
Abstract
Background:
Immigrants often work in jobs that are known as dirty, demanding, and dangerous. Globally, the agricultural occupations have been associated with the emergence of chronic kidney disease of unknown etiology (CKDu) primarily in outdoor worker populations. The disease has also been reported in immigrants in the United States who work in agricultural occupations, but little research has been done outside of agricultural workers to determine whether immigrants who work other occupations are at risk for developing CKDu.
Methods:
This study assessed the self-reported occupational histories of undocumented immigrants receiving frequent, emergent-only dialysis in Atlanta, GA. We assessed demographics, employment status, and work history, using the Grady Dialysis Questionnaire and the Occupational/Environmental Health History Form.
Results:
Fifty undocumented immigrants receiving frequent, emergent-only hemodialysis were recruited for this study. The average age was 49.5 years (SD ± 11.5), and the majority (52%) were female and originated from Mexico (66%). A majority (74%) reported having worked in the past 5 years and 28% reported currently working. A total of 68 unique jobs were reported. In decreasing order of frequency, our sample worked in occupations with documented renal toxicant exposures, such as applying pesticides in landscaping, heat exposure in agriculture, construction, landscaping, and dry cleaning, and lead paint fumes in construction.
Discussion:
Occupational histories provide a greater understanding of the exposures and working conditions of those receiving frequent, emergent-only hemodialysis. This exploratory study suggests that further research is needed to investigate and assess whether renal toxicants are associated with occupations with high numbers of undocumented workers.
Application to Practice:
A detailed and thorough occupational history should be conducted from those receiving frequent, emergent-only hemodialysis. Developing continuing education for nursing and medical staff in dialysis centers on taking an occupational history, mandatory State reporting requirements, and hazard communication training for workers should be considered. Collaborations between occupational health professionals, public health authorities, employers, dialysis providers, and clinicians who see undocumented workers is required to understand and develop appropriate prevention measures for this population.
Background
In 2019, the Bureau of Labor Statistics reported that 28.4 million immigrant workers were a part of the United States’ workforce, and approximately half of these workers were Latinx (Bureau of Labor Statistics, 2020). Approximately 7 million immigrant workers in the United States are undocumented (Svajlenka, 2020). Undocumented workers are recognized as one of the most vulnerable groups in society and often have jobs that are known to be “3-D” or dirty, dangerous, and demanding (Moyce & Schenker, 2018). When compared with documented workers, undocumented workers in the United States have been found to experience increased physical strain, greater exposure to environmental conditions and are more likely to work at a height (e.g., in roofing; Hall & Greenman, 2015; Moyce & Schenker, 2018). Furthermore, immigrants working outdoors have experienced acute kidney injury (AKI) during agricultural work shifts in both Florida (Mix et al., 2018) and California (Moyce et al., 2016, 2020).
Clinically, repeated AKI over time can lead to the development of chronic kidney disease (CKD) and, ultimately, end-stage renal disease (ESRD) requiring renal replacement therapy through hemodialysis (Chawla et al., 2014; Hsu & Hsu, 2016). This pathophysiological mechanism has been implicated in the development of CKD of unknown etiology (CKDu) that has been studied in multiple agricultural communities globally (Orantes-Navarro et al., 2017). However, there is a gap in the literature regarding the association between occupational heat exposure and renal functioning of undocumented workers in nonagricultural occupations (Smith et al., 2021). To address this gap, we sought to investigate the past occupational histories of undocumented immigrants receiving frequent, emergent-only hemodialysis at a single urban safety-net hospital in Atlanta, GA. The purpose of this study was to describe the work histories of undocumented workers with ESRD and investigate the potential association of occupational heat exposure with developing ESRD in this population.
Methods
This cross-sectional descriptive study examined the frequency of occupational heat exposure in undocumented immigrant workers obtaining emergency hemodialysis in Atlanta, Georgia between March and June 2019 at a local safety-net hospital, which funds the emergency dialysis for undocumented individuals with funds from the Emergency Medical Treatment and Labor Act (EMTALA).(Cervantes et al., 2018; Rodriguez, 2015) Since, EMTALA is intentionally vague in the language used within the policy, the implementation of EMTALA is mostly facility dependent (Brown & Brown, 2019) . Persons who present for emergent dialysis care, can enter the emergency department at any time of day for screening for the need of dialysis and treatment. However, since emergency dialysis is the only mechanism of dialysis available to undocumented immigrants in Georgia, our clinical partner has created a nurse practitioner (NP) led emergent dialysis program where undocumented immigrants can receive dialysis as needed through the emergency department. In spite of the removal of most barriers to access dialysis, the patients are not guaranteed to be dialyzed at the optimum schedule of 3 days a week; the majority receive dialysis twice weekly.
