
Abstract
Study Design:
A multicenter, retrospective review of C5 palsy after cervical spine surgery.
Objective:
Postoperative C5 palsy is a known complication of cervical decompressive spinal surgery. The goal of this study was to review the incidence, patient characteristics, and outcome of C5 palsy in patients undergoing cervical spine surgery.
Methods:
We conducted a multicenter, retrospective review of 13 946 patients across 21 centers who received cervical spine surgery (levels C2 to C7) between January 1, 2005, and December 31, 2011, inclusive. P values were calculated using 2-sample t test for continuous variables and χ2 tests or Fisher exact tests for categorical variables.
Results:
Of the 13 946 cases reviewed, 59 patients experienced a postoperative C5 palsy. The incidence rate across the 21 sites ranged from 0% to 2.5%. At most recent follow-up, 32 patients reported complete resolution of symptoms (54.2%), 15 had symptoms resolve with residual effects (25.4%), 10 patients did not recover (17.0%), and 2 were lost to follow-up (3.4%).
Conclusion:
C5 palsy occurred in all surgical approaches and across a variety of diagnoses. The majority of patients had full recovery or recovery with residual effects. This study represents the largest series of North American patients reviewed to date.
Introduction
Postoperative C5 palsy is a known complication of cervical decompressive spinal surgery. The incidence of this complication has been reported to be between 0% and 30% depending on procedure type and approach. 1 -36 Patients commonly present with new weakness in the deltoid and/or biceps brachii, sensory deficits, and/or pain in the shoulders, and dissatisfaction with surgery.* C5 palsy may present immediately after surgery or up to 2 months postoperatively † and can negatively affect postoperative quality of life in the short term. 14,35 The prognosis is usually good, although recovery time can vary depending on the severity of the deficit. ‡
The goal of this study was to review the incidence, patient characteristics, and outcome of C5 palsy in a large, multicenter retrospective review of cervical spine surgeries. Previous studies of C5 palsy have largely been limited to single-surgeon, single-institution studies with a relatively small number of cases to investigate. Our study marks the largest known study of postoperative C5 palsy to date.
