
Abstract
Study Design
Systematic review and Meta-analysis.
Objective
To compare radiological, functional and safety outcomes of implant removal vs implant retention following posterior fixation of thoracolumbar (TL) fractures.
Methods
Following PRISMA guidelines, we searched PubMed, Embase, Scopus, Web of Science, and Cochrane library from inception to October 2025. Randomised controlled trials (RCT) and comparative cohort studies comparing outcomes between planned implant removal and retention were considered. Primary outcome measures were Cobb angle correction, Oswestry Disability Index (ODI) and surgical site infection (SSI). Secondary outcomes included pain scores, kyphosis progression, reoperation rates, and patient reported outcome measures (PROM). Random effects models generated pooled mean differences (MD) and odds ratio (OR).
Results
Eight studies with 571 patients met the inclusion criteria. Radiological outcomes were comparable between the groups. Improvements in Cobb angle were similar for the 2 groups [MD: 5.04°, 95% CI: 0.03-10.05 (implant removal group) vs MD 6.38°, 95% CI: 1.89-10.87 (implant retention group); P = .70]. Kyphosis progression also did not differ between the groups (MD: 0.41°; P = .37). Functional outcomes improved significantly within both groups; however, pooled ODI analysis demonstrated no between-group difference (P = .81). SSI rates were low across all studies, with no significant difference between the 2 groups [Odds ratio (OR)-1.42; P = .30). Pain scores improved similarly in both the cohorts, and the reoperation rates were infrequent and comparable.
Conclusion
Implant removal after healed TL fractures provides no radiological or functional advantage over implant retention for most patients. Both strategies demonstrate meaningful improvements in pain, spinal alignment and disability, with low complication rates. Implant removal may benefit in select young and symptomatic individuals; however, routine removal may not be recommended. Individualized decision-making remains essential.
Level of Evidence
II.
Keywords
Introduction
Thoracolumbar (TL) fractures represent one of the most common spinal injuries encountered in trauma practice, and account for approximately 90% of all spinal fractures.1–5 These injuries predominantly affect the T11-L2 transitional zone, where the biomechanical stresses under routine physiological forces are the largest. 6 Pedicle screw fixation remains the most-widely employed surgical treatment for unstable TL fractures, allowing for immediate stability, restoration of sagittal alignment and early mobilization.3,7 Although advancements in surgical techniques, such as percutaneous fixation and short-segment instrumentation, have substantially enhanced the postoperative outcomes8,9; an important and yet unresolved question persists regarding the optimal postoperative management of implanted hardware once the bony union has been achieved.
Posterior instrumentation is frequently conceptualized as a temporary internal fixator (especially in percutaneous or non-fusion approaches), which may be removed after fracture consolidation so as to restore segmental motion, mitigate long term implant-related irritation, as well as reduce theoretical risks of adjacent segment degeneration (ASD), metal fretting, allergic reactions and stress-shielding induced osteopenia.1,3,5–26 The advocates of implant removal argue that hardware retention beyond the period necessary for fracture healing confers minimal biomechanical advantage while exposing the patients to potential long-term complications.5,10,21,24 Diverse retrospective studies and observational cohorts have suggested that implant removal may lead to enhanced function, range of motion (ROM) and mitigated pain, especially in the context of young, active individuals; and can potentially reduce screw loosening or implant failure rates.18,23,27 On the other hand, the disadvantages of routine implant removal include the need for a second surgery, surgical site infection (SSI), neurovascular complications, refractures, and loss of deformity correction (and potential spinal malalignment), especially in the absence of an anterior column support.28,29 While some studies have reported clinically insignificant or non-measurable improvements in PROMs following removal; others have demonstrated kyphosis progression or loss of disc integrity.2,12,25,30–32 In the elderly individuals, the physiological burden of reoperation and limited need for motion restoration further challenge the rationale for routine implant removal.5,18 Consequently, current clinical practice varies widely across diverse institutions and surgeons, with no available consensus or guidelines.
Existing literature is characterized by heterogeneity in study designs, fracture patterns, fixation strategies, fusion status, timing of implant exit and outcome measures.4,33 A majority of the studies are retrospective, with small sample sizes and variable follow-up, thereby limiting the generalizability of the conclusions.34–41 Until recently, high-quality evidence including RCTs on this subject was limited; and the balance between the benefits and risks of routine implant removal in the backdrop of spinal fracture fixation was fairly unexplored.18,19,23,42,43 Thus, a comprehensive synthesis of comparative studies evaluating implant removal vs retention was deemed necessary to clarify the impact on radiological alignment, functional recovery, pain outcome, and complication rates. This systematic review and meta-analysis were thus undertaken to evaluate the clinical and radiological outcomes following implant removal, in comparison with implant retention in patients treated surgically for TL fractures. By pooling contemporary evidence (including RCTs and comparative cohort studies), this review aims to provide clarity on whether implant removal confers any meaningful benefits, identify the patient subgroups who may benefit most; as well as develop evidence-based strategy for decision-making within spine trauma practice.
Methods
Study Design
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines 44 and adhered to Cochrane collaboration standards for comparative effectiveness research. 45 The review evaluated clinical and radiological outcomes of implant removal vs implant retention following surgical fixation of TL fractures.
Eligibility Criteria
We included RCTs and comparative cohort studies that assessed outcomes in patients who underwent spinal fixation for traumatic fractures of the TL spine.
Inclusion Criteria
Study Population
Patients undergoing posterior spinal instrumentation for traumatic TL fractures
Intervention
Elective or planned implant removal (
Comparator
Patients in whom the spinal implants were retained in-situ (
Outcomes
Primary outcomes were radiological correction (Cobb angle), functional improvement [Oswestry Disability Index (ODI)], safety outcome [surgical site infection (SSI)]. Secondary outcomes included pain scores [visual analog scale (VAS)], reoperation rates and additional patient-reported outcomes.
Exclusion Criteria
Case reports, narrative reviews, editorials, non-comparative studies, studies lacking extractable quantitative data and non-English full-text articles were excluded.
Search Strategy
A comprehensive search was performed across PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and Web of Science from inception to October 2025. Trial registries, including ClinicalTrials.gov and WHO ICTRP, were also searched using a combination of Boolean operators in key words such as “thoracolumbar fracture,” “implant removal,” “hardware retention,” “posterior fixation,” “kyphosis,” “ODI,” and “VAS.” Grey literature was explored through conference proceedings of major spine and orthopaedic societies. Reference lists of included studies and relevant systematic reviews were hand-searched to identify additional eligible reports. The search strategy combined controlled vocabulary and free-text terms for spinal instrumentation, implant removal, implant retention, and outcomes of interest. No restrictions were applied regarding year of publication; however, only full-text articles in English were considered.
