
Abstract
Background:
Effective smoking cessation interventions (SCIs) are urgently needed for the working population where smoking continues at high rates. Occupational health nurses (OHNs) could be effective in providing SCI, but self-efficacy was found to be a major barrier. The purpose of this study was to improve the delivery of SCI to those who smoke in the workplace and to explore nurse self-efficacy.
Methods:
Pretest and posttest were conducted on two groups, OHNs (n = 5) and smokers (n = 11) working at U.S. manufacturing facilities. OHNs were trained on motivational interviewing (MI) techniques who then recruited smokers to help them practice their newly acquired skills. The two groups were measured by Likert-type scale for OHN self-efficacy and smoker level of change toward quitting.
Findings:
Paired t-tests detected statistically significant differences in OHN’s preintervention and postintervention self-efficacy scores, t(4) = −4.46, p < .001,; d = 2.92) and smokers’ preintervention and postintervention stage of change toward quitting scores, t(10) = −9.07, p < .001,; d = 2.09), suggesting that the training and MI intervention were effective in increasing OHN self-efficacy and smokers’ motivation to change.
Conclusion/Application to Practice:
This quality improvement (QI) project indicated smokers can be successfully recruited and counseled using MI techniques, while simultaneously improving OHN self-efficacy toward helping patients. Theory-based applications brought OHNs and smokers together in a new paradigm resulting in positive changes for both. Secondary findings in the reverse nurse–patient role revealed success in an innovative recruitment method for smoking cessation.
Keywords
Background
Although smoking rates have continued to decline since the 1970s, smoking continues to be the single greatest cause of preventable disease worldwide (World Health Organization [WHO], 2015). In 2015, the WHO predicted that smoking would kill 5 million people annually. In the United States, the Centers for Disease Control and Prevention (CDC, 2015) reported that smoking was affecting about 22% of blue-collar workers. Furthermore, nearly 33 million working adults were currently using tobacco (Syamlal et al., 2017). An estimated 1.5 million workers die or suffer from smoking-related disability, and employers spend $300 billion in lost productivity and medical expenses each year.
Smoking continues to be an adverse health determinant for more than 20% of the working population which suggests that there is a need for employers to provide effective smoking cessation intervention (SCI) in the workplace (Syamlal et al., 2017). Cahill and Lancaster (2014) reported that implementing SCI in the workplace was up to three times more effective than interventions in other community settings. A study by Pinsker et al. (2015) found that blue-collar production workers had a higher prevalence of daily smoking (88%) compared to white-collar professionals (68%), and blue-collar workers were more likely to use SCI if it were easily accessible, there was no cost, and it took minimal time commitment (Yzer et al., 2015).
Successful SCI has been described as an “empathetic, personalized approach” with “assistance and follow-up” to help smokers quit (Anczak & Nogler, 2003, p. 203). SCI techniques are intended to be directed at individual smokers using communication skills that reinforce self-efficacy and are more effective than text messaging and web-based programs (Catley et al., 2015). Nurses can play a key role in advocating and promoting SCIs in the workplace (Rice et al., 2013), particularly when they make personalized visits. Patients who receive more intensive nurse interaction are more likely to quit, which provides justification for a nurse-led intervention (Zwar et al., 2015). Furthermore, nursing is considered the most trusted profession, and nurses are skilled at therapeutic communication and face-to-face interactions (Norman, 2016).
Yet, despite effective evidence-based practice guidelines for smoking cessation, large studies reported that all nurses do not consistently deliver SCI (Rice et al., 2013). Barriers exist including lack of time and organizational support (Leitlein et al., 2013), lack of role identification (Rice et al., 2013), and lack of nurses’ knowledge of SCI and perceived confidence (Fore et al., 2013; Leitlein et al., 2013; Rice et al., 2013). A study by Chatdokmaiprai et al. (2017), specific to occupational health nurses (OHNs), identified self-efficacy as the single most significant factor for providing successful SCI.
A recent integrative literature review identified a gap in the extant literature regarding nurse self-efficacy in SCIs (Thornberry et al., 2020). Their database search revealed 15 articles addressing SCIs conducted by nurses in general and only one specific to OHNs discussing self-efficacy. In the analysis, two major themes regarding nurse SCI self-efficacy emerged: (a) nurse characteristics and (b) organizational characteristics. Factors that positively and negatively influenced nurses’ self-efficacy included nurse training, academic preparation, attitude, social influence, and organizational support through policy, time investment, and theory-based training (Thornberry et al., 2020). Findings from this integrative literature review and studies on general nurse self-efficacy were used to support the design of this project.
The purpose of this project was to improve the quality and delivery of care to smokers in this U.S. company’s manufacturing facilities and to increase OHN self-efficacy in the delivery of SCI. The clinical practice questions guiding this work were as follows: (a) will OHN self-efficacy in SCI improve after theory-based motivational interviewing (MI) training and practice? and (b) will the OHN affect change in the smoking worker by moving them toward quitting? This study is relevant to occupational health because it applies research evidence to design theory-based educational programs and intervention methods to improve SCIs for smokers in the workplace.
Guiding Frameworks and Concepts
Concepts of self-efficacy and change theory were used to develop the project interventions for the OHNs and the smokers. Self-efficacy and situational confidence were first introduced by Bandura (1991). The constructs of self-efficacy evolved around an individual’s own perceived abilities to perform, organize, and execute an action to achieve a goal. In the Theory of Self-efficacy, a person’s motivation to perform a given task is dependent on how confident they feel about performing the task. Bandura found that self-efficacy comes from four sources: (a) actual behavior performance, (b) watching others perform the behavior, (c) verbal persuasion, and (d) emotional arousal (Bandura, 1991). The practice of a behavior had the strongest influence on self-efficacy (Darkwah et al., 2011). The OHN education and training for this project was based on these concepts which incorporated interactive discussions, situational polling questions, YouTube demonstrations, and practice sessions with smokers.
