
Abstract
Background: Effective smoking cessation interventions (SCIs) are indicated, particularly among the working population, where a higher than expected prevalence of smoking continues. Occupational health nurses’ (OHN) self-efficacy can affect SCI but current scientific literature is limited. The purpose of this integrative literature review was to determine factors that affect OHN self-efficacy and motivation for providing SCI and to guide research needed to enhance SCI programs. Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines, we conducted an integrative literature review. The strategy was an electronic data search of PubMed conducted between 2013 and 2018 and included peer-reviewed manuscripts written in English that addressed self-efficacy and its relationship to SCI. Findings: In total, 15 research articles met the inclusion criteria and two referred specifically to OHNs. Common themes revealed factors which positively and negatively influenced nurses’ self-efficacy, including training, academic preparation, as well as nurse attitudes and personal/social influence. Studies specific to OHNs identify self-efficacy as the most influential factor affecting nurse implementation of SCI. Organizational support and theory-based training are more effective in overcoming personal and social barriers affecting OHN self-efficacy. Conclusion/Application to Practice: The results of this review revealed attitude, innovation, perceived social influence, and self-efficacy were factors for nurses’ intention to implement SCI. Changes in the organizational environment supporting cessation programs and educational development, particularly theory-based training, should be further studied. Our findings suggest that designing programs utilizing these research findings to improve OHN self-efficacy could guide changes in clinical practice for motivating smokers to quit.
Background
Despite a decline in global smoking rates, they continue to be high (World Health Organization [WHO], 2015). In 2015, the WHO predicted that smoking would kill 5 million people annually. In the United States, the Centers for Disease Control and Prevention (CDC) reported that the smoking crisis was affecting about 22% of blue-collar workers. Furthermore, nearly 33 million working adults were currently using tobacco (Syamlal et al., 2017). In the same year, the CDC (2015) reported that 1.5 million workers die or suffer from smoking-related disability and employers spend US$300 billion in lost productivity and medical expenses each year.
These alarming statistics indicate smoking cessation interventions (SCIs) are a necessary health intervention for the American worker who smokes creating an urgent need to further explore and implement effective SCI in the workplace. Cahill and Lancaster (2014) reported that implementing SCI in the workplace was up to three times more effective than interventions in other community settings. A study by Pinsker et al. (2015) found that blue-collar workers had a higher prevalence of daily smoking (88%) compared with white-collar professionals (68%), and blue-collar workers were more likely to use SCI if it were easily accessible, there was no cost, and it took minimal time commitment (Yzer et al., 2015). Smoking continues to be an adverse health determinant for more than 20% of the working population emphasizing a need for employers to maximize effective SCI in the workplace (Syamlal et al., 2017).
SCI has been defined as an “empathetic, personalized approach” with “assistance and follow-up” to help smokers quit (Anczak & Nogler, 2003, p. 203). SCI techniques are supposed to be directed at individual smokers using communication skills which reinforce self-efficacy and are more effective than text messaging and web-based programs (Catley et al., 2015). Findings from the Cochrane Database of Systematic Reviews indicate that nurses can play a key role in advocating and promoting SCI (Rice et al., 2013). Studies have found that nurses are effective at implementing SCI, particularly when they make personalized visits. When patients received more intensive nurse interaction, they were more likely to quit which may be the effect of the nurse-led intervention (Zwar et al., 2015). Furthermore, nursing is the most trusted profession and nurses are skilled at therapeutic communication and face-to-face interactions (Norman, 2016).
A large systematic review by Rice et al. (2013) discovered that nurses did not consistently provide evidence-based techniques for SCI. Studies on nurse barriers for providing SCI included lack of time and organizational support (Leitlein et al., 2013), lack of role identification (Rice et al., 2013), and nurses’ knowledge of SCI and perceived confidence (Fore et al., 2013; Leitlein et al., 2013; Rice et al., 2013). A study by Chatdokmaiprai et al. (2017), specific to OHNs, reported self-efficacy as the single most significant factor for providing SCI. The purpose of this integrated literature review was to determine factors that affect OHN self-efficacy and motivation for providing SCI and to further guide research needed to enhance SCI programs for smokers in the working population. This study focused on nurse’s self-efficacy for providing SCI in clinics, hospitals, and workplace settings.
