
Abstract
Background:
Intensive care unit (ICU) nurses are at an increased risk of post-traumatic stress disorder (PTSD) due to their stressful work environment. Using the Walker and Avant conceptual analysis method, we sought to review the literature to better understand PTSD as it pertained to ICU nurses and its impact on their lives, patient care, and health care organizations.
Methods:
For the review, we searched the Cumulative Index of Nursing and Allied Health Literature (CINAHL), PubMed, and PsycINFO. The keyword searches included the terms “post-traumatic stress disorder” AND “psychological stress” AND “intensive care unit nurses.” Abstract and full text reviews were conducted. Ten articles met our inclusion criteria of being published in the past 10 years (2010–2020), peer reviewed, written in English, and referred specifically to PTSD and psychological stress in ICU nurses.
Findings:
Antecedents for PTSD in ICU nurses are their stressful work environment, where exposure to traumatic events is experienced, and a lack of support from their manager, coworkers, and organization. Defining attributes for ICU nurses with PTSD included reexperiencing, avoidance, negative alterations in cognition and mood, and hyperarousal. Consequences identified included burnout, job dissatisfaction, and the intention to leave their job. The conceptual definition of PTSD in ICU nurses was illustrated by the attributes, antecedents, consequences, model case, empirical referents, and by the negative impact on the nurse, patients, and the health care organization.
Conclusion/Application to Practice:
Hospital administrators, nurse managers, and occupational health nurses should ensure that policies and interventions are in place to recognize and reduce the risk of PTSD among ICU nurses.
Background
Post-traumatic stress disorder (PTSD) is a psychiatric disorder affecting nearly 5 million adults in the United States costing more than US$42 billion annually (Kilpatrick et al., 2013). Due to the nature of the job, namely, caring for complex, high-acuity patients, intensive care unit (ICU) nurses may be affected by numerous stressors and traumas in the workplace. These include performing cardiopulmonary resuscitation, frequently witnessing death and serious injuries of patients, caring for patients who are suffering, and performing futile care (Karanikola & Mpouzika, 2018; Mealer et al., 2007). Consequently, ICU nurses are at high risk of developing PTSD (Colville et al., 2017; Mealer et al., 2009; Rodriguez et al., 2017). Mealer et al. (2009) determined that approximately 33% of ICU nurses have symptoms of PTSD, and nearly 23% of ICU nurses meet the American Psychiatric Association (APA) diagnostic criteria for PTSD, much higher than that of general nurses (18%) and the general population (8%–10%).
Widespread attention was brought to the concept of psychological trauma after thousands of young soldiers experienced horrors during combat in World War I (Lasiuk & Hegadoren, 2006). The term “shellshock” was created to describe their condition with symptoms such as uncontrolled crying, feelings of numbness, inability to speak, and memory problems (Myers, 1915). During the 1960s and 1970s, physicians and researchers caring for Holocaust survivors (Nathan et al., 1964), rape victims (Burgess & Holmstrom, 1974), and abused children (Kempe & Kempe, 1978) accumulated more understanding of this unique type of psychological trauma and made significant scientific contributions (Lasiuk & Hegadoren, 2006). In 1980, with this new knowledge, and the extraordinary number of Vietnam veterans affected with chronic psychological distress, the American Psychiatric Association (APA) first included “post-traumatic stress” disorder to the Diagnostic and Statistical Manual of Mental Disorders (3rd ed.; DSM-III; APA, 1980; Crocq & Crocq, 2000). In 1994, the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) revised the definition of PTSD to include both direct and indirect traumatic events. Since then, PTSD has been recognized in health care professions, especially in nursing, that are continuously subjected to witnessing death and dying (Pai et al., 2017).
Currently, PTSD is described in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) as involving a direct or indirect exposure to a single traumatic event or repetitive episodes that results in symptoms and stress responses that last greater than one month. The DSM-5 revision changed PTSD from an anxiety-related disorder to a trauma- and stressor-related disorder and categorized symptoms that result from the traumatic event(s) into four clusters. The symptom clusters are reexperiencing the trauma, avoidance, negative alterations in cognition and mood, and marked alterations in arousal and reactivity (APA, 2013).
When ICU nurses suffer from the debilitating symptoms of PTSD, both their psychological and physical health is directly affected (Karanikola & Mpouzika, 2018; Ong et al., 2016). Patient care and the health care organization are also negatively influenced (Czaja et al., 2012; Salmon & Morehead, 2019). Patient care may be affected when ICU nurses with PTSD suffer from diminished concentration and cognitive ability, leading to medication errors or even sentinel events, such as events that result in a patient’s death or serious physical or psychological harm (Park & Kim, 2013). In addition, nurses may exhibit a lack of empathy toward their patients, sometimes termed compassion fatigue (Salmon & Morehead, 2019). Many ICU nurses with PTSD experience symptoms of burnout caused by excessive stress in the demanding work environment (Colville et al., 2017; Mealer et al., 2009; Rodríguez-Rey et al., 2019). Burnout arises from the inability to cope with work-related stress over an extended period of time and is characterized by emotional exhaustion, depersonalization (cynical or indifferent attitude toward one’s job), and decreased sense of personal accomplishment (Maslach et al., 1986; Vahedian-Azimi et al., 2019).
