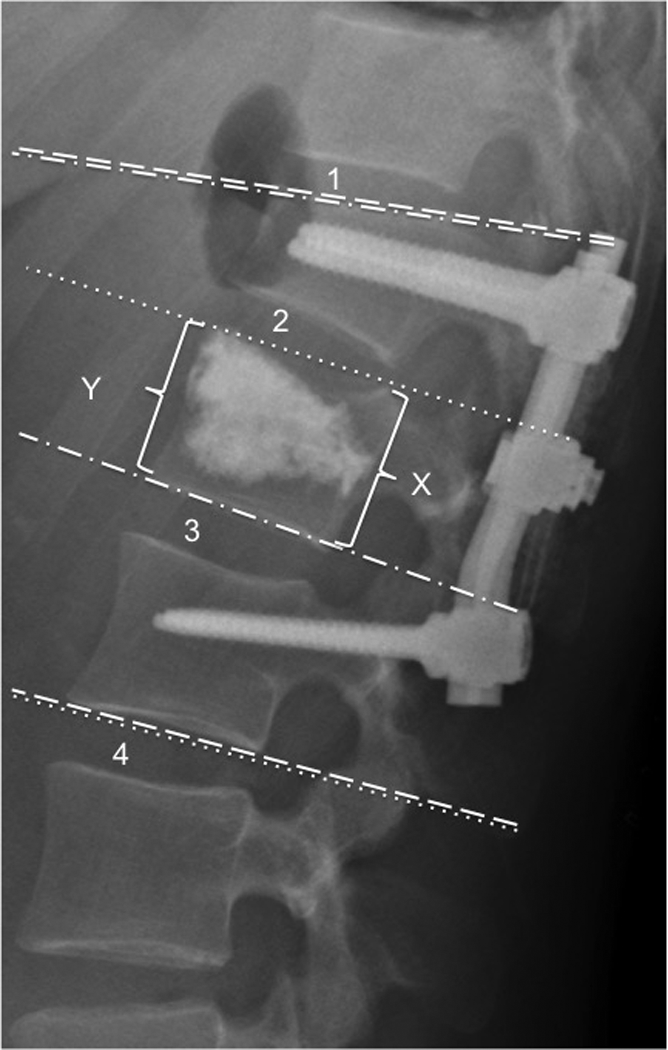
Bisegmental (—), cranial monosegmental (–•–), and caudal monosegmental (•••) Cobb angles. Disc height was measured according to Frobin at the 2 levels within rigid stabilization (3, 4) as well as at the cranial (1) and caudal (4) adjacent levels. Anterior (Y) and posterior (X) vertebral body height was measured at all follow-up intervals.
All measurements were done using digital DICOM images (PACS Sectra Workstation IDS7). The local ethic committee approved the study.
Statistical Analyses
For the comparison of outcome measures at different follow-up intervals, the Wilcoxon signed-rank test was used. To assess the influence of patient factors (age, gender, fracture location) on the postoperative change in Cobb angles, a generalized linear regression model was performed. Mann-Whitney U test was used for group comparisons. Values were reported as mean ± standard deviation. A P value <.05 was considered statistically significant. All statistical analyses were conducted using SAS 9.4 (SAS Institute, Inc, Cary, NC).
Results
Implant-Removal Group
The mean follow-up time after implant removal was 12.8 months (range: 11-14 months). There were no cases of perioperative complications or reoperations after the initial surgery or after the implant removal. At final follow-up all implants were intact and no screw loosening was seen. During implant removal, the fusion site was judged “fused” in all 29 patients.
Cobb Angle
The traumatic upper monosegmental Cobb angle (before stabilization) was 16.5 ± 4.3°. Bisegmental Cobb angle was 12.5 ± 6.2°, and lower monosegmental Cobb angle was 9.2 ± 6.2°.
Bisegmental Cobb angle increased on average from 6.8 ± 7.2° at t0 to 12.5 ± 9.0° at t2 and 14.1 ± 10.2° at t12. Similarly, upper monosegmental Cobb angle changed on average from 7.2 ± 5.3° at t0 to 11.6 ± 7.3° at t2 and 13.6 ± 8.0° at t12. The change of the lower monosegmental Cobb angle were not significant between 5.2 ± 5.4° at t0 to 6.2 ± 5.2° at t2 and 6.4 ± 5.9° at t12.