The transtheoretical model (TTM) was developed in the 1980s as an integrative theory utilizing the constructs of self-efficacy and intentions for change (Miller & Rollnick, 2012). The TTM has been used effectively in SCI therapy (Prochaska et al., 2008). Central to the TTM are the “Stages of Change” which fall under the constructs of motivational readiness to change (Prochaska et al., 2008). The TTM was used as a framework to develop interventions for the smokers in this quality improvement (QI) project.
MI is a client-centered counseling approach based on the concepts of TTM. MI addresses behavior change through interviewing techniques that work within the smoker’s own motivation for change (Miller & Rollnick, 2012). In this project, the TTM provided a conceptual model for OHNs’ understanding of the smokers’ change processes and education on MI were the basic skills learned and practiced to assist the smokers with moving through the stages of change toward quitting. The elements of MI included partnership, acceptance, compassion, and evocation. These interrelated counseling components sequentially assisted the OHN in building a relationship and to establish acceptance of the smoker. Communication skills included open-ended questions, affirmation, reflection, summarization, and provided information or advice with permission to assist smokers in behavior change (Miller & Rollnick, 2012). MI is based on four guiding principles to assist the OHN with knowledge of decisional balance and advancing smokers through stages of change: (a) resist advising or telling the smoker to quit; (b) understand what motivates the person to change; (c) use reflective listening to confirm understanding; and (d) empower the smoker to make health-related behavioral improvements (Rollnick et al., 2008).
MI can be an effective tool for helping smokers amplify personal discrepancies when they are not ready to quit. A meta-analysis found that smoking cessation rates increased using MI compared to usual care (Lindson-Hawley et al., 2015) and that multiple, brief, 20-minute sessions were effective (Aveyard et al., 2012). In this project, MI skills were taught to the OHNs preparing them with strategic questions using empathetic listening to help smokers’ resolve ambivalence about changing behaviors (Miller & Rollnick, 2012). The TTM incorporating MI techniques was an effective theory for health promotion and behavior change in smoking (Hettema & Hendricks, 2015) and have guided the development, interventions, and evaluation of this project.
Methods
This QI project used an educational intervention and a recruitment participation intervention. Two types of participants were involved in the project, OHNs and smokers, working at five U.S. manufacturing facilities. Self-efficacy in OHNs was measured before and after SCI training and practice, and stages of change toward quitting was measured in smokers before and after three MI counseling sessions with the OHN.
The project was conducted at one U.S. company’s rural-based manufacturing facilities where nearly one in 10 of the workers smoked. The OHNs provided routine occupational health services to workers at the worksite. The smoking participants were workers in maintenance and production areas who performed physical tasks involved with manufacturing. The smokers had opted out of a recently implemented company-sponsored smoking cessation program. The project director presented an overview of the QI project to the company leadership and to the OHNs (n = 8) as an adjunct to a recently introduced web-based quit program, sponsored by the company. The project goals were aligned with the company’s strategic plan to improve employee health and reduce the smoking rate. Leadership announced their support of the project and agreed to a cash incentive for the OHNs who participated and recruited three or more smokers.
A convenience sample of the company’s OHNs (n = 5) were recruited by the project director during a regular business team meeting. The OHNs were adult women median age 57 years and predominantly Caucasian ethnicity. They had a wide range of education and licensure attainment which ranged from high school diploma/LVN to master’s degree/APRN. There was an average of almost 18 years’ experience in occupational health nursing.
The smoking participants (n = 11) were recruited by the nurses through personal clinic encounters to form a convenience sample. The OHNs asked smokers if they had enrolled in a company-sponsored quit program. If the answer was no, the OHN asked the smokers if they would consent to be part of a QI project which would help the nurse practice newly acquired smoking cessation interviewing skills.
For this study, two groups received interventions. The OHNs received theory-based training in MI techniques and concepts in motivational change. The 90-minute MI training was scheduled during a regularly scheduled team meeting. The training included a PowerPoint presentation, interactive polling questions, group discussions, and a YouTube demonstration. Educational smoking cessation elements included: (a) significance and background of the problem; (b) evidence-based clinical practice guidelines; and (c) MI techniques (American Cancer Society, 2017; Furmanski & Sullivan, 2015; Pro Change Behavior Systems, 2017). The OHNs applied their skill with smokers for 3 months beginning in March and ending in May of 2018. Each nurse recruited their own smoking participants from their respective manufacturing worksites. The smokers were incentivized with a $50 gift card and scheduled for three 20-minute MI counseling sessions with the OHN during their regular work day. The OHN explained to the smoker this was a QI project and it was to allow the nurse to practice newly acquired smoking cessation interviewing skills. The nurse counseling sessions applying MI techniques was the intervention received by the smokers.
The instrument used to measure OHN self-efficacy was the modified Self-Efficacy and Behavior for Smoking Cessation Counseling Survey (Barta & Stacy, 2005) developed for hospital nurses in SCI. The tool has 14 questions related to the nurses’ confidence in providing SCI; examples include: “I can regularly ask patients about their smoking” and “I can be effective in changing a smoker’s behavior.” The answers were on a 5-point Likert-type scale ranging from not at all confident to very confident for an over-all very high confident score of 70 points and a low score of 14 points. The survey was designed to assess the nurses’ self-perceived capabilities in delivering SCI and had been tested for content reliability and validity (Preechawong et al., 2011). OHNs completed this survey as a pretest before their training and again after training and skills application with their smokers. For confidentiality, an alphanumeric code was assigned to each OHN’s survey and pretest and posttest data were collected using Qualtrics, an online survey software. The goal was to achieve a mean posttest score of 56 indicating OHN confidence for providing SCI. The rationale being the nurse would answer confident (4-points) to all 14 questions.
Once the smoker agreed to participate in the study, a pretest was administered by the OHN to determine the stage of change for quitting using the Process of Change Questionnaire: Smoking Version (PCQSV) (University System of Maryland [UMBC], 2018). This questionnaire was developed using the TTM and had been tested for reliability and validity in adult male smokers. A study by Sarbandi et al. (2013) provided evidence that the PCQSV was an appropriate tool for measuring SCI and the extent to which interventions could change people’s behavior. The PCQSV was used to help the nurse determine the smoker’s stage of change. Sample questions for the smokers included “I tell myself I can quit if I want to” and “I get upset when I think about my smoking.” The answers were on a 5-point Likert-type scale ranging from never to repeatedly for an over-all readiness to change score of 100 points. The goal was to achieve a mean posttest score of at least 70 by answering 10 of the 20 questions occasionally (3-points) and 10 questions often (4-points). This score was suggested the smoker had considered behavior change and had begun behavior changes to quit (UMBC, 2018).
