
Abstract
Background:
Post-traumatic stress disorder (PTSD) can result in severe depression. Yet, it is not clear how to improve health-promoting behavior and reduce depressive symptoms. This study aimed to examine whether social support mediates the link between PTSD, depression, and health-promoting behaviors.
Methods:
A cross-sectional study was conducted with 308 Korean Coast Guards in Gangwon-do, South Korea, in October and November 2020. The variables of PTSD and depressive symptoms were assessed using the Korean versions of the Impact of Event Scale-Revised and the Center for Epidemiologic Studies Depressive Scale-Revised. Health-promoting behaviors and social support were assessed using the Health-Promoting Lifestyle Profile-II and the Korean version of the Personal Resource Questionnaire 85-Part 2. Multiple regression analysis and Sobel tests were performed.
Findings:
Higher levels of PTSD symptoms and lower levels of social support were significantly associated with higher levels of depressive symptoms. Social support had a significant partial mediating effect on the association between PTSD and depressive symptoms. In addition, lower levels of PTSD symptoms and higher levels of social support were significantly associated with higher levels of health-promoting behaviors. Social support has a full mediating effect on the association between PTSD symptoms and health-promoting behaviors.
Conclusions/Application to Practice:
Our findings indicate that social support may mediate the association between PTSD symptoms and health outcomes. Occupational health nurses can use these findings to proactively develop interventions which improve social support for coast guard workers who are at risk of developing PTSD due to exposure to traumatic events on their job.
Background
The Korean Coast Guard performs various duties at maritime borders, including maritime security, maritime search and rescue, maritime traffic safety management, prevention and enforcement on maritime crimes, monitoring and control of marine pollution, and combating maritime smuggling (Bae, 2016; Korea National Statistical Korea, 2017). Therefore, they face the risk of experiencing psychological injuries due to continuous exposure to, not only physical injuries caused by violence during operations such as stopping illegal fishing, responding to maritime accidents, and crime prevention and enforcement but also to traumatic incidents such as witnessing fatalities and severe injuries from ship accidents and high-speed pursuits to arrest fleeing criminals on the run (K. H. Lee, 2017). Moreover, their isolated and confined working environments, on the sea and naval vessels, separate them from their families and social relationships (Bae, 2016).
Due to the nature of these duties, Korean Coast Guards are at a high risk of developing post-traumatic stress disorder (PTSD) (J. G. Kim & Kim, 2013; K. R. Park, 2020). The PTSD symptoms include re-experiencing the event, emotional pain, recurring memories, nightmares, desensitization, feelings of helplessness, memory impairment, and depression (Nina & Zygfryd, 2021). Prior research has shown that Korean Coast Guards show more depressive symptoms and have a lower quality of life, as they are more vulnerable due to stress and fatigue (B. D. Lee et al., 2014; J. S. Park, 2015) than other security occupational groups (B. D. Lee et al., 2014; J. S. Park, 2015). Furthermore, reports on the occurrence of depression in Korean Coast Guards over the last 5 years have revealed an age-standardized cumulative incidence of 5,524 people per 100,000, which is higher than firefighters (5,103) and police officers (4,639) (I. A. Kim & Kim, 2017). Therefore, this suggests that there is a need to investigate the relationship between PTSD and depressive symptoms among Korean Coast Guards.
Trauma related to the duties of Korean Coast Guards can induce depression (K. R. Park, 2020), and a focusing on Korean Coast Guards’ study (S. H. Kim & Lee, 2018) showed that approximately 15% of them were classified as high risk for PTSD. Furthermore, PTSD symptoms have a significant negative effect on various aspects of physical health like dietary habits, sleep habits, and degree of obesity (An, 2016). Based on prior studies reporting an inverse relationship between PTSD and physical activity (Hall et al., 2015; Jung et al., 2021), there is a need to investigate the relationship between PTSD symptoms and low levels of health-promoting behaviors among Korean Coast Guards.
In this way, PTSD symptoms have been shown to negatively affect physical and mental health, but it has been found that a high level of social support alleviates PTSD symptoms (An, 2016; Skogstad et al., 2013). This means that Korean Coast Guards with PTSD symptoms may be able to alleviate depressive symptoms and improve health-promoting behaviors through social support. Social support is gained through interactions with others to fulfill social needs; it signifies the extent to which a person perceives that they can rely on, care for, and love someone, as well as attain validation of their worth (Segrin & Domschke, 2011). Previous studies have reported that social support is an effective factor in preventing or alleviating PTSD symptoms (Moon et al., 2020) and plays a significant role in influencing health-promoting behaviors through the formation of emotionally stable social relationships (Carl & Amy, 2015).
Therefore, by identifying the mediating effect of social support on the relationship between PTSD symptoms, depressive symptoms, and health-promoting behaviors among Korean Coast Guards, this study aims to contribute to the preparation of interventions to ease depressive symptoms and improve health-promoting behaviors.
Methods
Design and Sample
This study was a cross-sectional study, and participants were recruited from the Donghae Korean Coast Guard, which has 461 Korean Coast Guards in the East Sea, Gangwon-do, South Korea. These Korean Coast Guards currently conduct maritime security, fishery protection, maritime safety, and monitoring and control activities to prevent marine pollution in the coast guard police boxes, patrol vessels, and offices (Korea National Statistical Korea, 2017). We explained the purpose of this study to the Department Head of each police station within the Donghae Korean Coast Guard in the Gangwon-do, and obtained permission to recruit from their police officer. Interested coastal police officers were recruited by posting a recruitment notice on the company bulletin board (office and intranet) at each police station (department). Written consent to participate was obtained by the researcher personally visiting the workplaces of Korean Coast Guards during inspection and break times, after explaining the research process.
This study was approved by the Institutional Review Board of Catholic Kwandong University (no. CKU-20-12-0710). All participants provided written informed consent.