Materials and Methods
We have conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. Medical records for 13 946 patients who received cervical spine surgery (levels from C2 to C7) between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation requiring evacuation, esophageal perforation, epidural hematoma, C5 palsy, recurrent laryngeal nerve palsy, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring reoperation, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, quadriplegia, intraoperative death, revision of arthroplasty and, pseudomeningocele. Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the list. Data was transcribed into study-specific paper case report forms. Copies of case report forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning, and data entry.
The results were presented as mean (standard deviation) and number (%) for continuous and categorical variables, respectively. P values were calculated using 2-sample t test for continuous variables and χ2 tests or Fisher exact tests for categorical variables. A P value less than .05 denoted significant differences. Statistical analyses were performed using SAS, version 9.4 (SAS, Cary, NC).
Results
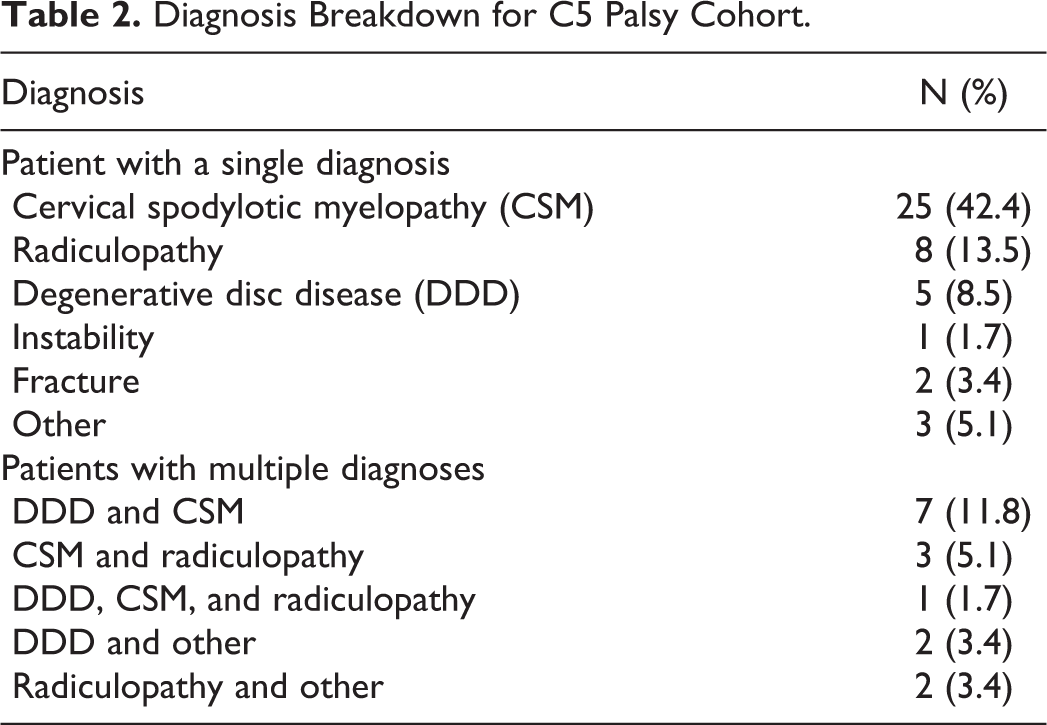
Of the 13 946 cases reviewed, 59 patients experienced a postoperative C5 palsy. The overall incidence rate was 0.41%, with rates across the 21 sites ranging from 0% to 2.5%. Table 1 shows the incidence rates by procedure type. There were 37 males (62.7%), and mean age was 60.9 ± 13.1 years. Mean height was 169.5 ± 13.2 cm, and mean weight was 83.8 ± 19.6 kg. Preoperative diagnoses are listed in Table 2. Of the 59 patients, 28 reported reoperation and postoperative Nurick scores (1.933 ± 1.23 and 0.893 ± 1.23, respectively). Nurick scores improved significantly (P < .001) after surgery. Mean number of levels treated was 4.5 ± 1.2, blood loss was 388.49 ± 6578.5 mL, and operative time was 210.3 ± 109.6 minutes. Grafting was used in 49 (83.1%) cases.
Incidence Rates by Procedure Typea.
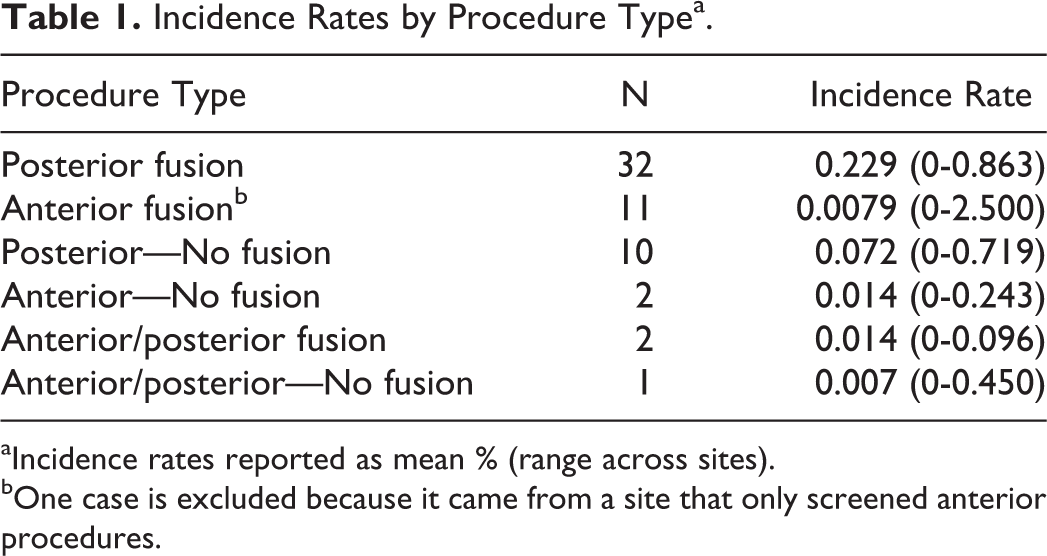
aIncidence rates reported as mean % (range across sites).
bOne case is excluded because it came from a site that only screened anterior procedures.
Diagnosis Breakdown for C5 Palsy Cohort.