Study Selection
All retrieved records were imported into Zotero for de-duplication and screened using Rayyan software. Two reviewers independently screened titles and abstracts, followed by a full-text review of potentially eligible articles. Disagreements were resolved by consensus or adjudication by a third reviewer. A PRISMA flow diagram was constructed to depict the number of records identified, screened, excluded, and included, along with reasons for exclusion (Figure 1). PRISMA flow diagram of inclusion of studies for analysis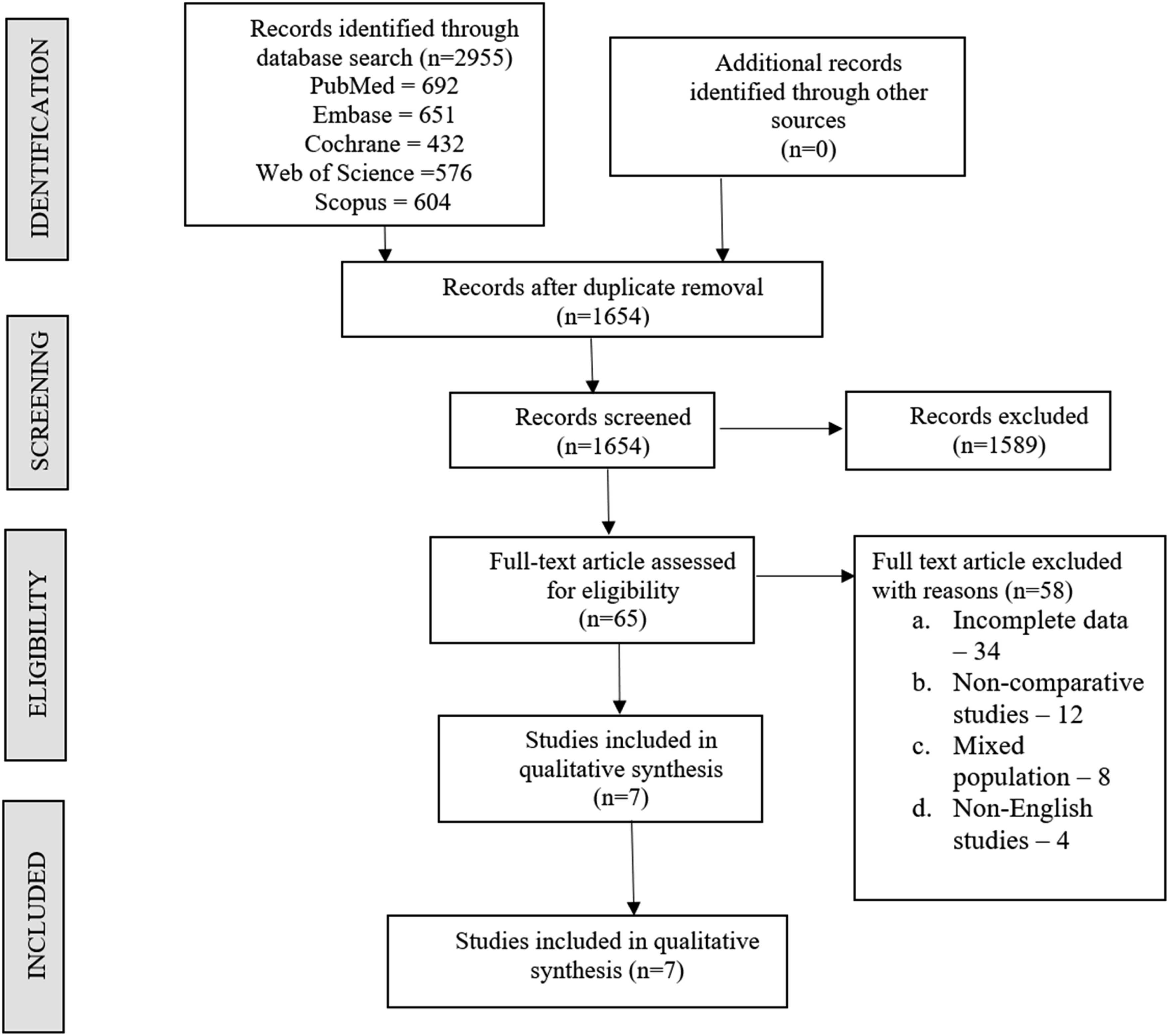
Data Extraction
Data extraction was performed independently by 2 reviewers using a standardised form. Extracted variables included study characteristics (author, year, country, design), participant demographics (sample size, mean age, sex distribution), intervention details (timing of implant removal, retention protocol), comparator details, and outcomes (Cobb angle, ODI, SSI, pain scores). Where outcomes were reported in heterogeneous formats (mean ± SD, mean + range, or descriptive statistics), harmonization was performed to ensure comparability. Missing standard deviations were estimated from ranges using established statistical methods.
Risk of Bias Assessment
Risk of bias was assessed independently by 2 reviewers. For randomised trials, the Cochrane Risk of Bias 2.0 tool was used, and for cohort studies, the Newcastle-Ottawa Scale (NOS) was applied. Disagreements were resolved by consensus.
Statistical Analysis
Continuous outcomes (Cobb angle, ODI, pain scores) were synthesised as mean differences (MD) with 95% confidence intervals (CI). Binary outcomes (SSI incidence) were synthesised as log odds ratios (OR) with 95% CI. Meta-analyses were conducted using random-effects models with restricted maximum likelihood (REML) estimation. Heterogeneity was quantified using I2 and H2 statistics along with the Galbraith plot, and explored through subgroup analyses comparing implant removal vs retention groups. Sensitivity analyses included leave-one-out meta-analysis and exclusion of studies at high risk of bias. Publication bias was assessed using funnel plots and Egger’s regression test. The certainty of evidence was evaluated using the GRADE approach, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. Data synthesis and statistical analyses were conducted using Stata version 17 (StataCorp LLC, College Station, TX, USA). Statistical significance was set at P < .05 as a priori.
Subgroup Analysis
A subgroup meta-analysis of the included studies was planned based on the fracture location (thoracic vs lumbar levels), age, and fusion status. Most studies focused on T11-L2 transitional fractures and did not report outcomes separately for thoracic and lumbar levels that prevented a subgroup analysis based on fracture location. Similarly, the data regarding the fusion status and overall outcome were also not consistently reported across the studies. However, subgroup analysis was performed to analyse the association between the overall outcome and age distribution of patients, wherever feasible.
Results
Study Selection
Characteristics of Studies Included in the Analysis
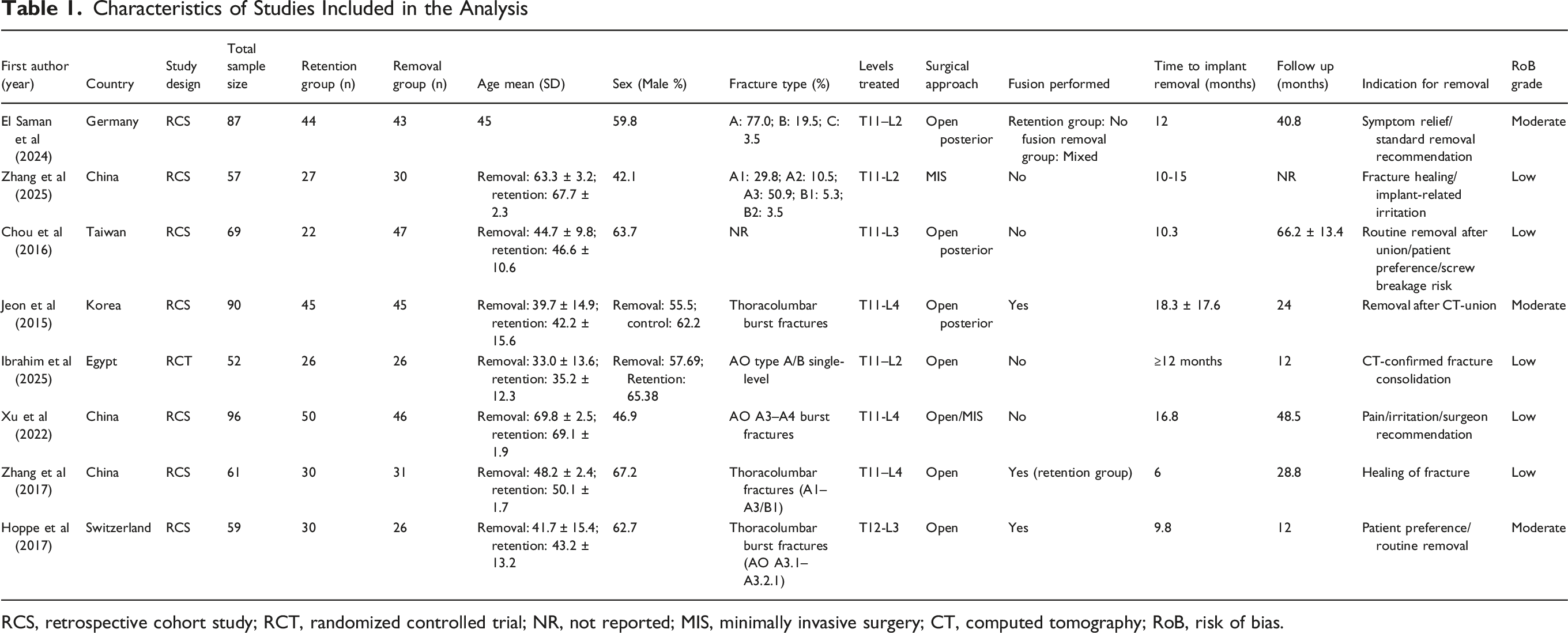
RCS, retrospective cohort study; RCT, randomized controlled trial; NR, not reported; MIS, minimally invasive surgery; CT, computed tomography; RoB, risk of bias.