Data were analyzed using the Statistical Program for Social Sciences (SPSS), version 25.0. Quantitative data were obtained from total survey scores to pretests and posttests for two types of participants (nurses and smokers) receiving interventions. A paired t-test was used to determine if there was a significant difference between pretest and posttest survey scores for nurse self-efficacy and smoker’s stage of change for quitting. Pearson’s correlations determined relationships between nurses’ total self-efficacy change scores and smokers’ total Stage of Change scores. The p-level used to detect significance was p < .05.
The Texas A&M University-Corpus Christi Office of Research Compliance Institutional Review Board deemed this project as QI and not human subjects research.
Findings
Smoker Comparisons
The smokers who agreed to be in the project were adult manufacturing workers (mean age = 40.73, SD = 11.9) who reported total previous years smoked (M = 22.82, SD = 10.4); current packs per day smoked (M = 1.18, SD = 0.51); and previous attempts quitting (M = 2.55, SD = 1.44). The participants were predominantly men and included Caucasians (n = 8, 72.7%) and Hispanics (n = 3, 27.27%). See sample characteristics of study population (Table 1).
Sample Characteristics of the Nurses and Smokers as the Study Population
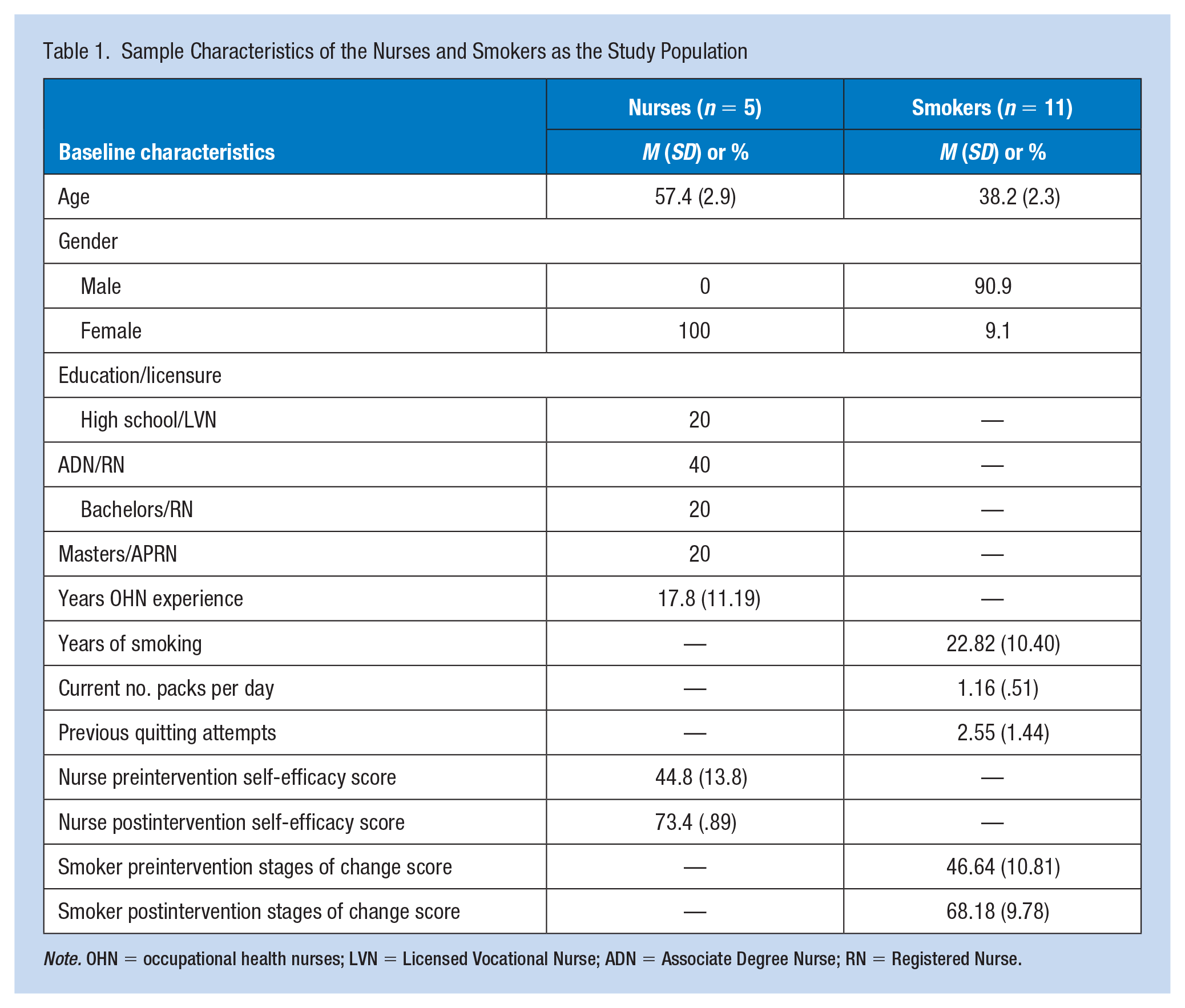
Note. OHN = occupational health nurses; LVN = Licensed Vocational Nurse; ADN = Associate Degree Nurse; RN = Registered Nurse.
Paired sample t-tests were conducted on smoking participants (n = 11) to detect a statistically significant difference between prenurse MI intervention smoker stages of change scores and postintervention scores. There was a significant difference in the smokers’ preintervention stages of change scores (M = 46.64, SD = 10.81) and postintervention (M = 68.18, SD = 9.78) stages of change scores t(10) = −9.07, p < .001, d = 2.08.