Loss of reduction (Cobb-angle change) of the bisegmental Cobb angle was measured in 86% (n = 25) of the patients at the 12-month follow-up visit where the loss of correction was mostly seen immediately after the implant removal; only 1 patient (3%) presented a delayed loss of reduction during follow-up (between 2 and 12 months after implant removal). A typical case is shown in Figure 2.

Typical case of a 29-year-old female with A3.2.1 fracture of L1 due to a horse riding accident, no neurological symptoms. (A) Primary CT scan shows a burst-split fracture of L1 and a previous known (old) compression fracture of T12. (B) Anteroposterior and lateral standing radiograph postoperative after open bridging stabilization T12-L2, monosegmental fusion of the upper segment T12/L1, and vertebroplasty L1 with PMMA. (C) Six months after initial operation, stable. (D) Two months after implant removal: loss of lordosis mostly in the cranial (–•–) but not in the caudal (•••) monosegmental motions segment. (E) Twelve months after implant removal: slight increase of kyphosis compared to 2 month postoperative 1.5° (overall of 8° loss of reduction after implant removal). The sagittal index of T12 stays stable over time.
The loss of correction mainly occurs in the cranial motion segment. Bisegmental and cranial monosegmental Cobb angles were significantly different between t0 and t2 (but not between t2 and t12), while no significant changes of the caudal Cobb angle could be observed over time. The mean changes in Cobb angles are illustrated in the Table 1.
Changes in Cobb Angles Between Different Follow-Up Intervals.
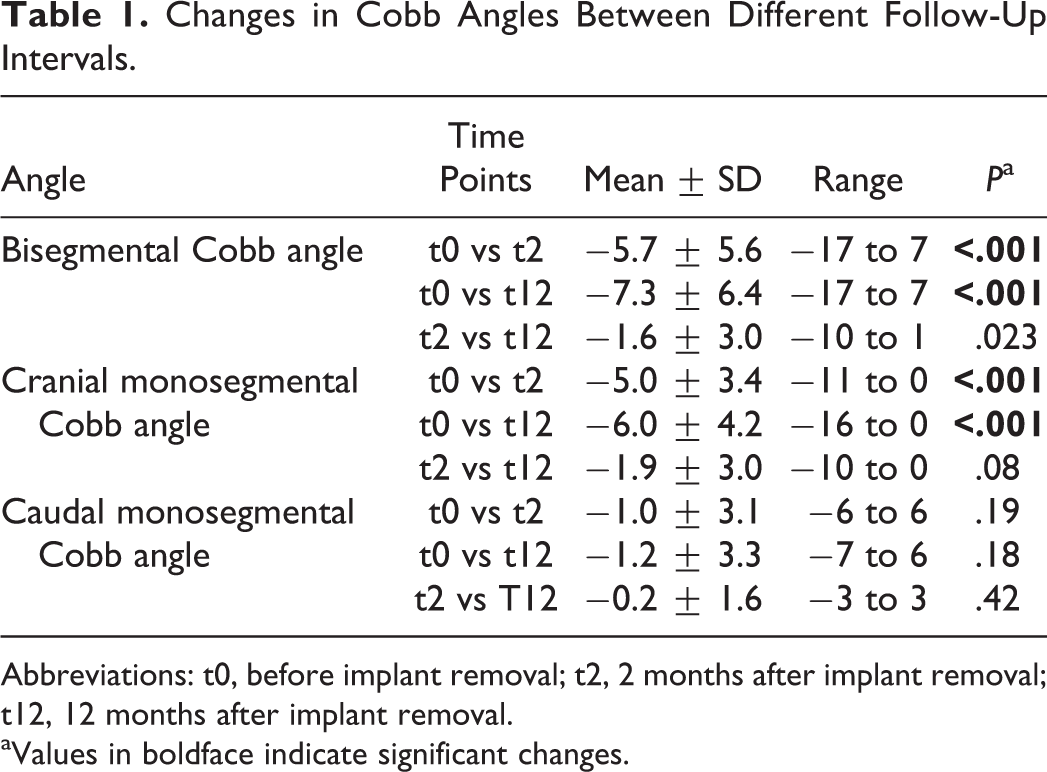
Abbreviations: t0, before implant removal; t2, 2 months after implant removal; t12, 12 months after implant removal.
aValues in boldface indicate significant changes.