All patients who received dialysis in the NP—run program—were eligible and approached to participate in the study. Potential participants were anyone that received emergent-only hemodialysis from March 2019 to June 2019 at our local safety-net hospital. During this period, the emergency dialysis center provided emergent-only hemodialysis to approximately 122 individuals who live and work in the surrounding community. The research team recruited participants within the emergent dialysis facility on 6 out of 7 days of the week (Monday thru Saturday) between 9 am and 2 pm while participants waited for their dialysis treatment. Furthermore, a snowball recruitment method allowed participants to identify peers who would be willing to participate in the study. Given the nature of emergent-only hemodialysis in the United States, all those receiving emergent-only hemodialysis were assumed to be undocumented (Cervantes et al., 2020; Rodriguez, 2015) and no one was directly asked their documentation status.
Compensation was not provided for participating in this study. Persons who were willing to participate in this study were provided informed consent in a private room of the dialysis facility by a bilingual (English<>Spanish) research assistant in the language of choice of the participant. The consent form was translated by a certified English<>Spanish translator and participants were provided a copy of the consent in their language of choice. The study was approved by the Emory University Institutional Review Board and the Grady Memorial Health System Review Board.
Data Collection
We utilized the Grady Dialysis Questionnaire, which was adapted from the Questionnaire for Heat-Related Illness Among Migrant Farmworker Populations in Southern Georgia (Fleischer et al., 2013) and the Farmworker Occupational Hazards Survey (Mix et al., 2018), to collect demographic information and self-reported occupational history pertaining to occupations of interest (e.g., agriculture, landscaping, construction, housekeeping/cleaning, and factory work). These survey tools have been administered to English and non-English speaking (i.e., Spanish and Haitian Creole) immigrant workers in both Florida and Georgia. Demographic variables included age in years, gender identity (male/female), primary language (English/Spanish), country of birth, years of education, have worked in last 5 years (yes/no), and currently working (yes/no). In addition, we inquired about the current industries of those working, having a history of working in the Southeastern United States (yes/no), the days worked per week and hours per day for those currently working, as well as having access to shade regular breaks, a lunch break, medical attention, and a toilet at work. The Occupational/Environmental History Form (Taking the Occupational History, 1983) was used to collect job-specific information, such as length of employment, industries ever having worked in, and known/perceived workplace hazards and exposures. Bilingual research assistants verbally administered surveys in either English or Spanish while participants waited for dialysis treatment or during dialysis treatment (based on participant preference).
Data Analysis
Survey data were stored in REDCap, a secure, online platform for data storage. Data were analyzed using R (version 3.5.3) for descriptive statistics which included calculating means and proportions for sociodemographic and occupational characteristics. Topic modeling was performed on free text within the Occupational/Environmental History form.
The text data collected using Occupational/Environmental History form (Taking the Occupational History, 1983) were prepared into a textual corpus for analysis by translating all text to English via a certified English-Spanish translator, where applicable; converting all text to lower case; removing extra white space, numbers, punctuation, and stop words; and assigning a unique ID to each word. Converting all words to lower case prevents letter case from affecting how a word is incorporated into the model. For example, “low” and “Low” would not be counted as two separate words (Yang & Zhang, 2018). In addition, the corpus was lemmatized (i.e., words in the corpus were stemmed to their root) to prevent the proliferation of words with similar meanings in the topic model (May et al., 2016). Please see the Supplemental Appendix A for more detailed information about the Topic Modeling methods that were used.
Results
Recruiters approached 70 participants. However, 20 declined to participate due to uncertainty about the study and its impact on their ability to receive care. Fifty (n = 50) persons agreed to participate in the study. The average age of participants receiving frequent, emergent-only hemodialysis was 49.5 years old with the majority identifying as female (52%). Almost all of the participants n = 49 (98%) identified as Latinx and the majority originated from Mexico (72%). Spanish was the primary language spoken. Approximately three quarters (74%) reported having worked in the last 5 years but only one quarter were currently working (28 %; Table 1).
