
Abstract
Study Design:
Systematic review and meta-analysis.
Objectives:
To compare biomechanical and functional outcomes between implant removal and implant retention following posterior surgical fixation of thoracolumbar burst fractures.
Methods:
A search of the MEDLINE, EMBASE, Google Scholar and Cochrane Databases was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
Results:
Of the 751 articles initially retrieved, 13 published articles pooling 673 patients were included. Meta-analysis revealed there was a statistically significant improvement in sagittal Cobb Angle by 16.48 degrees (9.13-23.83, p < 0.01) after surgical stabilization of thoracolumbar burst fractures. This correction decremented to 9.68 degrees (2.02-17.35, p < 0.01) but remained significant at the time of implant removal approximately 12 months later. At final follow-up, the implant removal group demonstrated a 10.13 degree loss (3.00-23.26, p = 0.13) of reduction, while the implant retention group experienced a 10.17 degree loss (1.79-22.12, p = 0.10). There was no statistically significant difference in correction loss between implant retention and removal cohorts (p = 0.97). Pooled VAS scores improved by a mean of 3.32 points (0.18 to 6.45, p = 0.04) in the combined removal group, but by only 2.50 points (-1.81 to 6.81, p = 0.26) in the retention group. Oswestry Disability Index scores also improved after implant removal by 7.80 points (2.95-12.64, p < 0.01) at 1 year and 11.10 points (5.24-16.96, p < 0.01) at final follow-up.
Conclusions:
In younger patients with thoracolumbar burst fractures who undergo posterior surgical stabilization, planned implant removal results in superior functional outcomes without significant difference in kyphotic angle correction loss compared to implant retention.
Introduction
Implant removal following surgical stabilization of thoracolumbar burst fractures is known to alleviate pain and functional outcomes in symptomatic patients.1,2 However, there exists ongoing debate as to whether patients who undergo surgical fixation with or without arthrodesis of thoracolumbar burst fractures should have their instrumentation routinely removed on follow-up.3,4The planned removal of implants, usually approximately 12 months later, has the purported benefits of reducing the long-term risk of stress shielding, infection, foreign body reaction, micromotion, instrumentation failure, adjacent level disease and metal fretting.5-9 These advantages of implant removal are countered by concerns that implant removal may lead to significant correction losses and progressive kyphotic deformity, irrespective of whether fusion has occurred.10-14
The importance of determining the appropriate disposition of implants following instrumented fixation of thoracolumbar burst fractures has become increasingly relevant for 2 reasons: prevalence of this injury and current surgical trend. Firstly, the thoraco-lumbar junction represents the transition point between the relatively fixed kyphotic thoracic and comparatively mobile lordotic lumbar regions and therefore is biomechanically the weakest point of the spine. 15 Consequently, fractures at this location constitute more than 90% of fracture of the spine, with burst fractures composing 10-20% of these injuries.16,17 This carries the potential for significant morbidity with over 50% being associated with neurological deficit and kyphotic deformity.18-20