Adverse effects of ICU nurses with PTSD also affect hospital-wide outcomes due to decreased quality of patient care from experiencing encumbering symptoms of PTSD, and retention issues, both of which can lead to significant monetary costs for the organization (Salmon & Morehead, 2019). The U.S. health care system is currently experiencing a critical shortage of ICU nurses (Chan et al. 2013). The turnover rate for ICU nurses is presently above 18% (Nursing Solutions, Incorporated, 2020). Replacing one ICU nurse cost would be $70,000 US (Society of Critical Care Medicine, n.d.). Using this estimate, a hospital with 40 ICU beds and 100 ICU nurses with an annual turnover rate of 18% would cost the hospital nearly US$1,260,000 per year (Moss et al., 2016).
The need for health care professionals and hospital stakeholders to better understand PTSD as it pertains to ICU nurses is critical to maintain the health of their employees, improve patient care, and optimize organizational outcomes. Gaps in the literature include the antecedent and the overall impact of PTSD among ICU nurses. Although there is ample research on PTSD now as opposed to decades ago, and in many populations, how this uniquely applies to ICU nurses and how they experience PTSD is not well articulated in the current literature. Thus, the purpose of this concept analysis was to clarify the concept of PTSD as it applies to ICU nurses using the Walker and Avant method (Walker & Avant, 2011). Implications for research and practice are provided.
Methods
Walker and Avant’s (2011) concept analysis method was chosen for its structured and rigorous process. A concept analysis is beneficial when a concept has changed over time because of new knowledge or when there is confusion concerning its definition. By using Walker and Avant’s eight-step framework, the concept is broken down into its components and differentiated