Characteristics of Included Studies
A. Study designs and populations: The only RCT (by Ibrahim et al,
15
2025) provided strong internal validity, while the rest of the studies were retrospective. The patient demographics varied widely, with the mean ages ranging between 33 and 70 years (indicating different fracture populations). B. Fracture types and levels: A majority of fractures were TL burst injuries (AO types A3/A4), extending between T11 and L4 levels. Six of 8 studies predominantly involved T11-L2 transitional fractures; no study reported outcomes stratified by pure thoracic vs lumbar levels. C. Surgical approaches and fusion: Open posterior fixation was the predominant surgical approach. The fusion practices varied: while some studies performed no fusion in both groups; some studies (eg, Zhang et al,
26
2017) performed fusion only in the retention cohort. D. Timing and Indications for Implant Removal: The typical removal timing ranged from 6 to 18 months, with some variability. The indications for implant removal in the reviewed studies were routine removal after union, painful or irritable hardware, surgeon recommendation and CT-confirmed union.
Risk of Bias Assessment
Five studies were rated low risk,5,12,25,26 including the RCT by Ibrahim et al
15
(2025), which demonstrated a strong methodological rigour (in terms of selection, comparability and outcome assessment). Three studies (El Saman et al,
14
2024; Jeon et al,
27
2015; and Hoppe et al,
16
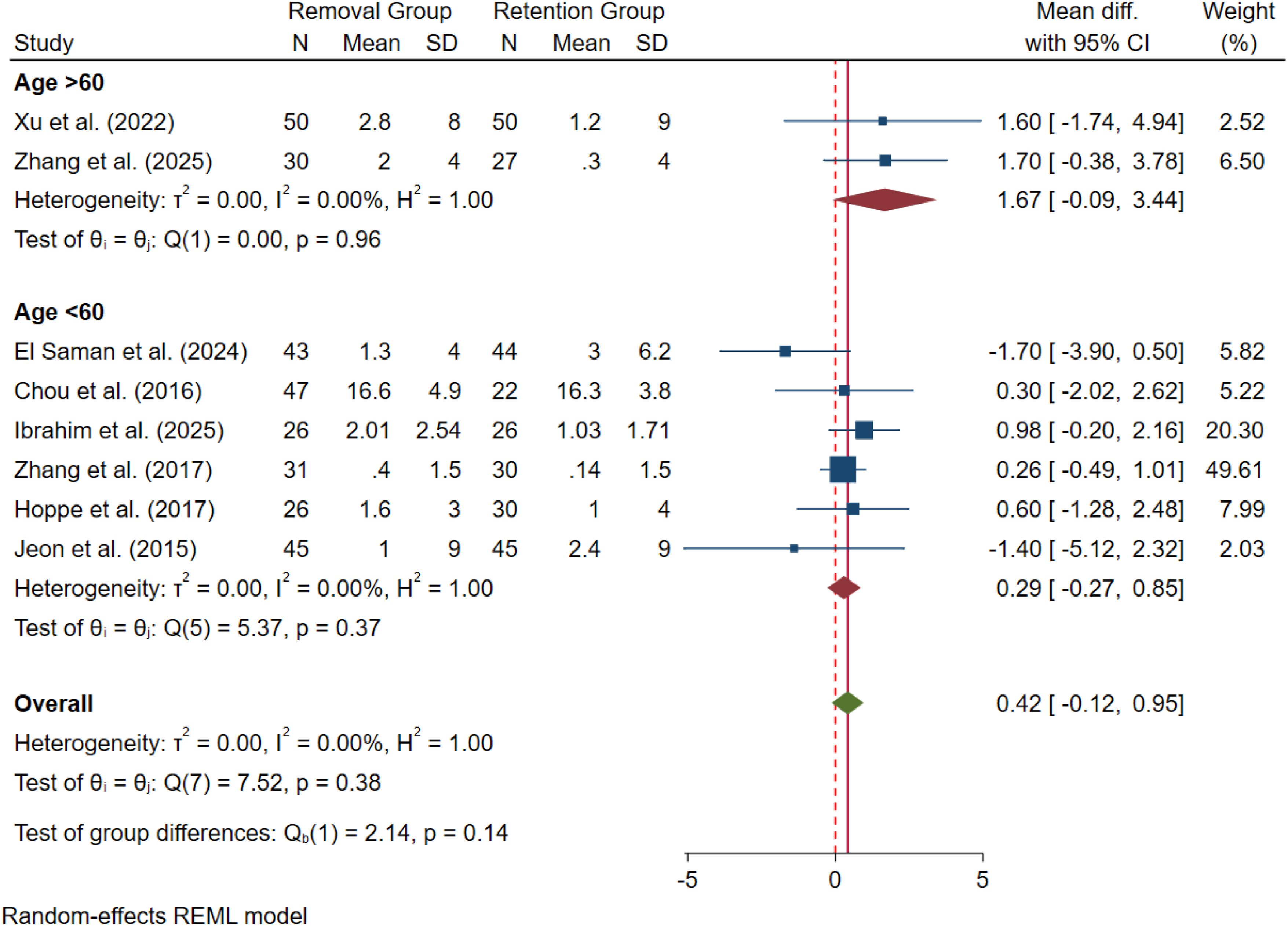
2017) were graded moderate risk, primarily due to baseline group imbalances, incomplete reporting of confounders and concerns regarding outcome measurements). No study was excluded for high risk of bias. Sensitivity analyses, excluding moderate risk studies, demonstrated no material change in pooled effect estimates. Forest plot comparing (A), the implant removal group to the implant retention group for radiological correction (Cobb angle change) at final follow-up compared to preoperative status; (B), advancement of kyphosis post-implant removal compared to the implant retention group Forest plot of subgroup analysis of the implant removal cohort among the included studies based on the age group categories and radiological correction (Cobb angle change) at final follow-up, as compared to preoperative status Forest plot of subgroup analysis among the included studies based on the age group categories and advancement of kyphosis (post-implant removal compared to the implant retention group)