As such, contemporary surgical management is aimed at correcting kyphotic deformity and minimizing neurological injury by direct or indirect decompression of the spinal cord or nerve roots to alleviate pain and facilitate early mobilization and functional recovery.17,21 This can be achieved by a variety of surgical methods. A common technique is the use of open or percutaneous pedicle screw fixation with either short or long segment instrumentation. The principal aim of our review and meta-analysis was to comprehensively evaluate both the biomechanical parameters and functional outcomes of planned implant removal versus implant retention following surgical fixation of thoracolumbar burst fractures. We hypothesized that the kyphotic correction losses would be equivalent between the 2 cohorts, but that instrumentation removal may result in superior functional outcomes while obviating long-term consequences such as adjacent level disease.
Methods
Eligibility Criteria
The Population, Intervention, Comparison and Outcome (PICO) query for this systematic review was: ‘In patients who have sustained thoracolumbar burst fractures who undergo posterior surgical stabilization with or without arthrodesis (P), does the planned removal of surgical implants (I) compared to implant retention (C) result in improved biomechanical or functional outcomes’.
Information Sources and Search
A systematic electronic search of Medline, EMBASE, Google Scholar and Cochrane Database of Systematic Reviews from their date of inception to May 2020 was conducted in a manner strictly adherent to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). 22 Keywords were deliberately selected to capture as many relevant articles as possible. The Medline database was queried with the following search terms using various Boolean combinations: ‘Implant’, ‘Instrument*’, ‘Screw*’, ‘Rod, ‘Metalware’, ‘Hardware’, ‘Remov*’, ‘Temp*’, ‘Vertebra*’, ‘Fracture’. It is noteworthy that the term ‘burst’ was not utilized in the searches, thereby capturing all studies which captured thoracolumbar fractures that may contain data suitable for subgroup analysis. Only studies in the language English in humans were included.
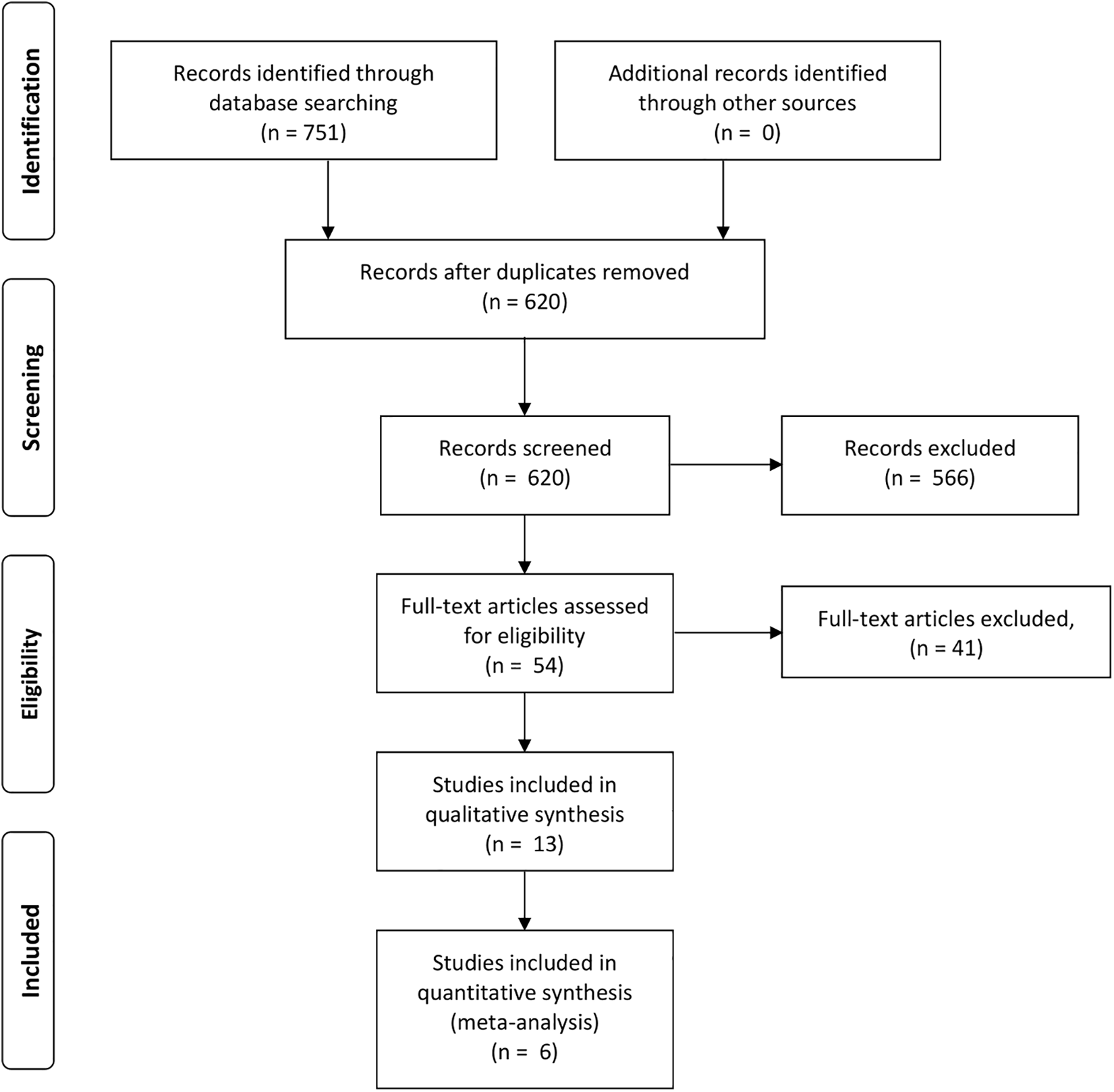
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram. 22
Study Selection
All retrieved titles and abstracts were independently screened by 2 reviewers (BK and TT). This was followed by full-text evaluation of the most relevant studies to determine their suitability for inclusion in the review. The references of all included studies were also interrogated to identify additional eligible articles. Discrepancies were discussed until consensus attained. Inclusion criteria were defined as: 1. Randomized or non-randomized controlled trials, cohort or case series studies examining thoracolumbar burst fractures with or without neurological deficit 2. Posterior surgical fixation, with planned subsequent removal of instrumentation at a defined time point 3. Documentation of clinical or radiological follow-up following removal of instrumentation 4. Acceptable follow-up outcomes include those which relate to clinical neurological status, functional improvement or radiological measures. 5. Where studies share part or all of their dataset, both are to be included in the qualitative review but only the study with the largest data is to be selected for meta-analysis.
Data Collection Process and Data Items
Appropriate studies underwent vigorous independent extraction of data into a preformatted spreadsheet by 1 author (BK), which was meticulously cross-checked by another (TT) in accordance with the Cochrane Handbook for Systematic Reviews. 23 Given the objective of performing a meta-analysis, quantitative variables of particular interest included: Cobb’s angle or kyphosis angle, segmental motion angle, vertebral body height, canal compromise, upper intervertebral angle, superoinferior endplate angle, sagittal index, range of motion scores, Visual Analogue Scale scores of back pain and Oswestry Disability Index results. No authors were contacted for further unpublished data.