Sociodemographic, Housing, and Basic Work History Characteristics, n = 50
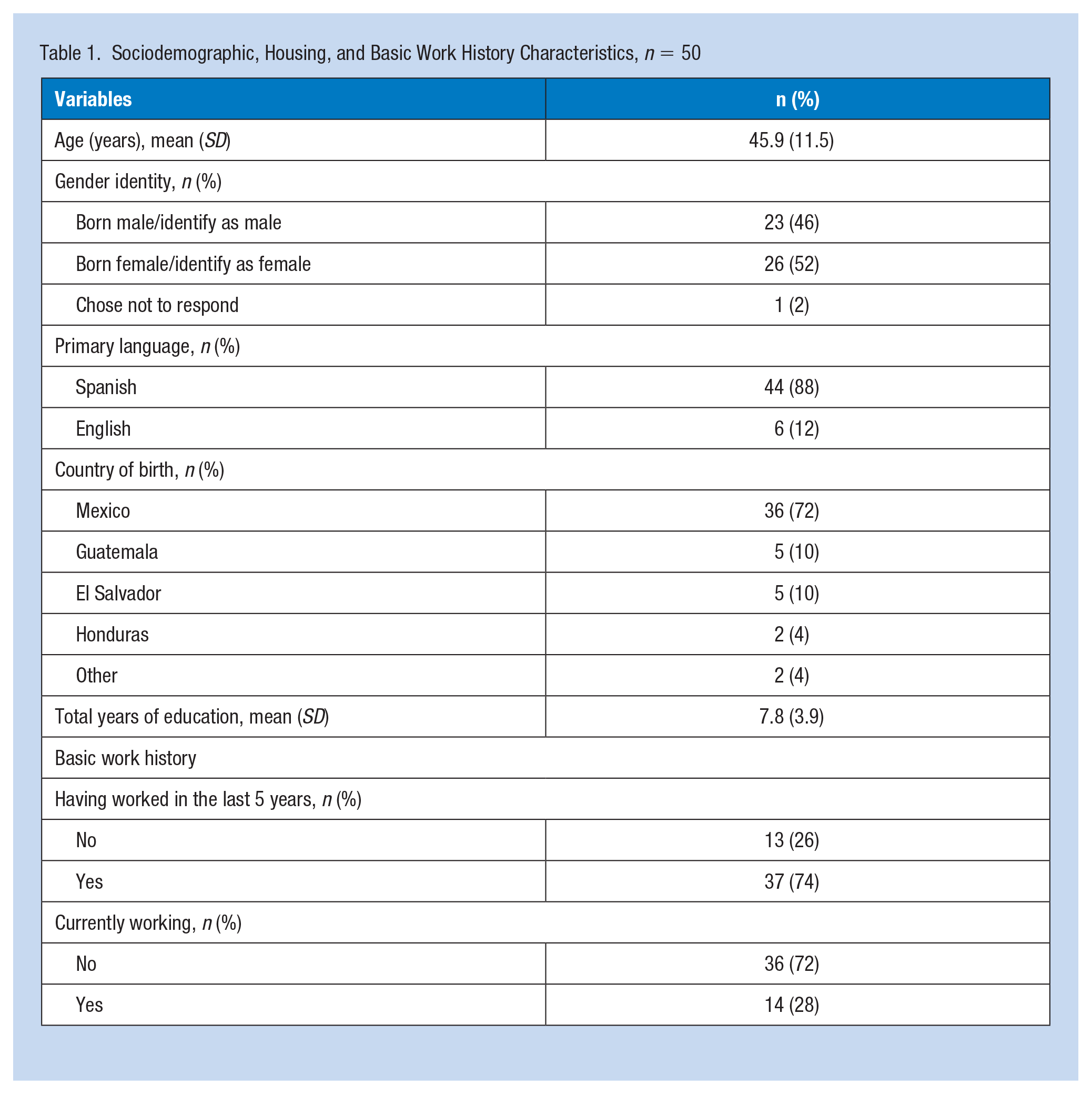
Of those currently working (n= 14), six (43%) worked in construction, three (21%) in housekeeping/cleaning, two (14%) in the restaurant industry, and three (7%) in industries classified as “other.” The majority of those currently working 12 (86%) reported having access to shade, 13 (93%) regular breaks, 10 (71%) lunch breaks, 13 (93%) any form of medical attention, and 11 (79%) had a toilet at work. They reported a total of 26 different, current jobs. Everyone interviewed as part of this study reported ever having worked with 14 (28%) reported past work in agriculture, 21 (42%) in construction, n = 10 (20%) in landscaping, 28 (56%) in housekeeping/cleaning, and 14 (28%) in a factory/processing plant. In addition, those having ever worked reported working in a total of 68 unique jobs (Table 2).