Radiological Outcomes
A. Cobb angle correction: Seven studies reported changes in Cobb angle between preoperative and final followup assessments. In the B. Kyphosis Progression: Based on the 8 studies which reported on the kyphosis progression after implant removal; there was no statistically significant increase in the post-surgical kyphosis (at final followup) in
Functional Outcomes [Oswestry Disability Index (ODI)]
Three studies contributed data on ODI. While in the Forest plot comparing the implant removal group to the implant retention group for functional outcome (ODI) at final follow-up compared to preoperative status Forest plot comparing the implant removal group to the implant retention group for (A), surgical site infection; (B), screw related complication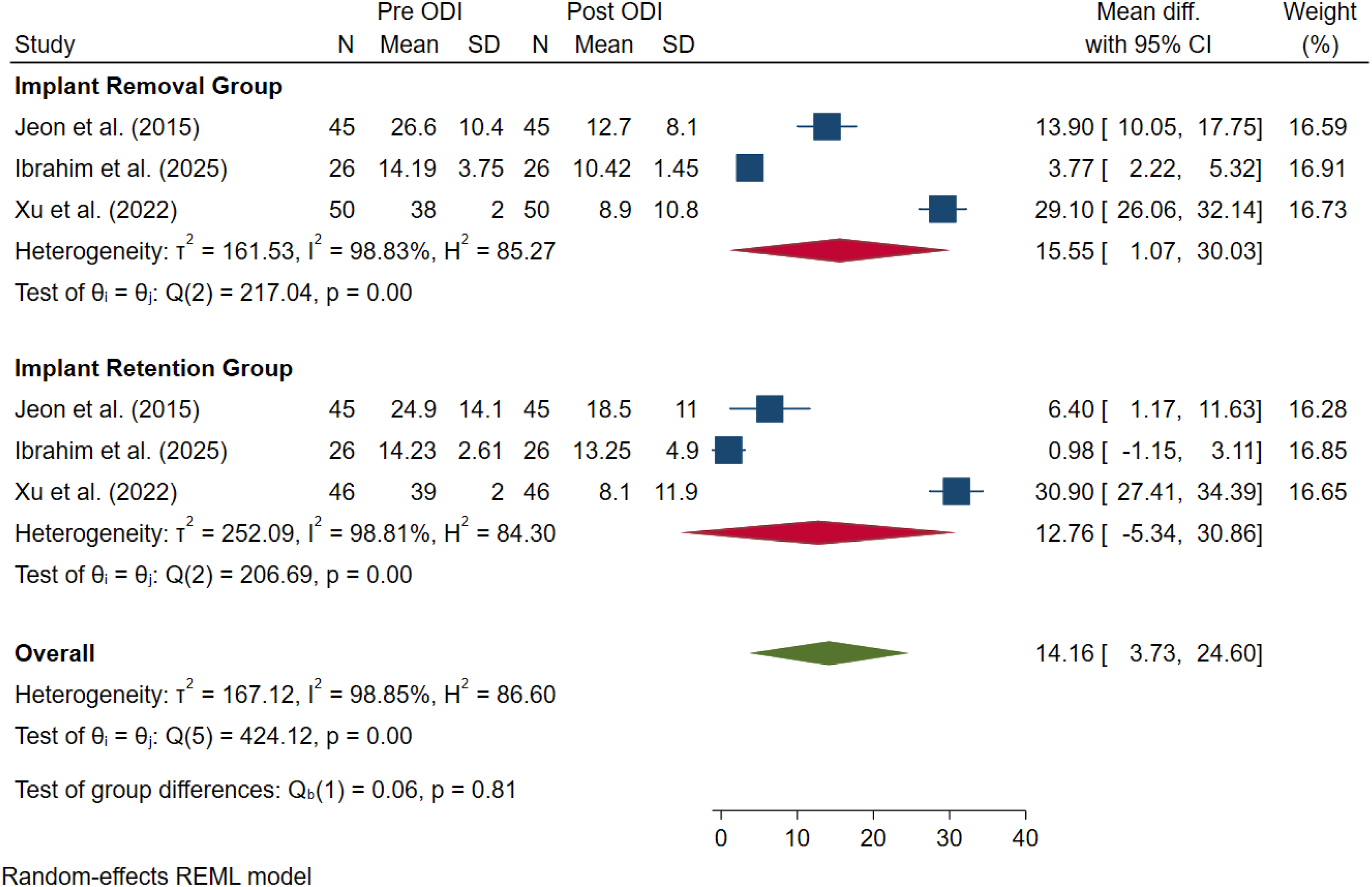

Safety Outcomes
A. Surgical Site Infection (SSI): Eight studies reported SSI rates. The pooled log odds ratio (OR) was –1.42 (95% CI: –4.11-1.28; P = .30; I
2
: 0%; Figure 6A). Thus, based on our analysis, it was evident that implant removal was not associated with enhanced risk of SSI. The events were rare, with a majority being superficial infections in the B. Screw-related Complications: Eight studies reported on mechanical (screw-related) complications. The pooled log OR was 0.59 (95% CI: –1.09-2.26; P = .80; I
2
: 29%; Figure 6B). Thus, the overall incidence of screw-related complications (screw loosening, implant breakage or back-out etc.) was not significantly higher with long-term retained implants
Secondary Outcomes
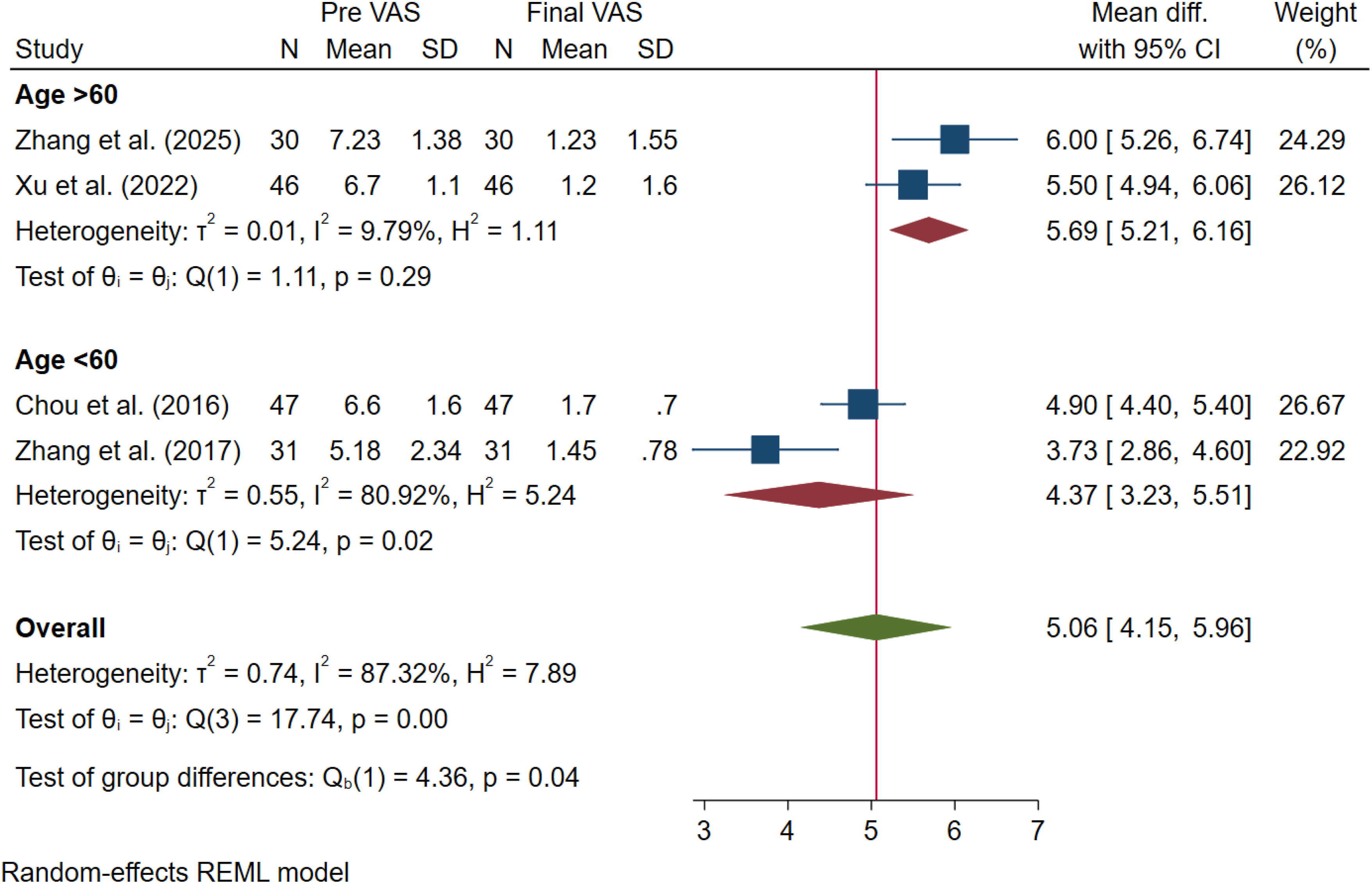
Pain Scores (VAS)
Both the groups showed significant within-group improvement (5-point reduction in pooled MD); with significant reduction in pain for both Forest plot comparing the implant removal group to the implant retention group for pain improvement (VAS change) at final follow-up compared to preoperative status Forest plot of subgroup analysis of the implant removal cohort among the included studies based on the age group categories for VAS outcome at final follow-up compared to preoperative status
Reoperation rates
The reoperation rates were infrequently reported (<5%), with no clear difference between
Other patient-related outcome measures (PROMs)
A minority of studies reported on additional PROMs (such as SF-36 physical (PCS) and mental component scores (MCS). These demonstrated improvements were consistent with ODI findings; with statistically significant within-group changes and non-significant intergroup (
