
Abstract
This pilot project aimed to improve depression symptoms and quality-of-life measures for individuals in a worksite disease management program. Two hundred forty-three individuals were invited to participate, out of which 69 enrolled. The participants had a history of diabetes, hypertension, or hyperlipidemia, and demonstrated depression using the Patient Health Questionnaire–9 (PHQ-9). The project consisted of counseling sessions provided every 2 to 4 weeks by a family nurse practitioner. PHQ-9 scores and those of an instrument that measures quality of life, the Veteran’s Rand–12 (VR-12), were compared pre-intervention and post-intervention to evaluate the effectiveness of the project. PHQ-9 and VR-12 Mental Health Component (MHC) scores improved significantly after 3 months of nurse practitioner-led individual counseling sessions. This project demonstrated that depression screening and therapeutic management, facilitated by a nurse practitioner, can improve depression and perceived quality of life in individuals with hypertension, hyperlipidemia, or type 2 diabetes.
Keywords
The Centers for Disease Control and Prevention (CDC; 2010) examined data from the Behavioral Risk Factor Surveillance System from 2006 to 2008 and found that depression occurs in 9% of the U.S. population. The population of the southeastern states has the highest prevalence of depression. Based on random telephone interviews, 9.6% of South Carolinians reported symptoms consistent with a diagnosis of depression during the previous 2-week period (CDC, 2010). In addition, the CDC noted that depression is more common in those with chronic disease (e.g., obesity, heart disease, and diabetes). Egede (2007) asserted that individuals with chronic disease have an increased risk of depression, with the risk for depression being double (odds ratio [OR] = 2.00) for those who have hypertension, almost double (OR = 1.96) for those with diabetes and more than double (OR = 2.30) for those with coronary artery disease. The risk for depression is further confounded by unhealthy behaviors such as smoking and lack of exercise (CDC, 2010). Identification of depression is the first step to treatment. Once identified, treating depression could potentially have a positive impact on unhealthy behaviors and ultimately improve the outcomes of chronic disease.
Background
The U.S. Preventive Service Task Force (2009) recommends screening adults for depression when support mechanisms are available to address positive depression screens. However, only 2.29% of clinic visits included depression screening during a 2-year cross-sectional review (Harrison, Miller, Schmitt, & Touchet, 2010). A gap in early identification clearly exists.
Comorbid depression with diabetes, hypertension, or heart disease is associated with increased morbidity and mortality risks (de Groot, Anderson, Freedland, Clouse, & Lustman, 2001; Egede & Ellis, 2010), increased health care utilization (Egede, 2007), increased functional disability (Egede, 2007), and decreased productivity (Egede, 2007; Egede & Ellis, 2010; Jain et al., 2013). In addition, depressed individuals are 2 to 3 times more likely to be noncompliant with recommended health care treatment (Bautista, Vera-Cala, Colombo, & Smith, 2012; DiMatteo, Lepper, & Croghan, 2000; Lin et al., 2004). The health care costs for patients with depression and diabetes are increased by 50% to 70% (Simon et al., 2005). Identifying depression in this population can decrease mortality and morbidity, increase productivity, and increase quality of life. A workplace health promotion clinic is an excellent site to conduct depression screening for workers with type 2 diabetes, hypertension, hyperlipidemia, and obesity due to the increased risk of these comorbid conditions and their impact on productivity, worker outcomes, and health care costs. Sherman and Click (2007) identified health promotion and disease management as an occupational health nursing role, demonstrating that nurses have an opportunity to positively affect outcomes through health promotion activities. By implementing screening in a pre-established wellness program, occupational health nurses can facilitate this process more efficiently. Self-care skills, such as healthful eating and regular exercise, combined with individual counseling can provide therapeutic benefit for depression as well as chronic illnesses.
Literature Review
Many studies have examined the relationship between depression and diabetes, hypertension, or heart disease. A MeSH search of PubMed, PsychInfo, Ovid, CINAHL, Cochrane Library, and Google Scholar was initiated using the search terms depression and heart disease, depression and diabetes, and depression and hypertension. These terms were used in various combinations with additional limits for meta-analyses, systematic reviews, randomized controlled trials, and reviews, which were also used in various combinations. In the event that no results were found, the limits for the level of evidence were completely or partially removed. Only English language articles published about the adult population were included. For the purposes of searching relatively current literature, limits were placed for the years from 2000 to 2014. The search resulted in the initial discovery of 47 articles. Twenty-eight of the identified articles were analyzed by the author.
