
Abstract
Background:
Intensive care unit (ICU) nurses are enduring unprecedented burden caring for COVID-19 patients. Few studies have reported types of work-related events that lead to occupational stress and post-traumatic stress disorder (PTSD).
Methods:
ICU nurses were recruited at an academic health science center to explore their experiences of caring for COVID-19 patients. Participants were interviewed for 1 hour using open-ended questions. Symptoms of PTSD were assessed using the PTSD Checklist, job satisfaction with a Likert-type scale, and intention to leave their job with a “yes or no” question. Semi-structured interviews were transcribed and analyzed using NVivo software; quantitative data were analyzed using frequencies and means with R 4.0.5.
Findings:
The ICU nurse sample comprised nine females and one male, all Caucasian, with a mean age of 26.6 years. Analysis of interview transcripts revealed six recurring themes: Change in Practice, Emotion, Patient’s Family, Isolation, Job Satisfaction, and Public Reaction. Quantitative findings revealed 7 of 10 met diagnostic criteria for PTSD. Most participants (7/10) were “somewhat satisfied” with their job. Five of 10 considered leaving their job in the last 6 months.
Conclusion/Implications for Practice:
Understanding the impact stressful pandemic-related patient care has on ICU nurses provides evidence that new policies are needed. Furthermore, qualitative findings provide insight into the best design and deployment of interventions to reduce stress and prevent development of PTSD. More research is needed to understand long-term effects of PTSD and to evaluate strategies to prevent PTSD during stressful emergency surges in intensive care.
Background
Intensive care unit (ICU) nurses are frontline workers, caring for the most critically ill patients. Due to their extreme level of responsibility and cumulative exposure to psychological stress and trauma, they are at high risk for developing post-traumatic stress disorder (PTSD; Levi et al., 2021; Salmon & Morehead, 2019). Schuster and Dwyer’s (2020) integrative review of 24 pre-COVID studies reported that 8.5% to 20.8% of registered nurses met the criteria for PTSD. The American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders (5th ed., DSM-5) ascertains that PTSD can develop after individuals experience a traumatic event (or cumulative episodes) causing considerable distress or impairment lasting longer than 1 month. The DSM-5 (American Psychiatric Association, 2013) identifies four symptom clusters of PTSD: (a) intrusive and recurring memories of the traumatic event(s), (b) avoidance of similar situations or reminders of the traumatic event(s), (c) negative changes in cognition and mood, and (d) hyperarousal and exaggerated startle response.
During the COVID-19 pandemic the literature has shown that some ICU nurses have suffered physical (e.g., sleep disturbances, headaches) and psychological symptoms (e.g., anxiety, depression, and in severe cases, suicidal contemplations) while caring for COVID-19 patients (Shen et al., 2020; Tan et al., 2020; Yifan et al., 2020). However, a gap exists in the literature on the types of work-related events that ICU nurses caring for COVID-19 patients’ experience that result in psychological distress and the impact this has on their health. This study aimed to investigate the lived experiences of ICU nurses caring for COVID-19 patients to understand and describe the stressful experiences and determine whether these experiences impacted their mental health and attitudes toward their careers.
Methods
A phenomenological methodology was selected as the most appropriate to investigate the lived experiences of ICU nurses caring for COVID-19 patients. A phenomenological approach can capture an in-depth analysis through textural (the ICU nurses’ perceptions) and structural descriptions (how they experienced the phenomenon) to “convey the overall essence of their lived experiences” (Creswell & Poth, 2018). Through the sharing of stories, a complex and detailed understanding of the phenomenon can be revealed (Creswell & Poth, 2018). Colaizzi’s (1978) procedural framework was used for the qualitative analysis. Questionnaires were administered by the principal investigator (PI) to obtain demographic information and to assess for PTSD, job satisfaction, and intention to leave their job.
Sample and Setting
A convenience sample of 10 ICU nurses caring for COVID-19 patients was recruited at an academic health science center in the southeastern United States within the period of August 10, 2020 to September 13, 2020. Recruitment techniques to incorporate a diverse sample of participants included visits to the unit to explain the study purpose and relay that all perspectives are valuable and needed. Snowballing, a recruitment method in which participants are asked to assist in identifying other potential participants (Sadler et al., 2010), was also employed. Inclusion requirements included that participants were currently caring for COVID-19 patients admitted to the ICU, at least 21 years old, and employed at the academic health science center for at least 6 months as an ICU nurse. Participants of all genders, races, and ethnicities were sought. Exclusion criteria consisted of ICU nurses who were unable or unwilling to meet for an audiotaped telephone interview for 60 minutes. Ethics approval for this research was obtained from a university institutional review board. Interviews were conducted over the telephone due to viral transmission precautions. Verbal informed consent was given by all participants prior to interviews. Participants were informed that they had the right to withdraw from the study at any time.