Measurement
Data Collection
Data were obtained using self-reported questionnaires collected between October 2020 and November 2020. The minimum sample size required to achieve the desired statistical power level of .90, an anticipated effect size of .15 for predictor variables of outcome variables, a type I error rate of .05, and 12 predictors was 157 participants (Cohen et al., 2003; Soper, 2023). The relevant Institutional Review Board approved this study, and all participants provided written informed consent.
Sociodemographic, health-, and work-related characteristics of the participants were collected using self-reported questionnaires. The sociodemographic characteristics were age (years), gender (female/male), marital status (yes/no), and educational level (high school degree, college degree, or more).
Health-related characteristics included body mass index (BMI) (calculated from self-reported weight and height [kg/m2]), daily sleeping hours, current smoking status (yes/no), current drinking (Korea Centers for Disease Control and Prevention [KCDC], 2021) defined as drinking any alcohol at least once a month (yes/no), and physical activity of health benefit (World Health Organization, 2021) defined as engaging in any of the following: vigorous-intensity activity for at least 75 minutes/week or moderate-intensity activity for at least 150 minutes/week. Current drinking was assessed by asking participants, “How often have you drank alcohol in the past year?” with responses including: 1 = never drank, 2 = less than once a month, 3 = once a month, 4 = 2~3 times a month, and 5 = more than 4 times a month. Physical activity was assessed by asking participants (KCDC, 2020), “During a typical week, how many days and how many hours do you engage in high-intensity sports, exercise, or leisure activities that make you feel out of breath or your heart beats very quickly for at least 10 minutes straight?” and “During a typical week, how many days and how many hours do you engage in moderate-intensity sports, exercise, or leisure activities that make you feel out of breath or your heart beats very quickly for at least 10 minutes straight?”
Work-related characteristics included shift work (yes/no), work type (vessel personnel or other personnel [police box, office]), employment duration (years), weekly working hours, frequency of breaks while working, and work intensity score. Work intensity was calculated as perceived workload multiplied by work frequency (Korea Occupational Safety & Health Agency, 2022). Perceived workload was assessed by asking participants, “During the past month, how do you perceive the workload in your current work?” on a 5-point Likert-type scale (1 = very easy, 2 = easy, 3 = a little hard, 4 = hard, and 5 = very hard). The frequency of work was assessed by asking, “During the past month, how frequently have you worked?” with responses including: 1 = 1-2 times/month, 2 = 2–3 days/week, 3 = less than 4 hours/day in an average 5-day work week, 4 = not less than 4 hours/day in an average 5-day work week, and 5 = not less than 8 hours/day in an average 5-day work week.
Exposure Assessment
The PTSD symptoms were measured using the Korean Version of the Impact of Event Scale-Revised (IES-R-K), which was validated by Eun et al. (2005). This scale consists of four factors: hyperarousal, avoidance, intrusion, and sleep and numbness. The 22-item scale measures characteristic PTSD symptoms and experiences during the week preceding the impact of an event. Each item is scored on a scale from 0 (never) to 4 (very often), according to symptom frequency. Scores were calculated by summing the individual item scores. Higher scores indicated more severe PTSD symptoms. Participants with IES-R-K scores of 25 or higher were considered to have probable PTSD, whereas those with scores of 18 to 24 were considered to have probable or partial PTSD (Eun et al., 2005), respectively. The IES-R-K scores of 17 or lower were considered normal (Eun et al., 2005). Cronbach’s ɑ for the scale was .83 in a previous study (Eun et al., 2005) and .97 in this study.
Outcome Measure
Social support was measured using the Korean version of the Personal resource Questionnaire 85-Part 2 (PRQ 85-Part 2) validated by Han et al. (2002). The PRQ 85-Part 2 contains 25-item with a 7-point Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). Scores were calculated by summing the individual item scores. Higher scores indicated higher levels of social support. Cronbach’s ɑ for the scale was .90 in a previous study (Han et al., 2002) and .88 in this study.
Depressive symptoms were measured using the Korean version of the Center for Epidemiologic Studies Depressive Scale-Revised (K-CESD-R), which was validated by S. Lee et al. (2016). The 20-item scale measures the characteristic depressive symptoms and behaviors experienced during the preceding week. Each item was scored on a scale from 0 to 4 according to symptom frequency: 0 = less than 1 day/week, 1 = 1–2 days/week, 2 = 3–4 days/week, 3 = 5–7 days/week, and 4 = almost every day during the preceding 2 weeks. Scores were calculated by summing the individual item scores. Higher scores indicated more severe depressive symptoms. Participants with K-CESD-R scores of 13 or higher were considered to have probable depression, whereas those with scores of less than 13 were considered normal (S. Lee et al., 2016), respectively. Cronbach’s ɑ for the scale was .98 in a previous study (S. Lee et al., 2016) and .92 in this study.
Health-promoting behaviors were measured using the Health-Promoting Lifestyle Profile-II (HPLP-II). The HPLP-II was developed by Walker and Hill-Polerecky (1996) and translated into Korean by Cho et al. (2014). It comprises six subscales: spiritual growth, interpersonal relationships, nutrition, physical activity, health responsibility, and stress management. This scale contains 52 items on a 4-point Likert-type scale ranging from 1 (never) to 4 (routinely). Scores were calculated by averaging the individual item scores. High scores on these scales indicated higher levels of health-promoting behaviors. Cronbach’s ɑ for the scale was .91 in a previous study Cho et al. (2014) and .95 in this study.
Data Analysis
Data were analyzed using IBM SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at a p < .05. Descriptive statistics of general characteristics and main study variables (depressive symptoms, social support, health-promoting behaviors, and PTSD symptoms) are expressed as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. To examine the correlations of depressive symptoms, social support, health-promoting behaviors, and PTSD symptom variables, Pearson’s correlation analysis was performed. Multiple linear regression analysis of two models was conducted: Model-1, hypothesis testing for the mediating effect of social support on the association between PTSD symptoms and depressive symptoms; and Model-2, hypothesis testing for the mediating effect of social support on the association between PTSD symptoms and health-promoting behaviors.