from similar concepts. The iterative process helps refine the concept by identifying all uses of the concept, and defining its key attributes, antecedents, and consequences. Implementation of this process is instrumental in explicating a model case, borderline case, and contrary case to better illustrate the concept. The final step is determining the empirical referents, which assists in measuring the concept (Walker & Avant, 2011). The steps in the Walker and Avant conceptual analysis method allow for better understanding of the concept across health care disciplines.
A review of the literature included peer-reviewed research articles published in the literature over the past 10 years, from 2010 to 2020. As seen in Figure 1, the databases searched include Cumulative Index of Nursing and Allied Health Literature (CINAHL), PubMed, and PsycINFO. The keywords used in the database searches included the terms “post-traumatic stress disorder” AND “psychological stress” AND “intensive care unit nurses.” The search resulted in 53 articles found in CINAHL, 97 articles in PubMed, and 142 articles in PsycINFO. The combined results of the database searches resulted in 292 articles. A total of 69 duplicates were removed. The resulting literature was examined by evaluating titles and abstracts for relevance. The inclusion criteria for this concept analysis included articles in peer-reviewed journals that performed or discussed studies that evaluated PTSD and psychological stress in ICU nurses and were written in the English language. This preliminary title and abstract review excluded 179 articles that were not articles on PTSD and psychological stress in ICU nurses, resulting in 44 articles that were eligible for full-text review. The 44 research articles were read in full, and references within the articles were also reviewed. After a thorough review, 34 articles were