Data Collection
Due to COVID-19 social distancing guidelines, semi-structured interviews were conducted via audiotaped telephone calls to minimize risk of COVID-19 transmission. The principal investigator (PI) conducted the semi-structured telephone interviews in a private room with a closed door. To reduce burden of study participation, participants were able to choose the time and date to be interviewed. Most participants shared their experiences from the privacy of their home, enhancing confidentiality. Sociodemographic information included age (in years), gender (male/female), ethnicity (Caucasian, African American, Latinx or Hispanic, Asian, Native American, Other), marital status (single, married or domestic partnership, widowed, divorced, separated), level of education (categories bachelor’s degree, licensed practical nurse, associate degree, master’s degree), years employed as an ICU nurse, and years at current position.
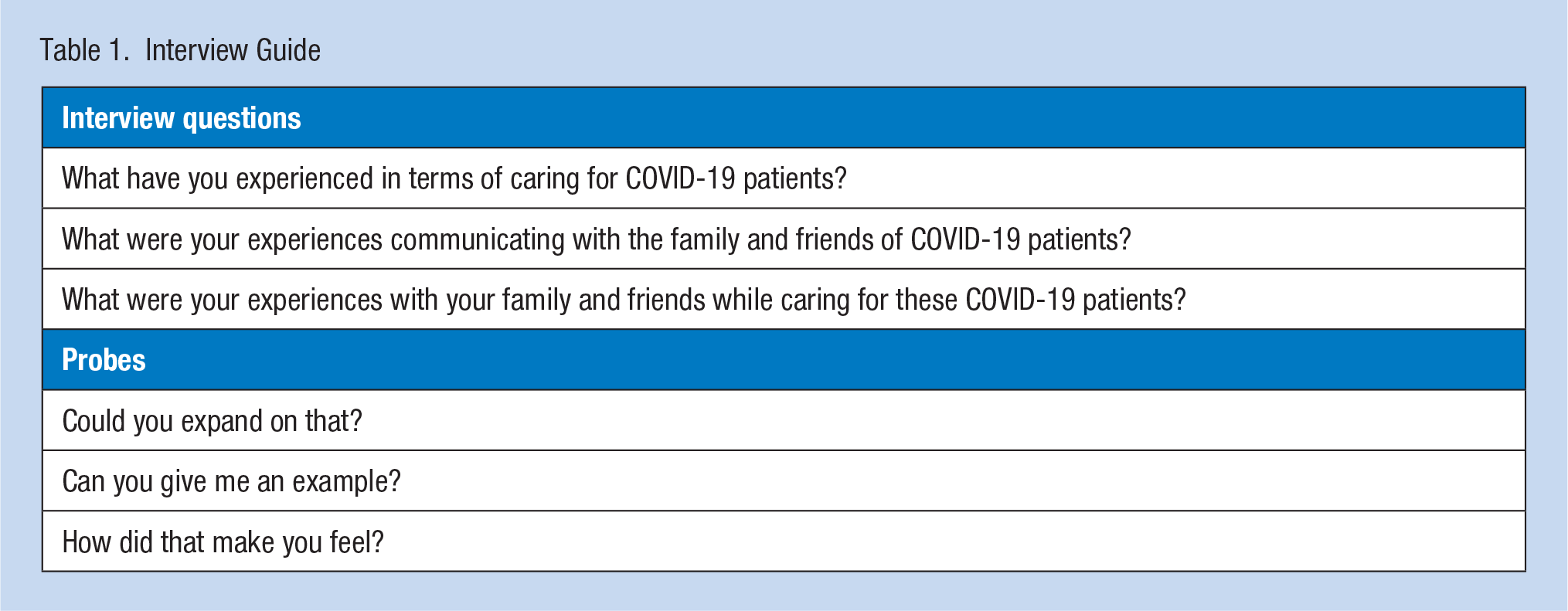
Following the tradition of phenomenology, open-ended questions were designed to explore the ICU nurses’ experiences, perceptions, thoughts, and feelings (Creswell & Poth, 2018). The questions asked about the ICU nurses’ experiences of caring for COVID-19 patients, experiences with the patients’ family members and friends, and experiences with their own families (Table 1). To gain thick, rich descriptions and reveal the underlying meaning behind their experiences, participants were encouraged to talk freely. Most importantly, and guided by the philosophy of phenomenology, the PI did not lead the participant or influence their response (Creswell & Clark, 2017).
Interview Guide
Participant interviews lasted approximately 1 hour (ranging from 47 to 70 minutes). A journal was used to reflect on thoughts that arose during the interviews. When redundancy of data from the group of participants was reached, recruitment concluded. The data were de-identified to protect confidentiality and identity of participants. Electronic data were stored on a password-protected computer, encrypted in OneDrive on the academic health science center’s server network, with only the unique identifier assigned to each participant. Other data included observations (e.g., crying, voices cracking with emotion, laughing) on the audio recordings and reflection notes.