Conceptual Framework
Bandura’s theory of self-efficacy is an effective model for exploring nurse’s self-efficacy when implementing SCI in the workplace. Albert Bandura defined self-efficacy as the innate thoughts and feelings of an individual for carrying out a task in a situation (Bandura, 1982). Self-efficacy determines an individual’s abilities to cope with obstacles and to initiate a task for achieving a goal (Stajkovic & Luthans, 1998). For instance, the nurse with high self-efficacy will exert sufficient effort in SCI and continue pursuit of various skills and techniques to complete this task, whereas a nurse with low self-efficacy is likely to cease effort. Bandura postulates that a person’s self-efficacy is affected by the environmental setting, social interactions, and one’s own experiences (Bandura, 1997). As for the nurse implementing SCI, self-efficacy is not only concerned about the skills a nurse has but also what a nurse can do under a variety of circumstances that generate competence and confidence. Our use of a conceptual model will guide this review in the interpretation of data and assist in the categorization of factors that may influence an individual’s confidence level when performing or executing a task, that is, influences on nurse’s self-efficacy for engaging in SCI.
Methods
Integrative literature review methods described by Whittemore and Knafl (2005) and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Liberati et al., 2009) were used to conduct this review. The strategy was an electronic data search of PubMed and CINAHL. The following search terms were used: nurse, occupational health, self-efficacy, smoking, cessation, and interventions.
The following inclusion criteria were used to screen the articles: (a) published in a peer-reviewed journal between 2013 and 2018, (b) written in English, and (c) addressed nurse’ self-efficacy and its effect or relationship to SCI. Articles on smoker’s self-efficacy or nurses as smokers were excluded. Also, studies researching other health care providers and not exclusively nurses were excluded.