excluded because they either were correlational studies, which only stated prevalence rates and did not describe symptoms of psychological stress or PTSD in ICU nurses, or the prime focus was on other topics, such as resilience, emotional exhaustion, or which type of ICU had the highest prevalence of PTSD. Thus, a total of 10 articles were included in this concept analysis.
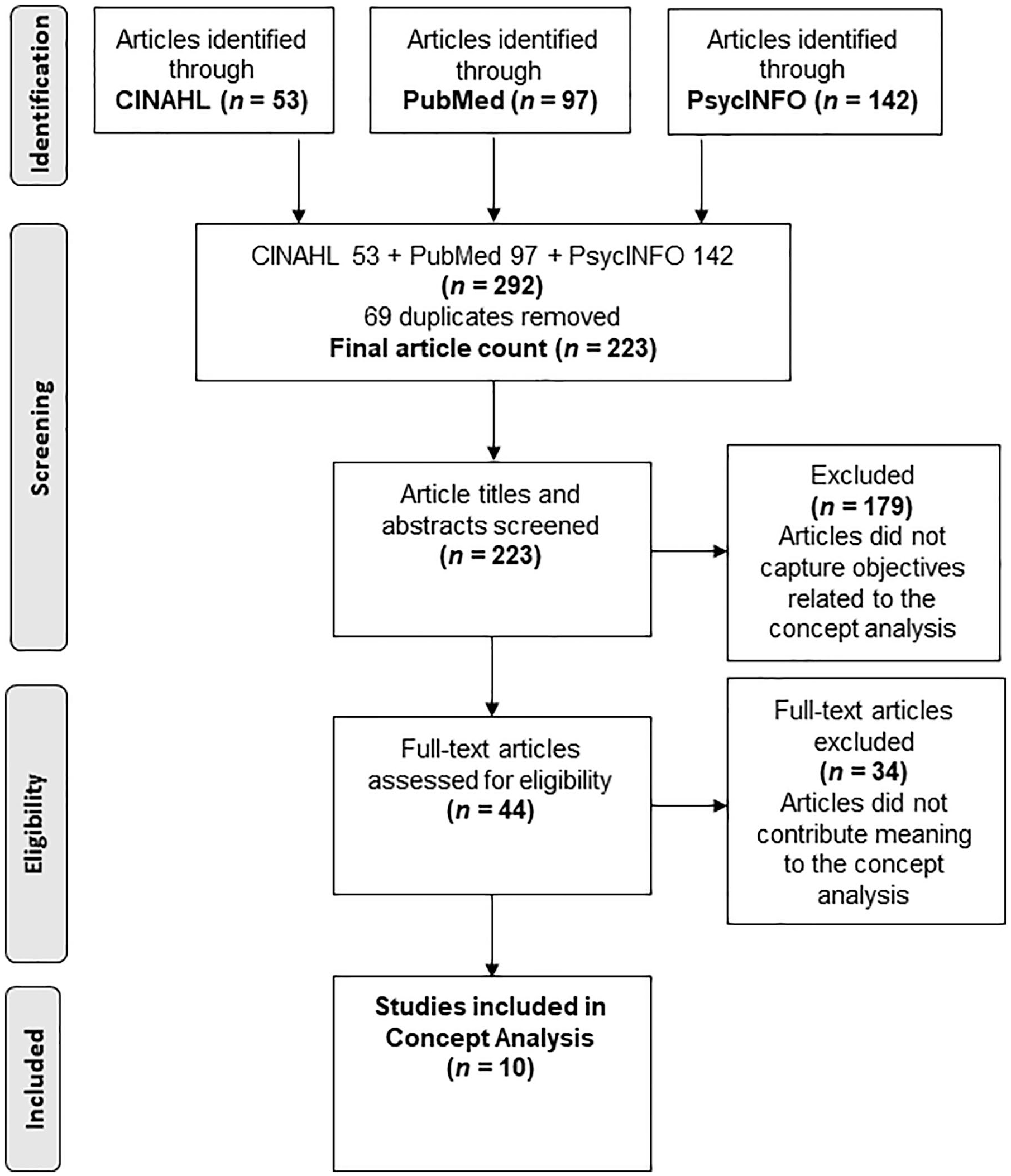
PRISMA diagram of identification of articles that contributed to the concept analysis of post-traumatic stress disorder in ICU nurses.
Findings
In Table 1, the content of each of the 10 articles was examined to determine what attributes, related symptoms, and consequences were specific to PTSD in ICU nurses. PTSD attributes were identified by carefully analyzing each of the 10 articles, and the information was subsequently recorded. At the conclusion of this process, the defining attributes were discovered, as these are the characteristics that appear repeatedly in a concept (Walker & Avant, 2011). Related symptoms were found in a similar manner and were comprised of both physical and psychological symptoms. Consequences were also discovered and often occur as a result of PTSD. Based on this, Figure 2 provides a visual summary of the antecedents, defining attributes, and consequences for the ICU nurse, the patient, and the health care organization.
Summary of PTSD Attributes, Symptoms, and Consequences Described by Selected Articles as They Pertain to ICU Nurses
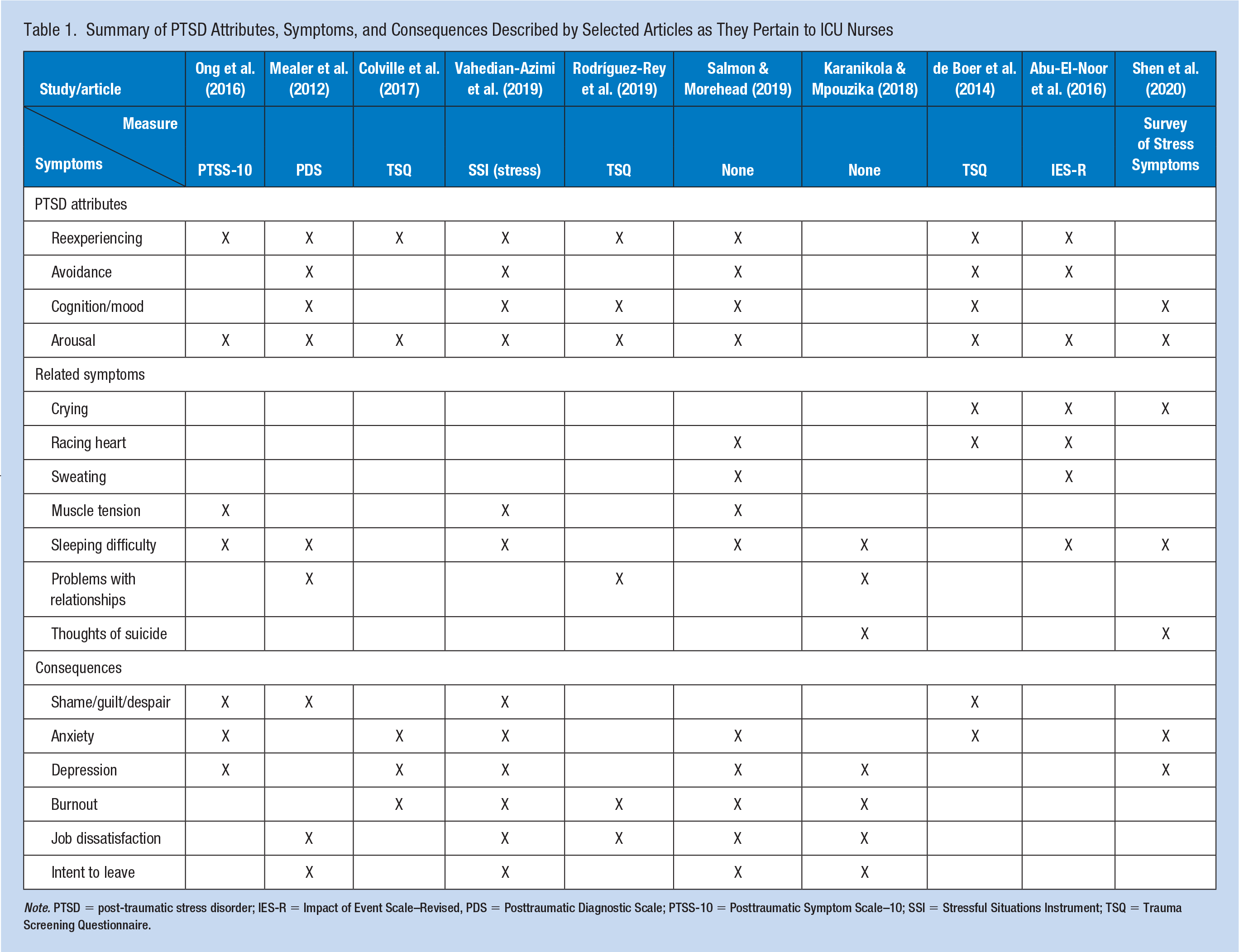
Note. PTSD = post-traumatic stress disorder; IES-R = Impact of Event Scale–Revised, PDS = Posttraumatic Diagnostic Scale; PTSS-10 = Posttraumatic Symptom Scale–10; SSI = Stressful Situations Instrument; TSQ = Trauma Screening Questionnaire.
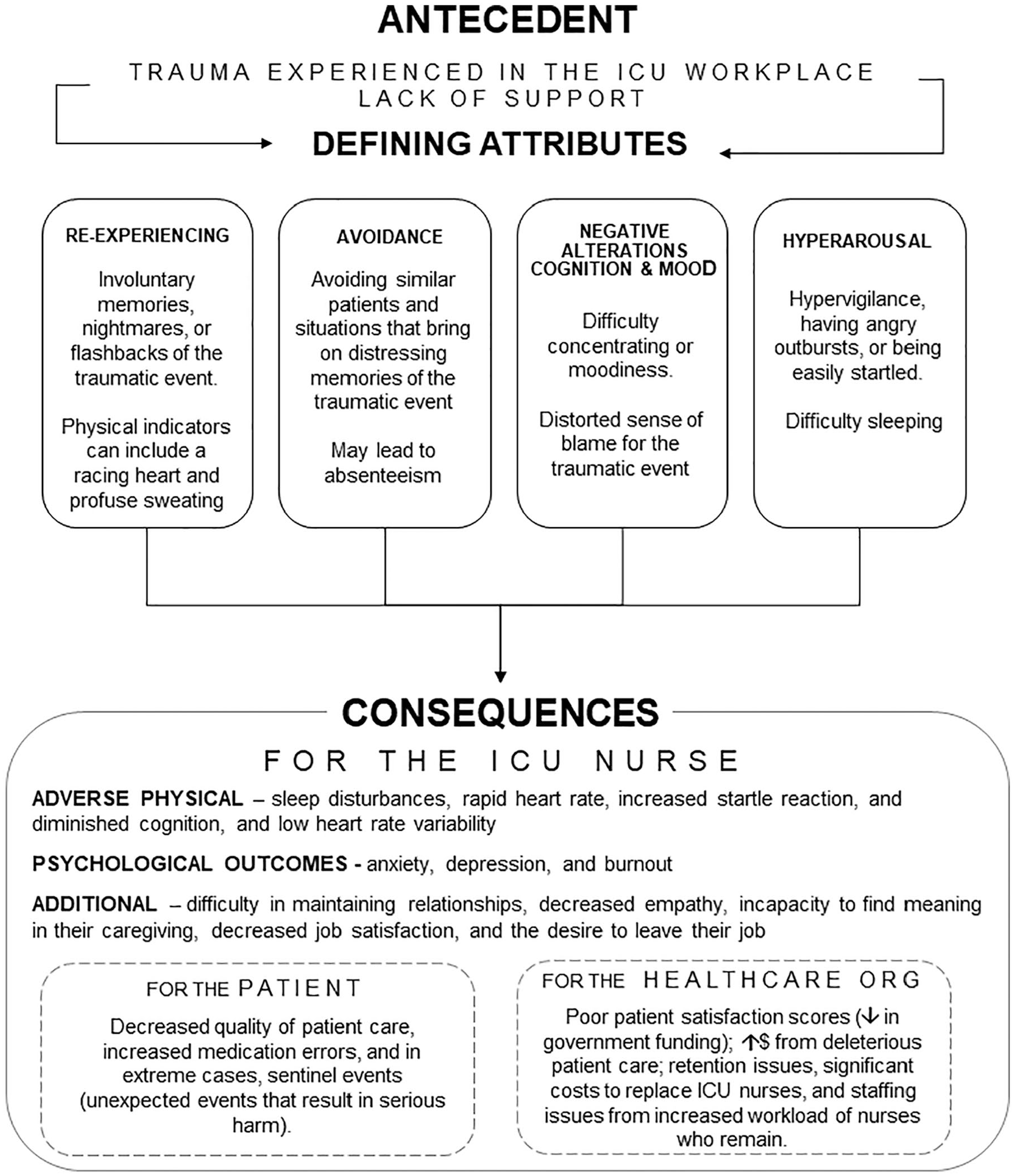
Antecedents, defining attributes, and consequences for ICU nurses with PTSD.