In evaluating the existence of depression in chronic illness, Findley, Shen, and Sambamoorthi (2011) conducted a retrospective longitudinal analysis investigating persistent depression rates in 1.38 million veterans who also had one or more comorbidities such as hypertension, heart disease, or diabetes. Over a 2-year period, the authors found a 17% prevalence of depression in the study population. Persistent depression risk for those veterans with all three comorbidities was the highest, with an adjusted odds ratio of 1.46 compared with those veterans with a history of only hypertension. Another study by Fortin et al. (2006) found that psychological distress increased with comorbidities and worsened with increasing severity of chronic disease. In a systematic review, strong Level 1 evidence demonstrated a higher prevalence of depression and diabetes, though researchers clarify that causation cannot be determined from their review (Ali, Stone, Peters, Davies, and Hunt (2006). In a meta-analysis of 20 studies, Anderson, Clouse, Freedland, and Lustman (2001) also found a link between depression and diabetes. They suggested that a multivariate analysis could control for confounding moderators and contribute to a better understanding of the relationship between depression and diabetes. Egede (2007) analyzed data on 30,801 adults from the 1999 National Health Interview Survey and found a significantly increased prevalence of depression in those respondents with diabetes, heart disease, and hypertension.
Those individuals with comorbid depression and chronic disease are 2 to 3 times less likely to adhere to recommended treatment (Bautista et al., 2012; DiMatteo et al., 2000; Lin et al., 2004), and have worse health outcomes as a result. Katon, Russo, et al. (2010) conducted a longitudinal study for more than 5 years and found that diabetics with persistent depression, compared with those without depression, demonstrated poor adherence to exercise and nutritional behaviors. De Groot et al. (2001) conducted a meta-analysis of 27 studies consisting of 5,374 type 1 and type 2 diabetics. They evaluated outcomes (i.e., microvascular and macrovascular complications). Their analysis revealed that a significant association existed between depression and diabetic complications (p < .00001, z = 5.94).
Individuals with depression suffer from disability and resulting loss of productivity, and use more health care than those without depression. Based on a one-time cross-sectional sample of 1,051 adults who completed a self-administered web-based Patient Health Questionnaire–9 (PHQ-9; see the appendix), Jain et al. (2013) discovered that 58% of individuals met depression criteria. Also of importance is that depression was associated with decreased work productivity. Egede (2007) conducted a retrospective observational study of 30,801 respondents to the 1999 National Health Interview Survey and identified 975 participants with major depression along with chronic disease. Those respondents with major depression and chronic diseases demonstrated significantly more health care utilization, more functional disability, and less productivity compared with those respondents without major depression.
A collaborative relationship between health care providers can facilitate depression management. Katon, Lin, et al. (2010) conducted a single blind randomized control trial (RCT) of 214 participants who had diabetes, coronary artery disease, or both along with comorbid depression. The intervention consisted of a clinic visit every 2 to 3 weeks during which a nurse monitored the participants’ management of depression, control of chronic disease, and self-care activities. Guideline-based collaborative care with guidance from a primary care physician, psychiatrist, and psychologist were the nurse’s resources. PHQ-9 scores, glycolated hemoglobin, low-density lipoprotein (LDL) cholesterol, and blood pressure were tracked in an electronic registry. After 12 months, participants were re-evaluated with the Symptom Checklist–20 (SLC-20). In addition, their glycolated hemoglobin, LDL cholesterol, and blood pressure were repeated. Compared with the usual care group, the treatment group showed significant improvements in all measures. The need for depression screening and addressing depression in those adults who exhibit symptoms was identified as a beneficial intervention. The TrueBlue study exemplifies this point. In this study, nurses collaborated with a general practitioner, psychologist, and project manager in the delivery of quarterly counseling sessions with patients who had depression along with either diabetes or coronary artery disease. Over a 2-year period, those who received counseling, versus those who were part of the usual care group, had improvements in depression symptoms, body mass index, systolic blood pressure, high-density lipoproteins, and 10-year cardiovascular risk (Schlict, Morgan, & Fuller, 2013). Katon et al. (2012) had similar findings in a RCT of participants with depression and poorly controlled diabetes or coronary artery disease. Participants responded to nurse case manager-facilitated behavioral and clinical guidance with resulting improvements in depression, systolic blood pressure, LDL cholesterol, and HgA1c. An equally important finding was identified during subsequent monitoring of the participants after the RCT. One year after cessation of the nurse case manager’s guidance, clients’ physical parameters worsened. This finding spotlights the importance of continuing an effective process.