Abstracts were appraised to determine if the article addressed the research question on nurse’s self-efficacy and SCI. Content of the remaining full-text articles was assessed to determine eligibility based on study quality and research specific to nurses and the research question. A flow diagram was constructed to depict the search and exclusionary process. Studies meeting all inclusion criteria were placed within a table of evidence and analyzed by the identification of categories and themes using qualitative constant comparison (Whittemore & Knafl, 2005).
Results
An electronic database search resulted in 247 articles (Figure 1). Screening for duplication resulted in non-duplicated articles (n = 179) requiring further screening for inclusion. Titles and abstracts were assessed, and articles focusing on smoker’s self-efficacy (n = 115) were excluded. Articles involving studies on other health care providers and not solely on nurses (n = 4) or on nurses as smokers (n = 1) were excluded. Ultimately, 15 peer-reviewed research articles were selected according to the content of the full text and included for analysis (Table 1). Of the 15 articles, two were specific to OHNs and SCI in the workplace.
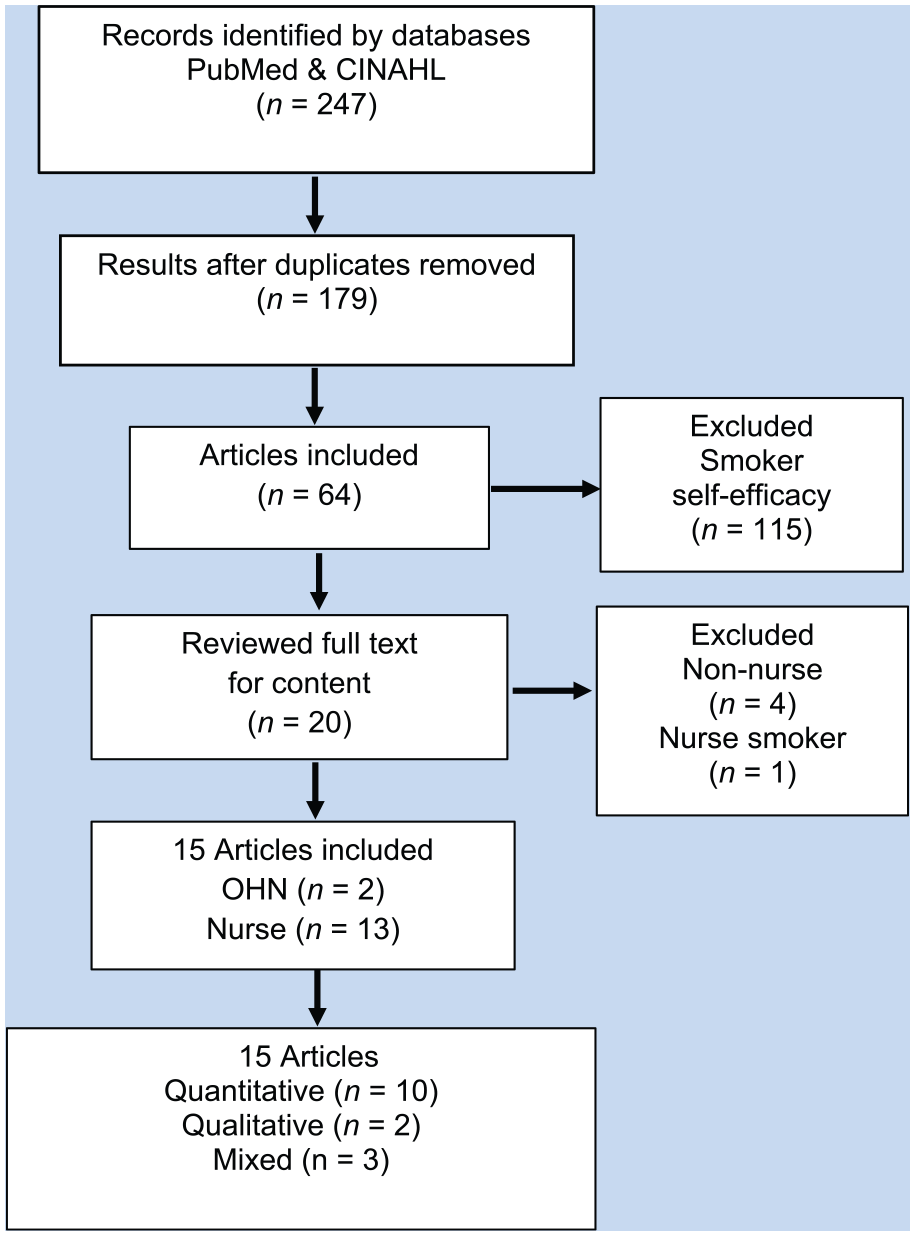
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram depicting the flow of the electronic data search and exclusionary process for the systemic review for self-efficacy and SCI.
Summary of Study Design, Nurse Type, Setting, Context, Intervention, and Outcome
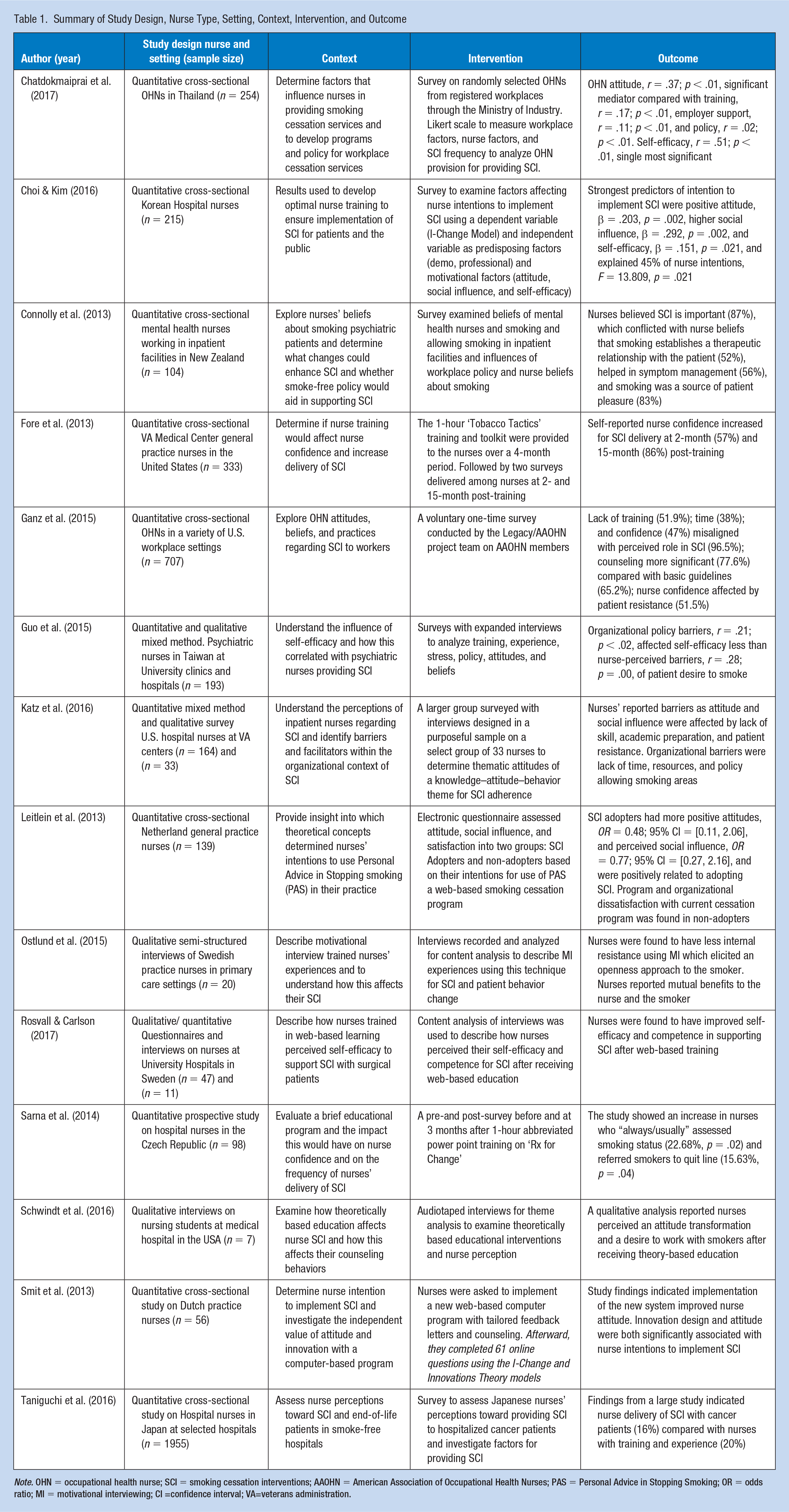
Note. OHN = occupational health nurse; SCI = smoking cessation interventions; AAOHN = American Association of Occupational Health Nurses; PAS = Personal Advice in Stopping Smoking; OR = odds ratio; MI = motivational interviewing; CI =confidence interval; VA=veterans administration.
Characteristics of the Studies