Identification of All Uses of the Concept
The American Psychological Association Dictionary of Psychology (2020) defines PTSD as “a disorder that may result when an individual lives through or witnesses an event in which he or she believes that there is a threat to life or physical integrity and safety.” The disorder may also occur from repeated exposure to traumatic events. The online Free Medical Dictionary (n.d.) defines PTSD as a “trauma- and stressor-related disorder” in DSM-5, arising from a traumatic event involving actual or threatened death, serious injury, or sexual violence to self or others.
Defining Attributes
The defining attributes are the most important aspect of the concept analysis because they offer the broadest insight into the concept (Walker & Avant, 2011). The prevailing defining attributes in the articles describing ICU nurses suffering with PTSD were determined after a thorough review. They are reexperiencing the traumatic event, avoidance, negative alterations in cognition and mood, and hyperarousal.
Reexperiencing
Eight of the 10 articles reviewed determined reexperiencing symptoms. Reexperiencing occurred as involuntary memories, nightmares, or flashbacks of the traumatic event (Abu-El-Noor et al., 2016; Colville et al., 2017; Ong et al., 2016). These reexperiencing events are typical immediately following a traumatic event; however, when they last longer than a few months, it can be a predictor of PTSD (APA, 2013). Reexperiencing can be triggered by tactile sensations, smells, noises, or unwanted thoughts (APA, 2013). Mealer et al. (2012) reported that one nurse could no longer eat salmon because the look and texture reminded her of her traumatic experience caring for her patient with an open wound: “. . . you could see down to the bottom of her spine and you could see like all the connective tissue.” Physical indicators were described when reexperiencing the traumatic event, such as muscle tension, a racing heart, and profuse sweating (Abu-El-Noor et al., 2016; de Boer et al., 2014; Salmon & Morehead, 2019).
Avoidance
Five of the 10 articles reviewed determined avoidance symptoms. Avoidance was exhibited by avoiding thoughts or feelings of the traumatic event (Salmon & Morehead, 2019). Avoidance was also demonstrated through avoidance of similar patients from the experienced trauma and absenteeism (de Boer et al., 2014; Salmon & Morehead, 2019). In de Boer et al.’s (2014) study, one ICU nurse stated, “certain patients were avoided . . . I sometimes feel the need to choose ‘risk-free’, patients.” Substance abuse and excessive alcohol use were other mechanisms of avoidance documented in ICU nurses with PTSD (Karanikola & Mpouzika, 2018; Mealer et al., 2012); and, in dire cases, some of the ICU nurses reported suicidal thoughts (Shen et al., 2020).
Negative alterations in cognition and mood
Six of the 10 articles determined symptoms of negative alterations in cognition and mood. Impaired cognitive ability and mood were exhibited as trouble concentrating or moodiness (de Boer et al., 2014; Salmon & Morehead, 2019). A distorted sense of blame for the triggering event also occurred (Mealer et al., 2012; Vahedian-Azimi et al., 2019). Lastly, there was a marked lack of interest in activities previously enjoyed (Vahedian-Azimi et al., 2019), as well as feelings of detachment and estrangement from friends and coworkers (Mealer et al., 2012). After ICU nurses had experienced trauma in the workplace and were suffering from PTSD, they felt changed from the person they were before and had feelings of detachment and estrangement (Mealer et al., 2012). For example, some felt that they no longer “really knew anyone,” or trusted anyone, and had no one with whom they could share their grief (Mealer et al., 2012).
Hyperarousal
Nine of the 10 articles determined symptoms of hyperarousal. Hyperarousal is a physiological response to stress, similar to the “fight or flight” response (APA, 2013). Hyperarousal symptoms in ICU nurses with PTSD included irritability, hypervigilance, angry outbursts, or being easily startled (de Boer et al., 2014; Shen et al., 2020). Difficulty sleeping (Ong et al., 2016; Shen et al., 2020) and problems maintaining interpersonal relationships were observed in two studies (Karanikola & Mpouzika, 2018; Mealer et al., 2012).
Antecedents and consequences
Antecedents are events or incidents that must occur prior to the occurrence of the concept (Walker & Avant, 2011). The antecedent for PTSD in ICU nurses is their stressful work environment where exposure to traumatic events are experienced through direct patient care, such as performing cardiopulmonary resuscitation, witnessing patients die, or seeing patients who are hemorrhaging (Karanikola & Mpouzika, 2018; Salmon & Morehead, 2019). Indirect exposures, such as repeated exposure to traumatic events in the ICU workplace, also qualify as an antecedent (APA, 2013). According to the Society of Critical Care Medicine (n.d.), approximately 20% of patients admitted to the ICU die. An additional antecedent for ICU nurses was observed as a lack of support from their manager, coworkers, and organization (de Boer et al., 2014; Mealer et al., 2012). A lack of support was felt by ICU nurses when (a) they reached out to their nurse manager for help but were criticized or reprimanded for their lack of knowledge (Mealer et al., 2012); (b) they felt they did not “really know” their coworkers, or were not being heard (de Boer et al., 2014); or (c) they did not feel appreciated by their organization (Salmon & Morehead, 2019). The lack of support, or perceived lack of support, may lead to feelings of aloneness, and can result in increased stress and psychological trauma (Spiegel, 1944).