Occupational Histories of Undocumented Immigrants Receiving Frequent, Emergent-Only Hemodialysis
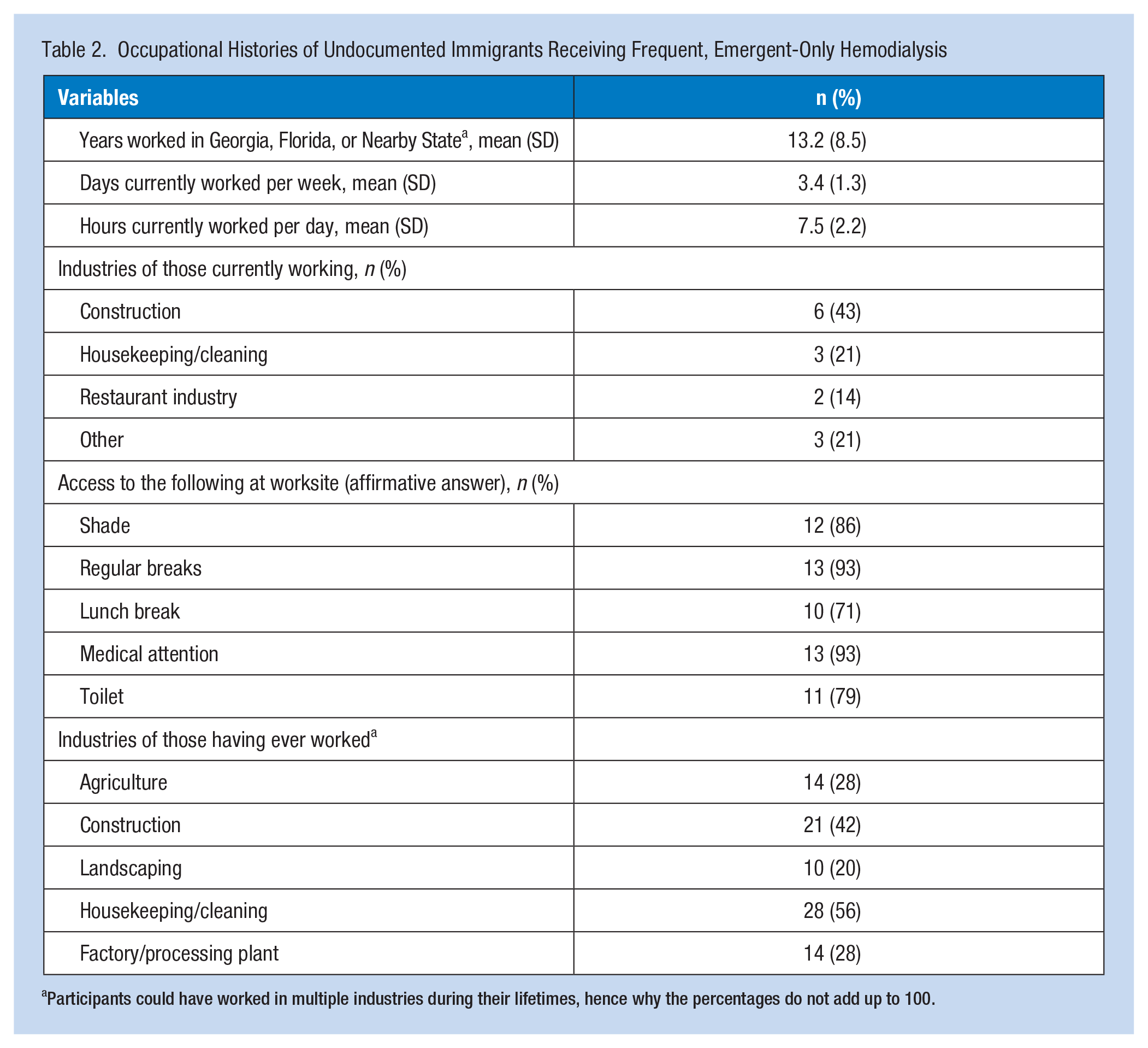
Participants could have worked in multiple industries during their lifetimes, hence why the percentages do not add up to 100.