The 15 articles reviewed and analyzed included nine quantitative cross-sectional studies (Chatdokmaiprai et al., 2017; Choi & Kim, 2016; Connolly et al., 2013; Fore et al., 2013; Ganz et al., 2015; Leitlein et al., 2013; Smit et al., 2013; Taniguchi et al., 2016), one quantitative prospective design (Sarna et al., 2014), three mixed-method qualitative–quantitative research designs (Guo et al., 2015; Katz et al., 2016; Rosvall & Carlson, 2017), and two qualitative interview designs (Ostlund et al., 2015; Schwindt et al., 2016).
These 15 studies including nurses from Japan (43%), the United States (27%), Thailand (7%), Korea (5%), Taiwan (5%), the Netherlands (5%), the Czech Republic (3%), New Zealand (3%), and Sweden (2%). The nursing backgrounds and settings included hospitals (49%), OHNs (22%), general practice clinics and primary care (21%), mental health (7%), and student nurses (1%). Most of the studies included cross-sectional surveys to determine what influenced nurse delivery of SCI (Chatdokmaiprai et al., 2017; Choi & Kim, 2016; Connolly et al., 2013; Ganz et al., 2015; Leitlein et al., 2013; Smit et al., 2013; Taniguchi et al., 2016). Two of the research designs used pre-and post-surveys to evaluate educational programs and outcomes of training (Fore et al., 2013; Sarna et al., 2014). Mixed-method studies interviewed volunteers from larger surveys for closer examination (Guo et al., 2015; Katz et al., 2016; Rosvall & Carlson, 2017). Two studies used semi-structured interviews for content analysis (Ostlund et al., 2015) and audiotaped interviews for theme analysis (Schwindt et al., 2016). A table of evidence (Table 1) was constructed summarizing each study’s design, sample size, nurse origin and practice setting, context, intervention, and outcome.
Synthesis of Findings
Two major categories emerged regarding self-efficacy, including (a) nurse characteristics and (b) organizational characteristics. Themes revealed across categories included nurse training, academic preparation, attitude, social influence, and organizational support through policy, time investment, and theory-based training.