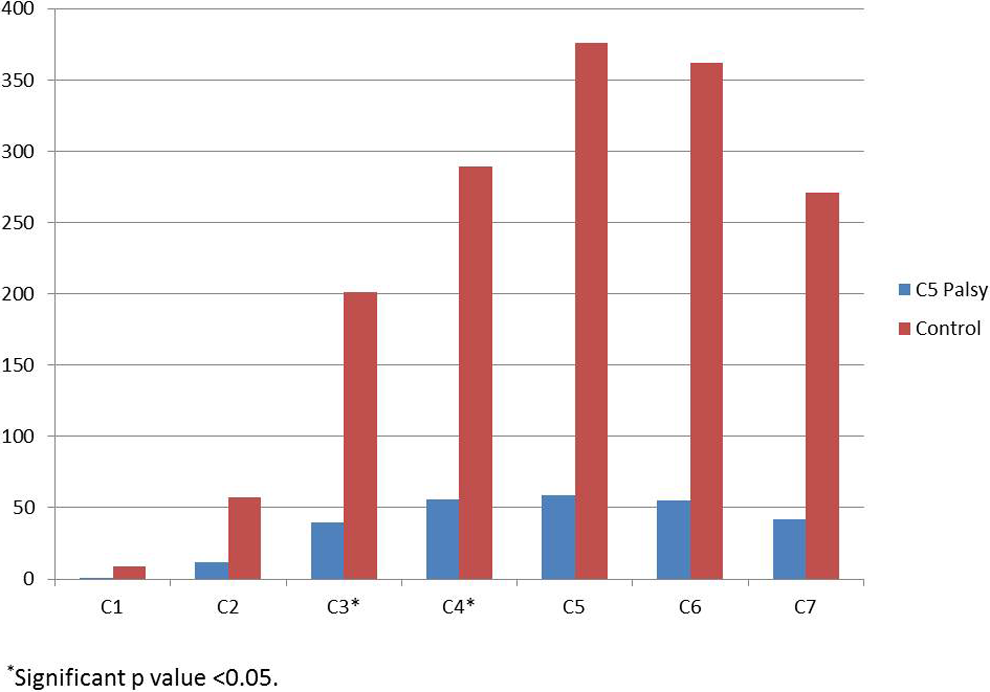
The time of initial onset of C5 palsy symptoms was reported for 54 of the 59 C5 palsy patients and ranged from immediately postoperative to 14 days postoperative (Figure 1). There were 29 cases delayed onset (>24 hours post-operative) C5 palsy.
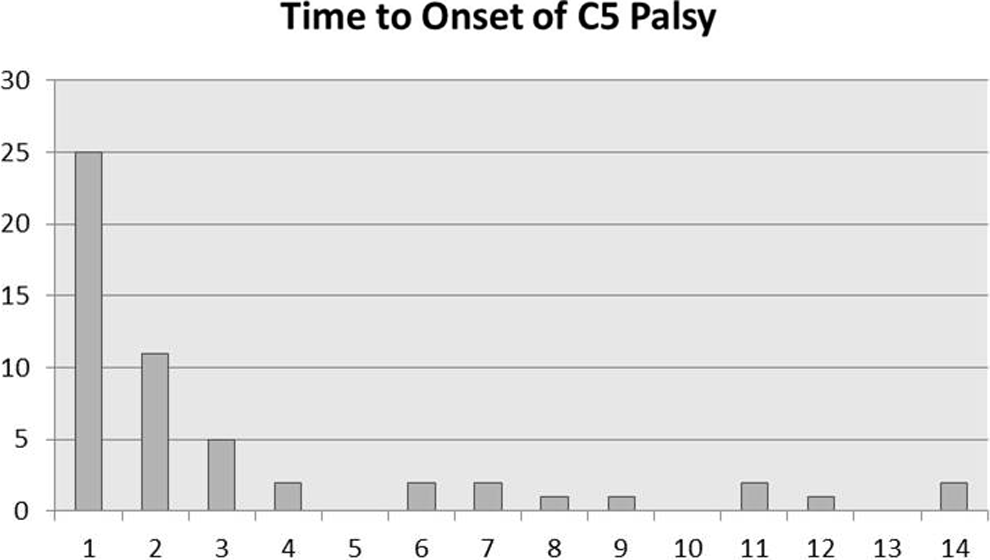
Time to onset of C5 palsy for 54 of the 59 patients studied. The x-axis is the time in days from procedure to onset of C5 palsy symptoms, and the y-axis is the number of patients experiencing the onset of C5 palsy at that given day.