Risk of Bias
Risk of bias in individual studies was assessed in accordance with Cochrane recommendations. 23 The Risk of Bias of Randomized Controlled Trials 2 (Rob 2) and the Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool was intended to be applied for any included randomized and non-randomized studies respectively.24,25 Two authors (BK and TT) independently evaluated the quality of included studies across all domains, before reaching consensus by discussion. The ‘Robvis’ tool was utilized to generate traffic light plots in accordance with Cochrane recommendations. 26
Statistical Synthesis and Analysis
Outcomes were meta-analyzed using a DerSimonian and Laird random effects model to control for heterogeneity between studies. The Higgins I-squared statistic was utilized as a measured of inter-study heterogeneity, with a figure greater than 50% deemed significant. 27 Forest plots of effect sizes were generated. Statistical significance was defined as a p value of < 0.05. All meta-analysis was performed using the open source statistical software Open MetaAnalyst (Providence, Rhode Island).
Results
Study Selection
The comprehensive search yielded 751 articles which was culled to 620 after discarding duplicate articles. Abstracts were screened resulting in distillation to 54 studies demanding full-text consideration. This eventually yielded 13 articles, consisting of 12 cohort studies and a single case-control trial. Common reasons for exclusion were absent documentation of clinical or radiological outcome following insertion or removal of implant, inappropriate inclusion of alternative fracture types and review articles lacking original data.
Study Characteristics
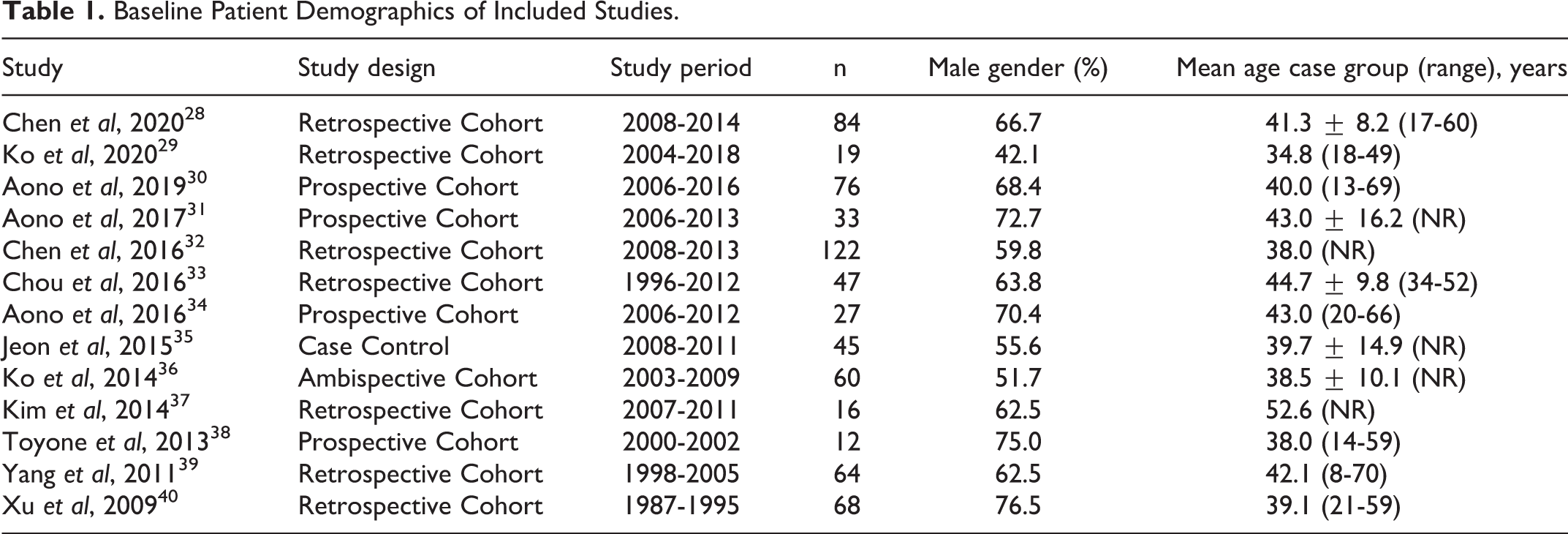
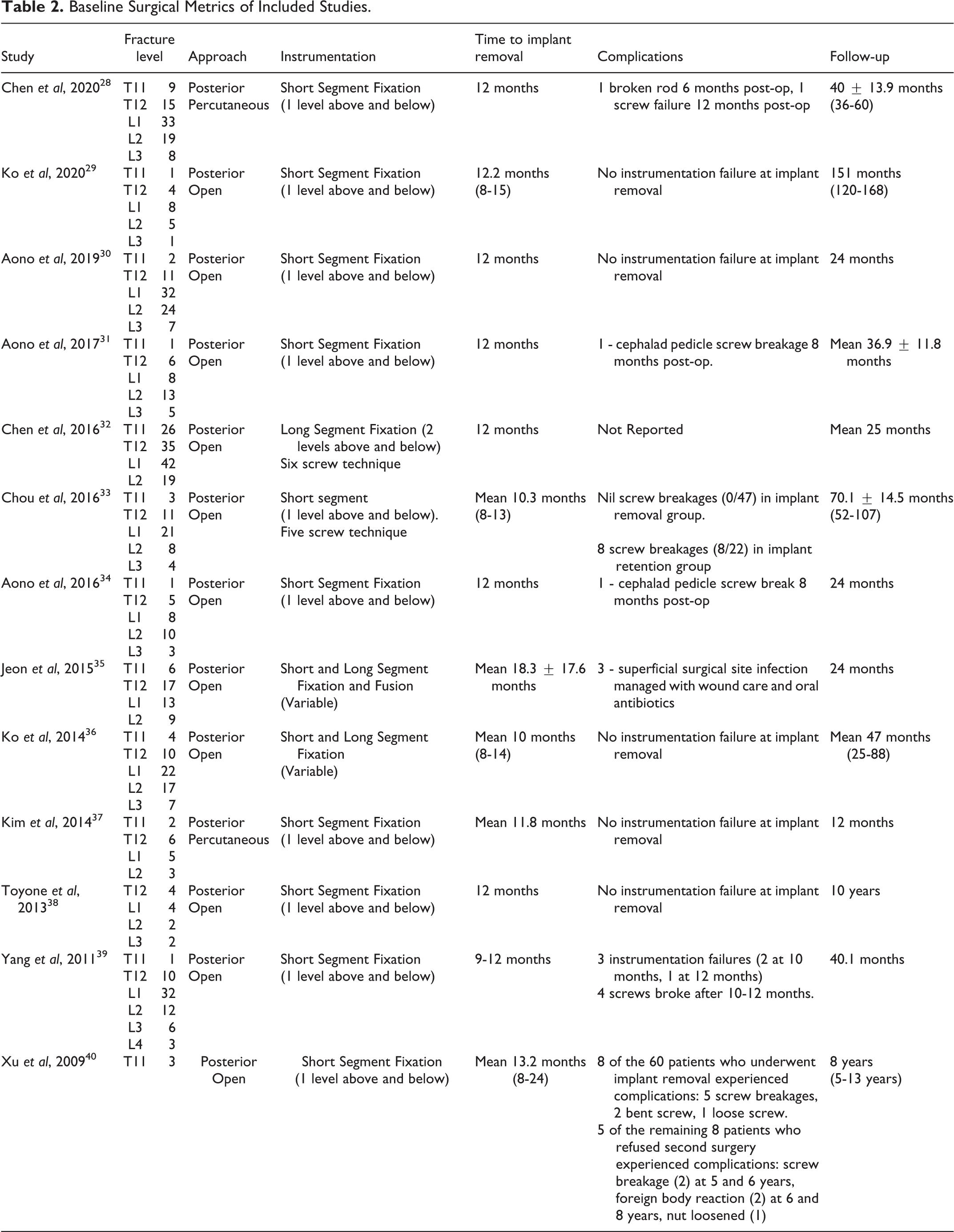
The 13 included studies examined 673 patients who underwent temporary fixation of a thoracolumbar burst fracture with planned implant removal at a later date (Table 1). The weighted mean age of the cohort was 40.5 years (range 13-70 years). Pooled standard deviation of age with data extractable from 5 studies was 11.5 years.28,31,33,35,36 The cumulative percentage of the studied population that was male was 63.7%. The most common level of burst fracture was L1 with 254 fractures (37.7%). Other levels were less commonly fractured with pooled results as follows: T11 with 59 fractures (8.8%), T12 with 148 fractures (22.0%), L2 with 156 fractures (23.2%), L3 with 52 fractures (7.7%) and L5 with 4 fractures (0.6%). All studies employed a posterior surgical approach, with 11 studies using an open technique and 2 utilizing a percutaneous method. Jeon et al were the only study to perform short-segment fusion with autoiliac corticocancellous bone graft. 35 The most common time of implant removal was 12 months (10-24 months) with follow-up occurring 12-120 months post-operatively (Table 2).
Baseline Patient Demographics of Included Studies.
Baseline Surgical Metrics of Included Studies.
Study Quality
Risk of bias assessment was performed with the Risk of Bias In Non-Randomized Studies (ROBINS-I) tool in a Cochrane endorsed fashion (Figure 2). 25 The intrinsic weakness of all studies was performance and detection bias given participants and their treating team were not blinded to the surgical intervention.