Topic Modeling Findings
During our analysis of the Occupational/Environmental History Form (Taking the Occupational History, 1983), which analyzed the various industries and tasks performed across a participant’s career, two main topics were present in the reported histories: indoor workers and outdoor workers (Figure 1). Within the indoor work model, the top five terms (i.e., word stems) were “clean,” ‘restaur’ [restaurant], “glove,” ‘none,’ and “cook.” The top five terms (i.e., word stems) of the outdoor work model were “construct” [construction], “glove,” ‘mask “everyth” [everything], and “work.” The two topics both mentioned “construct” [construction], “glove,” ‘mask “hous” [house], and “work.”
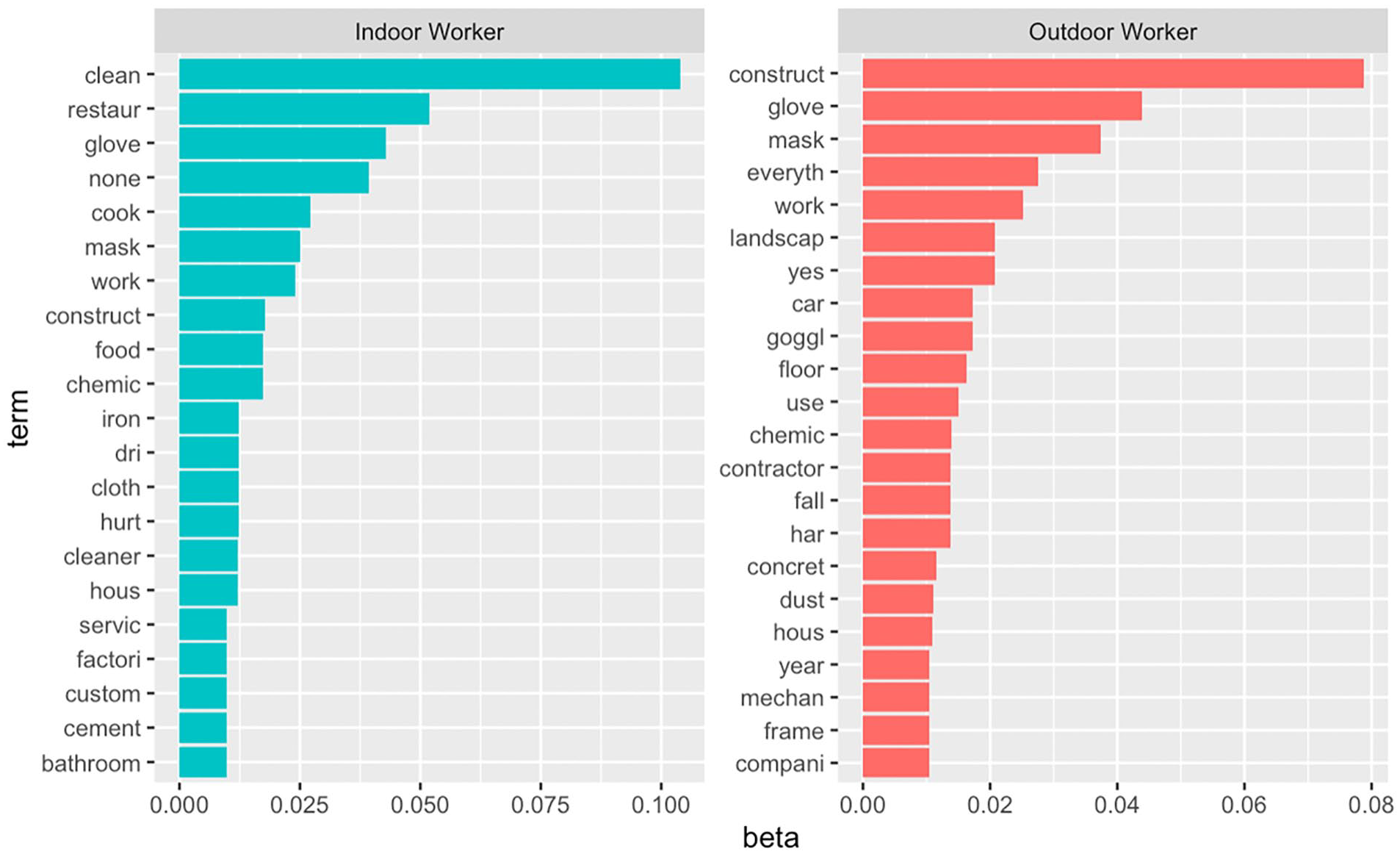
Topic modeling results showing two distinct topics in the occupational histories of participants.