Publication Bias and Certainty of Evidence
GRADE Summary of Findings Table
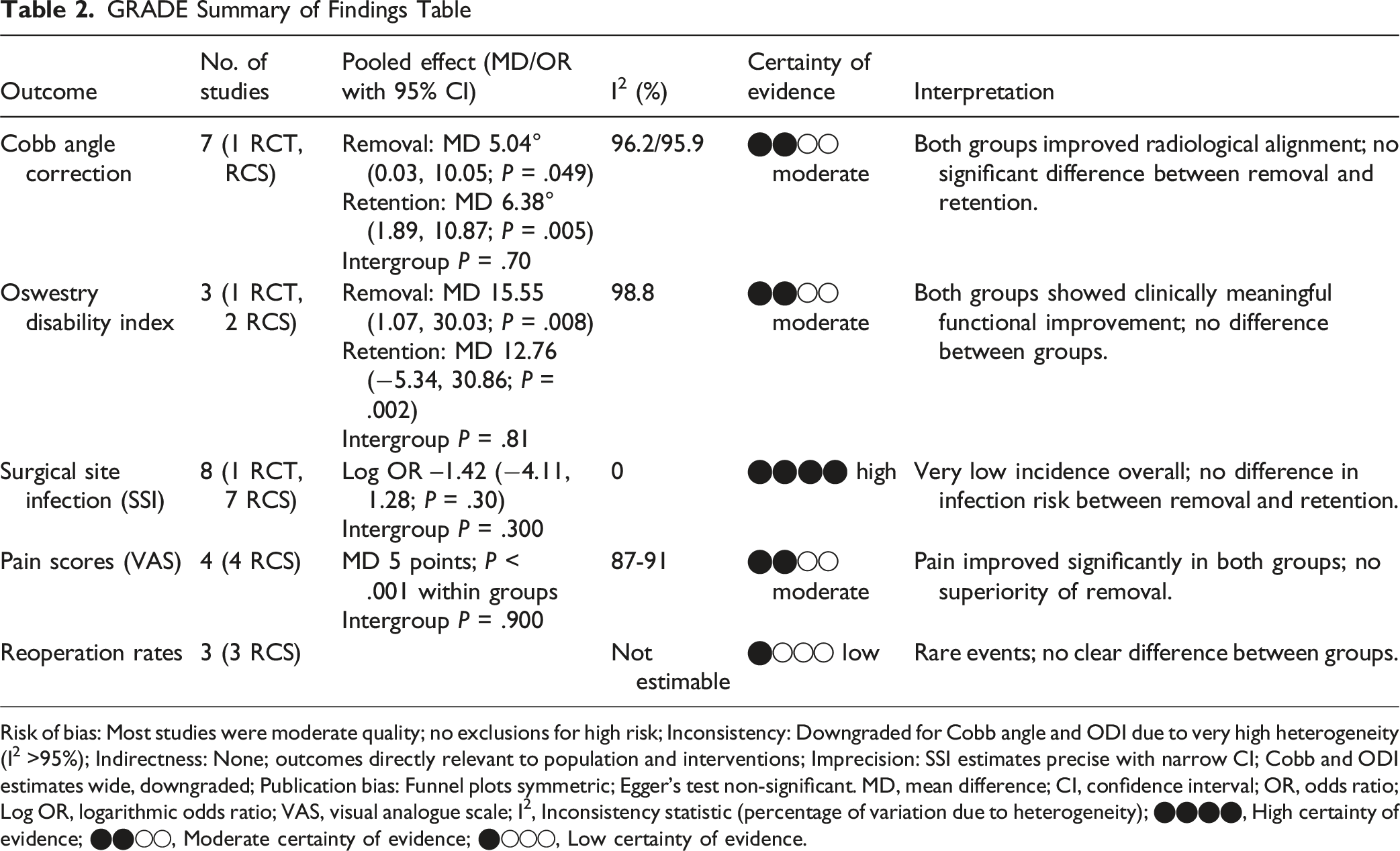
Risk of bias: Most studies were moderate quality; no exclusions for high risk; Inconsistency: Downgraded for Cobb angle and ODI due to very high heterogeneity (I2 >95%); Indirectness: None; outcomes directly relevant to population and interventions; Imprecision: SSI estimates precise with narrow CI; Cobb and ODI estimates wide, downgraded; Publication bias: Funnel plots symmetric; Egger’s test non-significant. MD, mean difference; CI, confidence interval; OR, odds ratio; Log OR, logarithmic odds ratio; VAS, visual analogue scale; I2, Inconsistency statistic (percentage of variation due to heterogeneity); ⬤⬤⬤⬤, High certainty of evidence; ⬤⬤◯◯, Moderate certainty of evidence; ⬤◯◯◯, Low certainty of evidence.
Discussion
This systematic review and meta-analysis synthesized the best available comparative evidence evaluating implant removal vs retention following posterior fixation of TL fractures. Across the 8 studies encompassing 571 patients including the first RCT 15 on this subject, several clinically important findings emerge. Overall, implant removal and retention produced similar radiological and functional outcomes, with no significant differences in Cobb angle correction, kyphosis progression, ODI improvement, VAS pain scores, and SSI. These findings challenge the long-held assumption that routine implant removal necessarily confers superior recovery; and instead support a more nuanced, patient-focussed, decision-making approach.
Radiological Outcomes: Stability Without Fusion is Predictable in Most Patients
Radiological correction improved significantly in both
Importantly, kyphosis progression following implant removal, a major concern historically, was not observed in the pooled data (MD 0.41°, P = .37). Only one included study (Hoppe et al 16 ) demonstrated a measurable increase (∼6°) following implant removal, particularly in younger patients and junctional fractures; however, even this radiological aberration did not translate into inferior clinical outcomes. Collectively, the evidence suggests that, in the absence of severe preoperative kyphosis, comminution or structural anterior column deficiency, implant removal does not predispose to clinically significant loss of correction.