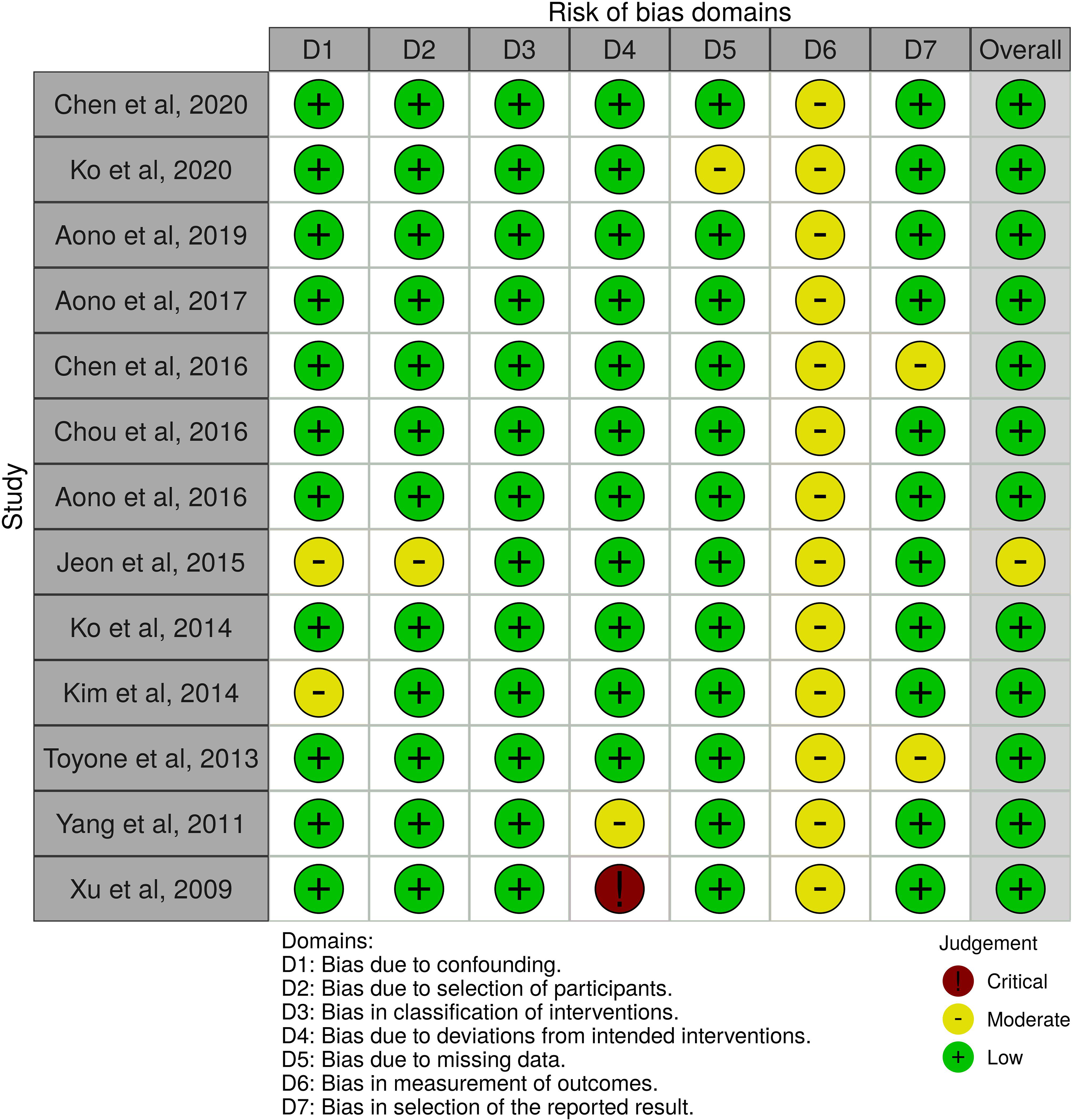
Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) Tool as endorsed by Cochrane. 25
Results of Individual Studies
A tabulated summary (Table 3) presents the pertinent clinical and radiographic outcomes of each study on the role of implant removal in thoracolumbar burst fractures.
Summary of Key Outcomes of Included Studies.
Cobb Angle (Sagittal)
The Cobb Angle (CA) was defined as the intersecting angle on a sagittal radiograph of lines drawn between the superior endplate of the vertebra one level cranial to the fractured vertebra, and the inferior endplate of the vertebra one level caudal to the fractured vertebra. 32 A positive value represents a kyphotic angle whereas a negative value signifies a lordotic angle. This same measurement was also referred to as the superoinferior endplate angle (SEIA) by 3 studies, and the local kyphotic angle (LKA) by another trial.30,31,34 Given its invaluable use as a surrogate of deformity correction after thoracolumbar burst fracture fixation, 12 of the 13 included studies in this systematic review reported the Cobb Angle as an outcome measure.29-40
Seven of these studies demonstrated that there was statistically significant loss of CA correction after implant removal. In their 2016 study, Aono et al found that just before implant removal at 12 months there was surgical reduction loss by 2.38 degrees, which deteriorated by another 7.58 degrees after removal. 34 This finding was replicated in their proceeding 2017 study in which instrumentation removal resulted in a 2.5 degree correction loss at 12 months just prior to removal, before falling by another 6.8 degrees after 12 months (p < 0.001). 31 Consistent with this, Aono et al again found in 2019 that there was 2.2 degrees of correction loss before implant removal that deteriorated by 6.9 degrees after removal of the temporary stabilization hardware (p < 0.001). 30
In a similar manner, Chen et al demonstrated that the CA markedly improved from 23.7 ± 4.3 degrees pre-operatively to −3.0 ± 1.2 after surgery (p < 0.001), yet returned to a kyphotic deformity of 4.2 ± 1.3 degrees (p < 0.001) at final follow-up suggesting a statistically significant loss of correction. 32 Losses in correction were also found at final follow-up by Toyone et al of 2 degrees at 10 year follow-up, while Xu et al determined a correction loss average of 12.1 degrees at 8 year review.38,40 Yang et al noted that the original pre-operative kyphotic angle of 18.9 degrees (4.5-39.3) demonstrated post-operative improvement to 0.5 degrees (-8.3 to 15.3), but worsened to 3.3 degrees (-4.5 to 16.4) before deteriorating even further at last follow-up (average 40.1 months) to 10.2 degrees (4-19.2) with statistically significant loss of correction (p < 0.001). 39
Conversely, the 2 studies which dichotomized their study cohort into an implant removal and implant retention group found no statistically significant loss of kyphotic correction between time of implant removal and final follow-up.33,35 Chou et al examined 2 groups who had similar baseline pre-operative baseline kyphotic deformities of 18.7 ± 6.9 degrees in the implant removal group compared to 18.8 ± 4.8 degrees in the implant retention group (p = 0.951). 33 After surgical fixation, there was also no significant difference in correction at 1.0 ± 3.2 degrees for the removal group and 1.1 ± 2.1 degrees in the retention group (p = 0.894). 33 Astoundingly, Chou et al found that was no difference in kyphotic deformity at final follow-up of 70.1 ± 14.5 months between the 2 groups with residual deformity of 17.7 ± 4.8 in the removal group versus 17.3 ± 5.0 in the retention group (p = 0.751). 33 Chou et al also argued there was no statistically significant loss in reduction at final follow-up (p = 0.800). 33
This sentiment was echoed by Jeon et al, who posited that between the implant removal and retention groups there were no significant difference in Cobb Angle pre-operatively (18.9 ± 11.2 degrees versus 22.4 ± 10.5 degrees, p = 0.615), post-operatively (11.5 ± 7.5 degrees versus 10.1 ± 6.9 degrees, p = 0.839) or at removal (12.9 ± 9.5 degrees versus 11.7 ± 19.8 degrees, p = 0.568). 35 Tellingly, this trend of equivalent kyphotic angle correction loss continued even at 1 year follow-up despite the implant being removed (15.4 ± 10.2 degrees versus 14.6 ± 8.9 degrees, p = 0.402) as well as 2 year follow-up (14.8 ± 11.5 degrees versus 14.1 ± 9.4 degrees, p = 0.774). 35 At the most severe end of the spectrum of thoracolumbar burst fractures in those with neurological deficit, Chen et al found there was no significant loss of correction from post-operatively (4.0 ± 1.9 degrees) to final follow-up (4.9 ± 2.0 degrees, p > 0.05). 28
Significantly, these 2 comparison studies reflect the powerful finding of the longest longitudinal study to date which followed patients for 10 years. 29 In their landmark trial, Ko et al found that the CA improved from 26.89 ± 6.08 degrees, at time of injury, to 10.37 ± 1.98 after implant removal 1 year, and remained at 10.11 ± 2.22 upon final follow-up. 29 Vitally, there was no significant loss of correction angle at last follow-up compared with 1 year after removal surgery (p = 0.71). 29 Interestingly, this finding was what Ko et al already suspected in their 2014 study which found that the significant kyphotic correction angle (p = 0.005) attained after surgical fixation was maintained at follow-up (mean 47 months). 36
Overall, seven studies found statistically significant loss of Cobb angle deformity correction after implant removal. However, the 2 comparative studies and the longest study to date suggest that this degree of kyphotic correction loss is similar regardless of whether the implant is retained or removed.