Nurse Characteristics
Training and Academic Preparation
In a survey conducted by the American Association of Occupational Health Nurses (AAOHN), training considerations were of concern to nurses for intentions to deliver SCI. Ganz et al. (2015) examined OHN attitudes, beliefs, and practices (n = 707) related to SCI and found that OHNs believed the AAOHN practice guidelines were effective and that their role was important for helping smokers quit (96.5%). About half of the respondents (51.9%) claimed that they had never received SCI training and did not feel confident in their abilities to deliver SCI (47%) but were interested in receiving training (65.1%). The researchers concluded that nurses who lacked training had less confidence and training was an indicator for nurse intentions to provide SCI. In a study by Chatdokmaiprai et al. (2017), training was a significant determinant affecting OHNs’ intentions for SCI. The researchers found of several mediators affecting self-efficacy; training had the strongest influence for implementing SCI, r = .17; p < .01, which positively influenced OHN self-efficacy for providing SCI, r = .51; p < .01, and self-efficacy had the greatest influence in promoting SCI to workers.
Sarna et al. (2014) determined a brief educational program for general practicing nurses had a positive impact on providing SCI. The researchers found nurses who received training resulted in increased knowledge and skills, showed stronger self-confidence and role identification in providing SCI, yet the training program was less effective for nurses who smoked.
Rosvall and Carlson (2017) explored the impact of a web-based SCI educational program for nurses. At 3 months after the training was completed, surveys and semi-structured interviews indicated the nurses’ perceived improved self-efficacy and demonstrated increased competence in providing SCI. In addition, Fore et al. (2013) found nurses who received an intense but brief educational module and were satisfied with their training demonstrated increased self-confidence in delivering SCI. Nurses’ perceived self-confidence was increased over time at 2-month (57%) and 15-month (86%) post-training, respectively. These studies indicate that training had a significant effect (p < .0001) on nurse’s self-efficacy for providing SCI.
Katz et al. (2016) found knowledge through personalized training and academic preparation were positive factors affecting nurse intentions for delivering SCI. Researchers conducted interviews of 164 nurses and discovered a knowledge–attitude–behavior theme which emerged in nurse adherence to SCI. Lack of training, skills, and skepticism about effectiveness of smoking cessation guidelines were barriers for nurse intentions to deliver SCI. In a large study by Taniguchi et al. (2016), Japanese nurses (n = 1,955) were surveyed to assess their perceptions toward providing SCI to hospitalized cancer patients. They found nurses having smoking cessation training and experience counseling smokers during academic preparation had increase intentions for delivering SCI (20%) compared with those who did not have training and experience (16%). The research suggests training and academic preparation is a significant factor for nurse intentions to deliver SCI while working with similar end-of-life cancer patients.
Attitude and Social Influence
Choi and Kim (2016) evaluated Korean nurses (n = 215) and predisposing factors which affect their intention to implement SCI in a self-administered questionnaire. The authors found significant predictors of intention to implement SCI, including a more positive attitude, β = .203, p = .002, higher social influence, β = .292, p <.001, and higher self-efficacy, β = .151, p = .021. Although attitude and social influence were predictors, self-efficacy and nurses’ level of perceived social influence was found to have the greatest predictor for SCI. Leitlein et al. (2013) investigated considerations for nurses’ implementation of SCI. The authors surveyed 139 nurses for attitude, social influence, and satisfaction. The responders were separated into two groups: SCI adopters and non-adopters, finding nurses’ attitude and social influence were positively related to adopting SCI. A logistic regression with determinants of SCI adopters presented significantly more positive attitudes, OR = 0.48; 95% CI = [0.11, 2.06], and perceived social influence, OR = 0.77; 95% CI = [0.27, 2.16]. Katz et al. (2016) used a mixed-method approach and found nurse’s attitudes were affected by skepticism about the effectiveness of smoking cessation guidelines and patient disinterest or resistance in quitting. These personal and social attitudes created negative internal barriers for nurses and affected behaviors for SCI delivery.
Chatdokmaiprai et al. (2017) determined variable mediators significantly correlated with providing SCI. The findings indicated OHN attitude, r = .37; p < .01, was the most significant mediator compared with training, r = .17; p < .01, employer support, r =.11; p < .01, and policy, r = .02; p < .01, for positively influencing OHN self-efficacy and SCI, r = .51; p < .01. Ganz et al. (2015) found OHNs believe practice guidelines are effective and have an important role in delivering SCI (96.5%). OHN attitude for discussing plans to quit and cessation counseling was more significant (77.6%) compared with providing counseling on basic guidelines (65.2%), and less significant was resistance to OHN advice (51.5%).