We suspect that stem “construct” appears twice due to those working in construction and in housekeeping/cleaning both reported working on construction sites. A portion of those who worked in housekeeping/cleaning reported cleaning the interiors of construction sites post-completion but were not categorized as working in construction if they were not physically building the infrastructure of interest. A similar phenomenon is likely occurring with the keyword “hous” [house] as there were people both constructing houses and cleaning houses. However, the fact that this happened provides some credibility to the topics produced from our unstructured data. If an appropriate model is produced, similar terms such as “housing construction” and “house cleaning” should be placed into separate topics as their underlying meaning is distinct and they reflect two separate underlying topics (McFarland et al., 2013).
Discussion
Participants of this study had two distinct topics (i.e., industry types) in their work histories; this knowledge promotes a better understanding of the work histories reported by those receiving frequent, emergent-only hemodialysis. The identification of two industry types provides evidence that prevention efforts to protect workers from the negative impacts of occupational heat exposure must be driven based on the unique needs of the occupational group of interest. For example, heat exposed workers in construction and landscaping could experience AKI at work like agricultural workers (Smith et al., 2021). However, there is the potential for occupational heat exposure, and subsequent kidney dysfunction, to be even greater for construction workers and landscapers due to the urban heat island effect (Heaviside et al., 2017).
To our knowledge, all studies that have been conducted in the United States describing the impacts of occupational heat stress on renal functioning in Latinx workers have been conducted with agricultural populations (Smith et al., 2021). In our sample, of those currently working, half reported working in construction and landscaping, occupations with known occupational heat exposure (Kearney et al., 2013; Levi et al., 2018) but the impact of heat on the workers’ renal function has not been studied. Work has been done to investigate the renal impacts of occupational heat exposure in countries other than the United States in construction workers (Al-Bouwarthan et al., 2020; Wesseling et al., 2016), miners (Donoghue et al., 2000), and manufacturing workers (Flouris et al., 2018; Venugopal et al., 2016). For future research, it will be important for studies to be conducted describing the effects of occupational heat effects on workers within the United States outside of agriculture. For example, Al-Bouwarthan et al. (2020) conducted research on construction workers in Saudi Arabia, which has a vastly different climate than that of the Southeastern United States, particularly Georgia, where this study took place.
In addition, upon further analysis, those who reported working in housekeeping/cleaning, specifically in dry cleaning environments, reported high heat conditions at work. Likewise, other indoor workers can be heat exposed, such as in the restaurant industry (Varghese et al., 2018), could potentially develop kidney disease through a similar pathophysiological process and should not be ignored by occupational health practitioners and researchers. This evidence highlights the complex needs of workers across occupations, therefore, single prevention efforts that have shown to be effective in rural agricultural workers, such as cooling vests (Chicas et al., 2021) and ensuring adequate water, rest, and shade (Wegman et al., 2018), may not be sufficient and may need to be utilized in tandem with each other to prevent morbidity and mortality related to occupational heat exposure in urban workers.
An occupational health hazard analysis is a tool that may be beneficial to ensure that adequate assessments of occupational hazards, such as heat exposure, are completed (Roughton & Crutchfield, 2016). Occupational hazard assessments allow for the identification of risk and the mitigation of risk to improve occupational well-being (Gan, 2019). Many different hazard analysis tools have been developed in the literature for a range of occupational hazards including nanomaterials (Dimou & Emond, 2017), lifting hazards (Spector et al., 2014, and more generalized approaches to hazard assessment (Mohamed et al., 2019); however, those interested in occupational heat exposure should ensure they are using a tool that specifically asks about heat and the appropriate mitigation strategies (i.e., air conditioning for indoor workers) such as the tool presented by Roughton and Crutchfield (2016). Future research should investigate the impact of occupational heat exposure in various occupations outside of agriculture to elucidate the association between occupation and ESRD development in this population.