Influence of Patient Characteristics on Secondary Cobb-Angle Changes
The univariate analysis showed that patient age influences the change of the cranial monosegmental as well as the bisegmental Cobb angle. In younger patients a higher loss of reduction was seen compared to older patients (Table 2 and Figure 3).
Influence of Patient Characteristics on Secondary Cobb Angle Changesa.
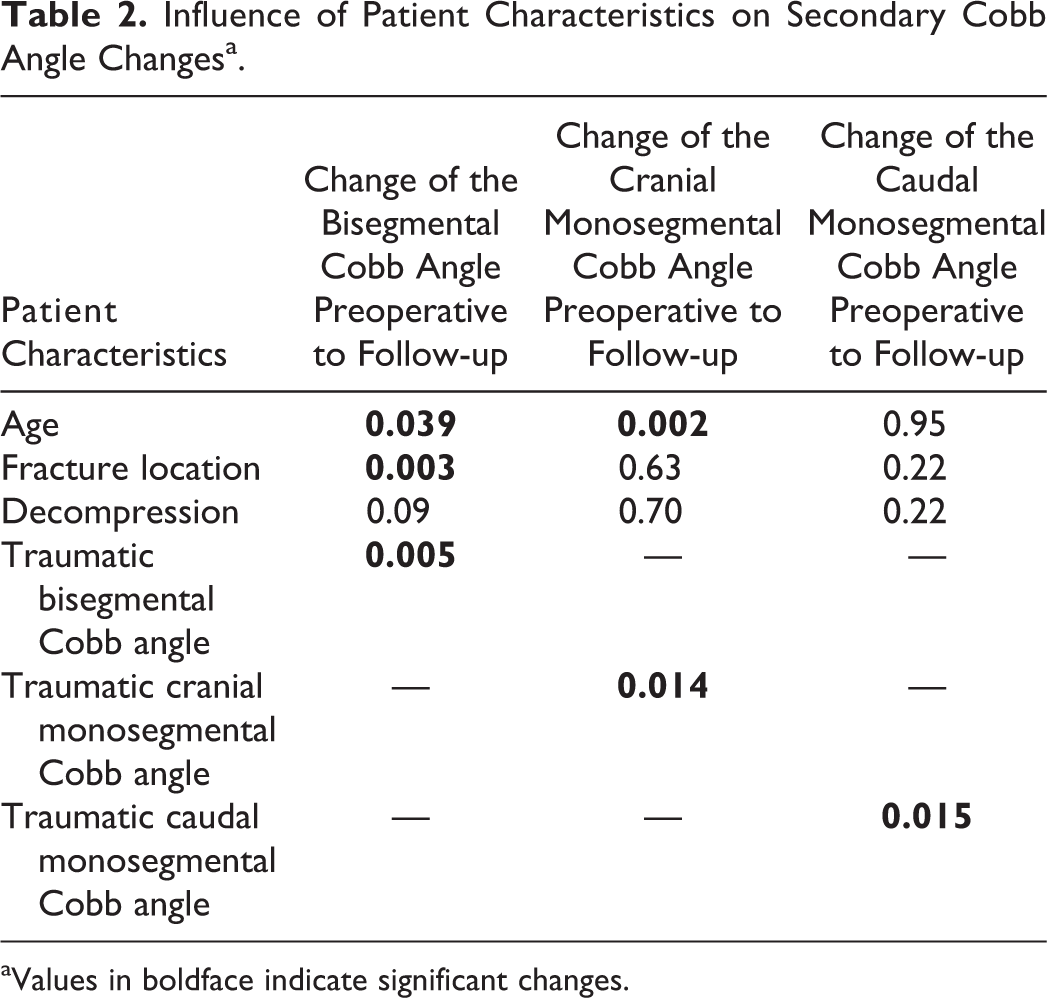
aValues in boldface indicate significant changes.