Project Design
A process improvement project was designed to address depression in those individuals with chronic illnesses using the Plan-Do-Check-Act framework. The primary purpose of the project was to implement a depression screening program for those with a comorbid diagnosis of hypertension, hyperlipidemia, or diabetes. Another purpose of the project was to provide participants with resources to improve their mental health, and determine whether the process improved depression severity. This process improvement project was constructed as a pre-post comparison of aggregate data evaluating self-reported depression and quality-of-life scores of a population in a worksite health promotion clinic in a southeastern coastal urban setting. Review of the process improvement project was conducted by a local university. The study met the criteria for quality improvement and was exempted from Institutional Review Board approval. The target group was invited to participate in depression screening using the PHQ-9. A quality-of-life measure using the Veteran’s Rand–12 (VR-12) was then administered to the individuals who reported depression. Those who demonstrated depression on the PHQ-9 were offered referral to the employee assistance program, in-network mental health, the supervising physician, clients’ primary care providers, or counseling sessions with the on-site family nurse practitioner (FNP). On-site FNP counseling was offered monthly for individuals with mild or moderate depression and twice a month for those with moderately severe or severe depression. Patient preference was taken into account for scheduling the counseling sessions either via telephone or on-site. Counseling sessions included general health counseling, identification of stress triggers, pre-identified appropriate responses to stress triggers, goal setting, problem-solving, deep breathing, meditation, and sleep hygiene. Principles of motivational interviewing as outlined by Rollnick, Miller, and Butler (2008) were used as a guide. More specifically, the concepts of skillful asking, listening, and informing aided in counseling patients toward change behaviors. Asking open-ended questions, practicing reflective listening, and sharing health-related knowledge were commonly used interview techniques by the nurse practitioner. Outcomes were measured using pre–post intervention scores on the PHQ-9 and VR-12. The instruments were administered during the first month of the program and again at the end of the third month of the program. Intended as a pilot project for participants of a worksite health promotion chronic disease management program, the process improvement program was designed for all individuals enrolled in the worksite health promotion clinic.
Setting and Population
The worksite health promotion clinic is located in the town hall of a municipality. Staffing consisted of an FNP and a medical assistant. An off-site family practice physician was available for consultation as needed. Enrollees consisted of active employees and their spouses, and retirees and their spouses. Types of employees included administrators, firefighters, police officers, recreational specialists, storm and drainage maintenance workers, sanitation workers, and groundskeepers. Designed for employees and spouses who have diagnoses of hypertension, hyperlipidemia, or diabetes, program participants had already been given a financial incentive, reduced insurance premiums, to participate in the town’s disease management program. The clinic was an adjunct to the employees’ health care provided by their primary care professionals.
All clinic disease management enrollees were eligible to participate in the process improvement project. Neither a previous diagnosis of or treatment for depression was a study exclusion. Letters promoting depression screening were sent to the 243 participants in the disease management program. Enrollment in the project was voluntary and did not affect one’s insurance premium cost. Program participants were invited to participate in the project’s five sessions including 2-hour open-house screening opportunities that were conducted in the evenings and on one Saturday. The on-site FNP explained the process to participants on an individual basis. Intake surveys were administered from June 1 to June 30. Post-implementation surveys were collected from September 1 to September 30.