The covariates in the multiple linear regression analysis of the two models were selected, based on the previous literature, with a cut-off of p < .20 from the results of the crude associations with the outcome variables (i.e., depressive symptoms and health-promoting behaviors) for hypothesis testing. All categorical covariates were dichotomously coded before inclusion in the linear regression models. Model-1 comprised multiple linear regression models for the outcome variables of depressive symptoms adjusted for age, sex, marital status, current drinking, daily sleeping hours, working type, frequency of breaks while working, and work intensity. Model-2 comprised multiple linear regression models for the outcome variables of health-promoting behaviors adjusted for age, sex, current smoking, current drinking, physical activity of health benefits, daily sleeping hours, shift work, working type, frequency of breaks while working, and work intensity.
Hypothesis testing for the mediating effect of social support was conducted using three equations and multiple linear regressions of the two models (Baron & Kenny, 1986). In Model-1, depressive symptoms (outcome) were regressed on PTSD symptoms (predictor) in the first equation, social support (outcome) on PTSD symptoms (predictor) in the second equation, and depressive symptoms (outcome) on both social support (mediator) and PTSD symptoms (predictor) in the third equation. In Model-2, health-promoting behaviors (outcome) were regressed on PTSD symptoms (predictor) in the first equation; social support (outcome) on PTSD symptoms (predictor) in the second equation; and health-promoting behaviors (outcome) on both social support (mediator) and PTSD symptoms (predictor) in the third equation. Finally, Sobel’s tests were conducted to evaluate the potential mediation of social support in the association between PTSD symptoms, depressive symptoms, and health-promoting behaviors.
Results
Descriptive Analyses
Of the 315 participants enrolled (response rate 68.3%), those with missing examination results or data (n = 7) were excluded. Therefore, 308 coast guards comprised the final sample.
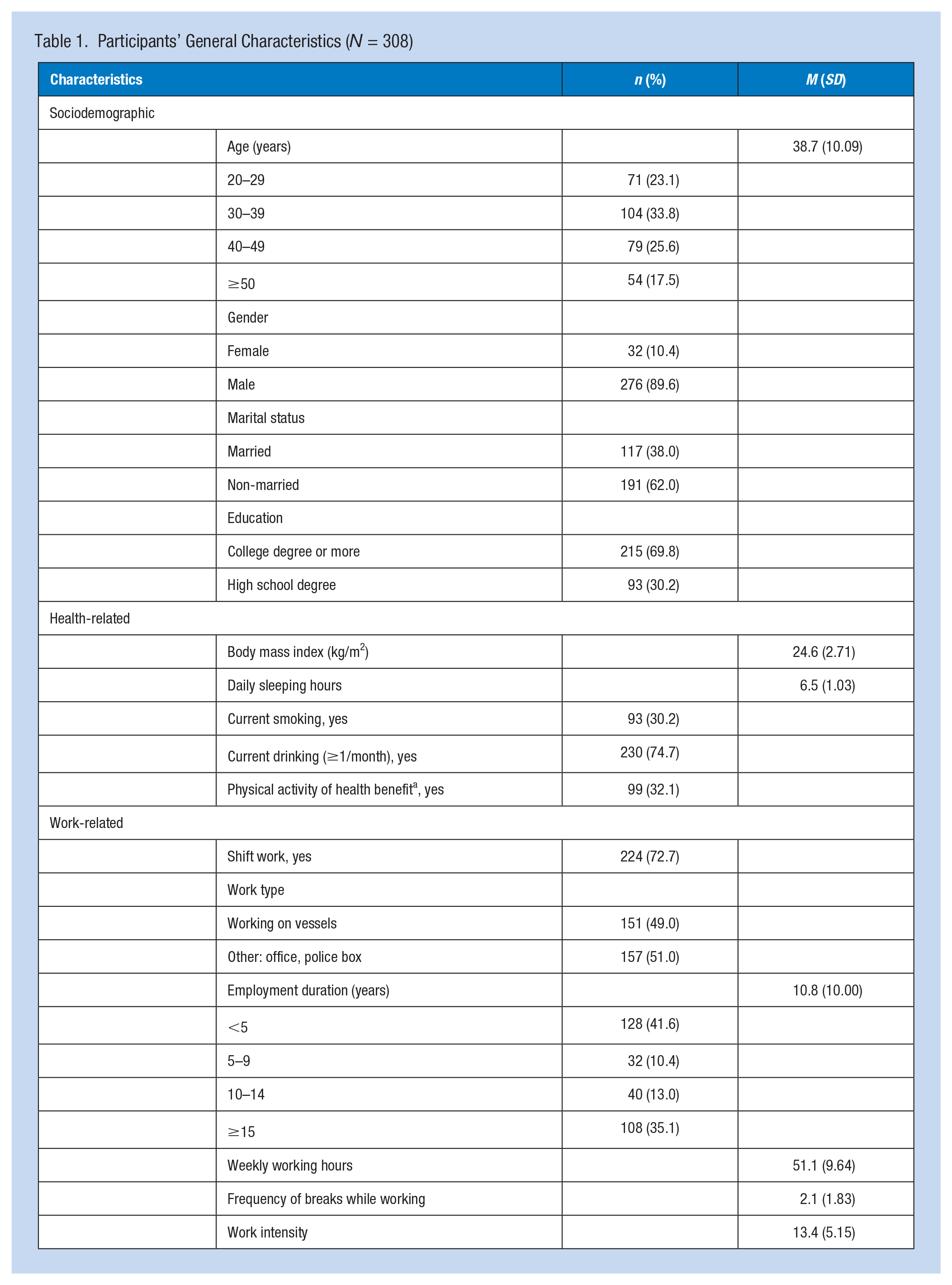
The participants in this study (N = 308) were mostly men (89.6%), 62.0% were unmarried, and 69.8% had a college degree or higher (Table 1). The mean BMI of the participants and daily sleeping hours were 24.6 kg/m2 and 6.5 hours/day, respectively. In total, 30.2%, 74.7%, and 32.1% of participants were current smokers, current drinkers, and physically active, respectively. Furthermore, 72.7% and 49.0% of the participants performed shift work and were working on vessels, respectively. The mean duration of employment was 10.8 years, and the mean weekly work time was 51.1 hours. The mean work intensity score was 13.4 (range = 1–25).