Consequences are events that ensue as a result of the occurrence of the concept (Walker & Avant, 2011). The development of PTSD in ICU nurses was shown to result in psychological consequences, such as feelings of shame and despair, and constantly wondering what could have been done differently for their patient (de Boer et al., 2014; Mealer et al., 2012). Long-lasting physical consequences also arose from the development of PTSD. According to Edmondson et al.’s (2013) meta-analytic review, PTSD was associated with increased risk of reduced heart rate variability (HRV), coronary heart disease, and cardiac mortality. HRV is the change of time intervals in consecutive heart beats; low HRV can indicate chronic stress and pathology (Thayer et al., 2009).
When ICU nurses suffered from symptoms of PTSD, there were also consequences for the patient (Salmon & Morehead, 2019; Vahedian-Azimi et al., 2019). Patient care was affected by each of the four defining attribute symptoms that the ICU nurses with PTSD experienced. For example, reexperiencing symptoms led to poor sleep quality for the ICU nurse resulting in physical exhaustion (Shen et al., 2020). Avoidance symptoms resulted in avoidance of similar patients (de Boer et al., 2014), or lack of quality care if they did receive a patient similar to that from the traumatic event. Negative alterations in cognition and mood translated to a lack of empathy toward patients (de Boer et al., 2014). Both Salmon and Morehead’s (2019) study and Vahedian-Azimi et al.’s (2019) study reported that ICU nurses with PTSD can experience diminished concentration and cognitive ability, which has been linked to medication errors (Park & Kim, 2013). Hyperarousal symptoms, such as feeling irritable or having angry outbursts, were endorsed by those ICU nurses with high scores measuring PTSD in Rodríguez-Rey et al.’s (2019) study.
Other consequences that were reported included anxiety, depression, burnout, decreased job satisfaction, and the desire to leave their job (Colville et al., 2017; Salmon & Morehead, 2019). These consequences also affect the health care organization (Moss et al., 2016; Salmon & Morehead, 2019). The majority of the articles analyzed reported on the prevalence of anxiety and depression in ICU nurses with PTSD. Yet not discussed, stress disorders, such as PTSD, anxiety, and depression are familial and heritable (Smoller, 2016) and can often overlap (Brady et al., 2000). The overlap of these disorders can lead to diagnostic confusion and, more importantly, the underdiagnosis of PTSD (Brady et al., 2000). Current research suggests that ICU nurses with PTSD had a higher risk of developing burnout syndrome (Colville et al., 2017; Rodríguez-Rey et al., 2019). With burnout syndrome, the ICU nurses suffered from emotional exhaustion, depersonalization, and feelings of failure (Maslach et al., 1986; Rodríguez-Rey et al., 2019). Both PTSD and burnout syndrome in ICU nurses were associated with job dissatisfaction and intent to leave their job, which can affect patient care and the financial bottom line of the hospital (Moss et al., 2016; Salmon & Morehead, 2019).
Example Cases: Model Case, Borderline Case, and Contrary Case
To illustrate how this concept manifests in ICU nurses, a model case, a borderline case, and a contrary case have been constructed. A model case is “a pure case of the concept, a paradigmatic example, or a pure exemplar” (Walker & Avant, 2011, p. 163). A borderline case has most, but not all, of the defining attributes; and a contrary case exemplifies what the concept clearly is not.
Model case
Pamela is a 32-year-old ICU nurse who works in an ICU of a large hospital. Over the past few weeks, she has been caring for a 71-year-old patient with COVID-19. Pamela’s patient only required supplemental oxygen in the form of a nasal cannula when first admitted, but now the patient is extremely anxious and gasping for air. The hospital has been inundated with COVID-19 patients, and supplies have dwindled. Pamela increases the patient’s oxygen, administers the ordered antianxiety medication, and puts in a stat call to the respiratory therapy team and the patient’s critical care doctor. Then, Pamela looks around the unit and wonders whether any of the other patients on ventilators might have recovered enough to be weaned. The alarms go off in Pamela’s patient’s room, and she realizes that her patient is experiencing a cardiopulmonary arrest. A code blue is called, and despite her efforts, along with the code team, the patient died. Pamela becomes consumed with thinking about what else she could have done to help her patient. She awakens from nightmares of the traumatic event, often finding that her heart is racing and that she is in a cold sweat. At work, she now avoids patients that remind her of this patient and becomes anxious when she gets new patient assignments. She is also having trouble concentrating and startles easily when she hears alarms. Her friends call her to get together for a walk, but she no longer takes pleasure in activities that she once enjoyed. This case includes all the defining attributes of PTSD: reexperiencing, avoidance, negative alterations in cognition and mood, and hyperarousal.