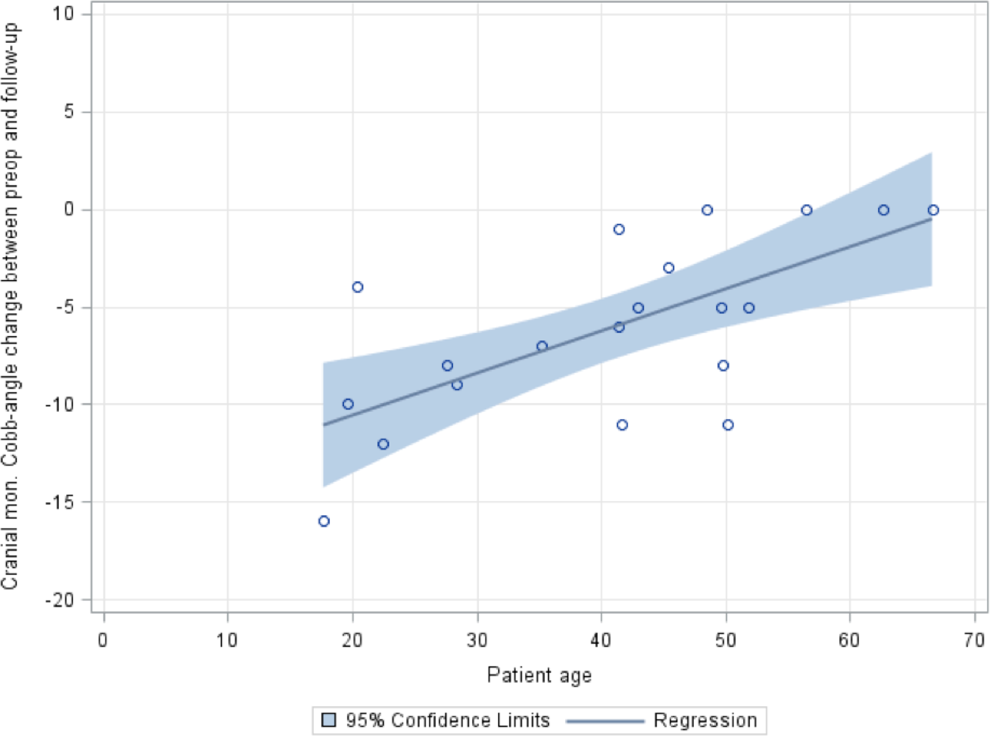
The change of the cranial monosegmental Cobb angle between t0 and t12 versus patient age.
Furthermore, fracture location also showed to influence the change of the bisegmental Cobb angle (Table 2). The loss of reduction is more pronounced if the fracture is closer to the thoracolumbar junction. Fractures of Th12 showed the highest and fractures of L3 the lowest loss of reduction (Th12: −12.4 ± 2.9°; L1: −9.5 ± 4.0°; L2: 0.1 ± 0.1°; L3: 1.1 ± 0.6°).
Moreover, the loss of reduction after implant removal correlated with the degree of traumatic kyphosis before stabilization for each Cobb angle. The higher the traumatic kyphosis, the higher is the loss of reduction after implant removal (Table 2).
Disc Height
The height of both discs within the regions of rigid stabilization decreased after implant removal without recovering between t2 and t12 (Figure 4).
