
Abstract
Study Design:
A literature review.
Objective:
To summarize the implant removal rate, common bacterial organisms found, time of onset, ratio of superficial to deep infection, and regurgitating the prevalence among all the retrospective and prospective studies on management and characterization of surgical site infections (SSIs).
Methods:
PubMed was searched for articles published between 2000 and 2018 on the management or characterization of SSIs after spinal surgery. Only prospective and retrospective studies were included.
Results:
A total of 49 articles were found relevant to the objective. These studies highlighted the importance of implant removal to avoid recurrence of SSI. The common organisms detected were methicillin-resistant Staphylococcus aureus, methicillin-resistant Staphylococcus epidermis, Staphylococcus epidermis, Staphylococcus aureus, and Propionibacterium acnes, with prevalence of 1% to 15%. A major proportion of all were deep SSI, with minority reporting on late-onset SSI.
Conclusion:
Long-term antibiotics administration, and continuous irrigation and debridement were common suggestion among the authors; however, the key measure undertaken or implied by most authors to avoid risk of recurrence was removal or replacement of implants for late-onset SSI.
Keywords
Introduction
Surgical site infections (SSIs) are extremely burdensome to the patients, a leading cause of morbidity, and a major cause of readmission with longer lengths of stay after spinal surgery. 1 Although meticulous prophylactic surgical practice is crucial to avoid such incidences, there is always some incidence of infection in or around the area that has been instrumented in surgery. 1,2 Many authors have summarized the key prevention and postsurgical management techniques for SSI in spine surgery; however, because of the varied nature of surgical practices and the numerous factors involved, the focus has been on overall preventative and management measures. 2 -4 In addition, SSIs in medical care are deemed as “never events” and their occurrence is considered to be influenced by the hospital policies and procedures. Such an outlook toward infection leads many practitioners and hospital system to bundle as many potential measures and/or increase the intensity (dosage in some cases) of individual measures, some to the point of redundancy. 5,6 The result of such practices is no less than controversial as can be exemplified simply by the previously cited ranges in prevalence of SSI. 7 Therefore, it is very useful to consistently evaluate the results of all recently published clinical practice, in an attempt to corroborate or nullify isolated variables into being effective or not. Few such variables during management of SSI are implant removal rate, common bacterial organisms found, time of onset, ratio of superficial to deep infection, and so on. Thus, the objective of this literature review is to summarize the findings on implant removal rate, common bacterial organisms found, time of onset, ratio of superficial to deep infection, and regurgitating the prevalence among all the retrospective and prospective studies on management and/or characterization of SSI.
Methods
The general method utilized for the literature review was adopted from Cochrane collaboration. Table 1 shows the search strategy that was developed for the PubMed database, for the period 2000-2018. Title and abstracts were reviewed to shortlist articles for full length review. The shortlisting was followed by full-text review of all references that appeared to retrospectively or prospectively address the key SSI management techniques at an event of surgical site infection.
Medline Search Strategy Using PubMed.
Results
A total of 79 full-text articles were retrieved after screening through titles and abstracts. Of these, only 49 articles were found relevant, and were used for the synthesis below. 8 –56 Below is the summary of their findings. Relevancy was determined purely based on if the articles answered any one of the following: (1) implant removal rate, (2) common bacterial organisms found following infection, (3) time of onset, and (4) ratio of superficial to deep infection. Furthermore, only prospective or retrospective studies were included.