Data Analysis
Interviews were transcribed verbatim within 24 hours of each audiotaped interview. Colaizzi’s (1978) seven-step method of qualitative data analysis was chosen to enhance credibility and trustworthiness in data collection and analysis. QSR International’s NVivo 12 (Victoria, Australia) qualitative data analysis software was used to analyze interview transcriptions. To promote trustworthiness, the PI and second author attempted to bracket any prior knowledge and beliefs about the phenomenon, acknowledging their ICU nursing experience.
Following Colaizzi’s (1978) steps, transcripts were repeatedly reviewed to become familiar with the core meaning. In the second step, significant statements were extracted from each transcript. The third step involved generating statements into codes and formulating meanings from codes. In the fourth step, formulated meanings of similar codes were organized into themes. Step 5 involved the integration of the coded statements into an exhaustive description of the phenomenon to gain conceptual understanding. Data analysis was performed alongside data collection to recognize when data saturation had been accomplished. Step 6 entailed identifying the fundamental structure of the phenomenon of the lived experience of ICU nurses caring for COVID-19 patients. Finally, in Step 7, findings were validated with participants to enhance rigor.
When code categories were firmly established, the PI and second author independently carried out analyses on the same data to establish reliability of coding (kappa coefficient = 0.89). Additional strategies to establish credibility and trustworthiness included generating thick, rich description, clarifying researcher biases from the onset, prolonged engagement in data collection, and member-checking to ensure participants’ meanings and perspectives were represented rather than the PI’s (Lincoln & Guba, 1985). Reliability of coding was accomplished through the use of two coders to analyze transcript data. Finally, to ensure trustworthiness and dependability of the research, an ongoing audit trail tracked the process of research, how decisions were made, and the procedure of conducting intercoder agreement checks (Lincoln & Guba, 1985).
Results
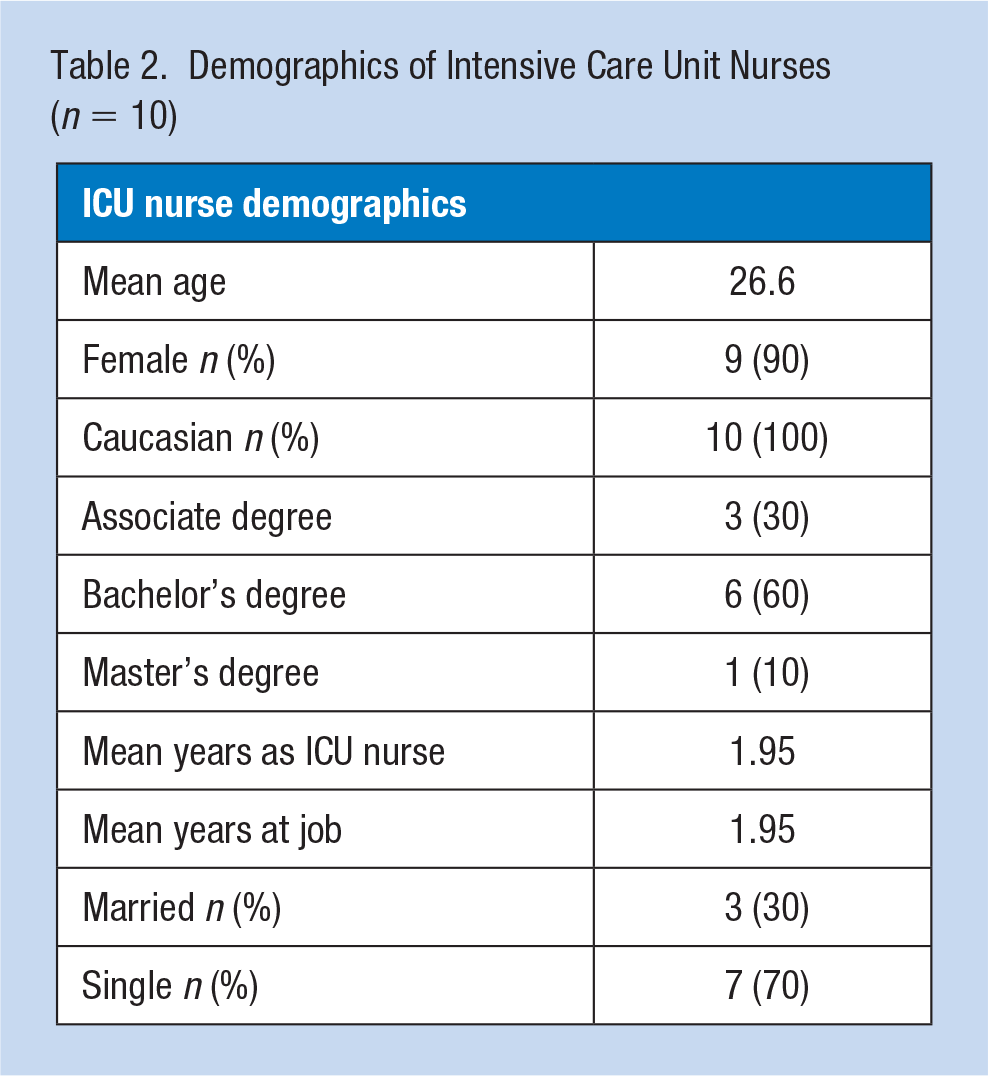
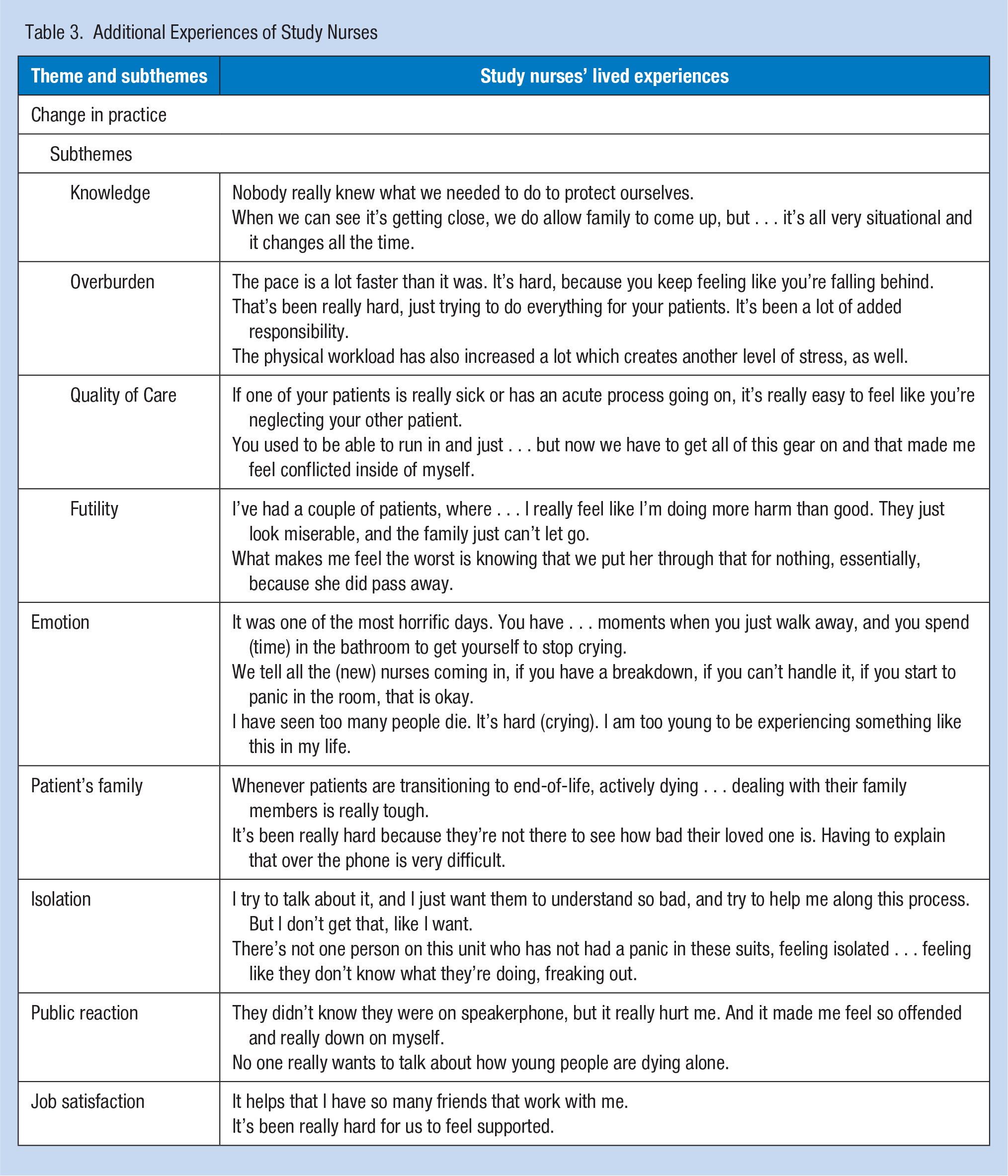
The ICU nurse sample comprised nine females and one male, all Caucasian, with a mean age of 26.6 years. Seven of the nurses were single and three were married. Mean years as an ICU nurse and mean years at job was 1.95 years (Table 2). The analysis of the interview transcripts revealed six recurring themes: Change in Practice, Emotion, Patient’s Family, Isolation, Job Satisfaction, and Public Reaction. The theme Change in Practice included four subthemes: Overburden, Knowledge, Quality of Care, and Futility. Experiences of study nurses can be found in Table 3.