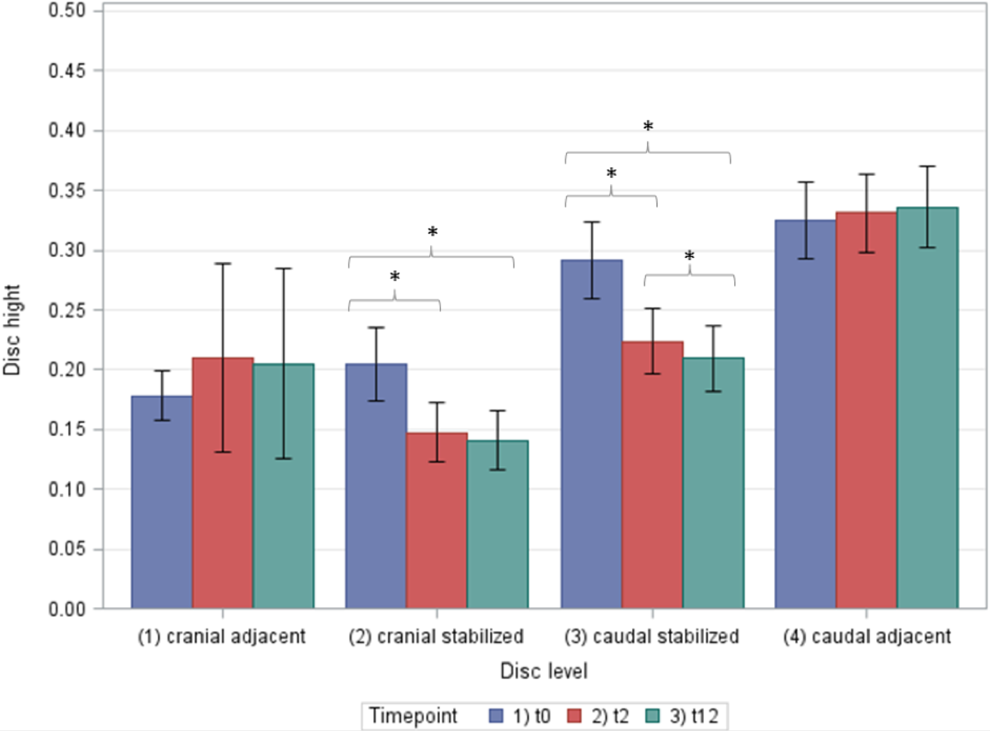
Change in disc height between different follow-up intervals at the levels 1-4. t0, before implant removal; t2, 2 months after implant removal; t12, 12 months after implant removal; *, significant changes.
The cranial and the caudal adjacent discs showed a tendency to increase in their disc height between t0 and t2, which was however not statistically significant (Figure 4).
Vertebral Body Height
The sagittal index of the fractured vertebral body remained unchanged during the observation period.
No-Implant-Removal Group
This represented the control group. Radiographic evaluations were preformed at a mean of 12.3 (range: 11-13 months; t0) and 21.8 (range: 19-26 months; t12) months after stabilizing surgery.
Upper, lower, and segmental Cobb angles remained nearly unchanged up to 24 months postoperatively. From t0 to t12, the mean bisegmental Cobb angle changed from 6.4 ± 6.9° to 7.4 ± 3.9°, the upper monosegmental Cobb angle changed from 7.0 ± 4.8° to 9.1 ± 4.7°, and the lower monosegmental Cobb angle changed from 5.5 ± 4.1° to 6.9 ± 5.2°.
Prior to implant removal, disc height of all measured segments were not significantly different between the 2 groups. Compared to the “implant-removal group,” patients without implant removal showed significantly higher heights of the intervertebral discs cranial and caudal to the fractured vertebra at final follow-up. This shows that after implant removal, included intervertebral discs lose height, as there was no significant difference before removal of the implants. Compared to the implant removal group and compared to the initial height, the disc height of the caudal adjacent segment (below the fusion) was significantly smaller at final follow-up. The disc height of the cranial adjacent segment was not significantly different at follow-up (Table 3).