Instruments
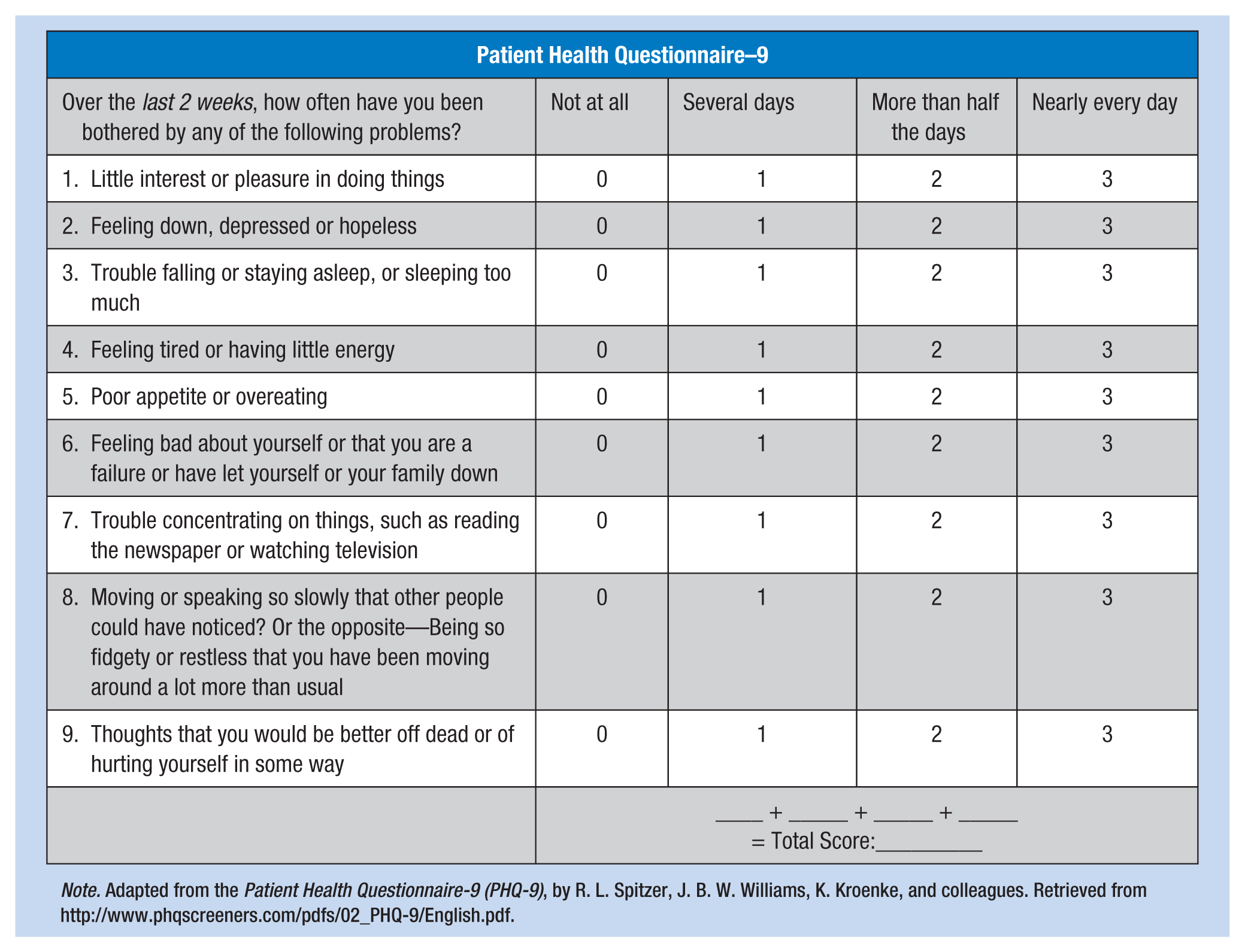
The PHQ-9 is a 9-item self-administered questionnaire that can be completed in five to ten minutes. Each item is scored from zero to three (range of total score 0-27) for symptoms the participants experienced during the previous two weeks. For scores greater than or equal to 10, sensitivity was 88% and specificity was 89% (Kroenke, Spitzer, & Williams, 2001). A score of 0 to 4 indicates no depression, 5 to 9 indicates mild depression, 10 to 14 indicates moderate depression, 15 to19 indicates moderately severe depression, and 20 to 27 indicates severe depression.
The VR-12 is a self-administered survey that measures quality of life and disease burden. It is a comprehensive survey that includes questions regarding eight physical and mental health domains including general health perceptions, physical functioning, role limitations due to physical and emotional problems, bodily pain, energy-fatigue, social functioning, and mental health (Iqbal et al., n.d.). These eight domains include a total of 12 questions that are further categorized into a physical component score (PCS) and a mental component score (MCS). Possible scores range from 0 to 100, with a score of 50 representing an average response. Higher scores reflect a greater sense of well-being, and lower scores reflect a lesser sense of well-being. According to Iqbal et al. (n.d.), the VR-12 is reliable and valid; the Veteran’s Administration has used this tool with approximately 432,000 patients annually. It is also used by the U.S. Centers for Medicare and Medicaid Services and was included in Health Plan Employer Data and Information Set 2007, a performance measurement data set. PHQ-9 data were examined using Microsoft Excel, and VR-12 data were analyzed using statistical analysis software (SAS).