Demographics of Intensive Care Unit Nurses (n = 10)
Additional Experiences of Study Nurses
Change in Practice
Overburden
Study nurses described a distinct change in practice since the pandemic began. They explained they were overburdened at work with an increase in the level of acuity of patients, daily workload, and number of patient deaths. One nurse stated, “I basically spent 10 hours in that patients’ room from the time they got there, until the time that they died.” Another nurse recalled, “I had two patients by myself and both just crashed at the same time . . . it just became a very stressful situation to get the help that I needed.” The ICU nurses must take time to put on PPE before entering the room and remember all needed supplies. A nurse explained, “You used to be able to run in and just help your patient, but now we have to get all of this gear on.” One nurse talked of the difference in the number of patient deaths, “One week my (assigned) patient died every single day.” The nurses also shared that many patients were dying alone because family members were not allowed on the unit due to risk of COVID-19 transmission. The family is called to come to the ICU only when the end of life is near. But the exact time a patient will die is hard to predict, so often, patients die alone. One nurse said, “I see people die all the time, but it’s just not like this . . . all alone.”
Knowledge
In the beginning of the COVID-19 pandemic, the ICU nurses had a critical need for knowledge about the novel coronavirus. One nurse recalled caring for her first patient infected with COVID-19: We didn’t know if PPE was going to be effective. We thought it’s really going to affect only those who are older or are immunocompromised, and very quickly our patient population was not representing that. With all of the obstacles, like PPE and not understanding the disease, (it) made taking care of these patients so much scarier.
The ICU nurses also discussed the lack of knowledge regarding ever-changing hospital policies concerning COVID-19, especially for proper PPE and visitation. One nurse stated, “Not knowing, like, what to do . . . not having concrete policies, but things just changing all the time. What sort of masks we have to wear . . . that just changes all the time.”
Quality of care
Study nurses spoke of how they were unable to give patients their usual quality care due to following hospital guidelines to minimize the risk of COVID-19 transmission (e.g., clustering care to reduce nursing encounters), time for donning PPE, and increased workload caring for these patients. One nurse stated, “I couldn’t (get in the room fast enough), and it caused my patient harm.” Another nurse reported, It makes me feel guilty because I’m on the outside (following hospital guidelines to minimize the risk of COVID-19 transmission). I should be doing everything to help them, but I feel like I can’t . . . I feel grief really.
And another nurse, “It makes you feel like a bad nurse . . . we do everything we can, but still we can’t do the little things like we used to do.”
Futility
The study nurses described experiencing futility; that they tried so hard to save their patients, yet kept witnessing so many patients die. One nurse said, “Every day you come in and you see the same type of patients over and over again. You see people die over and over again. It’s just like repetitive.” Another type of futility addressed was futile care, or medical treatment not likely to produce any meaningful benefit to the patient (Kyriakopoulos et al., 2017). One nurse stated, “I feel like these patients are lying here suffering, and we’re coding them, and we’re just intervening so much, when they are ultimately going to pass away.” Another nurse recounted, I remember being teary giving report, just thinking about all the things that we had been doing to this woman that seemed so unnecessary . . . to where in any other circumstance the family would just . . . let go peacefully, instead of spinal taps and neurological tests and everything.
Emotion
Study nurses were experiencing many negative emotions in their daily lives from caring for COVID-19 patients, including grief, worry, sadness, fear, and anger. They talked of an emotional “toll” from caring for these patients. One nurse described an episode of trying to save a COVID-19 patient’s life and reported frequently re-experiencing the event, “after the code, it literally looked like a war zone . . . and that is what haunts me every day in my dreams.” The nurses voiced their fear of bringing the virus home to family members, some of whom were newborns, elderly, or immunocompromised. One nurse stated, “I want to work, I don’t want to let my co-workers down, but I mean, I have to protect my family.” The nurses felt grief from the overwhelming amount of patient deaths and difficulty experiencing grief with the patient’s family. One nurse expressed how, for her, even the simple task of putting an isolation gown on a family member and taking it off carried so much emotional weight, . . . the intimacy of having to dress a family member up in the isolation garb and then take it off at the most distressed point in their life, and give them dignity, but also a goodbye with their loved one.
The nurses talked of their frustration battling COVID-19. One nurse said, “I just cried for two hours because I was just so frustrated, worn out, and tired.” Another nurse discussed the overall work environment, saying “We have always had really great teamwork, and we still do. It’s just, you could tell that there are underlying emotions: anger, frustration, and just numbness.” One nurse explained, “I definitely have felt like angry, like angry at my co-workers, angry at doctors, like just angry at people. I find myself just snapping at people and like, honestly, yelling sometimes, which is not like me.” Another nurse spoke of uncharacteristic anger and frustration that she recognized as a symptom of her experiences at work: I didn’t realize . . . that lashing out is a symptom. I was just so full of anger and I looked it (PTSD) up myself and I saw the signs and symptoms. And I was like, “this is new to me.” You know, there’s tons of “you could get help,” but I also feel like it’s my job.