Pearson’s correlation was conducted on smokers’ demographic variables and stage of change toward quitting scores. There was a strong positive statistcal correlation between smokers’ age and years smoked r(9) = .861, p = .001, and quitting attempts r(9) = .805, p = .003. There was a strong negative correlation between smokers’ stage of change score and age r(9) = −.698, p = .017 number of years smoked r (9) = −.645, p = .032, and number of attempts at quitting r (9) = −.761, p = .007. See Pearson’s correlation for smokers in Table 2.
Pearson’s Correlation Between Smokers’ Characteristics and Smokers’ Stages of Change Toward Quitting Score
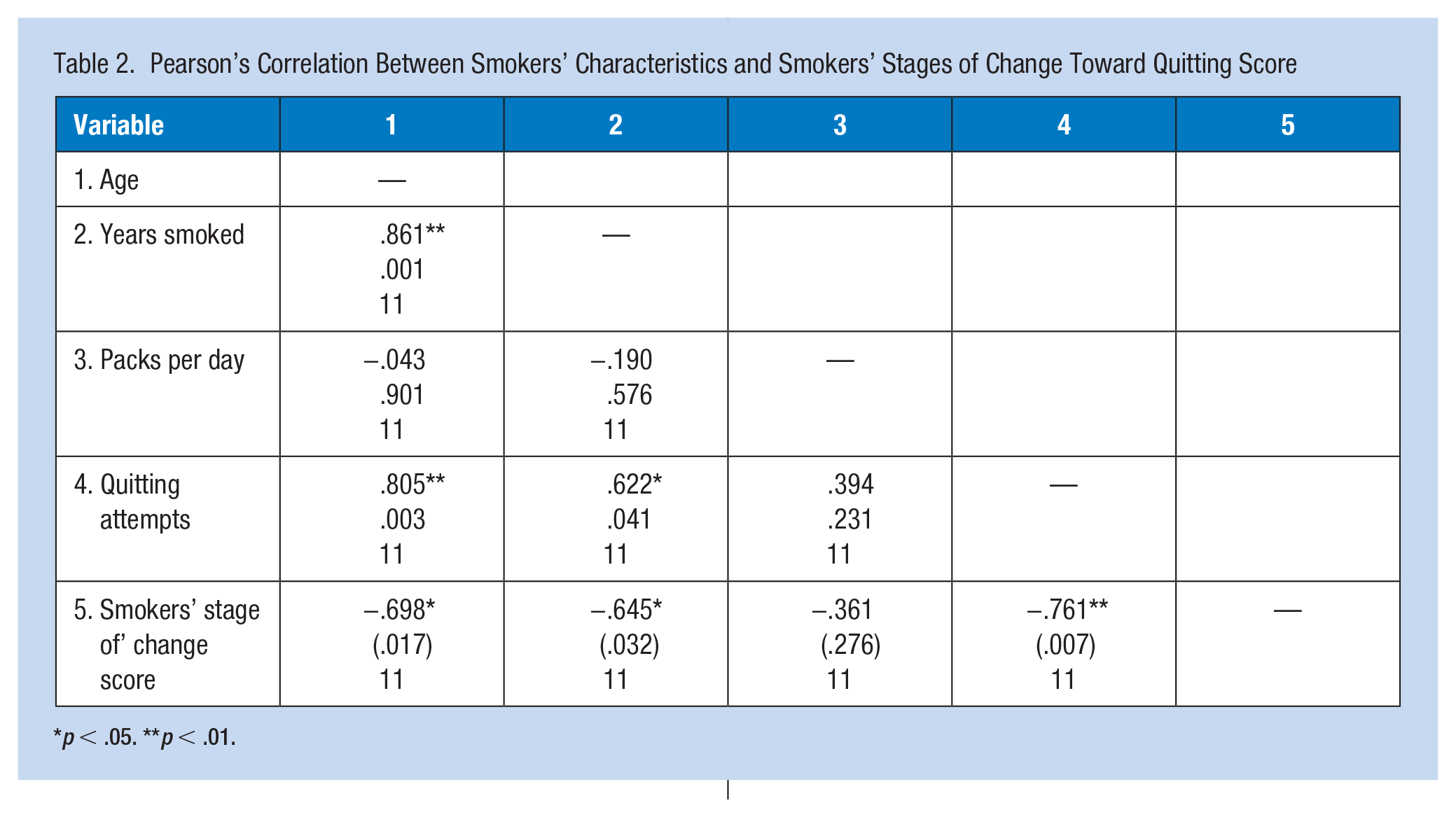
p < .05. **p < .01.
OHN Comparisons
Paired t-tests were conducted on self-efficacy survey data from nurse participants (n = 5). There was a significant difference in the nurses’ preintervention self-efficacy scores (M = 44.8, SD = 13.8) and postintervention (M = 73.4, SD = 0.894) self-efficacy scores; t(4) = −4.46, p = .011; d = 2.91). Results of paired t-tests and descriptive statistics for preintervention to postintervention changes in smoker’s stages of change and nurses’ change in self-efficacy scores can be found in Table 3.