Segmental Motion Angle
The theory of segmental motion angle is that on dynamic movement, between flexion and extension of the thoracolumbar spine, removal of implantation should facilitate a greater range of motion and therefore minimize the chance of adjacent level degenerative disease. 35 Jeon et al found that the segmental motion angle of the removal group improved from 1.6 ± 1.5 degrees after implant removal to 5.8 ± 3.9 degrees at 1-year follow-up (p = 0.000), and this persisted even at 2-year follow-up (5.9 ± 4.1 degrees, p = 0.000). 35 Kim et al also determined that range of motion significantly improved at final follow-up after implant removal (p < 0.01). 37
On the other hand, Ko et al found that segmental motion was greatest at 10.43 ± 3.32 degrees 1 year post removal surgery, and actually decreased to 9.27 ± 3.34 at last follow-up 10 years later showing a decline over time (p = 0.028). 29 However, this longitudinal study over 10 years may have been confounded by the increasing age of the patient and a natural progression for reduced range of motion with the natural history of a degenerative spine.
Vertebral Body Angle and Vertebral Body Ratio
Vertebral body angle (VBA), alternatively known as the vertebral wedge angle (VWA), is defined as the angle between intersecting lines which are drawn from the superior endplate of the fractured and the inferior endplate of the fracture vertebra.30-32,34 Along with anterior body height ratios (ABHR), it has been proposed as a marker of spinal deformity following thoracolumbar burst fractures.29,36 The value of the VBA lies in the fact that if the Cobb Angle demonstrates loss of correction but the VBA does not, one can deduce that it is actually the intervertebral disc spaces which have been greatly affected by the burst fracture rather than the bony structures themselves. This measurement was reported in 9 of the included studies.29-34, 36, 37, 39
Aono et al in 2016 determined that the VBA was reduced from 17.3 degrees (8-31) to 6.1 degrees (1-11) after surgery. There was already 0.5 degrees loss of correction before removal and a subsequent 0.3 degrees after removal, with no statistically significant loss of correction (p < 0.001). 34 In their later 2017 study, these authors concluded a similar finding of almost no loss of correction of VBA after pedicle screw fixation with or without vertebroplasty. 31 Aono et al continued with this tenet in 2019 by again arguing that VBA corrections were maintained after surgery with only 0.7 degrees loss of correction. 30
On the other hand, Chen et al found that the VWA improved from 35.9 ± 10.2 degrees on admission to 9.6 degrees after surgery (p < 0.001), and remained relatively stable at 10.3 degrees upon final follow-up. 32 Importantly, it was the upper intervertebral angle (UIVA) that demonstrated a statistically significant angle loss of 5.7 degrees (p < 0.001). 32 By comparing implant retention and removal cohorts, Chou et al also observed that there were statistically significant changes in the anterior third of the injured disc height and kyphotic angle in all patients. 33 Indeed, there were no changes in the actual fractured vertebral body height over time across both groups. 33
Considering the vertebral height as a ratio, there is conflicting evidence regarding the changes over time. Two studies by Ko et al both state that there is no significant difference in average anterior body height ratio (ABHR) after removal surgery and correction is maintained.29, 36 This is supported by the stable AVH that Chen et al observed with minimal loss from surgery (97.6% ± 6.5%) to final follow-up 94.3% ± 5.9%. 28 However, Kim et al found evidence of vertebral height loss of 15.3% after implant removal rising to 17.4% at final follow-up (p < 0.01). 37 This was confirmed by Yang et al who noted statistically significant improvement in both AVH and PVH after surgery, but a decline from 94.0% (71.2-107.6) before removal to 88.9% (70.2-103.7) and a decline from to 97.0% (75.2-106.8) pre-removal to 93.7% (74.0-101.2) at last follow-up respectively. 39
Nonetheless, Xu et al sensibly conclude that the height of fractured vertebral body clearly improves by an average reduction of 30.5% after surgery, and subsequent loss of correction observed is likely to be due to adjacent disc space loss rather than directly related to implant deformation. 40 Despite the inconsistent evidence regarding whether correction losses of vertebral body angle and vertebral body height ratios are maintained or sustained, all included studies are unanimous in their affirmation that temporary stabilization provides statistically significant vital reduction in kyphotic deformity of thoracolumbar burst fractures. Furthermore, it is imperative to understand that correction losses are observed 1 year after surgery even before implant removal. It is these losses, purported to be mainly due to loss of adjacent intervertebral disc height, which when followed long-term by Ko et al are found to remain stable. 29
Canal Stenosis
Five studies aimed to confirm the idea that the degree of spinal canal stenosis is expected to improve following surgical fixation and reduction of fracture deformity.28, 30, 31, 34, 39 Intuitively, Aono et al in 2019 determined that a mean canal narrowing was 46.9% (14–88%) pre-operatively markedly improves to 25.9% (7–48%) after surgery, before this trajectory was continued to 14.7% (5–34%) at 2 year follow-up. 30 This was in accordance with both their own earlier findings in 2016 and 2017, as well as those of Yang et al who tracked a preoperative mean canal narrowing of 41.4% to improve to 13.7% at final follow-up (p < 0.01) an average of 40.1 months later.31, 34, 39 Chen et al also found that canal stenosis was markedly improved post-operatively (94.2 ± 4.8%) and remained stable over time (93.7 ± 5.1%). 28
Quality of Life
Five studies utilized the visual analogue scale (VAS) to assess back pain, with 2 studies providing valuable comparative data between implant retention and removal groups.28, 33, 35-37 Jeon et al found that mean VAS scores improved in the removal group from 3.8 ± 2.1 at the time of implant removal, decreasing to 1.6 ± 1.6 at 1-year follow-up (p = 0.000) which was still significant at 2-year follow-up at 2.1 ± 1.7 (p = 0.000). Interestingly, the mean VAS score in the implant retention group was 3.9 ± 2.5 at 18-month follow-up, but this group reported greater levels of pain with scores of 3.5 ± 1.8 and 3.6 ± 1.6 at 1 and 2 year follow-up respectively without a statistically significant reduction (both p > 0.05). 35
Additionally, Chou et al demonstrated no difference in VAS at final follow-up between implant removal (1.7 ± 0.7) and implant retention (2.0 ± 0.9), p = 0.134. 33 Kim et al reported significant pain relief with the VAS scale after removal (p < 0.005), with Ko et al also exhibiting low mean VAS scores of 1.77 ± 0.99.36, 37 Even in patients who have suffered neurological deficits, Chen et al determined a statistically significant reduction in VAS scores with improvement from 7.8 ± 1.1 preoperatively to 2.9 ± 1.3 (p < 0.05) at 1 week postoperatively, and a continued positive trend to 1.2 ± 0.8 upon final follow-up. 28