Implant Removal/Retention Rate
In a study by Maruo et al, 16 154 of 197 (78%) of SSIs were eradicated within 90 days, of which 76% were also able to retain the implants. Forty-three of 197 (22%), which were not managed within 90 days, were considered failure in management of SSI. 16 However, 93% of these 78% aforementioned were superficial infections. 16 A few studies had close to 0% to 10% implant removal. 17 -20 Yin et al 21,22 in their 2010-2014 series were able to retain implant in 40 of 41 cases of late onset SSI. In contrast, many other studies required implant removal on all or majority of cases, for example, 13 of 13, 26 of 26, 20 of 20, 10 of 10 (100%), and so on. 23 -27 Di Silvestre et al, 28 in a long-interval SSI detection period (3 years), found the need for 100% removal of implants in all 15 SSI cases among the 540 cases operated upon. Nevertheless, other authors such as Kanayama et al, 29 even at short-interval SSI detection period, observed 8 of 8 (100%) in need of hardware removal. Another study looking at a specific bacterial species reported 31 of 68 (46%) had need for complete removal of implant, and additional 13 of 68 (19%) has partial implant removal. 30 Among few studies with significant yet not majority implant removal proportion, one identified 61 of 84 cases (73%) had implant retention with deep SSI, and 48 of 48 (100%) with superficial SSI. 31 Similarly, other cohorts showed at least 21 of 83 (25%), 26 of 44 (58%), 22 of 42 (52%) needing implant removal. 32 -34
Bacterial Genus/Species
The common type of bacterial infection was methicillin-resistant Staphylococcus aureus (MRSA): 10 of 14 (71%), 11 of 18 (61%), 7 of 20 (35%), 5 of 10 (50%); methicillin-resistant Staphylococcus epidermidis (MRSE): 9 of 21 (43%); coagulase-negative staphylococci (possibly Staphylococcus epidermidis): 