Limitations of this study include the cross-sectional nature of the study and reliance on self-reported occupational histories, which can introduce recall bias into the study. In addition, by utilizing a snowball recruitment, persons who were willing to participate may potentially have different occupational histories than those who chose not to participate. Recruitment also occurred in a rather unique emergent dialysis mechanism set up by the local safety-net hospital allowing for access to more frequent dialysis treatment, which may potentially decrease the generalizability of the findings. Finally, our use of topic modeling only utilized k = 2 for creating the final topic model. It is possible that with larger datasets of free-text data, a more robust analysis exploring the occupational histories within the outdoor and indoor worker groups could be conducted. Nonetheless, by utilizing topic modeling, we were able to identify two divisions or “topics” of occupational histories, which verified assumptions we held about what data would be present in the occupational histories of those who participated in our study.
Conclusion
In an increasingly warming climate, those who work outside or in hot indoor environments may be at even greater risk of heat-related renal disease. Furthermore, this study suggests that some immigrant workers are exposed to work conditions, other than agriculture, that potentially are associated with the development of CKDu. Given that those who had developed ESRD reported working across multiple occupation categories, work is needed that describes the impact of occupational heat exposure on renal functioning across occupational groups. Clinically, those who are working with emergent-only dialysis patients should be conducting routine occupational assessments of those who continue to work and providing educational resources on health and other occupational health hazards for their industry. This study also provided evidence that undocumented workers continued to work after developing kidney disease and did so in occupations that increase their risk for suffering the deleterious effects of continued occupational heat exposure. Finally, this study provided evidence that topic modeling is a useful tool for studying the unstructured, free text data that are often generated when conducting an occupational history assessment.
Applying Research to Occupational Health Practice
In response to the global pandemic of chronic kidney disease of unknown etiology, which disproportionately affects agricultural workers of Latinx descent, this assessment of occupational histories of undocumented immigrants receiving frequent, emergent-only hemodialysis showed that there are additional occupations at risk for suffering the kidney impacts of occupational heat exposure. These included workers in both construction and landscaping, as well as indoor environments, such as dry cleaning. This study will guide future efforts to identify occupation-specific impacts of heat exposure in occupations that commonly employ undocumented workers in the U.S. Occupational health nurses and professionals working with undocumented immigrants must conduct thorough occupational health hazard assessments and design tailored interventions to protect the health of these potentially heat exposed workers.
Supplemental Material
sj-docx-1-whs-10.1177_21650799211060695 – Supplemental material for Using Occupational Histories to Assess Heat Exposure in Undocumented Workers Receiving Emergent Renal Dialysis in Georgia
Supplemental material, sj-docx-1-whs-10.1177_21650799211060695 for Using Occupational Histories to Assess Heat Exposure in Undocumented Workers Receiving Emergent Renal Dialysis in Georgia by Daniel J. Smith, Valerie Mac, Lisa M. Thompson, Laura Plantinga, Lauren Kasper and Vicki S. Hertzberg in Workplace Health & Safety
Footnotes
Acknowledgements
The authors would like to acknowledge the persons who participated in this research for their time committed to participating in this survey. The first author would also like to thank Dr. Sarah Febres-Cordero for her insight when revising this manuscript’s discussion.
Author Note
Daniel J. Smith, PhD, APRN, CNE, was now affiliated to M. Louise Fitzpatrick College of Nursing, Villanova University.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Emory University Institutional Review Board on 10/26/2018. Study number IRB00103062.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Daniel J. Smith is a nurse practitioner and researcher. He is currently the Weingarten Endowed Assistant Professor at the M. Louis Fitzpatrick College of Nursing, Villanova University. This work was completed during his PhD studies at Emory university.
Valerie Mac is a nurse practitioner and epidemiologist. She is an Honorific Assistant Professor at the Nell Hodgson Woodruff School of Nursing, Emory University.
Lisa M. Thompson is a nurse practitioner and environmental health researcher. She is an Associate Professor and Director of Graduate Studies at the Nell Hodgson Woodruff School of Nursing, Emory University.
Laura Plantinga is a renal disease epidemiologist. She is an Associate Professor at the School of Medicine, Emory University.
Lauren Kasper is a dialysis nurse practitioner and patient experience coach at Grady Health System.
Vicki S. Hertzberg is a biostatistician. She is a Professor and Director, Center for Data Science, as the Nell Hodgson Woodruff School of Nursing, Emory University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.