Patient’s family
The pandemic brought new policies, including restrictions on visitation. The ICU nurses were sympathetic that family members were not allowed on the unit due to minimizing viral transmission. With this new restriction, the nurses were burdened with added responsibilities. Nurses now had a primary role in discussing patient status and care and often sought to help families connect using tablets and cell phones. When family were able to come to the unit (usually because the patient’s condition had declined considerably), they were often in shock after seeing their loved one for the first time since admission. One nurse acknowledged, “It’s been really sad to see people come in from being fine at their house, you know, yesterday and then the next time their family sees them we are withdrawing care (or) we’re there coding (the patient).” One nurse talked about an experience with family: When she came in and saw him for the first time . . . she went through every range of guilt . . . trying to shake the patient awake . . . telling me to turn everything off and yelling at me and yelling at the doctors because she was just so taken aback by all the drips and machinery all over her husband (crying). It was very scary . . . and also, the stress because I didn’t know how to handle that type of situation.
The nurses also spoke of the difficulty of witnessing patients die alone. The nurses used tablets or phones for families to see and talk to patients. During these times, families were having their most personal conversations. One nurse described a final call from family to say goodbye: I think, um, honestly . . . (sniffling, voice cracking) the worst experiences are the most stressful experiences with families. There was this one woman (and) her children on the telehealth, taking turns (talking), and she ended up passing that night, and (crying hard now) they said, “Mom, you’ve got to get better, (voice cracking), you just can’t leave us now.” And that’s just not the way to say goodbye to people.
Isolation
In the beginning of the pandemic, most of the ICU nurses self-imposed isolation due to fear of spreading the virus. One nurse explained, When we first started, I wouldn’t go around my parents . . . or grandparents for the fear that I was going to be the cause to get them sick. It was really hard . . . I went, like, two months without seeing them.
Family and friends were also fearful of contracting the virus due to their caring for COVID-19 patients. One nurse recalled seeing family for the first time after self-isolating from them, “They didn’t want to see us, and the first time I saw them I didn’t know if I could hug them. It’s really hard. You feel ostracized.” Another nurse stated, “our hospital (in the beginning) . . . treated us like we were dirty. They told us we weren’t allowed to work on other units. (Some) doctors who had consults would refuse to come on our unit.” At times, study nurses also felt isolated from each other while busily caring for COVID-19 patients: There’s been situations where . . . things that I just couldn’t really handle by myself . . . felt very unsafe for me and the patient, and just kind of lost for what to do . . . my patient is desatting (desaturation of oxygen level) and I look out the window and there’s no other nurses around. And I just feel panicky, like what do I do? Even though I’ve been a nurse for (some) years, I still just feel really scared. I feel like a new nurse all over again.
Public Reaction
Study nurses discussed how angered they were that they were putting their health and their families’ health at risk caring for COVID-19 patients, and yet some people ignored social distancing guidelines. One nurse said, “I think the hardest part, is for me, seeing how the rest of the world, especially in the beginning, didn’t take it seriously, and didn’t social distance, and still don’t now.” The nurses spoke of being shunned by family and friends. One nurse recalled, “At the beginning, I had several family and friends who didn’t want to see me. I understand . . . they’re coming from a place of safety, but it did hurt me.” Study nurses also spoke of personal injury from others due to caring for COVID-19 patients, “Sometimes my friends say, ‘can we please just stop talking about COVID’ and it kind of hurts my feelings.”
Job Satisfaction
Study nurses had differing feelings about job satisfaction. One nurse said, “ I have a very strong work ethic. I want to work. I love my job.” Other nurses reported on aspects of their job they were not happy about. One nurse stated, One of the most stressful things . . . is that we weren’t really asked to care for COVID-19 patients. It was like here is this disease . . . we don’t have enough PPE . . . but just get in there and do it.
Another nurse recounted how she felt when the hospital reduced salaries due to pandemic-related financial consequences: You know, toward the beginning . . . (they) cut our pay. We just felt like that was such a big slap in the face, and that definitely contributed, I think, to a lot of our stress. Now we’re getting COVID pay. We just talk about all the time how we wish administration and higher ups would come down to the unit for a day and see what we deal with.