Participants’ General Characteristics (N = 308)
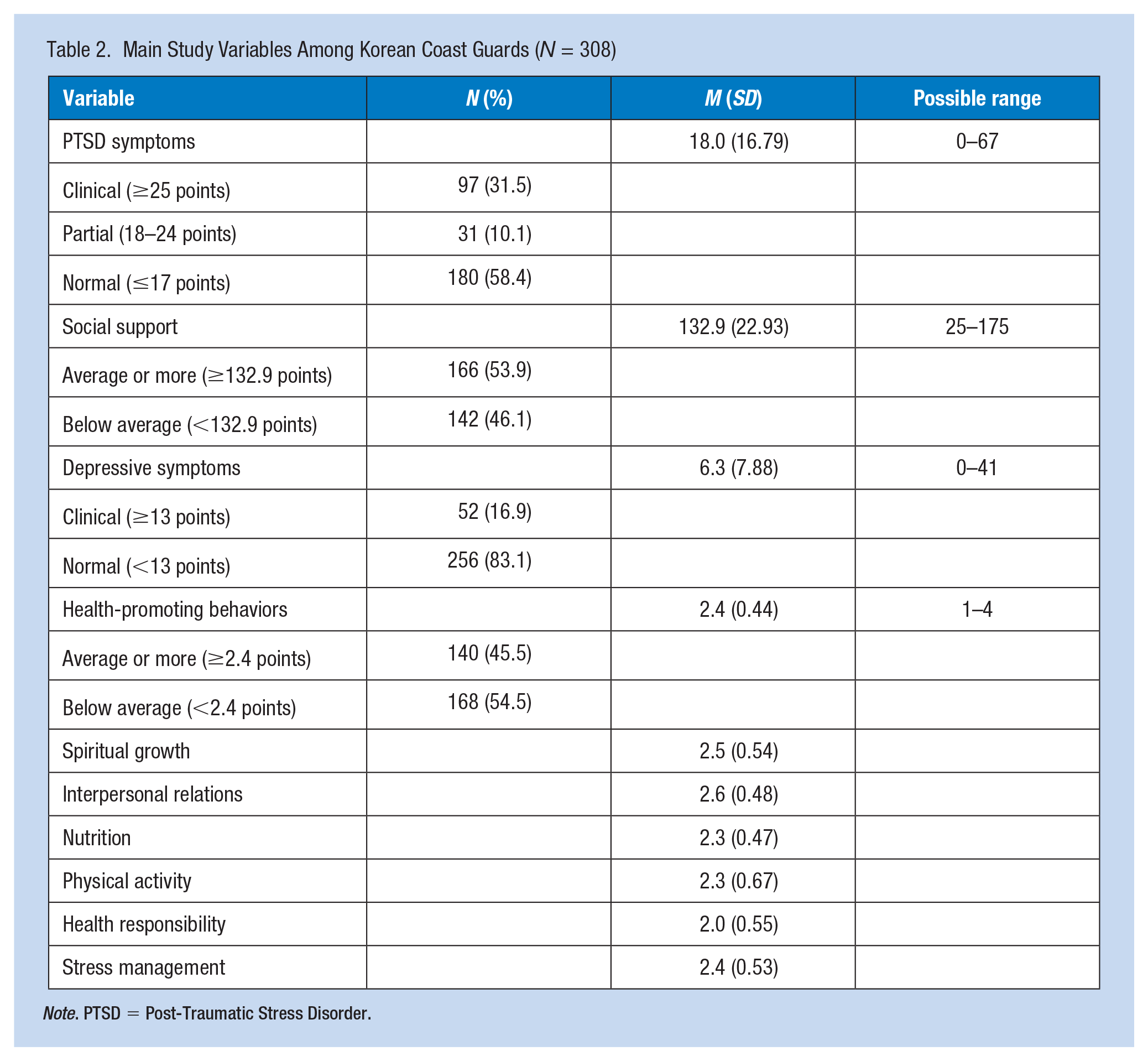
The PTSD symptoms were 31.5% and 10.1% of participants having a risk of clinical and partial PTSD, respectively (Table 2). The mean social support score was 132.9 (range = 64–175), with 53.9% having an average or more of social support. The depressive symptom was 16.9% having a risk of clinical depression. The mean total health-promoting behavior score was 2.4 (range = 1–4), with 45.5% having an average or more of total health-promoting behavior.
Main Study Variables Among Korean Coast Guards (N = 308)
Note. PTSD = Post-Traumatic Stress Disorder.