Descriptive Statistics and Paired t-Test Results Comparing Preintervention and Postintervention Scores for Smokers’ Stages of Change and Nurses’ Change in Self-Efficacy
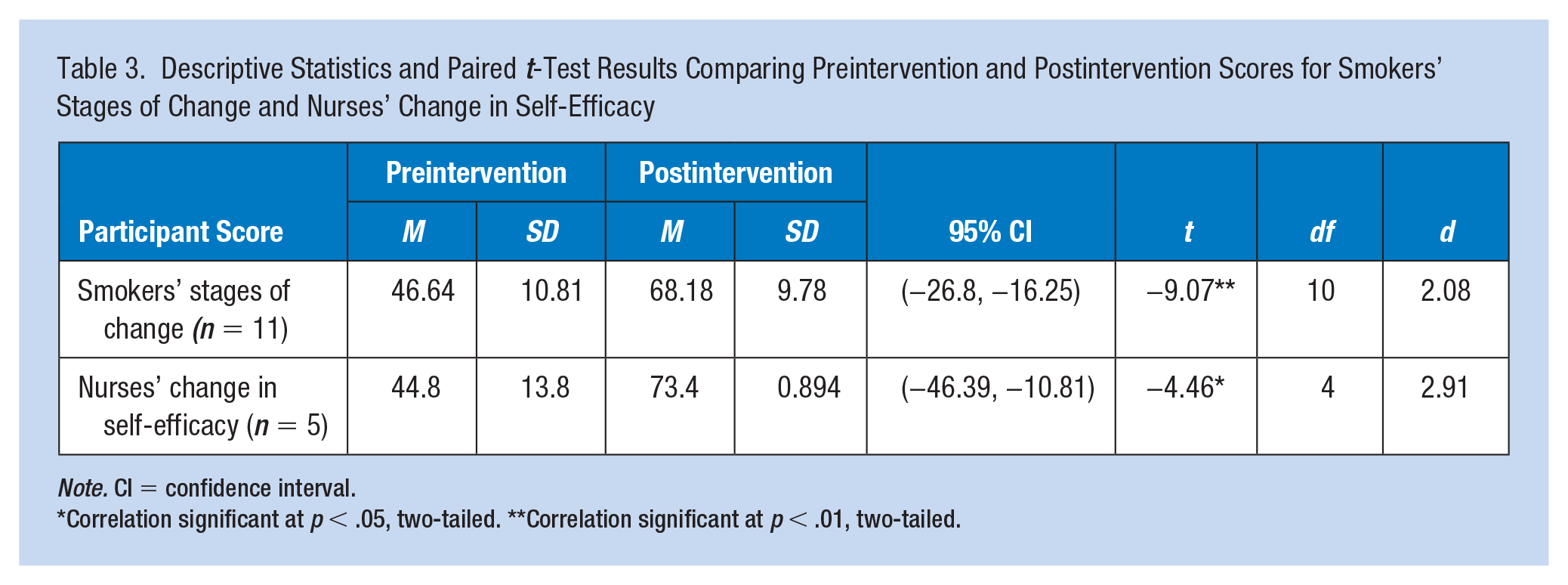
Note. CI = confidence interval.
Correlation significant at p < .05, two-tailed. **Correlation significant at p < .01, two-tailed.
Pearson’s correlation was conducted on nurses’ demographic variables and stages of change scores. There were no significant correlations between demographic variables and change in self-efficacy scores for nurses. There were no significant correlations between mean change scores of smokers by nurse and nurses’ mean change in self-efficacy scores. There were no significant correlations between the nurses’ postintervention self-efficacy score and the nurses’ change score r (3) = .523, p = .366. The relationship between the nurse’s preintervention self-efficacy score and their change scores were strongly and inversely (negatively) related r (3) = −.998, p < .01.
Discussion
Our postintervention goal for nurses (self-efficacy survey score of 56) was exceeded (postintervention mean score = 73) and our goal for smokers (smoker stages of change survey score of 70) was almost reached (postintervention mean score = 68). Our goal was to increase nurses’ mean self-efficacy score to at least 56 (a rating of at least “confident” on all 14 questions). Total mean self-efficacy scores for nurses increased from 45 to 73, a 62% increase. Moreover, we exceeded our goal score of 56 by 30%. Smokers’ mean scores increased from 47 to 68 from preintervention to postintervention, almost reaching this project’s goal score of 70, but more importantly, increasing these smokers’ readiness to change by 45% from preintervention. Changes from preintervention to postintervention in both smokers and nurses were statistically significant and clinically significant. Cohen’s d values and the percentage improvements for both groups of participants indicated the intervention made a significant difference in nurses’ self-confidence and smokers’ readiness to change. See nurses self-efficacy pretest and posttest scores. In Figure 1 and smokers pretest and posttest stages of change scores in Figure 2.
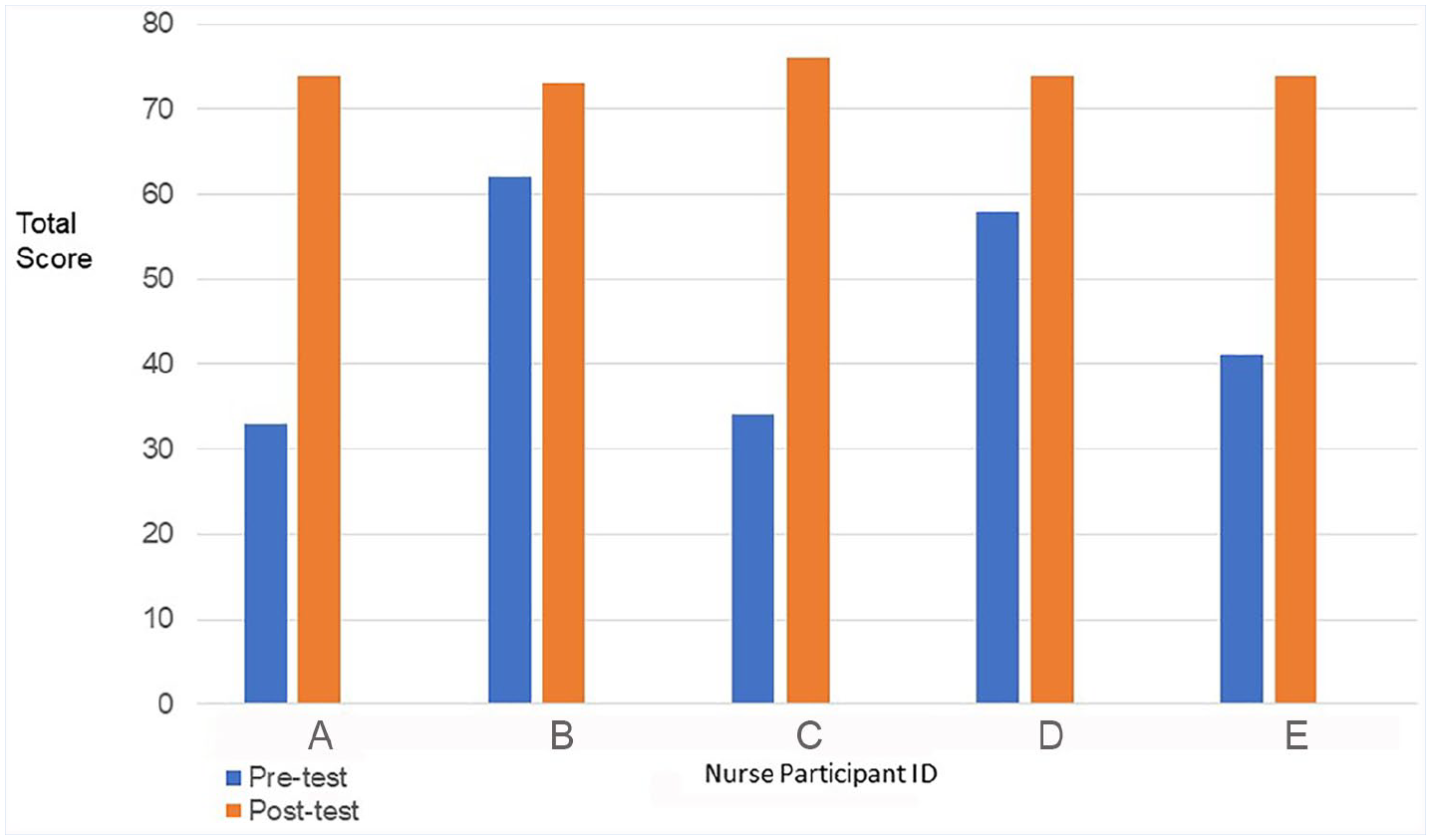
Nurse self-efficacy pretest and posttest scores.