Quantitative Results
The quantitative portion of this research assessed for PTSD using the PTSD Checklist-5. The 20-item scale measures PTSD using the four DSM-5 cluster symptoms: re-experiencing of traumatic event(s), avoidance of reminders or similar situations, negative alterations in cognition and mood, and hyperarousal symptoms. Blevins et al.’s (2015) initial psychometric evaluation determined the PCL-5 was a psychometrically sound measure and exhibited strong reliability and validity. Cronbach’s alpha coefficient of internal consistency was .94 and retest reliability was .82. Of the 10 ICU nurses, 7 (70%) met the diagnostic criteria for PTSD using a PCL-5 cut-point score of ≥31. Job satisfaction findings determined that 1 of the 10 (10%) ICU nurses was very satisfied with their job; 7 (70%) were somewhat satisfied, 1 (10%) was neither satisfied nor dissatisfied, and 1 was somewhat dissatisfied. Five of the 10 (50%) participants had considered leaving job in the last 6 months.
Discussion
Infectious disease outbreaks affect frontline health care workers disproportionately, from threatening their lives, to changing and stressful work demands, and coping with high death rates, all of which can further heighten their fear, anxiety, and stress (Mohammed et al., 2015). Through the sharing of the study nurses’ stories, an intricate and detailed description of their experiences underscored the psychological stress and trauma these nurses lived through (and continue to endure) caring for COVID-19 patients. Our study nurses experienced many changes in practice, including overburden at work; lack of knowledge, or ever-changing knowledge of the COVID-19 virus and hospital policies; not being able to give patients their standard quality of care; and futility. Study nurses experienced overburden at work due to increased workload, heightened acuity of patients, and added work responsibilities. There was also ever-changing knowledge of the virus and associated hospital policies. Study nurses could no longer give patients their standard quality of care because of COVID-19 transmission precautions, time for donning PPE, and increased workload caring for these patients. For nearly two decades, the nursing profession has been ranked as one of the most trusted professions (Gallup Incorporated, 2020). Study nurses experienced feelings of guilt and inadequacy from not being able to maintain quality of care for their patients. Study nurses perceived their efforts as futile due to the unprecedented number of patient deaths or when they felt patients would no longer benefit from aggressive care. Jameton (1984) created the term “moral distress” to illustrate when nurses are constrained to do things that they believe are morally wrong. End-of-life care that is perceived to be overly aggressive is an especially common source of moral distress (Dodek et al., 2019; Henrich et al., 2016). These changes in practice, echoed in prior research (Crowe et al., 2021; Galehdar et al., 2021; Lapum et al., 2021; Schroeder et al., 2020; Silverman et al., 2021), caused study nurses significant stress.
Study nurses suffered a wide range of emotions while caring for COVID-19 patients, including worry, fear, grief, anger, and frustration. These emotions are in accordance with other study findings which illustrated nurses’ fear of COVID-19 transmission to themselves and/or their family (Galehdar et al., 2021), moral distress from not being able to give their best care (Galehdar et al., 2021; Jia et al., 2021), and difficulty in hearing the heart-wrenching last words of grief-stricken family members (LoGiudice & Bartos, 2021). Also distressing for our sample of nurses, and other nurses caring for COVID-19 patients during the pandemic, was witnessing patients dying alone (Crowe et al., 2021; LoGiudice & Bartos, 2021; Robinson & Stinson, 2021).
After many months of self-imposed isolation from family and friends without contracting the virus, study nurses felt safer and began to see family again, practicing social distancing. However, similar to other studies (Crowe et al., 2021; Kackin et al., 2020), some family and friends were fearful of reuniting with them, resulting in study nurses feeling ostracized. In contrast to our findings, however, the ICU nurses in Kackin et al.’s (2021) study preferred to isolate from others when they felt shunned. One reason cited was the risk of being stigmatized by society. Another type of isolation some study nurses experienced was isolation from coworkers due to increased workload and coworkers being busy in patients’ isolation rooms. This caused them psychological distress when alone with their patient whose condition was deteriorating. Renowned psychiatrist Herbert Spiegel (1944) found that a lack of support, or even a perceived lack of support, can cause a sense of aloneness which can result in psychological trauma during distressing situations.
Study nurses experienced both stress and anger when individuals disregarded the importance of social distancing, while they were being pushed to the brink at work and placed themselves and their family at risk. The significant stress study nurses experienced caring for COVID-19 patients adversely impacted most study nurses’ job satisfaction. An unsettling survey by the American Nurses Association (2020), with responses from more than 32,000 nurses caring for patients during the COVID-19 pandemic, found 87% were very or somewhat afraid to go to work. It is well-documented that psychological stress experienced in the workplace contributes to a high turnover and results in some nurses leaving the nursing profession altogether (Lim et al., 2010; Morley et al., 2020; Vahedian-Azimi et al., 2019).
Findings from the quantitative data analysis also provided insight into the psychological stress study nurses experienced caring for COVID-19 patients, as 7 of 10 study nurses met diagnostic criteria for PTSD. While our quantitative findings of PTSD are not generalizable due to the small sample, Greenberg et al.’s (2021) study found an alarming 49% of ICU nurse participants who cared for COVID-19 patients with probable PTSD (in a sample of 344 ICU nurses). Furthermore, nearly 20% of these nurses reported thoughts of self-harm or suicide.