Treatment and Outcome
Of the 59 patients with postoperative C5 palsy, 30 patients (50.8%) received no treatment, 9 underwent physical therapy (15.3%), 3 underwent an additional surgical procedure (5.1%), and 17 underwent additional conservative treatment (28.8%). Of the 3 undergoing additional surgical procedures, one underwent an Oberlin nerve transfer, one underwent revision of instrumentation and exploration of C5 root, and one underwent 3 additional procedures to address wound issues as well as revision C4-5 foraminotomies and decompression of the nerve root. At most recent follow-up, 32 patients reported complete resolution of symptoms (54.2%), 15 had symptoms resolve with residual effects (25.4%), 10 patients did not recover (17.0%), and 2 were lost to follow-up (3.4%). Time to recovery was reported for 27 patients and ranged from 1 month to 1.5 years (Figure 2).
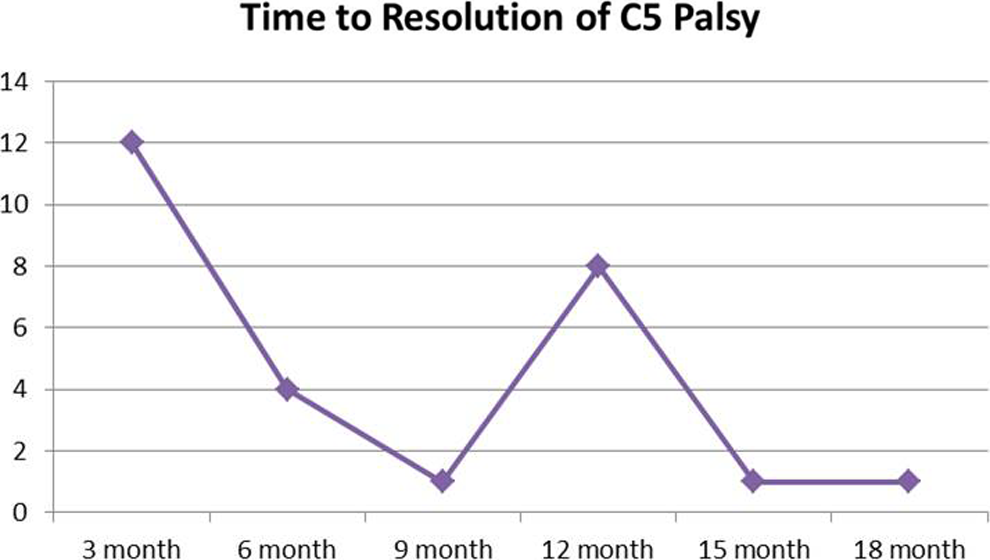
Time to resolution of C5 palsy for 27 of the 59 patients studied by 3-month intervals.
Figure 3 shows representative imaging of a 58-year-old right-handed male with progressive symptoms of cervical myelopathy and mid-subaxial compression as seen on T2 magnetic resonance imaging (A and B). He underwent a posterior C4-7 decompression and C3-T1 instrumented fusion (C and D). The patient went on to develop a bilateral C5 palsy on postoperative day 2 with sensory loss and a manual muscle test (MMT) of 1/5 in the deltoid. Postoperative imaging (E and F) showed no evidence of compression despite the patient’s symptoms. He made a full recovery after 8 months with physical therapy.
A 58-year-old male with symptomatic mid-subaxial compression as seen on T2 MRI (A and B) underwent cervical laminectomy and cervicothoracic fixation (C and D). He developed a bilateral isolated C5 palsy day 2 after surgery. Postoperative imaging showed no compression (E and F). The patient recovered after 8 months with physical therapy.