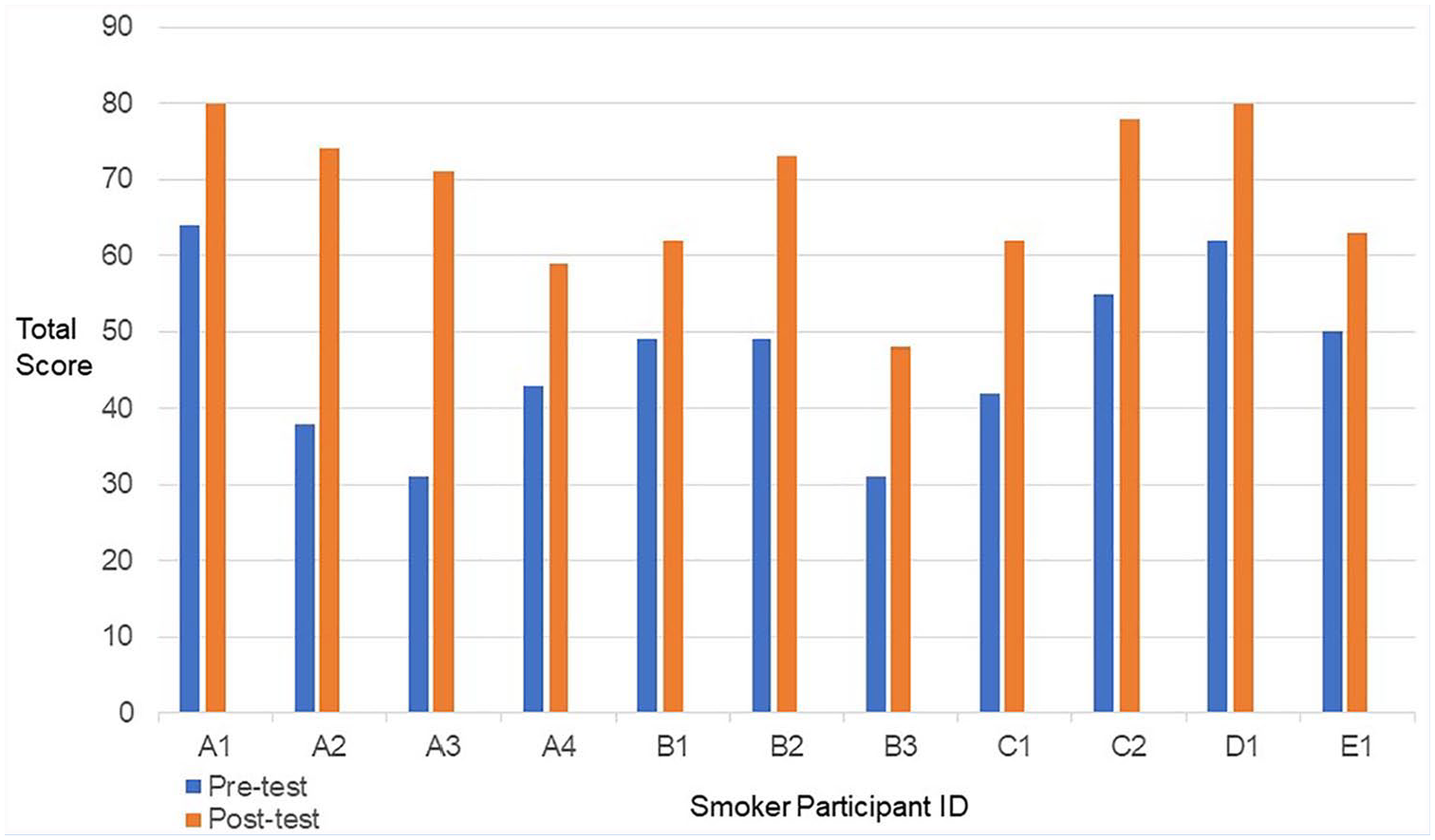
Smokers pretest and posttest stages of change scores.
The large effect sizes seen in both groups, smokers, and nurses, were important findings in this study. The nurses’ postintervention self-efficacy scores substantially increased, indicating the education and the practical application of MI techniques provided to OHNs greatly increased their SCI. The smokers’ postintervention stage of change scores substantially increased, indicating counseling provided by the OHNs affected their change in motivation toward quitting. This suggested that the nurse education and skills application can make a substantial difference in smokers’ change toward quitting. Similarly, Fore et al. (2013) found nurses who received SCI education and were satisfied with their training had a significant effect (p < .0001) on their self-efficacy. Moreover, their perceived self-confidence was increased over time while implementing their training skills and potentially increasing quit rates.