Bivariate Analyses
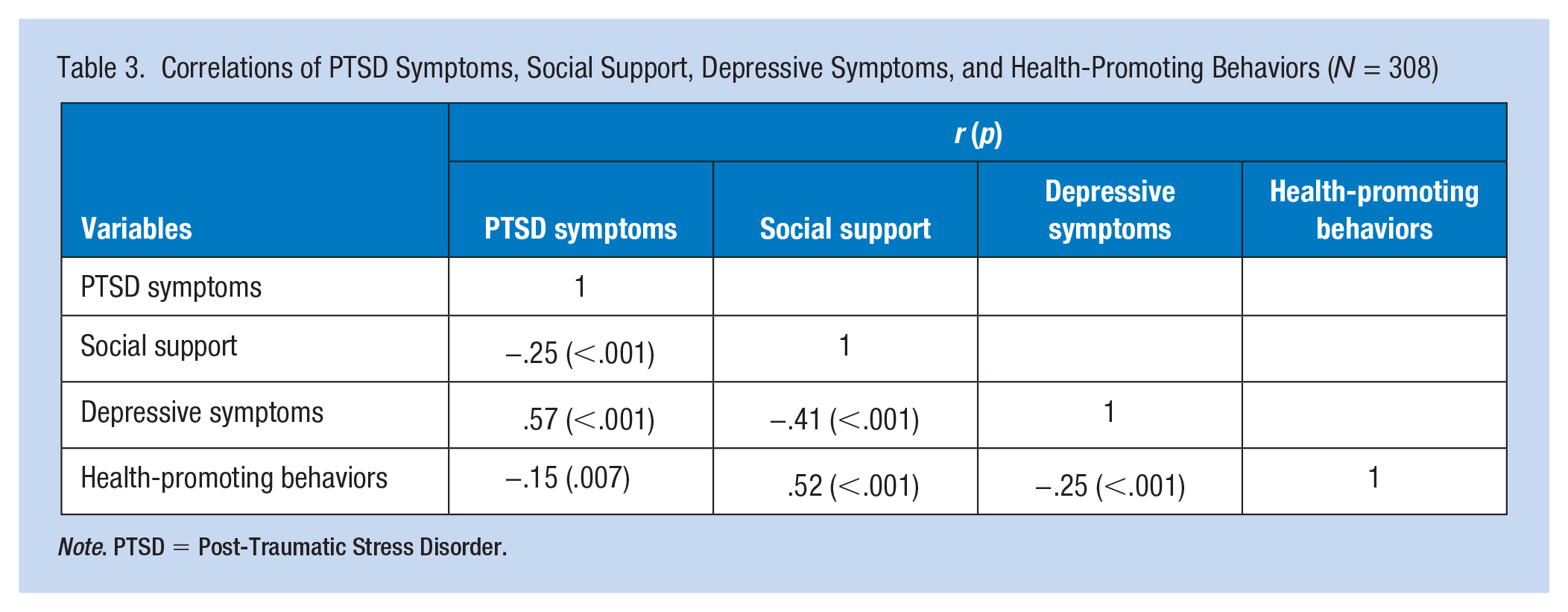
The PTSD symptoms were negatively correlated with health-promoting behaviors (r = −.15, p = .007), social support was positively correlated with health-promoting behaviors (r = .52, p < .001), and depressive symptoms were negatively correlated with health-promoting behaviors (r = −.25, p < .001) (Table 3).
Correlations of PTSD Symptoms, Social Support, Depressive Symptoms, and Health-Promoting Behaviors (N = 308)
Note. PTSD = Post-Traumatic Stress Disorder.
Multivariate Analyses
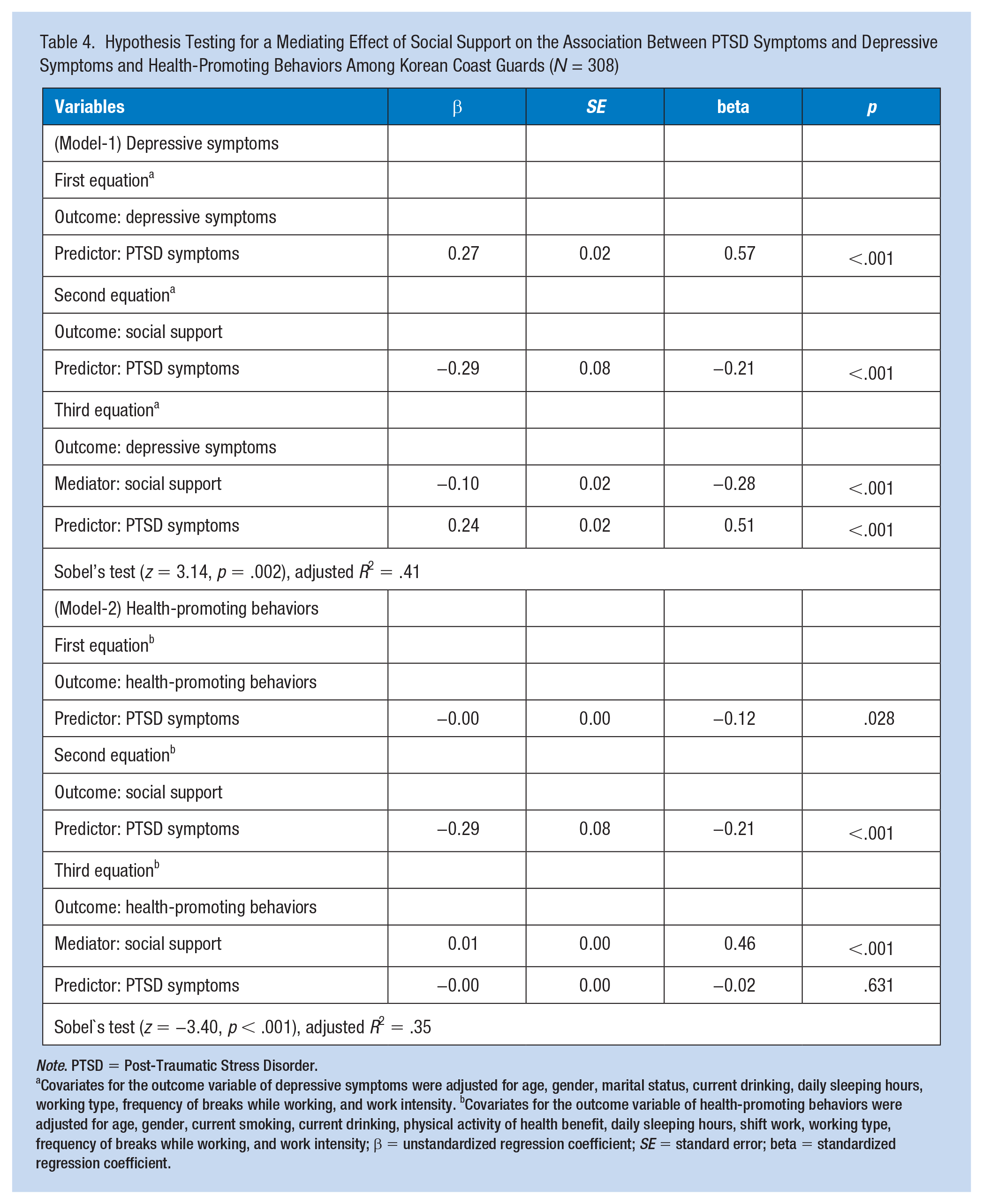
Hypothesis testing for the mediating effect of social support was conducted using three equations and multiple linear regression in the two models (Table 4).