A similar finding is reported using other measures of low back scale, such as the Greenough scale by Chou et al: there was no difference at final follow-up between implant removal (66.8 ± 7.1) and implant retention (65.7 ± 5.3), p = 0.52. 33 By the same token, Ko et al discovered 83.3% of patients volunteer good to excellent results on the Smiley-Webster scale. 36 Aono et al, Toyone et al and Xu et al assessed patients’ functional status using the Denis pain scale, and all studies demonstrated that there were no patients so severely limited that they were unable to perform their activities of daily living.34, 38, 40
In a similar manner, Ko et al reported statistically significant improvement in Oswestry Disability Index (ODI) scores from 15.86 ± 7.93 to 7.96 ± 7.38 at last follow-up (p < 0.001). 29 Jeon et al concurred with this finding when they noted that mean ODI at implant removal was 26.6 ± 10.4 improving to 16.3 ± 11.5 at 1-year follow-up (p = 0.000), which was further reduced to 12.7 ± 8.1 (p = 0.000) at 2 years. In patients with neurological deficit who registered exceptionally high disability indices, Chen et al witnessed a remarkable fall in disability from 86.1 ± 8.8 preoperatively to 15.9 ± 6.4 (p < 0.05) at 1 year, and a further improvement to 8.4 ± 4.6 at final follow-up. 28 This finding at the severe end of the spectrum of neurological deficit should be interpreted with caution, given some improvement might be attributed to adjuvant measures and time since injury rather than solely the removal of implants. In contrast to these studies, Jeon et al observed no statistically significant change given the ODI of the control group from the initial ODI of 24.9 ± 14.1 at 18 months remained without statistically significant change at 22.1 ± 13.7 and 18.5 ± 11.0 respectively on review at 1 and 2 years (both p > 0.05). 35
What can be deduced from these assessments of pain and functional status is that implant removal may result in improved pain compared to implant retention, as measured by the VAS system, as well as reduced disability scores as quantified by the ODI.
Neurological Status
Seven studies determined that implant removal does not result in adverse neurological outcomes when assessed by the American Spinal Injury Association (ASIA) Impairment Scale or the Frankel Grade. 31-34, 38, 39 28 Aono et al and Toyone et al demonstrated that all patients improved by at least 1 ASIA grade at final follow-up.30, 38 Indeed, Chen et al found that 92% of patients improved at least 1 grade post-operatively. 32 Yang et al affirmed this by showing that 61 of their 64 patients either improved or remained neurologically intact, with 3 pre-existing paraplegic patients unchanged. 39 Only Chou et al quantified the neurological status with the Frankel system, and found a mean improvement of 1.2 grades (0-2) in the removal group versus 1.4 grades (1-2) in the retention group although the statistical significance of this is unclear. 33
Magnetic Resonance Imaging (MRI) Findings
Given the aforementioned radiographic features suggest disc height loss is likely to contribute to the majority of correction loss of the Cobb angle, 2 studies attempted to examine the intervertebral disc with magnetic resonance imaging (MRI).34, 38 Aono et al found that disc degeneration accelerated at least 1 grade in their entire cohort of patients, and correction loss correlated with back pain scores. 34 By the same token, Toyone et al found that upper and lower adjacent discs demonstrated statistically significant degeneration as classified by the Minura system. 38
Complications
The pooled implant removal cohort experienced 14 hardware related complications of 673 patients in total (2.1%) prior to instrumentation removal. A paucity of long-term follow-up precludes accurate evaluation of instrumentation failure over time. However, what is known is that Chou et al observed screw breakages in 8 of their 22 patients in the retention group, while Yang et al also noted 4 additional screw breakages.33, 39 Tellingly, Xu et al reported that 5 of the 8 patients who refused a second operation to remove instrumentation experienced complications necessitating a return to theater anyway. 40
Meta-Analysis: Cobb Angle
Six studies contained extractable data for inclusion in the meta-analysis in the evaluation of the Cobb Angle.30, 32, 33, 35, 36, 38 Importantly, the largest study by Aono et al from 2019 was included given the authors have published 3 studies on the subject with a shared dataset. Similarly, only the larger of the 2 studies published in 2014 by Ko et al was included. 36 Given that the study by Chen et al included only those patients with thoracolumbar burst fractures who sustained a neurological deficit, the data regarding disability and pain on the ODI and VAS respectively was disproportionately inflated and would have skewed the meta-analysis. 28 For this reason, this study was excluded and is instead qualitatively analyzed. On meta-analysis, operative intervention resulted in a significantly improved post-operative Cobb Angle by 16.48 degrees (9.13-23.83, p < 0.01) compared to pre-operative kyphotic deformity (Figure 3). This correction was sustained even after implant removal at final follow-up with an improvement by a mean difference of 9.68 degrees (2.02-17.35, p < 0.01). However, meta-analysis comparing Cobb Angle at time of removal and at final-follow-up did demonstrate a significant loss of correction of 5.82 degrees (3.93-7.71, p < 0.01).
Meta-analysis of sagittal Cobb Angle preoperatively versus postoperatively (A), preoperatively versus final follow-up (B) and at time of removal versus final follow-up (C).
Crucially, 2 studies directly evaluated an implant retention cohort against an implant removal group.33, 35 The implant removal group demonstrated a 10.13 degree (3.00-23.26, p = 0.13) loss of reduction from time of removal versus final follow-up compared to a 10.17 degrees (1.79-22.12, p = 0.10) loss in the implant removal group (Figure 4). By the paired student t-test, there is therefore no statistically significant difference in loss of kyphotic correction between the pooled implant removal and retention groups (p = 0.97).
Meta-analysis of Cobb Angle loss of correction from time of removal versus final follow-up in implant removal cohort (A) and implant retention cohort (B).
Meta-Analysis: Visual Analogue Scale
Two eligible studies reported quantitative data relating to the VAS score (Figure 5).33, 35 In the combined implant removal group, the mean improvement in VAS score was 3.32 (0.18 to 6.45, p = 0.04). Regarding the merged cohort of implant retention patients, there was only a reduction in pain score by 2.50 (-1.81 to 6.81, p = 0.26) which did not attain statistical significant. By the paired t-test, there was a statistically significant difference in back pain as measured by the VAS with a mean difference favoring implant removal over retention of 0.82 (95% CI 0.23 -1.42, p = 0.007).
Meta-analysis of Visual Analogue Scale (VAS) score pre-operatively versus final follow-up in implant removal cohort (A) and implant retention cohort (B).