Borderline case
Kayla is a 32-year-old ICU nurse working in a surgical ICU at a local hospital. She receives a 30-year-old female patient, post motor vehicle accident from the operating room. The patient is intubated and receiving a massive transfusion of packed red blood cells, but the patient continues to hemorrhage from the abdominal surgical site. Blood is saturating the patient’s gown and sheets. Despite the massive transfusion of blood, the patient experiences a cardiopulmonary arrest and expires. In the next few months, Kayla cannot stop thinking of the patient hemorrhaging and has been having nightmares about the event. At work, Kayla becomes anxious when she is assigned patients after abdominal surgeries because they remind Kayla of losing this patient. Fortunately, she has been able to care for patients after other types of surgeries with ease. She is also able to enjoy her life outside of work. Kayla has symptoms of reexperiencing and avoidance but does not demonstrate symptoms in all the symptom clusters, and therefore demonstrates a borderline case.
Contrary case
Krista is a 29-year-old ICU nurse at a trauma center who receives an 18-year-old male after he accidently shot himself in the face when falling out of a deer-hunting stand. Krista is horrified by the young man’s wounds but continues to work with competence to stabilize the patient. The patient experiences a cardiopulmonary arrest and expires, despite her appropriate interventions, along with other nurses on the unit and the code team. Krista is visibly shaken by the loss of her patient and cries with other staff members who attempted to save the young man. She talks to the nurse manager and team leader immediately after the event and feels better after seeking their support. After work, she meets a friend to go workout. Although Krista was subjected to a traumatic event, she experiences none of the attributes of PTSD.
Empirical Referents
The final step in a concept analysis is determining empirical referents. Empirical referents are actual phenomena that demonstrate the existence of the concept (Walker & Avant, 2011), and therefore are concrete representations of the concept of interest. The disorder of PTSD has been defined and classified by DSM-5, giving rise to symptom clusters, which then formed the basis for screening tools for PTSD, such as the Posttraumatic Stress Disorder Checklist (PCL-5), which is used extensively in research as a measure of PTSD symptoms (National Center for PTSD, n.d.). The PCL-5 was revised to reflect DSM-5 changes to the PTSD criteria. The PCL-5 is a self-report measure that can screen individuals by assessing the presence and severity of PTSD symptoms. The items are rated on a 5-point Likert-type scale (0 = not at all to 4 = extremely). The scale contains 20 items divided into four subscales of symptom clusters specified in the DSM-5: reexperiencing (five items), avoidance (two items), negative alterations in cognitions and mood (seven items), and hyperarousal (six items). Individuals must have at least one symptom of intrusion, one symptom in avoidance, two symptoms in negative alterations in cognition and mood, and two symptoms of hyperarousal to be indicative of PTSD. The PCL-5 has been shown to have strong internal consistency (α = .94) and test–retest reliability (r = .82), and is a psychometrically sound self-report measure of DSM-5 (Blevins et al., 2015).
Discussion
There is little found in the literature as to how PTSD applies to ICU nurses and how they experience PTSD in the workplace. The concept of PTSD as it pertains to ICU nurses is unique and should be recognized by health care professionals and hospital stakeholders to benefit the health of the nurse, patient, and organizational outcomes. Antecedents for ICU nurses consisted of a stressful work environment, where some experienced cumulative traumatic episodes, and a lack of support from coworkers, their manager, or the organization. It has been recognized for decades that a change in the workplace environment is necessary to reduce stress in the ICU (Karanikola & Mpouzika, 2018).
The prevailing defining attributes found in the literature were reexperiencing, avoidance, negative alterations in cognitions and mood, and hyperarousal. When ICU nurses suffered from these PTSD symptoms as a result of trauma in the workplace, the psychological burden was especially difficult because they spent the majority of their day in the environment where the trauma occurred (Salmon & Morehead, 2019). Furthermore, their job required them to work in a fast-paced environment and to sometimes make quick and critical decisions based on the slightest imbalance in their patients’ condition, while titrating intravenous medications, for example (Rodriguez et al., 2017). When suffering from PTSD symptoms, such as impaired cognition, a high-stress workload adds to further stress, especially if they have no tools or intervention to manage their symptoms (Park & Kim, 2013).
Consequences identified were found to affect the nurse, patients, and the health care organization. Consequences for the ICU nurse involved feelings of shame, despair, and constantly wondering what could have been done differently for their patient (Mealer et al., 2012; Ong et al., 2016). Other consequences included anxiety, depression, and burnout (Colville et al., 2017; Shen et al., 2020; Vahedian-Azimi et al., 2019). Patients suffered the repercussions of PTSD symptoms of the ICU nurses, which ranged from a bad mood, or lack of empathy (e.g., negative alterations in mood), to an angry outburst (e.g., hyperarousal), or avoidance of the patient (e.g., avoidance).
The health care organization is negatively affected by substandard job performance, poor patient satisfaction scores (leading to a decrease in government funding), and increased costs from deleterious patient care (Moss et al., 2016; Salmon & Morehead, 2019). Stress can result in cognition impairment, and reduction of stress is needed to improve nurses’ cognitive impairment (Park & Kim, 2013). Finally, the health care organization is affected by absenteeism and retention issues (Moss et al., 2016; Salmon & Morehead, 2019). Nurses may leave their job, seeking to escape the effects of their trauma. Significant costs are incurred to replace ICU nurses who choose to leave their job, and staffing issues arise from increased workload for nurses who remain (Moss et al., 2016; Salmon & Morehead, 2019).