Two studies on mental health nurses revealed barriers to SCI delivery with smoking psychiatric patients. Connolly et al. (2013) surveyed nurses (n = 104) caring for smoking mental health clients in inpatient facilities. They discovered that 83% of the nurses believed smoking relaxes the client and is a source of patient pleasure and helps them cope. Although 87% of the nurses believed it was their role to support clients to be smoke-free, 52% perceived their acceptance of the smoking behaviors was helpful to establish a therapeutic relationship, and 56% believed smoking helped with symptoms management. The researchers suggested an important outcome of this study was to focus on the nurse’s role in finding healthy ways of establishing a client relationship (Connolly et al., 2013). Guo et al. (2015) also studied the social behaviors of psychiatric nurses and their attitudes for providing SCI services. The nurses (n = 193) reported their experiences with the smoker and that their understanding of the patients’ motivations to smoke were “self-treatment.” The nurses reported low scores for self-efficacy correlating with low efforts for SCI (scores 20.4-55.3 on a scale of 100) and their perception of the patient’s self-treatment was the most critical factors in providing SCI services. The researchers suggested that nurses should establish an awareness of patient motivations to smoke so they can be accurately assessed for SCI (Guo et al., 2015).
Organizational Characteristics
Support Through Policy
After interviewing nurses in VA clinics, Katz et al. (2016) found barriers to SCI due to lack of organizational policies to ban smoking. The nurses reported they felt helpless without administrative support during patient interviews. They claimed when attempting to educate patients on smoking cessation, the patients could easily access smoking areas, and without institutional support, the nurses felt their efforts to implement SCI were undermined.
Guo et al. (2015) surveyed psychiatric nurses and found a positive but weak correlation on self-efficacy to the effects of a smoke-free policy, r = .21; p < .02. Policy and institutional restrictions on smoking were not a significant factor for nurse’s self-efficacy compared with nurse-perceived barriers, r = .28; p = .00; for example, the nurses’ understanding of the patients’ motivation to smoke. Another study by Chatdokmaiprai et al. (2017) found employer support directly and positively influenced delivery of SCI by nurses but did not significantly influence nurse’s self-efficacy.
Chatdokmaiprai et al. (2017) found OHNs were more likely to provide cessation services when their employers had tobacco control policies. Another study by Ganz et al. (2015) found about one quarter of OHNs surveyed had practice guidelines in their work settings but did not have the resources needed to support smoking cessation development programs and were not receiving reimbursement for providing SCI. Chatdokmaiprai et al. (2017) and Ganz et al. (2015) concluded employers need to establish smoke-free policies and provide resources to both employees and nurses to improve SCI services. These processes or procedures for both smokers and nurses can facilitate OHN delivery of SCI (Ganz et al., 2015).
Time Investment
Several articles reported external factors, such as time investment and organizational commitment, affecting nurses’ intentions to provide SCI (Ganz et al., 2015; Katz et al., 2016; Leitlein et al., 2013; Ostlund et al., 2015). Nurses at veteran hospitals were interviewed by Katz et al. (2016) who reported organizational barriers as insufficient time with heavy workloads which prevented them from providing SCI. Nurses were discouraged because it was difficult to “find the time it takes to talk” along with limited resources affecting their behaviors in delivering SCI. (Katz et al., 2016). In a study by Leitlein et al. (2013), nurses were categorized as “non-adopters,” believing SCI is “too time-consuming” and dissatisfaction with current cessation program activities. In a study by Ganz et al. (2015), one third of OHNs surveyed had competing priorities and time constraints preventing them from assisting smokers. Ostlund et al. (2015) interviewed nurses trained to use motivational interviewing (MI) techniques for SCI and found nurses did neither have the time it takes to interview patients properly nor were they able to reflect on patient responses and feedback for methods used. Ostlund et al. (2015) suggested time invested in training and supporting nurses using MI techniques would make significant public health advancements.
Theory-Based Training
Articles specific to theory-based training described how techniques using MI affected the nurse–patient relationship. Ostlund et al. (2015) conducted semi-structured interviews with nurses who used theory-based SCI with smokers. Researchers found mutual benefits to the nurses and the patients. Nurses experienced less internal resistance using MI, which elicited an openness from the smoker. Consequently, the MI approach was helpful for alleviating emotional stress for both nurses and smoking patients (Ostlund et al., 2015).