12 of 27 (45%), 3 of 9 (33%); Staphylococcus aureus: 31 of 51 (61%), 7 of 17 (41%), 6 of 20 (30%), 3 of 10 (30%); polymicrobial: 7 of 17 (41%); methicillin-resistant coagulase-negative staphylococci (MRCNS): 1 of 10 (10%); Aspergillus fumigatus (a. fumigatus): 1 of 10 (10%); gram negative, anaerobic such as Propionibacterium acnes, antibiotic-resistant strains: 5 of 9 (83%). 17,18,20,23-24,29,35 -38
SSI Onset Time
Studies that specified the onset interval of SSI, early onset (<30 days) constituted 162 of 225 (72%), 7 of 14 (50%), 13 of 20 (65%), 33 of 41 (80.5% skewed proportion; because authors didn't report late onset SSI), 42 of 51 (82% skewed). 16,19,24,37,39 Delayed onset (30 days to 1 year) constituted 57 of 225 (25%), 5 of 14 (35%), 3 of 20 (15%), 8 of 41 (19.5% skewed), and 9 of 51 (17.6 skewed), whereas late onset (>1 year) constituted 6 of 225 (3%), 2 of 14 (15%), and 4 of 20 (20%). 16,19,24,37,39
Deep Versus Superficial SSI
Another variable that existed was identification of deep versus superficial infection. Some recorded the distribution, whereas others focused on deep SSI (via exclusion of superficial SSI). Deep SSI constituted 2 of 4 (50%), 11 of 22 (50%), 22 of 29 (76%), 10 of 17 (58%), 29 of 54 (53%), 64 of 78 (82%), 53 of 104 (51%), 1409 of 2344 (60%), 12 of 27 (45%), 7 of 9 (77%), 2 of 2 (100%), 84 of 132 (64%), 69 of 79 (87%) among various studies, whereas superficial SSI constituted 2 of 4 (50%), 11 of 22 (50%), 7 of 29 (24%), 7 of 17 (42%), 24 of 54 (47%), 13 of 78 (16.7%), 41 of 104 (39%), 867 of 2344 (37%), 15 of 27 (55%), 2 of 9 (23%), 48 of 132 (36%), 10 of 79 (13%). 25,26,29,31,36,40 -45
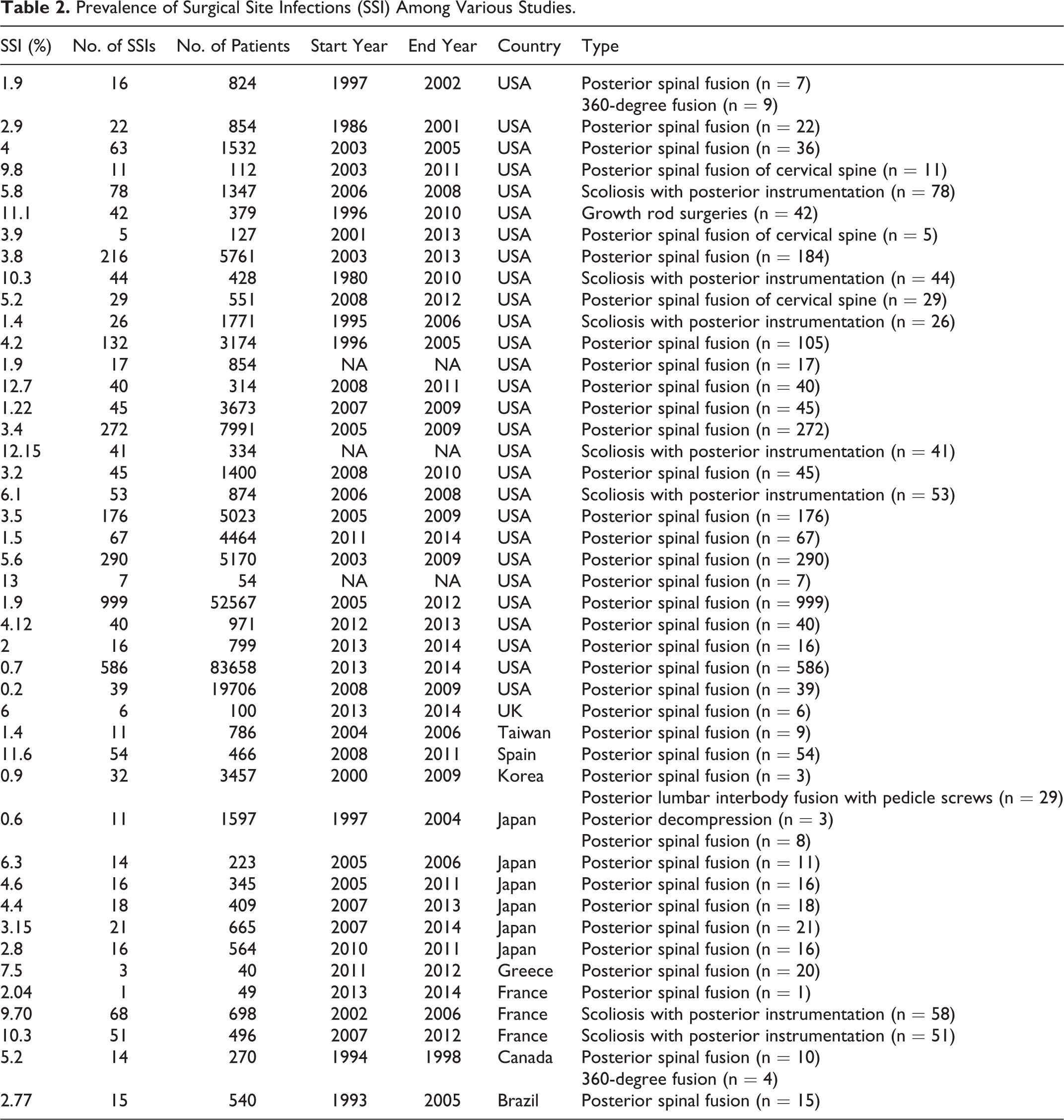
SSI Incidence Rate
The SSI incidence rate itself varied and is presented in Table 2.
Prevalence of Surgical Site Infections (SSI) Among Various Studies.