At the start of the project, the OHNs claimed lack of time was a barrier. This was addressed by designing fewer and shorter counseling interventions with the smoker. Research studies indicate MI delivery was affected when duration and frequency were shortened. Lundahl et al. (2010) looked at MI delivery time and number of sessions in treatment success and found a significant positive relationship when MI sessions were compared to groups with fewer interventions. This suggests more MI sessions could lead to better outcomes. Lundahl et al. (2010) also found sessions lasting more than 20 minutes could be more successful than interventions of 20 minutes or less. But there were overlapping confidence intervals suggesting the extended length of sessions was not significant. VanBuskirk and Wetherell (2014) discovered the total time for an MI session was not a significant moderator of effect size for substance abuse groups. Limiting the MI intervention to three 20-minutes sessions did not impact the outcomes of this project. The total overall nurse mean change respective to smoker change increased for both nurses and smokers. There were no significant correlations between mean change scores of smokers by nurse and nurses’ mean change in self-efficacy scores.
There could be inconsistencies with nurse delivery in SCI by the varied backgrounds, education, and experience levels. A similar research study (Prochaska et al., 2008) looked at consistency in MI delivery and compared methods. Prochaska et al. (2008) found no significant differences between interventions based on the TTM of Health Behavior Change and MI interventions. While these were two different interventions the outcomes were similar. This lack of standardization in MI counseling did not cause significant differences in the intervention outcomes. Nevertheless, even with the variable nurse characteristics and possible inconsistencies in delivery, the goals and expected outcomes of this project were still met.
The results of this QI project suggested education and practice using MI skills significantly improved OHNs’ self-efficacy; the nurse’s use of MI techniques during intervention significantly improved the smoker’s motivation to quit. No matter where the nurse began in her level of self-efficacy, low or high, there was a statistically significant and a large positive change in all nurses, supporting that MI training and practice may increase nurses’ self-efficacy in implementing successful SCI. The differences in the nurses’ preintervention self-efficacy scores could be related to demographic variables such as age, licensure, education, experience levels, and personal attitudes; however, no significant associations were found in this small sample. Regardless of the nurses’ pre-self-efficacy scores, there was an overall high level of improvement in self-efficacy scores postintervention meaning all nurses regardless of self-efficacy in SCI can benefit from education and training.
There was not a significant association between the nurse’s preintervention self-efficacy score and the smoker’s change in motivation score. This suggests that education and skills practice improved nurse’s self-efficacy scores enough so that, regardless of how low their preintervention self-efficacy scores were, they could gain enough self-confidence to provide successful MI counseling. This means that providing nurses with training and education can make a difference in smokers change toward quitting.
Paradigm Shift
The substantial change in smokers’ motivation to quit could be attributed to the QI project design. The initial steps in this project were dramatically different from the nurse in an authoritative role when encountering smokers who had been resistant to quitting. Traditionally, the nurse approaches the smoker by advising they quit, providing information on the health detriments of smoking, and offering assistance. In this project, the nurse asked the smoker to be part of a QI project that was mandatory for the nurse to do, thus the nurse asked the worker “Will you help me practice and apply my motivational interviewing skills?” rather than telling the smoker, “Let me help you to stop smoking.” This approach completely changed the usual dynamic between nurse and employee: the employee aids the nurse to improve skills, and in this new paradigm, the nurse is the focal point of need, not the smoker. Similarly, a student–teacher scenario in nursing education found nursing students performed better and were more satisfied when their roles were reversed (Betihavas et al., 2016).
This initial change in the process removed the nurse from the ask-advise-assist model, (Agency of Healthcare Research and Quality, 2015) which is not consistent with the MI approach because it demotivates thoughts and feelings for behavior change. The QI project or any situation in which the nurse becomes the focus of change and not the patient, permits the freedom of behavioral change to begin unharnessed when the nurse is positioned to begin MI while avoiding phrases such as “Let me help you quit” or “I can assist you in quitting.” Righting and resisting, common pitfalls in MI, are side-stepped as the nurse begins using MI without the common roadblocks encountered in telling the person they need smoking cessation counseling. Is it possible the large positive effects from this study stem from the initial steps of an intervention aligned with a theory-based framework? The smoker experienced a role reversal when they agreed to be a participant in a study to help the nurse with her skills. This reversed relationship could open doors for more receptivity, allowing the forces of MI to take effect with smokers.
Role of MI in Modifying the Nurse–Patient Relationship
The elements of MI include partnership and acceptance of the smoker, which is an interrelated counseling component of MI. Once a partnership is established with the smoker, the nurse begins the MI processes to build on the stages of change. The trained nurse is only influential if they can meet and talk with the smoker. Nurses discovered smokers were much more receptive to them when they were recruited to help the nurse. The usual advice smokers receive from the nurse in SCI may have been met with less resistance because the nurse was asking for their help and they did not feel the pressure to change. The smoker was asked for assistance and in exchange was valued as a participant in a project aimed at the nurse’s improvement, not their own improvement. This reverse nurse–patient relationship led the smokers, perhaps unknowingly, to more openly engage with the nurse; and the nurse, who was trained to empathetically listen using MI, to establish a closer kinship with the smoker. To the smoker, the intervention by the nurse was more acceptable related to feelings of professional connectivity rather than personal neediness, which could create resistance to combat feelings of lesser self-efficacy. The transformation of these reversed roles between the nurse and the smoker could be the reason for the large effect size.
This study had several limitations. The sample size of the pilot project was small and can affect statistical findings. A strength is the sample was gathered from one company’s five manufacturing facilities across the United States. However, findings are applicable only to these work facilities as the purpose of the project was to improve care provided at this company.