Meta-Analysis: Oswestry Disability Index
Two studies contained data suitable for meta-analysis regarding the Oswestry Disability Index.29,35 There was a statistically significant improvement in disability at time of implant removal compared to 1 year follow-up by 7.80 points (2.95-12.64), p < 0.01 (Figure 6). This improvement was maintained at final follow-up with an even greater benefit of 11.10 points (5.24-16.96), p < 0.01 (Figure 6).
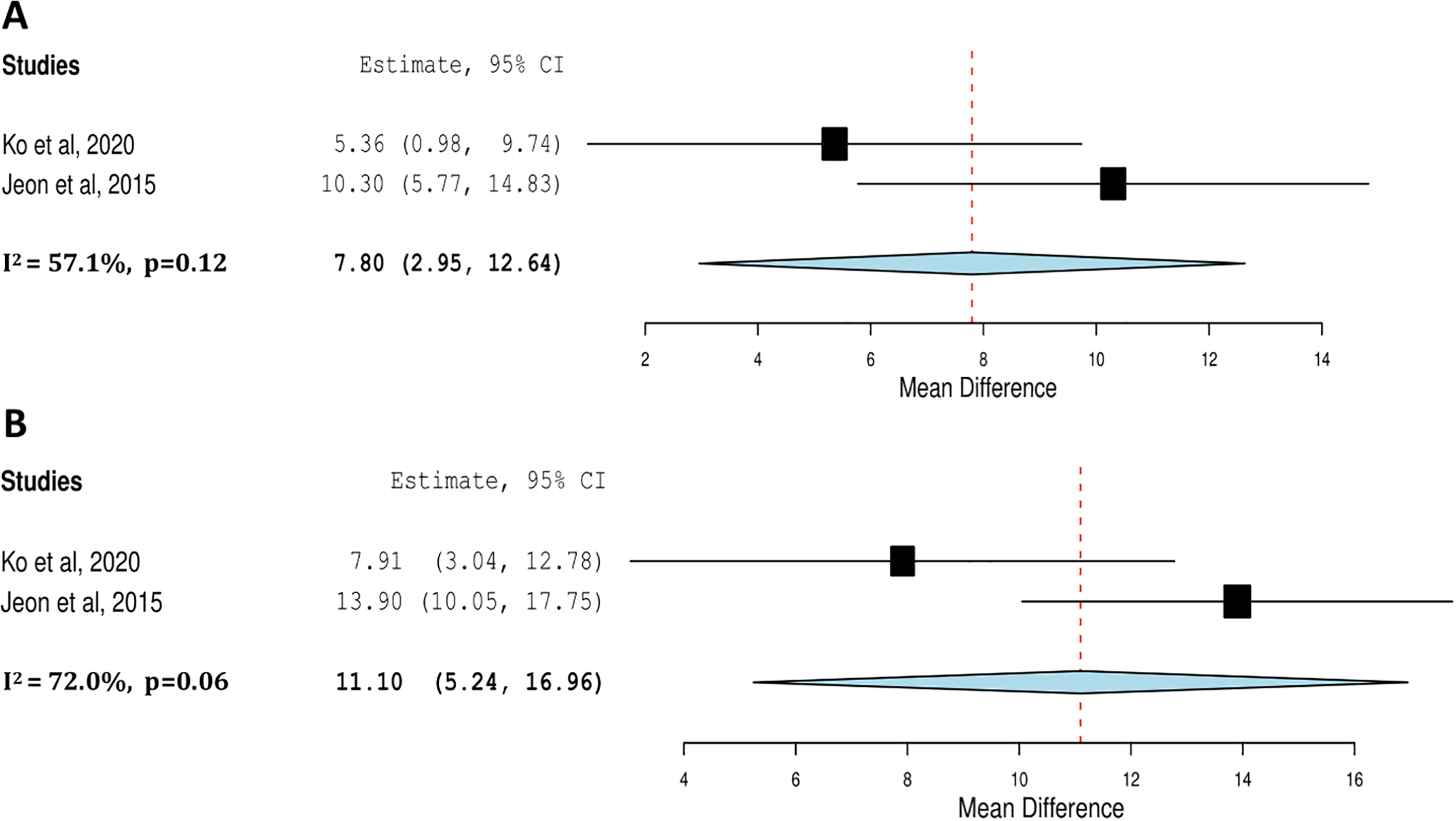
Meta-analysis of Oswestry Disabilty Index (ODI) of function at time of implant removal versus 1 year follow-up (A) and final follow-up (B).
Discussion
We present the first systematic review and meta-analysis which compares the biomechanical and functional outcomes of planned implant removal versus implant retention following surgical fixation of thoracolumbar burst fractures. The principal focus of our review was to evaluate the utility of routine planned implant removal in patients who have undergone surgical fixation without clear symptoms related to their instrumentation.3, 4 On one hand, Deckey et al and Alpert et al argue that the observed kyphotic correction loss that occurs after implant removal is compelling evidence to leave instrumentation in situ.41, 42 This is weighted against the benefits of removing instrumentation and therefore minimizing the risk of failure, breakage, infection and adjacent level disease while restoring segmental range of motion.6-9, 43, 44 Our novel analysis determined that there is no significant difference in decrementing kyphotic correction loss with both instrumentation strategies, yet there appears to be superior functional outcomes with implant removal. This is a notable finding given the routine removal of implants following surgical stabilization with or without arthrodesis has previously remained controversial.3,4,45
It is vital to recognize that our study deliberately excluded the cohort of overtly symptomatic patients, such as those with pain or disability, related to infection or hardware failure. Stavridis et al have already observed markedly improved pain scores following instrumentation removal in these circumstances. 1 This was furthered by Smits et al who demonstrated a subsequent translation into superior quality of life outcomes on longer-term follow-up. 2 Instead, we emphasize our focus upon patients in whom surgical fixation of thoracolumbar burst fractures has occurred and the subsequent removal of implants is a planned event rather than one triggered by significant symptomatic disability.
The anatomical theory underpinning loss of correction over time is explained by the fact that vertebral bodies are composed of an external layer of cortical bone and an inner layer of cancellous bone. 46 Burst fractures are the product of a combination of flexion, axial and rotational forces which lead to compromise of the outer cortical surface and compression of the cancellous surface. 20 As such, this leads to progressive kyphotic deformity and loss of AVH which surgical fixation attempts to combat. Indeed, our meta-analysis of the sagittal Cobb Angle affirms the existing tenet that surgical fixation of thoracolumbar burst fractures results in a significant improvement in kyphotic deformity by 16.48 degrees (9.13-23.83, p < 0.01). This improvement is less marked, yet still maintained at time of implant removal with a pooled correction of 9.68 degrees (2.02-17.35, p < 0.01). The pivotal finding of our meta-analysis was that there is equivalent kyphotic correction loss in sagittal Cobb angle regardless of whether implants were removed (10.13 degrees, 3.00-23.26) or retained (10.17 degrees, 1.79-22.12) at long term final follow-up (p = 0.97).