Comparison of Disc Height at Disc Levels and Their Changes Between Patients With and Without Implant Removal.a
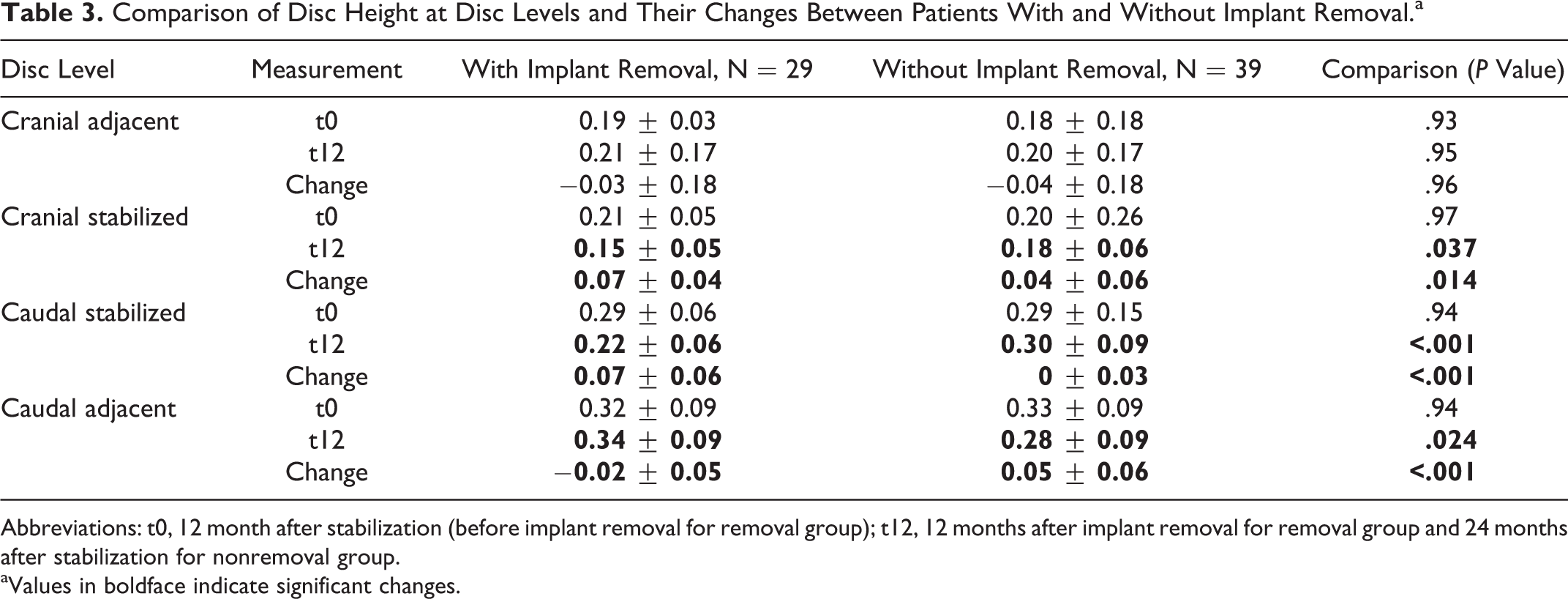
Abbreviations: t0, 12 month after stabilization (before implant removal for removal group); t12, 12 months after implant removal for removal group and 24 months after stabilization for nonremoval group.
aValues in boldface indicate significant changes.
Discussion
Restoration and preservation of sagittal plane alignment presents the primary goal in the treatment of anterior unstable lower thoracic and lumbar type A fractures. The main drawbacks of stabilizing procedures include accelerated adjacent disc degeneration, 22 disc collapse of the injured disc space above the fracture, 23 functional problems, and possibly pain. 24 In spinal surgery implant removal is performed for a number of indications; in short posterior stabilization for fracture treatment implant removal can be performed to unblock the nonfused motion segments, usually 9 months to 1 year after surgery. The results of this study prove loss of reduction after implant removal with a 5° to 7° average bisegmental loss of reduction within the first year, questioning the adequate anterior column support of this treatment option.
In 86% of patients, loss of reduction was visible. The loss of reduction occurs in the motion segment above the fracture, but not in the motion segment below it. This is explained by the fact that in most incomplete and complete burst fractures, the superior endplates and disc are more severely injured resulting in posttraumatic disc degeneration and height loss when loaded after implant removal. In a systematic review, Verlaan et al 25 reported an average correction loss of 7.6° at follow-up after short posterior stabilization alone without implant removal. The authors performed a subgroup analysis of short posterior stabilization with and without additional transpedicular spongioplasty demonstrating that, patients with a spongioplasty show higher loss of correction at follow-up (9.6°) compared to other patients (7.4°). Further studies, combining PMMA vertebroplasty and short-term stabilization, 14,26 reported an average loss of reduction around 3.0° without implant removal 1 year after surgery. The results of our control group show similar findings, emphasizing that loss of disc height is inconsiderable without implant removal. Nevertheless, without implant removal, the disc below the fusion loses significant height within the first 2 years following stabilization. Radiological signs of adjacent disc degeneration may be prevented by an early implant removal, but this question cannot be answered with this study.