Hypothesis Testing for a Mediating Effect of Social Support on the Association Between PTSD Symptoms and Depressive Symptoms and Health-Promoting Behaviors Among Korean Coast Guards (N = 308)
Note. PTSD = Post-Traumatic Stress Disorder.
Covariates for the outcome variable of depressive symptoms were adjusted for age, gender, marital status, current drinking, daily sleeping hours, working type, frequency of breaks while working, and work intensity. bCovariates for the outcome variable of health-promoting behaviors were adjusted for age, gender, current smoking, current drinking, physical activity of health benefit, daily sleeping hours, shift work, working type, frequency of breaks while working, and work intensity; β = unstandardized regression coefficient; SE = standard error; beta = standardized regression coefficient.
Model-1 hypothesis testing for the mediating effect of social support on the association between PTSD and depressive symptoms was evaluated using three equations. In the first equation, PTSD symptoms were significantly positively associated with depressive symptoms (β = 0.27, p < .001). In the second equation, PTSD symptoms were significantly negatively associated with social support (β = −0.29, p < .001). In the third equation, regressing depressive symptoms (outcome) on both PTSD symptoms (predictor) and social support (mediator) met the three requirements for a partial mediating effect of social support: (a) social support was significantly associated with depressive symptoms (β = −0.10, p < .001); (b) the β for the association between PTSD symptoms and depressive symptoms from 0.27 in the first equation (direct relationship of PTSD symptoms on depressive symptoms, Figure 1A) to 0.24 in the third equation (indirect relation of PTSD symptoms on depressive symptoms via social support, Figure 1B). The association in the third equation remained significant (β = 0.24, p < .001), and (c) Sobel’s test showed a significant mediating effect of social support (z = 3.14, p = .002). Social support accounted for 41% of the variance in depressive symptoms.
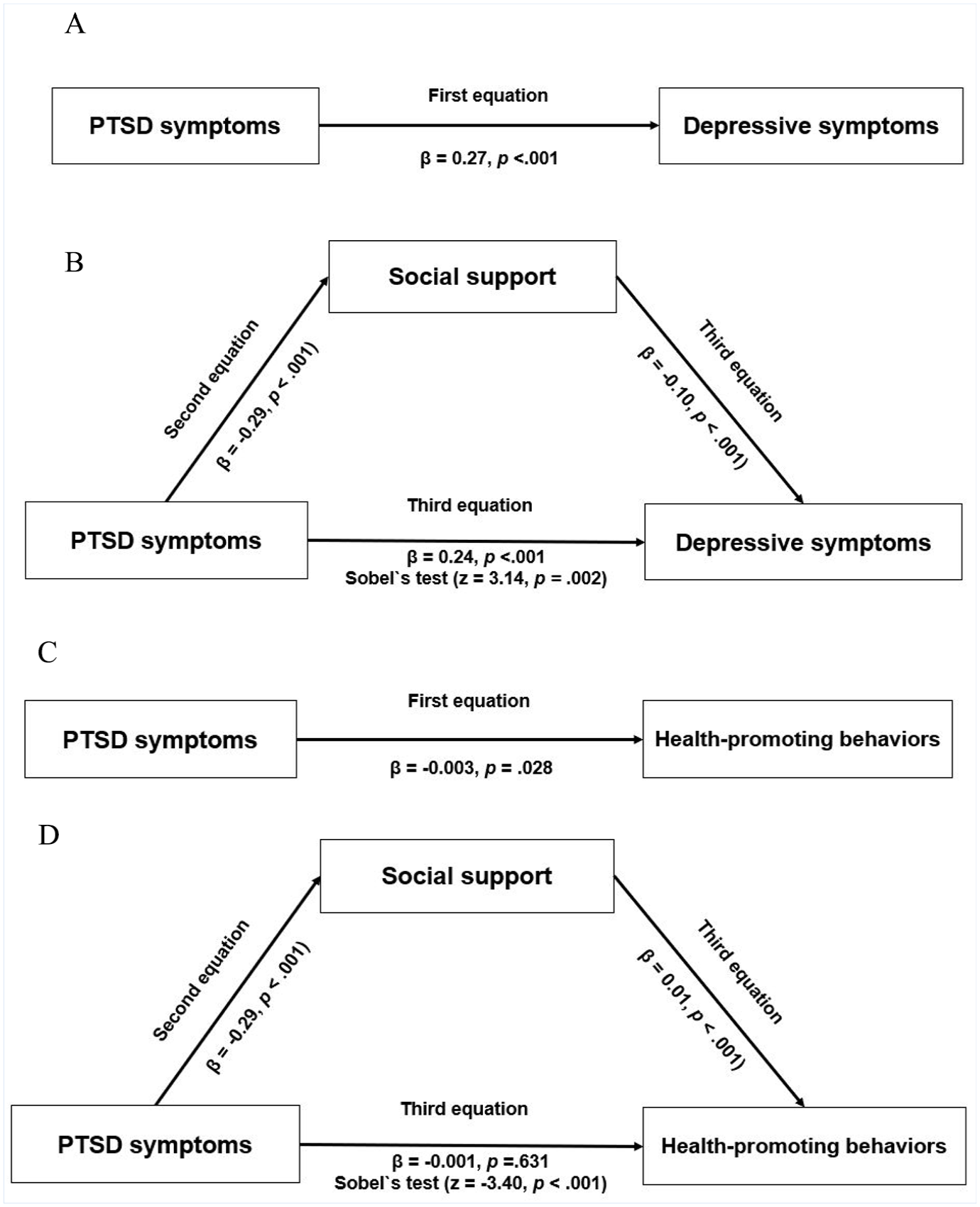
(A) Direct Pathway From PTSD Symptoms to Depressive Symptoms; (B) Indirect Pathway From PTSD Symptoms to Depressive Symptoms via Social Support; (C) Direct Pathway From PTSD Symptoms to Health-Promoting Behaviors; (D) Indirect Pathway From PTSD Symptoms to Health-Promoting Behaviors via Social Support.