Implications for Occupational Health Nursing
The findings of this concept analysis contribute to important implications for occupational health nursing practice. Despite the prevalence of PTSD in ICU nurses, policies addressing screening and interventions are notably lacking in our health care system. Symptoms of PTSD lasting longer than 1 month should be addressed as soon as possible to prevent manifestation of persistent symptoms and the development of anxiety, depression, and burnout syndrome (Greene et al., 2016; Mealer et al., 2009). By understanding the concept of PTSD as it relates to ICU nurses, prompt identification and diagnosis can occur, and timely treatment initiated.
Initial assessment of mental health at point of hire for ICU nurses and ongoing assessment checks can assist in early identification and prevention of PTSD. HRV can be a valuable, noninvasive measure in detection of psychological stress and assessment of the autonomic nervous system (Bornemann et al., 2019; Hourani et al., 2020). If low HRV is discerned at point of hire, nurse managers could suggest mindfulness-based cognitive training (MBCT) to mitigate psychological stress. In addition, the nurse will be better equipped to determine whether she or he is suitable for the position and working in such a stressful environment.
Although PTSD has been recognized as a critical problem in ICU nurses, there are few evidence-based interventions available in practice. The use of real-time, HRV assessment via a wearable device (e.g., a chest belt that transmits data to a wristwatch with software technology), when used in conjunction with a resilience training program, such as MBCT, can offer a much-needed intervention for ICU nurses (McCraty & Atkinson, 2012). The employment of MBCT would likely improve psychological health and result in ICU nurses having the ability to continue working in the stressful environment of the ICU and not leave their position or their profession (Salmon & Morehead, 2019). Large-scale randomized clinical trials are needed to establish the effectiveness of interventions, such as HRV assessment in conjunction with MBCT, on physical and psychological outcomes so that ICU nurses can manage the stress and trauma they must face in their work environment (Salmon & Morehead, 2019).
Lastly, a healthy work environment in the ICU must be achieved to reduce the risk of development of PTSD (Karanikola & Mpouzika, 2018; Salmon & Morehead, 2019). Managers can establish a healthy work environment and support for ICU nurses by recognizing commendable efforts on a job well done to make the nurse feel valued as an employee and allowing collaboration, ensuring their voice is heard (Happell et al., 2013). The National Institute for Occupational Safety and Health (2011) introduced the Total Worker Health Program in 2011, recognizing that workplace interventions are needed to improve the overall health and well-being of the worker. Hospital administrators, nurse managers, and occupational health nurses must work together to implement policies and interventions to reduce the risk of PTSD for their ICU nurse employees.
A limitation of this concept analysis is that it only utilized peer-reviewed articles in the English language from online research databases, leaving the potential for missed references. A paucity exists of peer-reviewed articles regarding PTSD with a strict sample of ICU nurses. A few articles included some physicians, or other ICU personnel, in study samples concerning PTSD prevalence in the realm of intensive care.
Conclusion
This concept analysis provides a better understanding of overall attributes, antecedents, and consequences, on PTSD among ICU nurses. The cases (e.g., model, borderline, and contrary cases) also illustrate the examples of ICU nurses who are experiencing PTSD and who are not. Furthermore, PTSD measurement that can be used in research studies as well as in the workplace (either by nurse managers or coworkers) to capture ICU nurses who are likely to have PTSD was provided. Conceptual clarity of PTSD in ICU nurses provides a foundation for health care professionals and hospital stakeholders to address the gap for better communication of the concept and much-needed policies and interventions to aid ICU nurses with PTSD in the burden they carry.
In Summary
The concept of PTSD as it applies to ICU nurses is unique and should be recognized by health care professionals and hospital stakeholders to benefit the health of the nurse, patient, and organizational outcomes.
The concept of PTSD in ICU nurses is unique as they are repeatedly exposed to the occupational situations contributing to this condition. Although PTSD has been recognized as a critical problem in ICU nurses, there are few policies and evidence-based interventions available in practice.
Hospital administrators, nurse managers, and occupational health nurses must work together to implement policies and interventions to reduce the risk of PTSD for their ICU nurse employees.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Paula Levi is a full-time doctoral student and National Institute of Occupational Safety and Health Fellow at the University of Alabama at Birmingham, Birmingham, Alabama, USA. She, as first author, is responsible for the research, drafting and editing of the article, and approved the final version.
Patricia A. Patrician is a professor and Rachel Z. Booth Endowed Chair in Nursing at University of Alabama at Birmingham, Birmingham, Alabama, USA. She contributed to the writing, editing, multiple revisions of the article, and approved the final version.
David E. Vance is a professor at the School of Nursing, University of Alabama at Birmingham, Birmingham, Alabama, USA. He contributed to the conceptual idea, outlining the article, writing and editing multiple revisions of the article, and approved the final version.
Aoyjai P. Montgomery is a postdoctoral fellow at the School of Nursing, University of Alabama at Birmingham, Birmingham, Alabama, USA. She contributed to the writing, editing, multiple revisions of the article, and approved the final version.
Jacqueline Moss is a professor and associate dean for technology and innovation at the School of Nursing, University of Alabama at Birmingham, Birmingham, Alabama, USA. She contributed to the conceptual idea, writing, editing, multiple revisions of the article, and approved the final version.