Implications for Occupational Health Nursing Practice
These positive affects built on theory-based concepts of self-efficacy and change were uniquely situated in the workplace and redesigned by the OHN who invited smokers to participate in a QI project. The doorways to the intervention structure opened differently and were aligned with company goals for improvement, creating less resistance from the smoker and more opportunity for the nurses to listen and talk with their smoking patients. The OHNs were surprised at the change in resistance from the smokers when they were asked to help the nurse as opposed to being asked to help themselves. Smokers who had initially shown resistance to SCI, agreed to participate. So, was flipping the need for assistance from the smoker to the nurse, a different method for approaching smokers? A processes diagram of this QI project models the interventions, the participant dynamics, and the process movement. In the Quality Improvement Change Process Model (Figure 3), the intervention arrows are orange, indicating nurse training and nurse provided MI counseling with the smoker. This QI project used theory-based applications in the first steps when the nurse was removed from the adversarial role and asked the smoker to partner with her in developing her skills. This shift in the nurse–patient relationship aligned witfh the spirit of MI where the nurse partners with the smoker. When the nurse asked the smoker to help, this resulted in improved receptivity as seen in the top green arrow. The nurse then applied the MI intervention techniques, guiding, and listening, and the smoker moves upward in the motivation to change scale while the nurse also advances in self-efficacy to produce a change.
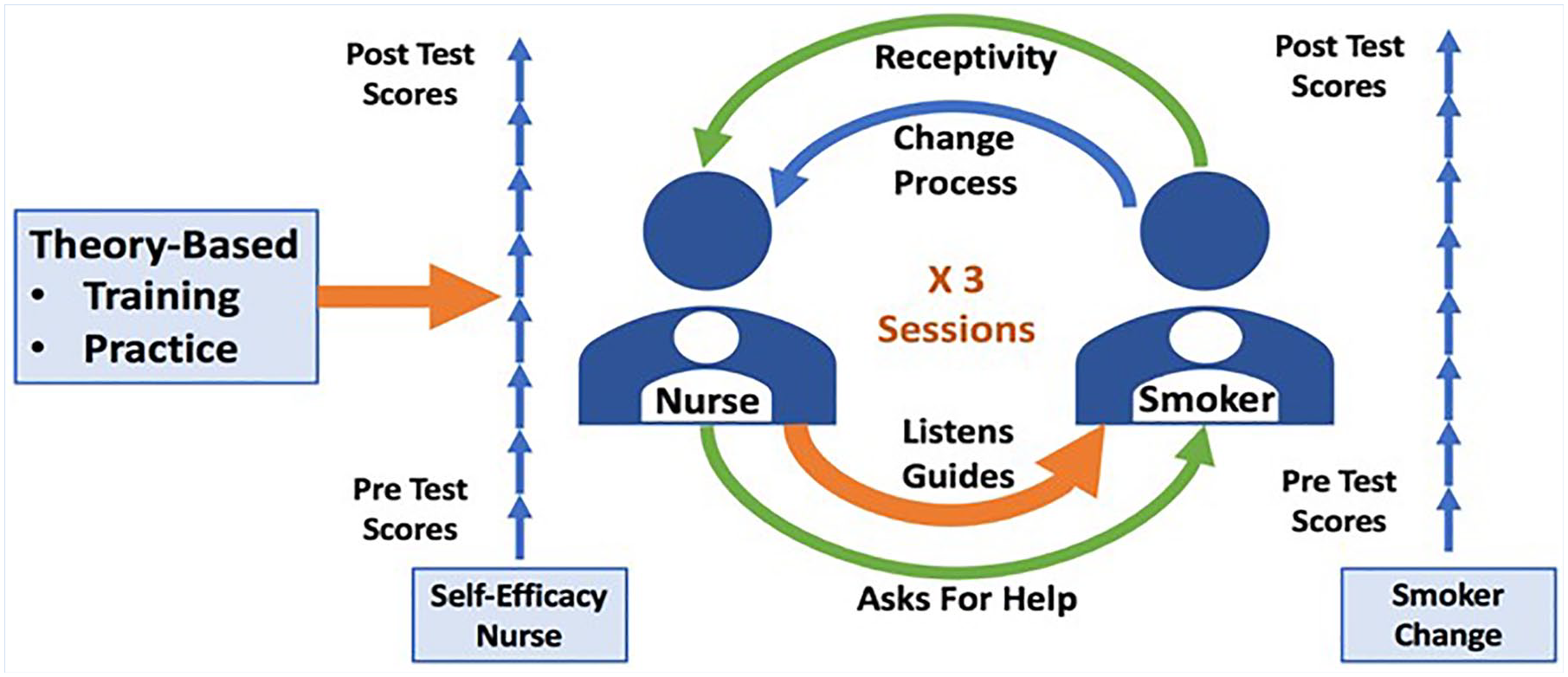
Quality improvement process change model depicting the interventions of the participant dynamics and the process movement.
Applications to Professional Practice
Quality improvement work in the occupational health setting can be pivotal for applying effective SCI and discovering influences affecting a smoker’s change toward quitting. The positive changes demonstrated in this QI project, could direct more studies and OHN deployment for future QI work. Forthcoming studies may look at using this innovation of a flipped nurse–patient recruitment method to improve smoker’s reception of SCI and more effectively move smokers closer to quitting for improving healthcare outcomes. Furthermore, MI techniques can greatly affect health-related behavior change, not only in smoking workers, but in all avenues of health promotion. Future work should focus on OHN self-efficacy and projects designed to flip the doorways to improve worker health making them more willing to enter. This QI project, if repeated in greater numbers by OHN’s, could provide more data to determine if this approach should be a process change for improved quality of health and well-being in the workplace.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Amy Thornberry, DNP, APRN, FNP-C, COHN-S is the primary author. She is a nurse practitioner and certified Occupational Health Nurse and Leader for the Occupational Health Programs at Celanese North America. She was the primary contributor to the design of the work, acquisition, analysis, and interpretation of data.
Theresa J. Garcia, PhD, RN is an assistant professor of nursing at Texas A&M Corpus Christi College of Nursing and Health Sciences contributing to the analysis and interpretation of data and critical revision for intellectual content.
Jessica Peck, DNP, RN, CPNP-PC, CNE, CNL is a nurse practitioner and professor of nursing, contributing by analysis and interpretation of data, critical revision, and final approval of the version to be submitted.
Elizabeth Sefcik, PhD, RN, GNP, BC is an assistant professor at Texas A&M Corpus Christi College of Nursing and Health Sciences contributing to revision, accuracy, and integrity of the final version.