Functional Outcomes: Meaningful Improvement Occurs Regardless of Hardware Status
Both implant removal and retention groups demonstrated significant improvements in ODI from baseline to final followup. The magnitude of improvement exceeded established minimal clinically important differences (MCID) in nearly all studies, reflecting the natural recovery trajectory after TL fractures. The absence of between-group differences implies that implant removal is not required for functional improvement in the general patient population. Although some individual studies, especially those involving younger or more active cohorts, reported superior pain or disability outcomes following implant removal; these findings were not consistently reproduced across the broader evidence base. The RCT by Ibrahim et al 15 reported statistically superior EQ-5D-5L and ODI scores in the implant removal group; however, the pooled data revealed no overall functional superiority attributable to implant removal.
Pain Outcome and Motion Restoration: Benefits Are Highly Context-Dependent
Pooled VAS pain scores improved substantially within both treatment groups. Despite claims that implant removal alleviates hardware-associated irritation or restores segmental motion; our analysis did not demonstrate a significant between-group difference. Nonetheless, motion restoration remains a biologically plausible mechanism for symptom relief, especially in non-fusion constructs, supported by biomechanical studies and selected clinical cohorts.4,23,27,41 Younger patients, individuals with high physical demands and those treated with minimally-invasive percutaneous fixation, are most likely to experience symptomatic improvement following implant removal. This aligns with findings from Visagan et al 23 and Jeon et al, 27 who reported subjective benefit in 60-70% of individuals after screw removal. These subgroup effects, while clinically relevant, were insufficiently consistent or large in magnitude to influence the pooled outcome.
Safety and Complications: Removal Is Safe, but Not Risk-Free
SSIs, screw-related complications and reoperations were rare in both the groups. The pooled OR of SSI were low and equivalent between
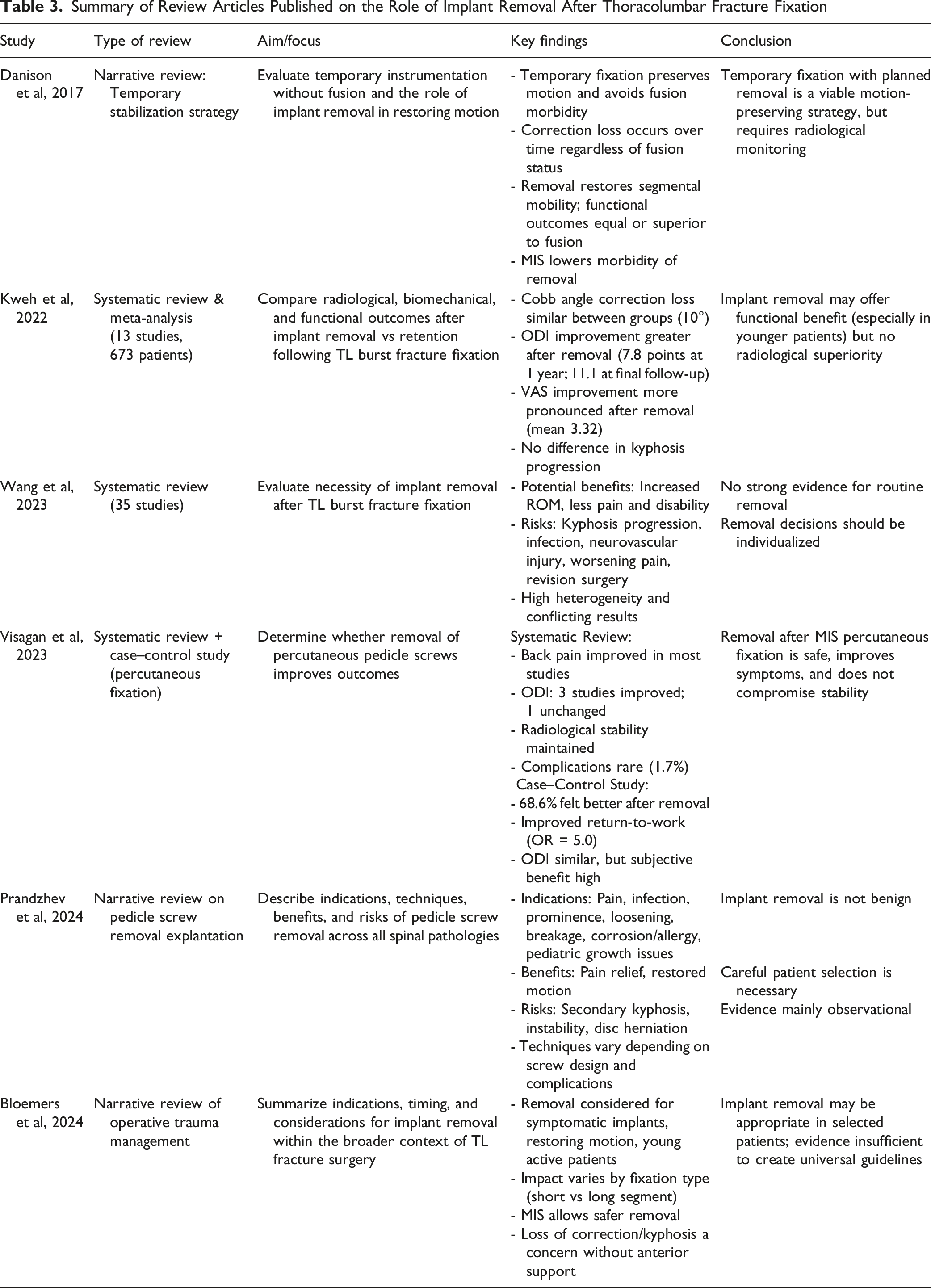
Interpretation in the Context of the Current Literature
Summary of Review Articles Published on the Role of Implant Removal After Thoracolumbar Fracture Fixation
Integrated Synthesis of Observations From Prior Review Articles on Implant Removal vs Retention in Thoracolumbar Fractures
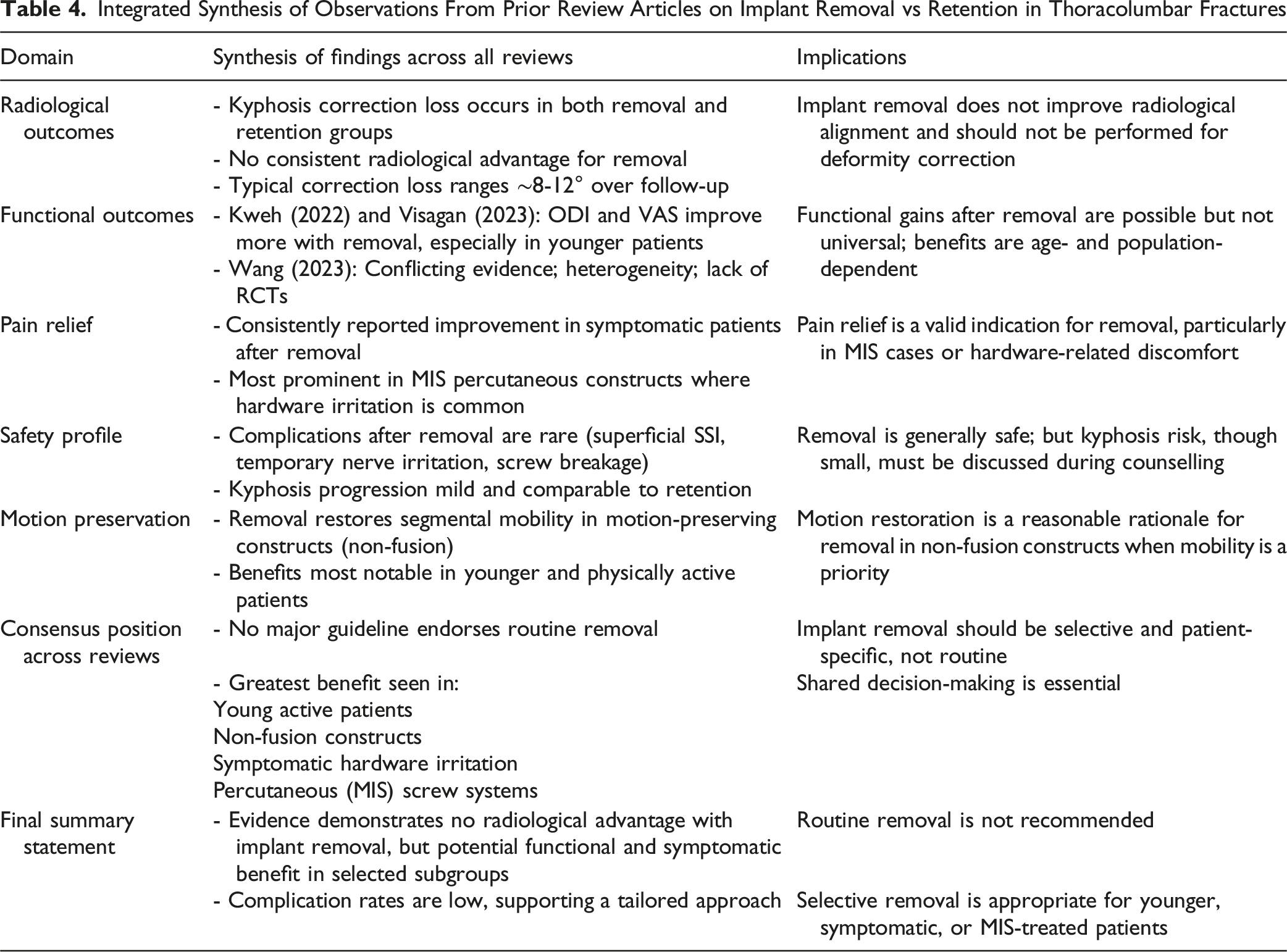
Importantly, emerging evidence in elderly patients (Xu et al 5 ) questions the utility of removal in populations with limited mobility demands or greater operative risk. In contrast, younger individuals, patients with symptomatic implants and those seeking maximal segmental mobility may derive more meaningful improvement, supporting a more selective, instead of a universal approach.