Discussion
C5 palsy after cervical spine surgery is a challenging postoperative complication to study. Inconsistencies in the definition of C5 palsy throughout the literature may result in varying results. The most widely accepted definition defines C5 as a motor paresis of the deltoid muscle and/or the biceps brachii muscle of more than one grade after cervical decompression surgery without any associated deterioration of myelopathic symptoms. 6,19,29 Bydon et al defined C5 palsy as a motor decline of the deltoid muscle function by at least 1 level in a standard MMT within the 6-week postoperative period. 33 Eskander et al defined it as MMT score of ≤3 on a scale of 5. 28 Hasegawa et al defined C5 palsy as deterioration of motor function by at least 1 level in a standard MMT of the deltoid and/or bicep without aggravation of lower extremity function, the appearance of a new sensory disturbance between postoperative day 0 and 2 months after surgery, or both deterioration of motor function and the appearance of a new sensory disturbance. 23
Previous studies have attempted to identify risk factors for the development of postoperative C5 palsy. Preoperative diagnosis may have an impact on the development of C5 palsy. Kalisvaart et al reported incident ranges of 2.8% to 12.1% in patients with cervical spodylotic myelopathy (CSM), 2.1% to 14% in those with ossification of the posterior longitudinal ligament (OPLL), and 0% to 3% in patients with cervical disc herniation. 19 OPLL has been reported to be a risk factor for developing postoperative C5 palsy.* Nakashima et al, Nakamae et al, and Wu et al all reported a greater risk of developing C5 palsy in OPLL patients those than patients with CSM, 1,12,13 with Wu et al finding 9.2-fold greater risk in OPLL patients. A preoperative diagnosis of CSM has also been linked with higher incidences of postoperative C5 palsy than those patients with degenerative disease or radiculopathy. † In a study of 134 patients undergoing anterior decompression and fusion, Kim et al reported an overall incidence of 4.3%. In that study, C5 palsy did not occur in the 30 patients with radiculopathy; excluding these patients, the rate of C5 palsy rose to 5.8% for CSM patients. 17 In our study, 64.4% of C5 palsy cases had preoperative diagnoses of CSM, with 25.4% having degenerative disc disease and 23.7% having radiculopathy. The incidence of OPLL was not documented.
The type of procedure performed may also affect the risk of developing C5 palsy. In a review of 1001 anterior and posterior cervical decompressions, Bydon et al reported an overall C5 palsy rate of 5.2%, with a 1.6% rate in anterior procedures and 8.6% in posterior procedures. 33 Procedures involving internal fixation have been linked with higher rates of C5 palsy. 4,15,32 Takemitsu et al reported the risk of developing C5 palsy to be 11.6 times greater in patients undergoing laminoplasty with posterior instrumentation versus laminoplasty alone. 4 In patients with severe OPLL, Chet et al reported an 8% incidence rate in patients undergoing laminoplasty, while patients undergoing laminectomy and fusion had a C5 palsy rate of 14%; patients undergoing anterior corpectomy did not report any cases of C5 palsy. 32 Nassr et al looked at C5 palsy rates across 4 different procedure types (laminoplasty, laminectomy and fusion, anterior corpectomy, and circumferential). 11 Although no significant differences in C5 palsy incidence were reported, the authors hypothesized that the study was underpowered to detect a significant difference and that the trend was toward higher rates with laminectomy and fusion. 11 In our study, 42 of the 59 C5 palsy cases (71.2%) occurred after a posterior-only procedure, with 32 of those 42 cases involving spinal fusion (Table 1).
Even within a particular procedure type there is a high degree of variability in C5 palsy rates. Duetzmann et al performed a systematic review of the literature of cervical laminoplasty and found that 16% of the studies reported a C5 palsy rate of >10%, 41% of studies reported a rate of 5% to 10%, 23% of studies reported a rate of 1% to 5%, and 12.5% reported a rate of 0%. 40
Treatment and Outcome
There is no standardized treatment for C5 palsy, 6,29,31,35 and cases of C5 frequently resolve spontaneously without treatment. 20,23,29 If treatment is prescribed, physical therapy, pain management, or other conservative methods are typically used.*
Foraminotomy has been proposed to treat patients with C5 palsy, either prophylactically † or as a subsequent operative treatment. 12,17,20,39 In a study of patients undergoing expansive laminoplasty, Komagata et al found that patients who underwent bilateral partial foraminotomy showed significantly lower incidences of palsy (0.6% vs 4.0%) than those who did not. 16 Hojo et al recommended prophylactic foraminotomies at C4-5 if there are findings of foraminal stenosis on preoperative computed tomography. 21 Nakashima et al reported 10 cases of C5 palsy after cervical posterior fusion, 4 of which underwent subsequent foraminotomies at C4-5. 12 Of these cases, 3 improved by ≥2 MMT, while the fourth case showed minimal improvement.