While the study by Rahamimov et al did not find any correlation between age and loss of reduction, 14 according to our data younger patients seem to be less suitable for this treatment as they show a significantly higher loss of reduction after implant removal than older patients. In younger patients, an anterior column support by cage/bone graft may potentially provide for improved results. 27
Moreover, severe initial traumatic kyphosis predicts a negative impact on loss of reduction after implant removal. In such patients a higher loss of reduction after implant removal has to be expected. The same is true for fractures near to the thoracolumbar junction. An explanation for the latter effect may be the extinct biomechanics in the transition zone of rigid thoracic to the less rigid lumbar spine. It might be speculated that these patients may benefit from an additional anterior procedure instead of posterior transpedicular cement augmentation, but the evidence on this is lacking.
An influence of an additional decompression and, therewith, a potential weakening of the posterior structures could not be shown.
Several studies have highlighted the importance of a sufficient reconstruction of the anterior loadbearing column in an attempt to prevent a secondary loss of correction. 27,28 The caudal disc, below the injured level, which was only temporarily stabilized, also to a lesser extent, lost disc height and did not recover to last follow-up. Müller et al found similar results in their study. 6 The extent to which the height loss of the caudal stabilized disc is due to sequelae of an extensive traumatic damage must be confirmed experimentally. Another possible explanation is that the rigid stabilization and, thus, shielding of physiological intervertebral disc loading during temporary fixation may lead to a reduced cyclic fluid flow into the disc, which possibly affects a loss of disc nutrition and supply causing early disc degeneration particularly in younger patients. 29,30 In addition, a certain overdistraction of the segments while performing the instrumented reduction of the fracture has to be assumed and would explain a loss of disc height without degeneration. As we have no information on disc height prior to the fracture it is not possible to confirm this hypothesis.
Verlaan et al 31 described the degenerative changes of the disc adjacent to a fractured vertebra undergoing a similar treatment strategy with implant removal in a smaller and more heterogeneous patient cohort. In general, our results are in line with the Verlaan’s study, but we focused more on sagittal alignment and loss of reduction. We could show that secondary loss of reduction after implant removal occurs within the disc space, usually cranial to the fracture, most probably due to the posttraumatic disc degeneration as Verlaan et al have shown. As a consequence of both our findings, we conclude that in cases of expected disc injury and especially in younger patients, a 360° monosegmental fusion is better indicated to prevent secondary loss of reduction resulting from collapse of the disc space. In elderly patients with degenerated discs and reduced disc space, further degeneration and disc collapse is limited, due to which our proposed treatment strategy is adequate and safe.
There are some limitations to this study. The sample size is small and there was no comparison to a group undergoing additional anterior stabilization. This will need to be addressed in future studies. Furthermore, it would be interesting to know if the motion of the “affected” disc is comparable to that of the normal population after implant removal—functional flexion and extension bending X-rays would be required to address this question. Moreover, a CT scan before implant removal would be beneficial for confirmation of posterolateral fusion. One other limitation of our study is the lack of clinical short-term and long-term data. Minor radiological changes could be of less importance. On the other hand, an aggressive (anterior and/or long posterior) reconstruction may result in better initial radiological outcome but higher complication rates in the short and long terms. This should provide a base for further investigations.
Conclusion
Transpedicular vertebroplasty in combination with posterior transpedicular stabilization provides sufficient stability in thoracolumbar type A fractures for up to 24 months with an increased risk of adjacent segment disease with early implant removal. After implant removal some increase of the overall kyphosis, which takes place in the segment above the augmented vertebra, must be expected. In younger patients, in fractures near to the thoracolumbar junction and in patients with a high fracture kyphosis, a greater loss of reduction may be expected; therefore, for these select groups, the recommendation of additional anterior fusion without implant removal can be made.
Footnotes
Authors’ Note
This study was approved by the local ethics committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.