Furthermore, this kyphotic deformity is likely a consequence of intervertebral disc subsiding into the fractured vertebral body space now newly vacated by compressed cancellous bone. There are 3 pertinent radiographic features which we have previously alluded to in our results section which, when synthesized, support this idea. Firstly, the vertebral body angle (VBA) or vertebral wedge angle (VWA) was found to be preserved without statistically significant loss of correction in 3 studies.30-32, 34 In combination with this, the actual vertebral height was found to be stable by Chou et al and Yang et al.33, 39 Secondly, Xu et al actually reported that the height of the fractured vertebral improves by 30.5% after surgery due to reduced axial compression from gravitational force being relieved by the surgical construct. 40 Finally, Chen et al definitively measured the upper intervertebral angle (UIVA) of the disc space as an independent measure of the vertebral body height and concluded this angle contributed to 90.5% of the Cobb Angle. 32
Consequently, our meta-analysis acknowledges there is loss of correction of Cobb Angle over time. However, given VBA and ABHR remain without significant change while the UIVA markedly decreases, the majority of this loss can likely be attributed to disc height loss. This supposition was supported by magnetic resonance imaging studies performed by Aono et al and Toyone et al, who noted that the disc degeneration was accelerated in burst fractures and this was a relevant corollary of lower back pain scores.34,38 By extension, this is evidence that using kyphotic angle correction losses as a surrogate marker of surgical outcomes may not be the most accurate predictor of kyphosis recurrence. 47 Instead, Aono et al posit that extent of disc destruction predicts kyphosis recurrence while Kim et al identified a load sharing classification score of more than 6 as a significant risk factor of recurrent deformity.30, 47 Wang et al thus suggested that quantification of the vertebral wedge angle, as an indirect marker of disc space collapse, should be the priority and key marker of operative success rather than kyphotic angle. 48
More significant than pure radiological markers is the translation of this effect of implant removal on functional outcomes. Indeed, our review contends that removal of implants intuitively does result in improved segmental motion angle.35,37 In turn, Jeon et al theorized that restoration of segmental motion is likely to explain the pain improvement that Smits et al and Stavridis et al observed following implant removal.1,2 Alanay et al examined implant removal in a cohort of patients who underwent degenerative spine surgery, rather than for thoracolumbar burst fractures, but nonetheless determined an astonishing 84% of their patients experienced a functional improvement following implant removal. 49
Consistent with these findings, our meta-analysis demonstrated that VAS improved by a statistically significant mean of 3.32 points (0.18 to 6.45, p = 0.04) in the removal group, while in the retention group there was a statistically insignificant improvement by 2.50 points (-1.81 to 6.81, p = 0.26). Importantly, this is the first meta-analysis to date that has resulted in pooled data that shows a clear functional superiority of implant removal over retention at final follow-up. A similar positive trend in functional status after implant removal is observed when meta-analysis of the Oswestry Disability Index is performed, with improvement observed at 1 year follow-up after implant removal by 7.80 points (2.95-12.64, p < 0.01). This was sustained on meta-analysis of final follow-up figures, which was more than 10 years in the case of Ko et al, with a soaring functional benefit by 11.10 points (5.24-16.96), p < 0.01. 29 Strikingly, this is likely to not only be of statistical significance but also clinical relevance given the established threshold for a minimal clinically important difference (MCID) with respect to ODI is estimated to lie between 12.4 and 12.8 points.50, 51
This review is timely given a vast array of management options continues to exist for the management of thoracolumbar burst fractures, ranging from conservative management to complex staged anterior-posterior approaches. However, open or percutaneous posterior stabilization with or without arthrodesis has gained increasing popularity.13,17,52 This surgical strategy is often less invasive than an anterior trans-thoracic approach, yet still achieves reduction of kyphotic deformity and anatomical re-alignment of the spine.12,11 It is possible to achieve direct decompression of canal stenosis and removal of displaced retropulsed bone fragments, as well as indirect reduction by ligamentotaxis.29,53 With appropriate patient selection guided by McCormack’s triple pronged load-sharing classification system, Parker et al found great success in repairing thoracolumbar burst fractures with posterior fixation alone.54, 55 There is also emerging evidence that there is no significant difference in kyphotic correction losses or final kyphotic angle between instrumentation with or without arthrodesis.12-14 The fact that the majority of studies in our review elected to perform surgical stabilization without fusion is telling and possibly foreshadows future trends in spine trauma management.28-36,38-40,47
In light of our novel findings, we advocate for planned removal of posterior spinal instrumentation given the superior functional outcomes compared to implant retention yet similar decrementing correction losses compared to implant retention. It is also noteworthy that in both studies by Chou et al and Jeon et al who compared implant removal versus retention cohorts, the final kyphotic angle eventually almost regressed to the pre-operative kyphotic angle regardless of whether implantation occurred or fusion was performed.33,35 Absolute predictors of implant failure are still unknown, although factors such as osteoporosis and smoking as well as vertebral fracture morphology have been studied.56,57 A final consideration when evaluating the utility of implant removal is the morbidity itself associated with undergoing an additional procedure. Peri-operative risk varies on an individual basis, but this further adds complexity to the joint clinical decision between surgeon and patient. What our review suggests is that in younger patients who sustain thoracolumbar burst fractures which undergo surgical stabilization, planned implant removal in a delayed fashion results in similar correction losses with significant benefits of improved quality of life and superior functional outcomes without fear of future instrumentation failure or complication.
The strengths of our study were 3-fold. An exhaustive search yielded an international and comprehensive systematic review and meta-analysis of the available literature on implant removal after posterior fixation of thoracolumbar burst fractures. This lends a high degree of external validity and applicability. Additionally, shared radiographic and functional outcome measures among included studies enabled a meta-analysis to be performed and provide pooled results. Finally, the quality of all the included studies was moderate to high with generally low risk of bias on evaluation by the ROBINS-I risk of bias tool conferring a reasonable sense of internal validity. Our stringent criteria minimized selection bias from skewering our results given we demanded studies to declare that implant removal was a planned prospective decision to be routinely performed in patients.
Unfortunately, our study was limited by the paucity of available direct comparative data between implant retention and removal cohorts. There were only 2 studies which specifically followed-up both retention and removal groups with respect to radiographic correction loss and functional performance. The majority of our studies also examined patients who underwent stabilization without fusion, and while there is increasing evidence that arthrodesis is not necessary in this particular subgroup, the role of implant removal in the cohort who does undergo arthrodesis still requires specific clarification. An absence of randomized controlled evidence in this area also reduced the overall quality of the analysis, but we acknowledge that the fact that implant removal requires a second operation means a control arm may encounter difficulty in effective blinding of participants. Inevitably, this may have resulted in an inherent performance bias due to the unblinded nature of both participants and researchers in all of our included trials.
Conclusion
In younger patients who sustain thoracolumbar burst fractures requiring posterior surgical fixation, routine planned posterior implant removal results in improved quality of life without any significant difference in decrementing kyphotic correction loss compared to implant retention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.