Regional Considerations: Thoracic vs Lumbar Fractures
Biomechanical differences between the thoracic and lumbar spine may theoretically influence outcomes following implant removal. The thoracic spine benefits from rib cage stabilization and reduced motion, whereas the lumbar spine is characterized by greater segmental mobility and axial loading. These differences could potentially impact kyphosis progression, motion restoration and pain outcomes following hardware removal.
However, the majority of included studies primarily involved fractures within the T11-L2 transitional zone, and outcomes were not reported separately for thoracic vs lumbar levels. As a result, regional subgroup analysis was not methodologically feasible. Future prospective trials with stratified reporting by anatomical region are warranted to clarify whether lumbar fractures derive greater functional benefit from implant removal compared with thoracic injuries.
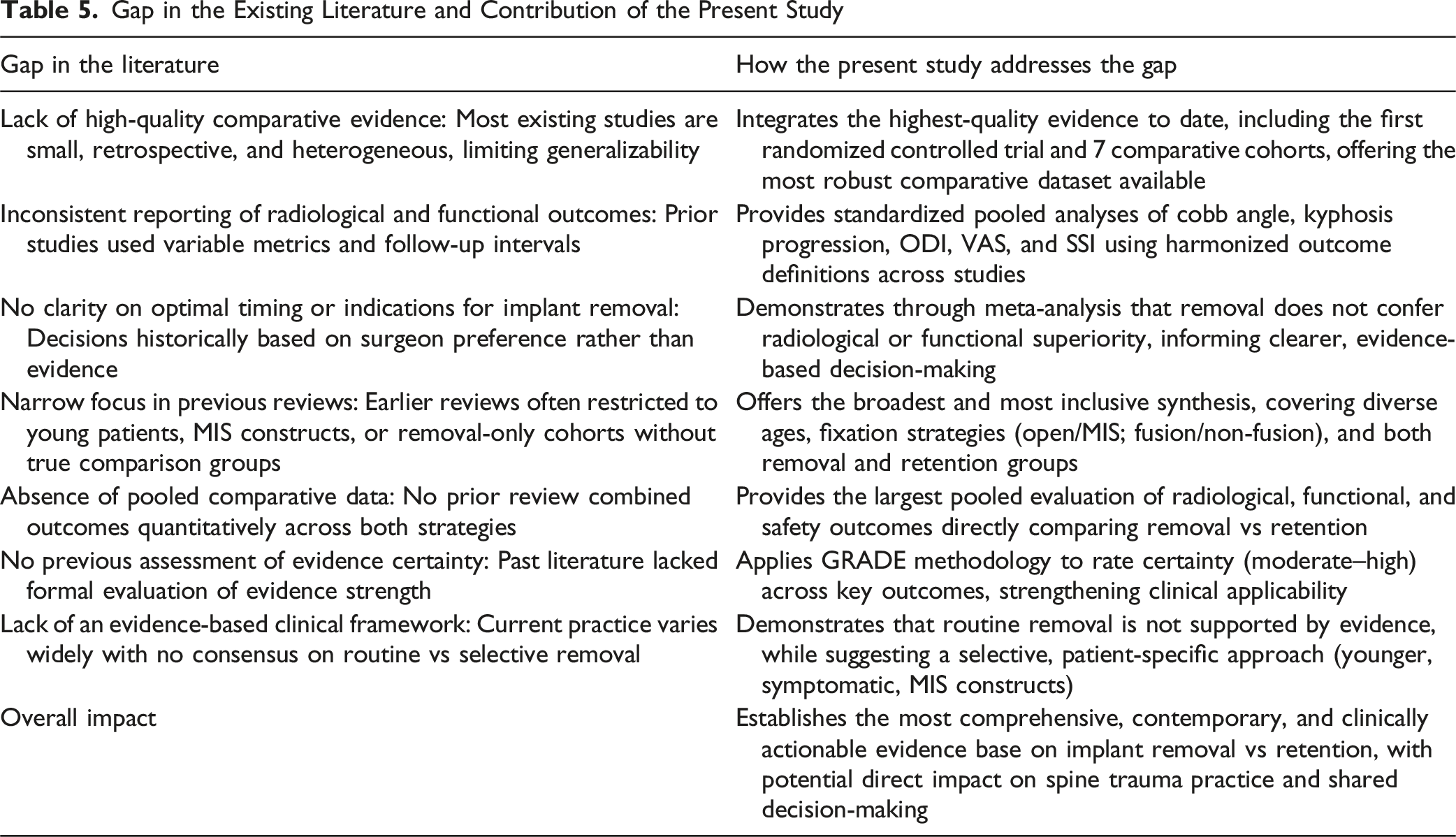
Clinical Implications of Our Observations
Based on the current evidence, the following principles may guide clinical decision making: a. Routine implant removal is not indicated for a majority of healed TL fractures b. Selective removal is reasonable in younger, active patients or those with symptomatic implants or motion preserving constructs (non-fusion, MIS/percutaneous fixation) c. Radiological Safety of implant removal procedure (if indicated) is reliable, with minimal risk of kyphosis progression in well-healed fractures d. Elderly patients may not benefit substantially and may be better managed with implant retention e. Shared decision making must incorporate patient expectations, activity level, surgical risk profile and fracture morphology. Table 5 summarizes the gap in the existing literature; and how the findings of the current study address the concerns and ambiguity on this subject. Gap in the Existing Literature and Contribution of the Present Study
It is important to distinguish between routine implant removal and symptom-driven removal. While routine removal after union is not supported by pooled evidence, removal for symptomatic hardware irritation remains a valid indication. Patients with implant prominence, paraspinal muscle irritation, or discomfort during activity, particularly after minimally invasive percutaneous fixation, may experience meaningful subjective improvement following removal. Thus, removal should be individualized rather than protocolized.