However, the use of prophylactic foraminotomy remains controversial 11,19,43 as there is an increased risk of nerve damage with an additional foraminotomy being performed. Bydon et al found that C4-5 foraminotomy was actually strongly correlated to the development of C5 palsy. 33 Katsumi et al found that while prophylactic foraminotomy decreased the rate of C5 palsy, it did not eliminate it completely. 18 Additional research is needed to determine the effectiveness of this technique in preventing C5 palsy.
Time to recovery from C5 palsy is likely related to the severity of the deficit. ‡ In a review of published cases, Sakaura found that 47.8% of mild palsy cases resolved in less than 3 months; however, 52% of severe cases took up to 6 months to recover. 6 Nassr et al reviewed 750 consecutive multilevel cervical decompression procedures and found that time to improvement ranged from 1 to 104 weeks with an average of 20.9 weeks. 11 In that study, 71.4% of patients reached maximal improvement within 6 months; however, 19.1% of patients had some residual deficit at final follow-up. 11 Imagama et al reviewed 1858 patients undergoing cervical laminoplasty for chronic compression myelopathy and reported complete recovery in 67% of patients and residual deficit in 33%. 43 Kim et al reviewed 134 cases of anterior cervical decompression and fusion for cervical degenerative disc disease with a time to improvement range of 2 to 6 months, with one patient having no resolution of C5 palsy. 17 More than half of the C5 palsy patients in our study reported complete resolution of symptoms, although 15 had residual effects and another 10 did not recover.
Limitations
Data with regard to the 13 887 patients without C5 palsy was limited to procedure type only; as such, we were unable to provide incidence rates by diagnosis, age, or other related parameters. This study was a retrospective review, and as such the authors were limited by the availability of the data in the medical record. C5 palsy cases, especially subtle deficits, may not have been adequately documented in the medical record. The most common definition of C5 palsy is a motor decline of the deltoid muscle function by at least 1 level in a standard muscle test 33 ; oftentimes factors such as pain limitation, incomplete documentation, and early improvement in deficits may allow deficits to be missed. Furthermore, sensory deficits in this distribution may often be misdiagnosed.
In this study we evaluated all cervical operations, many of which were for radiculopathy and not myelopathy, anterior operations, fusions without decompression (eg, pseudoarthroses, deformity correction, C1-2 fusions), procedures for trauma, metastatic disease, and infection, as well as procedures that often did not involve the C4-5 level. Given that many of these operations are less likely to lead to C5 palsy (in contrast to the diagnosis of OPLL or severe CSM), this may explain why our incidence is lower than reported in the literature. However, our results may reflect a more accurate rate of C5 palsy across all cervical procedure types and the true C5 palsy incidence may in fact be lower than previously reported.
Conclusion
C5 palsy is a known postoperative complication of cervical spine surgery. In this study, we reviewed 13 946 cervical spine operations and found the incidence to be 0.41%, with a range from 0% to 2.5% across all sites. C5 palsy occurred in all surgical approaches and across a variety of diagnoses. The majority of patients had full recovery or recovery with residual effects. This study represents the largest series of North American patients reviewed to date. Future prospective studies will provide additional insight into the prevention, treatment, and outcome of patients with C5 palsy.