Mealer et al.’s (2012) study investigated traumatic event(s) nurses with probable PTSD (21% of 744 nurses) experienced, citing failure to save a patient (50%), performing futile care (36%), and witnessing patients die (29%) as the top events that caused the trauma. Similarly, our study found events that inflicted psychological stress or trauma included witnessing many patients die, compounded by the fact that many died alone; performing futile care; being isolated from coworkers when their patient’s condition was declining; and frequently hearing their patients’ family members’ heart-wrenching last words to their loved one. The nurses in our study (mean age = 26.6 years; mean years of ICU experience = 1.95 years), and in ICUs in general, are younger than the overall nursing population (Data USA, 2019; National Council of State Boards of Nursing, 2017). d’Ettorre et al.’s (2021) systematic review of health care workers caring for patients during the COVID-19 pandemic also found a high rate of post-traumatic stress in young health care workers with low work experience. More research is needed to examine the difference in how nurses experience traumatic work, occupational, or work-life events at different levels of experience and/or age.
Limitations
Although the researchers sought to recruit a diverse group of nurses, there was a lack of racial and sexual diversity among participants. It is possible that the difficult experiences reported by these ICU nurses, who all identified as White, may differ from other ethnicities. For instance, research suggests that Blacks experience higher levels of violent victimization and a higher lifetime prevalence of PTSD when compared with Whites; Asians may experience substantially lower levels of violent victimization and are at lower risk for the development of PTSD (Brooks Holliday et al., 2020; Roberts et al., 2011). In addition, women are approximately twice as likely to suffer from PTSD as men (National Center for PTSD, n.d.). Of note, in the study state, 81% of nurses are White, 15% Black, and 4% consist of other races (Alabama Board of Nursing, 2016). Furthermore, only 10% of nurses are male. Further limitations include that this study was limited to a particular ICU unit and findings may not be generalizable to other COVID units. Quantitative findings are not generalizable due to the small sample size.
Implications for Practice
The findings of this research contribute to important implications for occupational health nursing practice. Hospital administrators, nurse managers, and occupational health nurses need to develop and implement policies and evidence-based interventions to mitigate or prevent development of PTSD for their ICU nurse employees. Offering ICU nursing staff ongoing psychological support, as needed (e.g., incident debriefing, counseling, or support through an employee assistance program) and as opt-out rather than opt-in may increase participation. Mental health screenings should be made accessible and affordable. Identification of symptoms of PTSD must be confidential and seeking treatment should not threaten nurses’ licensure or employment.
Early identification of psychological stress and PTSD can assist in prevention of long-term health consequences, including cardiovascular disease, diabetes, and hypertension (Dyball et al., 2019). A McKinsey Global Institute (2021) study found 62% of 400 frontline nurses who cared for COVID-19 patients believed that active monitoring of nurse distress would be effective in supporting the well-being of nurses. Heart rate variability (HRV) is an objective, noninvasive, and low-cost tool that can measure psychological stress and autonomic nervous system function (Ge et al., 2020; Kim et al., 2018). Past research has found a significant association between PTSD and reduced, or low, HRV (Ge et al., 2020; Schneider & Schwerdtfeger, 2020). If low HRV indicating psychological stress is observed, nurse managers and occupational health nurses can recommend a program where skills in self-regulation techniques are learned (e.g., focused breathing techniques) in conjunction with HRV monitoring. Enabling ICU nurses to monitor their HRV and practice self-regulation techniques can be an effective strategy to reduce psychological stress and equip them with tools to remain in the ICU workforce.
Applying Research to Occupational Health Practice
This study aimed to investigate the lived experiences of ICU nurses caring for COVID-19 patients to heighten the understanding of what this means in the nurses’ personal and professional lives. An intricate description of their experiences emphasized the psychological stress and trauma these nurses lived through caring for COVID-19 patients. Analysis of interview transcripts revealed six recurring themes: Change in Practice, Emotion, Patient’s Family, Isolation, Public Reaction, and Job Satisfaction. Quantitative findings revealed 7 of 10 study nurses met the diagnostic criteria for PTSD, 7 of 10 were only “somewhat satisfied” with their job, and 5 of 10 considered leaving their job in the last 6 months. The findings of this research contribute to important implications for occupational health nursing practice. Hospital administrators, nurse managers, and occupational health nurses must develop and implement policies and evidence-based interventions to mitigate or prevent development of PTSD for their ICU nurse employees.
Footnotes
Acknowledgements
The authors would like to thank the ICU nurse participants for taking time to participate in this research.
Authors’ Note
IRB-300005501 Approval was obtained from the Institutional Review Board on July 30, 2020, for “Intensive Care Unit Nurses’ Experiences of Caring for COVID-19 Patients.”
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.