Schwindt et al. (2016) examined theoretically based educational interventions and nurse perception for how this affects counseling behaviors using SCI. Researchers found nursing students applied concepts of empathy and developed a non-judgmental attitude. Nurse interviewees responded with an understanding of the therapeutic approach and explained they felt these behaviors were exhibited during patient encounters. The theory-based education helped them overcome negative perceptions about the smoker and created a transformational desire in the nurse to work with their smoking patient. Ultimately, the benefits of theory-based education were found effective in establishing a therapeutic partnership with the smoker.
Smit et al. (2013) used a theory-based implementation strategy, Diffusion of Innovations theory (Rogers, 1995), and asked nurses to use a new web-based computer SCI program and begin recruiting smokers as a trial. Nurses completed 61 online questions using the I-Change and Innovations Theory models after implementing a new web-based computer program. Rogers’ Diffusion of Innovations theory integrates three characteristics: attitude, social influence, and self-efficacy. The researchers determined, while having the nurse use a new program, multiple cognitive factors occurred in a progression of phases: knowledge, persuasion, decision-making, implementation, and confirmation which led to nurse initiation. They also found nurses with a positive attitude toward the new computer-tailored SC program correlated with the nurses’ initiative to implement the program. Furthermore, Smit et al. (2013) found that implementing the program and use of an innovative practice model generated a multiplying affect and attitude, innovation, perceived social influence, and self-efficacy were all factors affecting nurse intentions to implement SCI.
Discussion
This review reports data from a focused area of literature exploring factors affecting nurses and self-efficacy in providing SCI. There were insufficient studies of OHN’s to focus solely on them. Organizational characteristics, such as lack of time, conflicting policies, and limited provisions for training, particularly theory-based training, were discussed as external negative factors affecting nurse attitudes and behaviors in SCI delivery. Such organizational barriers created a perpetuation of ineffective behaviors and non-stimulating cessation programs. In the theory of self-efficacy, an individual must be able to regulate their environment to feel confident in performing and attaining a skill or behavior. Policies that do not support SCI programs or a smoke-free environment create barriers and deregulate nurse intentions. Consequently, a work setting allowing employees time to talk with the nurse about smoking cessation is a better business investment than employee time spent at the smoke stand. These changes in practice and policy support an environment conducive to promoting SCI and give the nurse a feeling of control. Aligning company goals and objectives for time and financial to support smoking cessation can promote self-efficacy for both the nurses and employees.
This review indicates nurse characteristics are predictive of SCI implementation. The internal negative factors related to nurse self-efficacy describe lower levels of knowledge, skill, experience, and education. Training improves nurse self-efficacy, and theory-based training is even more effective in affecting nurse confidence and influence with the smoker. Bandura described self-efficacy as an individual’s perceived abilities to perform and execute a task. These abilities improve through practice, persuasion, and by watching others (Bandura, 1997). Studies utilizing training which incorporates theory-based learning were all effective in increasing nurses’ self-efficacy and should be a consideration for improving SCI.
Also described were nurses’ adverse attitudes toward a willingness to provide SCI. Social influence was affected by perceived patient resistance and misconception of the smokers’ intentions to quit. Bandura (1995) believed behavior is an outcome of social expectancies and incentives received from others. When nurses experience resistance from smokers they are faced with feelings of lesser self-efficacy. Mental health nurses lost their incentive when smoking was perceived as a benefit for psychiatric patients. These perceptions were negative influences on nurse self-efficacy in providing SCI. Specifically, OHNs reported barriers, including lack of training, poor self-efficacy, and perceptions of smoker résistance which prevented them from providing SCI services to workers. Time limitations and competing priorities were negative external barriers for assisting smokers but most respondents (51.5%) claim smoker resistance to their advice is a greater barrier (Ganz et al., 2015), and poor self-efficacy is related to lower SCI rates.
MI and theory-based techniques are described as successful in motivating smokers to quit while also motivating nurses to provide SCI. Personal barriers created by preconceived thoughts on smoker intentions to quit and internal resistance can be overcome using MI. A conducive social environment is created through MI enhancing a therapeutic relationship with mutual benefits for the smoker and the nurse. The introduction of an innovative SCI program increased nurse implementation rates and suggested that attitude, social influence, and self-efficacy are cognitive motivators for delivering SCI. Inferences can be made from this review to reveal theory-based training, positive nurse attitudes, perceived influence on the smoker, and innovations improve nurse self-efficacy and that nurses experienced a transformation when using MI techniques. These findings highlight relationships in research for developing SCI programs and projects conducive for OHN self-efficacy in SCI.