Model-2 hypothesis testing for the mediating effect of social support on the association between PTSD symptoms and health-promoting behaviors was also evaluated using three equations. In the first equation, PTSD symptoms were significantly negatively associated with health-promoting behaviors (β = −0.003, p = .028). In the second equation, PTSD symptoms were significantly negatively associated with social support (β = −0.29, p < .001). In the third equation, regressing health-promoting behaviors (outcome) on both PTSD symptoms (predictor) and social support (mediator) met the three requirements for a full mediating effect of social support: (a) social support was significantly associated with health-promoting behaviors (β = 0.01, p < .001); (b) the β for the association between PTSD symptoms and health-promoting behaviors ranged from −0.003 in the first equation (direct relationship of PTSD symptoms on depressive symptoms, Figure 1C) to −0.001 in the third equation (indirect relation of PTSD symptoms on depressive symptoms via social support, Figure 1D). The association in the third equation was not significant, and (c) Sobel’s test showed a significant mediating effect of social support (z = −3.40, p< .001).
Discussion
In this study, PTSD symptoms showed the high-risk (clinical) group, accounted for 31.5% of the participants. This was somewhat lower than the findings of a PTSD survey conducted by the Ministry of Public Safety and Security (2016), which demonstrated a high-risk group of 37.3. The high risk for PTSD symptoms among coast guard personnel compared to other occupational groups could be attributed to the unique and constrained work environment of maritime operations. The psychological burden of responding to emergencies in a maritime setting, coupled with the inherent risks of seafaring duties, where self-protective measures are inherently limited, likely contributes to this phenomenon (T. R. Lee & Chang, 2019).
We also found that the risk group for clinical depression symptoms in Korean Coast Guard was 16.9%. In a previous study that utilized the same tool, compared to other occupational groups, the risk group among the police officers in shifts was 25.7% (M. S. Kim, 2021), while firefighters were 34.4% (G. S. Kim et al., 2014). This finding differs from the results of the National Health Insurance Service, which showed that the prevalence of depression among Korean Coast Guard was higher than that among firefighters and police officers (I. A. Kim & Kim, 2017). According to previous studies, police officers tend to deny experiencing extreme stress and perceive psychological difficulties as a personal vulnerability (J. P. Park & Kim, 2016; Reavley et al., 2018). Moreover, there is a high likelihood that they will not actively disclose their mental and psychological issues because of concerns about social stigma and potential negative career consequences (I. A. Kim & Kim, 2017; J. Y. Lee et al., 2017; K. H. Lee & Lee, 2013). Considering organizational characteristics, it may be necessary to consider the possibility of defensive responses to questions related to depression.
Since depression is characterized by persistent mood decline, decreased motivation and interest, lethargy, anxiety, and reduced concentration (Kennedy, 2008) it may be that coast guards experiencing depression may encounter challenges that negatively impact their job performance, resulting in work impairment and difficulties maintaining concentration (Reavley et al., 2018). Furthermore, depression has been recognized as both a direct and indirect contributor to suicidal thoughts and suicide and is a primary symptom of PTSD. Approximately 60% of individuals who die by suicide are found to have experienced major depressive disorder or related conditions (Joe et al., 2006). Hence, actively managing the psychological well-being of professions like the Korean Coast Guard, which face heightened risks of PTSD and depression, becomes imperative.
We also observed a significant partial mediating effect of social support between PTSD and depressive symptoms. The Buffering Hypothesis suggests that social support from others influences the appraisal process of individuals in response to life events, mitigating the negative effects of stress and aiding in adaptation. It has been indicated that social support plays a significant role in preventing or alleviating mental health issues such as depression (Raffaelli et al., 2013). These findings also allow for the interpretation that social support may have served as a buffering mechanism, lowering the depressive score among the subjects, by mitigating the relationship between higher PTSD symptom score within the Korean Coast Guard and elevated depressive symptom score. According to a study on the impact of PTSD on firefighters’ physical and mental health, it was observed that social support played a role in alleviating and regulating certain aspects of PTSD symptoms (An, 2016). In addition, a systematic literature review of work-related PTSD reported that low social support increased the risk of PTSD symptoms (Skogstad et al., 2013). Social support can serve as an effective intervention for PTSD, contributing to the prevention, recovery, and improvement of both physical and mental well-being through the establishment of positive and healthy social relationships. In particular, occupational health nurses can develop evidence-based intervention strategies to facilitate social support from supervisors and between co-workers for promoting the health of the Korean Coast Guard (H. J. Kim & Choo, 2018).