Results
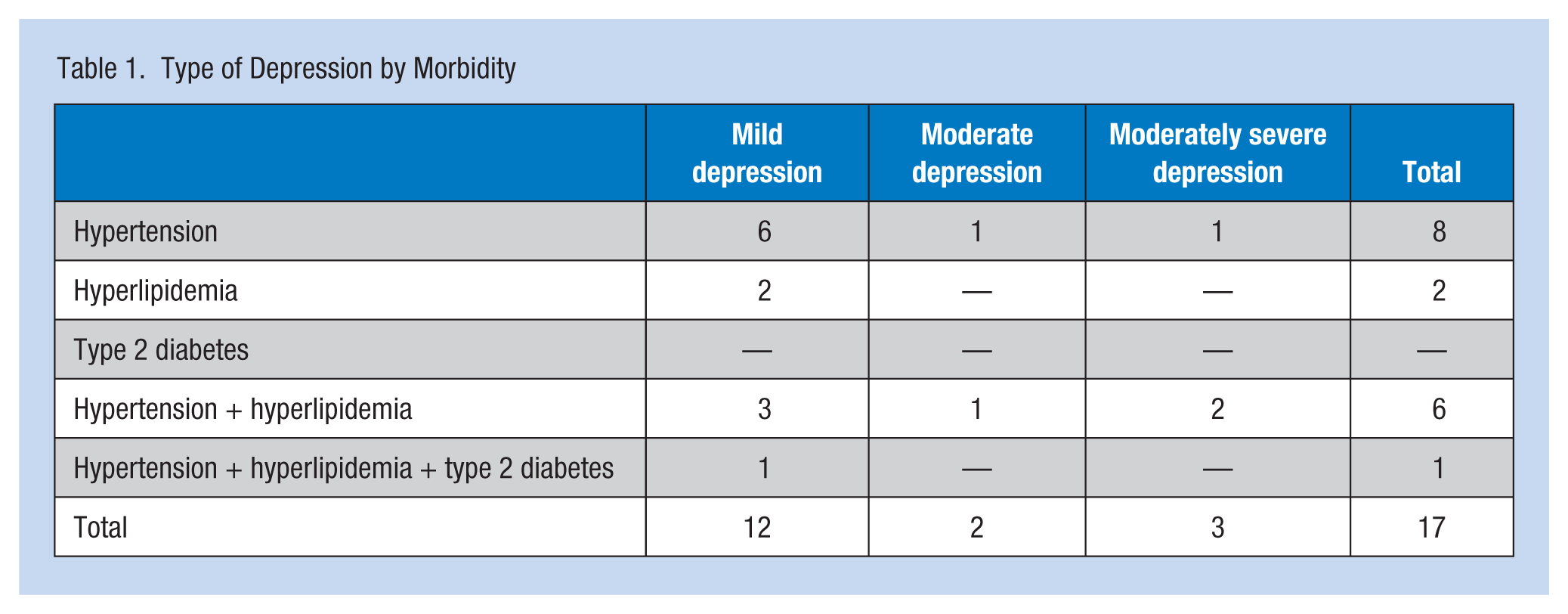
Sixty-nine individuals participated in the screening. Depression was reported by 17 individuals who completed the VR-12. Initially, the prevalence of depression was 24.6%. One participant was terminated from her position and, therefore, did not complete the post-implementation survey. The remaining 16 workers completed the 12-week program. As depicted in Table 1, the initial PHQ-9 results revealed that 12 participants were experiencing mild depression, two participants moderate depression, and three participants moderately severe depression. The median score on the PHQ-9 pre-implementation was 9.3, with a range of 12; the mean PHQ-9 pre-implementation score was 9.3. After the 12-week program, the median and mean PHQ-9 scores were 4.5 and 4.9, respectively, with a range of 11. Pre-intervention VR-12 PCS mean was 45.4, and post-intervention VR-12 PCS was unchanged. VR-12 MCSs had a pre-implementation mean of 43.4, and a post-implementation mean of 50.3. Thus, both depression symptoms and perceived mental health quality of life were improved at the end of the 3-month timeframe.