Discussion
In majority of the studies, patients who presented with SSI had to be readmitted for irrigation and debridement and implant removal/replacement. However, there were also fewer studies where revision surgery for SSI was not necessary in all the patients, for example, 9 of 14 (64%) with mean hospital stay of 43 days. 39 Key steps for management included irrigation and debridement, vacuum-assisted wound closure (VAC) in 25% and more cases, and variable term antibiotics administration (both intravenous and oral). 17 -20,24,28,31,36,39,44,46 -53
Many authors concluded that eradication of deep SSIs was not possible without complete removal of spinal implants. In addition, repeated site debridement could not eradicate SSI either while the implants (pedicular and/or interbody constructs) were retained, and therefore removal in most or all patients was later necessary. 23,27 Furthermore, one of this study also disclosed that the average number of surgeries required for infection treatment to be 4 (range 1-16), leading up to an average cost of SSI treatment range from quarter of a million to just shy of a million dollars per patient. 27 A smaller proportion of such recovering patients still presented with residual back pain and reduced activity. 23 To reconcile differences in practices (complete versus partial removal of implants), recently Khanna et al 54 presented a thorough retrospective analysis on implant retention and its association with antibiotic administration and onset interval. They associated delayed onset or late onset SSI patient with higher risk of SSI recurrence in absence of hardware removal. Most of their cases with early or delayed SSI were able to retain implants with early aggressive debridement. 54 When comparing the type of SSI (deep vs superficial, and late vs delayed vs early onset SSI) among these studies, eradicating deep SSI with delayed and late onset infections were most difficult, with majority needing repeated debridement and drainage. 16,29 A common problem was that of late onset SSI with low virulent p. acnes. Being low virulent bacteria, it remained undetected in the early intervals leading to widespread biofilm formation on the implants, later leading to a resilient onset of SSI. 30 For instance, because of repeated detection of P acnes, 8 of 68 (11.7%) patients underwent multiple revision surgeries in one series. 31 An exception to this trend was the study by Yin et al, 21 where they retained implants in most cases with late-onset SSI (S aureus was the common organism). It should be noted that they also noticed negative culture results in seven patients with late onset SSI (hence the underlying risk of undetected growth of organism) and one with hardware loosening due to recurrence of infection. 21
Most common organism detected were MRSA, MRSE, S epidermis, S aureus, and P acnes; nonetheless there were also others like polymicrobial and gram negative cited in the studies. 17,18,20,23,24,29,35 -38 Authors noted that gram negative infection was common in early infections, whereas later ones presented with S aureus, P acnes, and so on. 39 In many studies, the interval of infection onset was limited to early, that is, <30 days, <90 days, between 30 and 90 days, or <6 months for detection of SSI, or was not mentioned. 24,27,55,56 In few, the authors specifically looked at late onset infection with average occurrence about 70 months with 15 of 540 index cases (2.77%). 28 Longer term studies, extending over 6 years also concluded 56 to 80 months as average SSI detection length with total incidence of 68 P acnes cases of 698 index cases (9.7%). 30 There were higher proportion of deep SSI over superficial SSI in most studies. Higher incidence of failure in management of SSI (recurrence) were seen with iliac fixation, polymicrobial infections, P acnes infections (of which many often were delayed or late onset), and >6-level fixation. 16
As shown in Table 2, the SSI incidence rate could be argued to be a result of varied spinal surgical practices and reporting methods, including differences in prophylactic measures, quality of hospital facilities, duration of follow-up, and the country of practice at the minimum. 7,57 -61
Besides physical examination, common diagnostic tools used to detect infection are imaging (computed tomography and magnetic resonance imaging), blood culture, C-reactive protein, erythrocyte sedimentation rate, white blood cell count, and other inflammatory biomarkers. Many of these methods provide high positive predictive value but relatively lower negative predictive value. Lower negative predictive value implies that there still exist possibilities of hidden contamination, which presents itself as full-blown infection at a later interval, as delayed or late onset SSI. Furthermore, unlike superficial infection (localized to the skin and subcutaneous tissue), most deep infections lack superficial presentations making their diagnosis solely presumptive. Thus, a more cautious pathway in management of late-onset SSI may be complete removal or replacement of implants in such cases. Some authors of these studies concluded that attempts made to retain implants only lead to multiple reoperations, higher costs, and patient burden. 27 Recent studies on identification of occult infection led hardware loosening, and propensity of bacterial infestation and growth on implant surfaces outside and inside the theatre provides further evidences of levels of higher uncertainty (of subsequent infection) involved in the management of SSI and its preventive measures. 62 -68
Conclusion
Based on the data presented in myriads of prospective and retrospective studies, it is perhaps prudent to replace or remove the existing implants for management of late onset deep SSI. Additionally, although a wide range of SSI incidence rates have been observed, there exists uniformity in the type of bacterial organisms being reported.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. AA reports royalties from Paradigm Spine, Joimax, consultancy from Spinal Balance, editorial board membership from Clinical Spine Surgery and Spine, outside the submitted work. AKA and VKG reports royalties from Paradigm Spine, Joimax, investment/options from Osteonovus and Spinal Balance, outside the submitted work. SG reports consultancy for Spinal Balance and Si Bone, resident and fellow education committee, CME committee, website and digital platform committee, Chair for NASS, and international committee member for AAOS, outside the submitted work. Rest of the authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.