Footnotes
Authors’ Note
This study was ethically approved by the institutional ethics committees at all participating sites.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sara E. Thompson reports grants from AOSpine North America during the conduct of the study; Zachary A. Smith reports grants from AOSpine North America during the conduct of the study; Wellington K. Hsu reports grants from AOSpine North America during the conduct of the study, personal fees from Medtronic, personal fees from Stryker, personal fees from Bacterin, personal fees from Graftys, personal fees from Ceramtec, personal fees from Relievant, personal fees from Bioventus, personal fees from Globus, personal fees from SpineSmith, outside the submitted work; Ahmad Nassr reports grants from AOSpine North America during the conduct of the study; Thomas E. Mroz reports other from AOSpine, grants from AOSpine North America during the conduct of the study, personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; David E. Fish reports grants from AOSpine North America during the conduct of the study; Jeffrey C. Wang reports grants from AOSpine North America during the conduct of the study; Michael G. Fehlings reports grants from AOSpine North America during the conduct of the study; Chadi A. Tannoury reports grants from AOSpine North America during the conduct of the study; Tony Tannoury reports grants from AOSpine North America during the conduct of the study; P. Justin Tortolani reports grants from AOSpine North America during the conduct of the study, other from Globus Medical, grants from Spineology, other from Innovasis, outside the submitted work, and in addition, Dr. Tortolani has a patent Globus with royalties paid; Vincent C. Traynelis reports grants from AOSpine North America during the conduct of the study, and Medtronic – Royalties, Consultant Globus – Institutional Fellowship Support; Ziya Gokaslan reports grants from AOSpine North America during the conduct of the study, grants from AOSpine North America, personal fees from AO Foundation, grants from AOSpine, outside the submitted work; Alan S. Hilibrand reports grants from AOSpine North America during the conduct of the study, other from Amedica, Vertiflex, Benvenue, Lifespine, Paradigm Spine, PSD, Spinal Ventures, outside the submitted work, and in addition, Dr. Hilibrand has a patent Aesculap, Amedica, Biomet, Stryker, Alphatec, with royalties paid; Robert E. Isaacs reports grants from AOSpine North America during the conduct of the study, grants and personal fees from NuVasive, Inc., personal fees from Association for Collaborative Spine research, outside the submitted work; Praveen V. Mummaneni reports grants from AOSpine North America during the conduct of the study, other from Deputy Spine, grants and other from AOSpine, other from Globus, other from Springer Publishers, other from Thieme Publishers, other from Taylor and Francis Publishers, other from Spincity/ISD, outside the submitted work; Dean Chou reports grants from AOSpine North America during the conduct of the study, other from Globus, other from Medtronic, other from Orthofix, outside the submitted work; Sheeraz A. Qureshi reports grants from AOSpine North America during the conduct of the study, and is a consultant and receives royalties from Stryker Spine, Biomet Spine, and RTI; Evan O. Baird reports grants from AOSpine North America during the conduct of the study; Zorica Buser reports grants from AOSpine North America during the conduct of the study; Michelle J. Clarke reports grants from AOSpine North America during the conduct of the study; Adeeb Derakhshan reports grants from AOSpine North America during the conduct of the study; Elizabeth L. Lord reports grants from AOSpine North America during the conduct of the study; Eric M. Massicotte reports grants from AOSpine North America during the conduct of the study, grants from Medtronic, Depuy-Synthes Spine Canada, personal fees from Watermark consulting, grants from AOSpine North America, nonfinancial support from AOSpine North America, outside the submitted work; Michael P. Steinmetz reports grants from AOSpine North America during the conduct of the study; Jonathan Pace reports grants from AOSpine North America during the conduct of the study; Peter I. Cha reports grants from AOSpine North America during the conduct of the study; Erica L. Gee reports grants from AOSpine North America during the conduct of the study; D. Alex Stroh reports grants from AOSpine North America during the conduct of the study; Khoi D. Than reports grants from AOSpine North America during the conduct of the study; and K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plantiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work; Samuel K. Cho reports grants from AOSpine North America during the conduct of the study; grants from OREF, personal fees from Stryker, from Medtronic, personal fees from DePuy Synthes, outside the submitted work; Rick C. Sasso reports grants from AOSpine North America during the conduct of the study; personal fees from medtronic, grants from medtronic, grants from K2, outside the submitted work; Paul M. Arnold reports grants from AOSpine North America during the conduct of the study; other from Z-Plasty, other from Medtronic Sofamore Danek, other from Stryker Spine, other from FzioMed, other from AOSpine North America, other from Life Spine, other from Integra Life, other from Spine Wave, other from MIEMS, other from Cerapedics, other from AOSpine North America, outside the submitted work; Mohamad Bydon reports grants from AOSpine North America during the conduct of the study; Anthony F. De Giacomo reports grants from AOSpine North America during the conduct of the study; Bruce Jobse reports grants from AOSpine North America during the conduct of the study; Daniel Lubelski reports grants from AOSpine North America during the conduct of the study; Mark Corriveau reports grants from AOSNA during the conduct of the study; Sungho Lee reports grants from AOSpine North America during the conduct of the study; Dhananjay Chatterjee reports grants from AOSpine North America during the conduct of the study; Erik N. Mayer reports grants from AOSpine North America during the conduct of the study; Owen J. McBride reports grants from AOSpine North America during the conduct of the study; Allison K. Roe reports grants from AOSpine North America during the conduct of the study; Marisa Y. Yanez reports grants from AOSpine North America during the conduct of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc, a 501(c)3 nonprofit corporation.