Type of Depression by Morbidity
Discussion
Depression scores in this sample and setting were higher than expected. Given that the FNP was well established in the clinic and had earned the trust of participants, it is possible that participants felt more comfortable reporting their symptoms compared with studies in which participants completed instruments anonymously. Following the intervention, the number of individuals who met the criteria for a diagnosis of depression was 50% less than before the intervention. At process improvement project completion, the VR-12 MCSs also improved. The findings of this process improvement project are consistent with previously reported findings that a nurse-led clinic is an ideal environment for the provision of effective mental health counseling.
Several limitations of the project were identified. Those employed as police officers were likely underrepresented. Anecdotally, this group verbally expressed concerns about having their mental health documented in a clinic that is part of employees’ human resources department. Reporting bias may also have played a role in the outcome. The target population and the screener had been working together for several years and had developed solid rapport. This situation may have resulted in reporting bias. Had the screener been less known to this population, self-reports of depression and quality-of-life indices may have been reported differently.
The design of the VR-12 is another possible limitation. Response choices are not provided with the same polarity. An individual may have misconstrued the meaning of some of the questions in relation to the other questions. In addition, the use of a scoring algorithm and SAS software is required to analyze the data. For a busy clinician, data analysis is a time-consuming task. A more straightforward quality-of-life instrument might be a better choice for data interpretation.
Conclusion and Implications
In this setting, participants responded positively to self-management and goal setting. An increase in self-efficacy perception increased the potential for better control of chronic illness and cost savings for the health care system. Collaboration with other health care providers, including primary care providers and mental health providers, is strongly recommended. Furthermore, it is crucial for primary care providers to screen and address depression. Assessing and addressing depression in the chronically ill must be viewed as part of the treatment plan similar to regular exercise and healthy diet. Previously mentioned counseling strategies, general health counseling, identification of stress triggers, pre-identified responses to stress triggers, goal setting, deep breathing, meditation, and sleep hygiene, are ideal tools for busy clinicians to incorporate in their care.
This process improvement project, in conjunction with recent literature, suggests that nurses and nurse practitioners can play integral roles in the improvement of chronic disease management outcomes. One of the strengths of this process improvement project is its ability to be replicated in other worksite clinics. Replication and long-term data collection could provide the health care and business communities with necessary data to continue, expand, or improve these programs. Further research about long-term disease management outcomes, the role of collaborative care in such endeavors, and cost containment or improvement for this population of workers is needed.
Footnotes
Appendix
| Patient Health Questionnaire–9 | ||||
|---|---|---|---|---|
| Over the last 2 weeks, how often have you been bothered by any of the following problems? | Not at all | Several days | More than half the days | Nearly every day |
| 1. Little interest or pleasure in doing things | 0 | 1 | 2 | 3 |
| 2. Feeling down, depressed or hopeless | 0 | 1 | 2 | 3 |
| 3. Trouble falling or staying asleep, or sleeping too much | 0 | 1 | 2 | 3 |
| 4. Feeling tired or having little energy | 0 | 1 | 2 | 3 |
| 5. Poor appetite or overeating | 0 | 1 | 2 | 3 |
| 6. Feeling bad about yourself or that you are a failure or have let yourself or your family down | 0 | 1 | 2 | 3 |
| 7. Trouble concentrating on things, such as reading the newspaper or watching television | 0 | 1 | 2 | 3 |
| 8. Moving or speaking so slowly that other people could have noticed? Or the opposite—Being so fidgety or restless that you have been moving around a lot more than usual | 0 | 1 | 2 | 3 |
| 9. Thoughts that you would be better off dead or of hurting yourself in some way | 0 | 1 | 2 | 3 |
| ____ + _____ + _____ + _____ |
||||
Note. Adapted from the Patient Health Questionnaire-9 (PHQ-9), by R. L. Spitzer, J. B. W. Williams, K. Kroenke, and colleagues. Retrieved from http://www.phqscreeners.com/pdfs/02_PHQ-9/English.pdf.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Elizabeth Jensen, DNP, APR N-BC, CNE, is a retired Navy family nurse practitioner who is now faculty at the Medical University of South Carolina. For the past 15 years, her clinical work has been in family practice and worksite health promotion settings.
Bonnie P. Dumas, PhD, MBA, is a biostatistician and Research Assistant Professor in the College of Nursing, Medical University of South Carolina. She is a Six Sigma Black Belt.
Barbara J. Edlund, PhD, ANP, BC, is a professor in the College of Nursing at Medical University of South Carolina and a certified adult nurse practitioner.