Importantly, the present metaanalysis primarily evaluates routine elective removal after fracture union rather than symptom-driven removal. While several individual studies report subjective improvement in patients with hardware irritation, these outcomes were not consistently quantified across comparative cohorts and could not be pooled. Thus, conclusions regarding removal for clearly symptomatic hardware should be interpreted separately from routine removal strategies (Figure 9). Funnel plot for Cobb angle and Galbraith plot to explore the publication bias and heterogeneity in included studies for analysis, respectively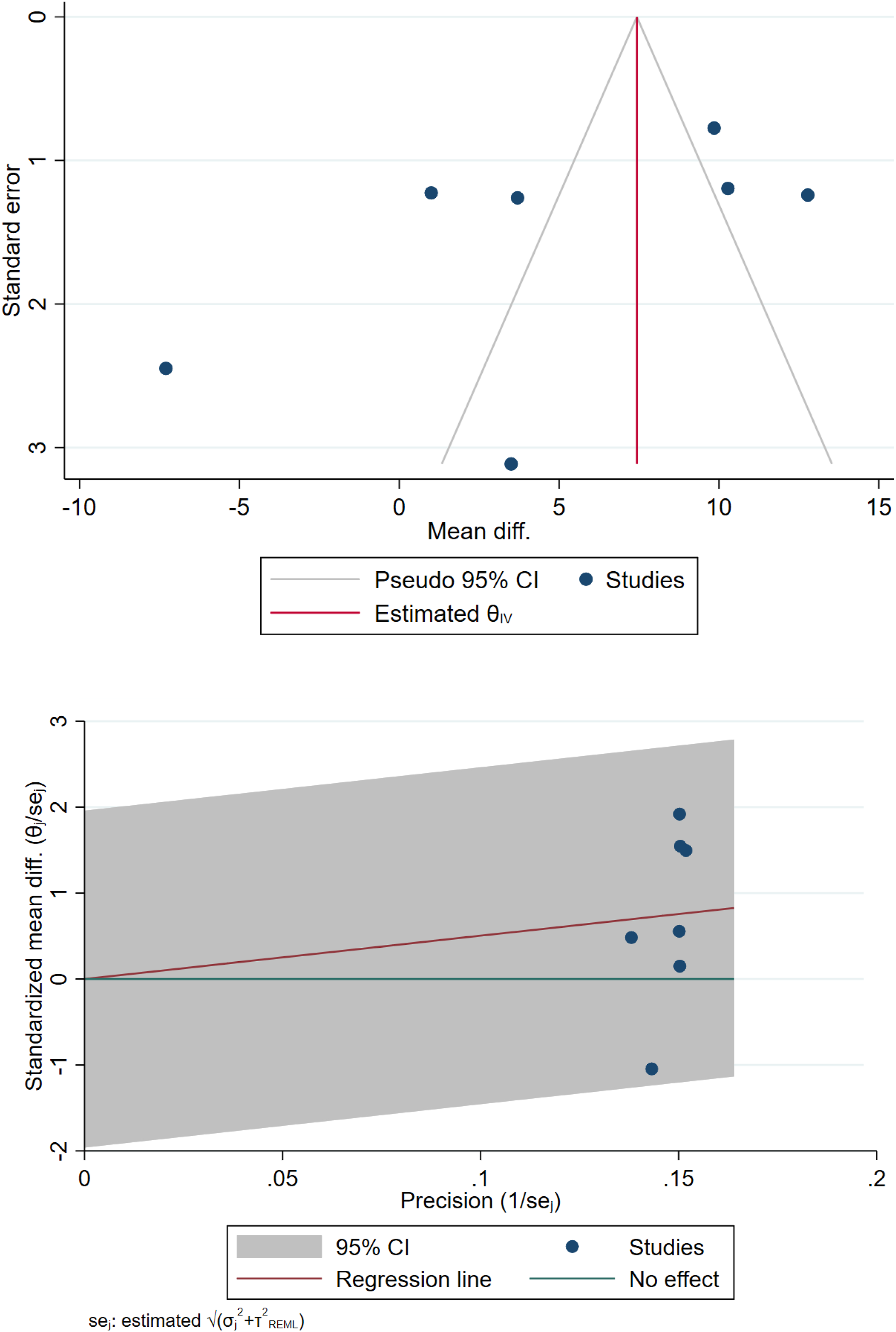
Strengths and Limitations
This review is strengthened by comprehensive methodology, adherence to PRISMA standards, inclusion of the highest-quality evidence; and the ability to quantify pooled radiological and clinical outcomes.
Some of the crucial limitations include the predominance of retrospective data, heterogeneity in fracture patterns and fixation strategies, inconsistent followup intervals, and variation in removal timing. The high heterogeneity in ODI analyses reflects these differences. Subgroup analyses were limited by insufficient granular data, particularly regarding fusion status, anterior column integrity and physiologic age.
An additional limitation is the inability to perform subgroup analyses by fracture localization (thoracic vs lumbar) or anterior column integrity due to lack to granular reporting in the included studies. Most studies pooled transitional T11-L2 fractures without stratified outcome data, limiting region-specific conclusions.
The present analysis was limited by lack granular subgroup reporting across included studies. Specifically, outcomes were not consistently stratified by fusion status, anterior column integrity, or fracture comminution severity. These variables may influence biomechanical behaviour and functional recovery following implant removal and warrant prospective investigation.
Long-term outcomes beyond 3 years were inconsistently reported, limiting assessment of late adjacent segment degeneration or delayed mechanical complications. Additionally, cost-effectiveness analyses comparing removal vs retention strategies were not available in the included literature.
Future Directions
Future research should prioritize adequate powered randomized controlled trials stratified by fracture localization (thoracic vs lumbar), construct type (fusion vs non-fusion), and patient activity level. Particular attention should be directed toward younger, high-demand populations treated with motion preserving constructs, where the potential functional benefits of implant removal may be more pronounced. Long-term followup beyond 3 to 5 years is required to evaluate adjacent segment degeneration, disc health and delayed mechanical changes. Additionally, formal cost cost-effectiveness and health economic analyses are needed to better define the economic and functional implications of selective implant removal strategies.
Conclusion
Implant removal after posterior TL fracture fixation offers no radiological or functional superiority over implant retention for the general patient population. Both strategies achieve stable sagittal alignment, meaningful recovery, and low complication rates. Removal may benefit carefully selected patients, particularly younger, symptomatic individuals treated with non-fusion constructs, but the routine practice of implant removal cannot be recommended. Individualized, evidence-informed, decision-making remains essential.
Author Contributors
Dr SMuthu and Dr VKV contributed to the conceptualization and design of the research goals and aims. Dr SMuthu developed the methodology and statistical framework. Dr SM, DVKP carried out the data collection. Data validation and ensuring the accuracy of results were undertaken by Dr SMuthu and Dr VKV. Writing the original draft of the manuscript was managed by Dr SMuthu, and Dr VKV, with Dr KS, Dr SKRC, Dr LH, Dr ST providing critical revisions and editing. Visualization and creation of figures were executed by Dr SMuthu. Supervision and coordination of the project were led by Dr SMuthu. Dr KS, Dr LH, Dr ST and Dr SKRC helped in the revision of the manuscript. All the authors approved the final version of the manuscript.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data generated in the study will be made available upon reasonable request to the authors.