In this study, the level of health-promoting behaviors significantly decreased as the level of PTSD symptoms increased. This suggests that individuals with PTSD symptoms may experience a decrease in appetite, lack of energy, and feelings of lethargy, making it difficult to maintain healthy habits. According to a systematic literature review on the relationship between PTSD symptoms and physical activity and dietary habits (Hall et al., 2015), there may be a negative association between PTSD and physical activity and dietary habits, which is consistent with the findings of this study. Previous studies have addressed the relationship between PTSD and unhealthy behaviors (e.g., smoking and alcohol/drug abuse), but relatively few studies have investigated the relationship between PTSD and health-promoting behaviors (Hall et al., 2015). Hence, it is necessary for more studies to be conducted regarding the correlation and impact of PTSD symptoms on health-promoting behaviors. Our study showed a significant mediating effect of social support on the relationship between PTSD and health-promoting behaviors. Social support was also identified as significant variable influencing health-promoting behaviors in a study on Korean Navy soldiers (I. A. Kim et al., 2017). A study investigating the relationship between health-promoting behaviors and social support in men (Sanaati et al., 2021) also showed that social support has a direct influence on health-promoting behaviors, underpinning the findings of this study.
The increasing PTSD symptoms among Korean Coast Guard personnel were influenced not only by individual characteristics but also by support from family and colleagues, the work environment, and culture (Moon et al., 2020). Therefore, for effective interventions to promote health, it is important to focus not only on individual characteristics but also on various factors such as support from family, organizations, local communities, and social networks. To reduce depressive symptoms and enhance health-promoting behaviors, it is crucial to strengthen social support and establish practical measures for prevention and management within the workplace. Currently, the Korean Coast Guard has systems and programs for mental health established. Since 2014, a psychological counseling program has been in operation to manage PTSD symptoms, which includes education on PTSD and individual counseling through one-to-one sessions and mindfulness care camps (Moon et al., 2020). However, there is low program participation, as many individuals may not perceive the necessity of program involvement or try to handle their issues privately due to concerns about how they might be perceived by others (T. R. Lee & Chang, 2019). Therefore, regardless of the severity of depression, it is considered essential to prioritize cultural and therapeutic shifts within the Korean Coast Guard regarding mental health care. Organizational-level efforts are needed to improve awareness and promote education regarding both physical and mental health among the Korean Coast Guard personnel.
Limitations
The generalizability of this study’s findings is limited because it targeted only a subset of the Korean Coast Guard. Therefore, future research should include a broader sample of coast guard personnel working in various regions or conduct comparative analyses with similar occupational groups at risk for PTSD. In addition, it is crucial to consider not only individual characteristics but also the interpersonal and organizational factors surrounding them to understand the factors influencing depression and health-promoting behaviors at multiple levels in future research. Furthermore, we propose conducting follow-up studies to explore specific approaches that can enhance social support for individuals identified as high risk for depression and PTSD symptoms. Such studies could help identify concrete measures to strengthen social support among target participants.
Implications for Occupational Health Nursing Practice
Social support plays an important role in the relationship between psychological health (e.g., PTSD and depressive symptoms) and health-promoting behaviors. This study found that PTSD symptoms were linked to the adverse outcomes of depressive symptoms and decreased health-promoting behaviors among the Korean Coast Guard. Social support had a mediating effect on the relationship between PTSD symptoms and health outcomes. We also found that social support plays a full mediating role between PTSD symptoms and health-promoting behaviors that lead to positive health outcomes such as optimal well-being, personal fulfillment, and productive living (Walker & Hill-Polerecky, 1996). Occupational health nurses should consider social support strategies to strengthen workers’ social networks when developing health promotion programs for workers who experienced PTSD in the workplace. For example, social support interventions may include talking therapies or soft skills such as empathy and emotional expression, facilitated through peer-mentoring programs in the workplace (Waqas et al., 2021). Meanwhile, Korean Coast Guards, who are frequently exposed to traumatic events, neglect their own health management because of the negative connotations surrounding the focus and passive organizational climate of psychological health management (S. A. Lee & Jang, 2019). To provide active intervention for workers who are frequently exposed to traumatic events, it is necessary to enhance awareness within the organization. Therefore, occupational health nurses should implement social support strategies that consider their organizational characteristics and working environment to improve the health outcomes of workers who have experienced traumatic events.
Applying Research to Occupational Health Practice
We found that social support plays a role as a partial mediator in the relationship between PTSD and depressive symptoms and as a full mediator in the relationship between PTSD symptoms and health-promoting behaviors among the Korean Coast Guard in the East Sea, South Korea. In other words, post-traumatic stress may cause negative outcomes in psychological health and health behaviors, and social support plays a mediating role in these relationships. Therefore, social support may provide interventional insights to reduce negative health outcomes among workers experienced to post-traumatic stress. In particular, occupational health nurses should develop intervention strategies for social support to prevent diseases among workers who are easily experienced to PTSD due to disasters and accidents. The findings of this study may help develop intervention strategies aimed at fostering organizational-level social support. These interventions would serve to promote the well-being of workers who may be susceptible to PTSD following disasters or accidents.
Footnotes
Acknowledgements
The authors thank the contribution of the Donghae Coast Guard station in the East Sea, Gangwon-do, South Korea.
Author Contributions
H-JK contributed to the study conceptualization, funding acquisition, data curation, formal analysis, investigation, methodology, project administration, supervision, and manuscript draft. H-ES and MY contributed to the study conceptualization, formal analysis, methodology, and manuscript draft. All authors were involved in the manuscript review, revision, and final approval process.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Research Foundation of Korea (NRF) grant by the Korea government (no. NRF-2019R1G1A1100800).
Ethical Approval
This study was approved by the Institutional Review Board of Catholic Kwong University (no. CKU-20-01-0710) on October 28, 2020.