Limitations
This review had several limitations. The literature search was conducted by one author reviewing abstracts from many articles extracted from two databases. Also, the author screened for the focus areas from the articles on SCI and subjectively determined themes for OHN and nurse self-efficacy. Generalizability was affected due to the paucity of evidence related to OHNs. Conclusions were drawn from a larger population of a variety of practice nurses. Furthermore, most of the studies were from varied settings and multiple countries outside of the United States.
Conclusion
Use of a conceptual model provided strength for clear selection of themes and interpreting data for analysis. Although current evidence regarding OHNs self-efficacy in SCI is limited, this review could serve as a gateway for future program development. Nursing research specific to occupational health programs could facilitate nursing practice to address the amelioration of an unexpectedly high incidence of smoking among workers. Existing practice settings should aim to resolve internal and external difficulties facing nurses and develop ongoing training solutions for theory-based interventions. Research should identify programs specific to the occupational health setting and SCI training that supports individual environmental, social, and behavioral aspects. Program designs should address not only external factors related to organizational barriers but also internal, personal factors for developing an empathetic, non-judgmental approach without making assumptions about the smoker’s desire to quit. Future studies will be necessary to develop innovative programs for SCI in the occupational health setting and to stimulate nurse confidence and motivation. These changes, in practice, will support the utilization of OHNs as effective agents in reducing smoking rates and improving the health outcomes of workers.
As OHNs advance total worker health, the ability to motivate change will begin with the OHN who feels personally motivated to intervene for change. A dynamic step in preventing smoking illness and disability lies in the OHN-worker communication pathway and poor self-efficacy is related to lower SCI rates. The hierarchy of controls in the Total Worker Health (TWH) model eliminates, substitutes, and redesigns the workplace (CDC, 2018) but without considerations for OHN self-efficacy, the core application of education and personal encouragement could be lost. Implications for research include projects and new concepts utilizing theoretically based strategies to combine principles of self-efficacy, the power to change, and innovative ways to operationalize the OHN in changing at-risk behaviors.
In Summary
Smoking continues at unexpectedly high creating ongoing health implications for many American workers
Despite effective evidence-based practices guidelines for smoking cessation, nurses report they do not consistently deliver this life-saving message
Self-efficacy is found to be the single most significant factor predicting OHN delivery of SCI
An integrative literature review was conducted to discover that common themes affect nurse’s self-efficacy for SCI delivery, including theory-based training, personal, and social influences
Findings from this integrative literature review will be used for future studies to design projects to improve OHN self-efficacy and increase SCI in the workplace
Applying Research to Practice
Occupational Health Nurses (OHN’s) who want to provide smoking cessation interventions (SCI) must assess their competency and barriers to self efficacy. Occupational Health Program Managers should be aware of and address self-efficacy barriers and provide Motivational Interviewing (MI) and other theory-based training as well as organizational support such as tobacco control policies in order to improve self efficacy of nurses providing SCI. Rice et al. (2013) discovered nurses are effective in assisting patients with quitting smoking but do not consistently deliver evidence-based practice guidelines. In a recent study (Chatdokmaiprai et al., 2017), researchers found OHN self-efficacy was the single most significant factor predicting the provision of SCI to workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Amy Thornberry, DNP, APRN, FNP-C, COHN-S is the primary author. She is a nurse practitioner and certified Occupational Health Nurse and Leader for the Occupational Health Programs at Celanese North America. She was the primary contributor to the design of the work, acquisition, analysis, and interpretation of data.
Theresa J. Garcia, PhD, RN is an Assistant Professor of nursing at Texas A&M Corpus Christi College of Nursing and Health Sciences, contributing to the analysis and interpretation of data and critical revision for intellectual content.
Jessica Peck, DNP, RN, CPNP-PC, CNE, CNL is a nurse practitioner and professor of nursing, contributing by analysis and interpretation of data, critical revision, and final approval of the version to be submitted.
Elizabeth Sefcik, PhD, RN, GNP, BC is an Assistant Professor at Texas A&M Corpus Christi College of Nursing and Health Sciences, contributing to revision, accuracy, and integrity of the final version.