
Abstract
Background: The incidence of alcohol and substance misuse continues to be a problem in the workplace. Methods: A partnership between two universities and a federal agency implemented SBIRT (Screening, Brief Intervention, and Referral to Treatment) into a three-credit, 7-week online Community and Environmental Health Course for licensed nurses earning their Bachelor of Science in Nursing degree. SBIRT is an early intervention, targeting nondependent substance users before needing specialized treatment. Findings: Over seven semesters, 119 students completed the SBIRT curriculum. We observed a significant increase in knowledge about standard drink sizes and recognizing the most reliable alcohol use questionnaire (Alcohol Use Disorders Identification Test [AUDIT]). Students perceived themselves as competent in assessing patient readiness to change, making the best treatment decisions, and referring patients for appropriate care. Most students found significant value of SBIRT in their current practice setting. Conclusion/Application to Practice: The SBIRT curriculum was found to be a valuable tool for nurses in screening and referring patients to care who are at risk of alcohol and drug misuse. It is important for occupational health nurses to learn the necessary skills for assessing workers for alcohol and drug misuse. The occupational health nurse is encouraged to practice their skills at every patient encounter for purposes of refining their skills. Employers are concerned about drug and alcohol misuse in the workplace and occupational health nurses are the optimal group to intervene with workers who need assistance.
Keywords
Background
In 2015, a university in the mid-Atlantic region of the United States was awarded a grant within the School of Health Sciences (SHS) by the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Center for Substance Abuse Treatment (CSAT). The purpose of the grant was to implement Screening, Brief Intervention, and Referral to Treatment (SBIRT) training as part of the Health Professions Student Training (SBIRT–Student Training) grant. The grant was a community partnership and collaboration between the university’s SHS, the School of Pharmacy of a neighboring research University, and a Family Practice Residency Program of a local health network. The SBIRT modules were embedded into the curricula of the SHS programs and faculty were recruited as “Champions” within the Physician Assistant, Occupational Therapy, Physical Therapy, Nursing, and Counseling Psychology programs to promote SBIRT in their programs, thus affecting clinical change at all levels.
SBIRT
SBIRT is a comprehensive public health approach for the delivery of early intervention and treatment services through universal screening of persons at risk of developing substance use disorders, as well as those currently misusing substances. The core components of SBIRT include (a) screening with validated screening tools and motivational interviewing procedures to assess patient usage risk; (b) use of screening results to select the appropriate level of care; (c) administering a brief intervention aimed at helping the patient understand current risks and initiating the process of behavior change through a short 5- to 15-minute discussion; and (d) referring the patient to more extensive treatment with access to specialty care when appropriate. The goal is identification of behavioral health problems, even if the patient is not currently seeking intervention or treatment (SAMHSA White Paper, 2011). SBIRT has been used in a broad range of health care settings, including emergency departments, hospitals, primary care, workplace wellness programs, rehabilitation facilities, long-term care, colleges, and universities (SAMHSA White Paper, 2011).
As part of this effort, the SAMHSA Center for Integrated Health Solutions (CIHS) collected and populated a library of resources to guide users in applying these principles in the community. The key feature to ensure a successful SBIRT intervention is the use of motivational interviewing techniques that focuses on four basic principles, including (a) expressing empathy and avoiding arguing, (b) developing motivation to change, (c) rolling with ambivalence, and (d) supporting self-efficacy (the client’s belief of their ability to successfully make a change) (Brobeck, Bergh, Odencrants, & Hildingh, 2011).
SAMHSA has reported that SBIRT screening can be cost-effective, saving US$3.81 in health care costs for every dollar spent on intervention (Gentilello, Ebel, Wickizer, Salkever, & Rivara, 2005; SAMHSA White Paper, 2011). The National Institute on Drug Abuse (2017) reported that the overall cost of substance misuse was US$300 billion for tobacco (2010), US$249 billion for alcohol (2010), US$193 billion for illicit drugs (2007), and US$78.5 billion (2013) for prescription opioids. These figures included annual costs for crime, lost work productivity, and health care. In the United States in 2017, 15.8% of men and 12.2% of women were smokers (Centers for Disease Control and Prevention, 2019) despite 50 years of anti-tobacco campaigning. Talbott Recovery (2018) and Ahrnsbrak, Bose, Hedden, Lipari, and Park-Lee (2017) observed in a national study on drug use and health in 2016 that approximately 10% of the U.S. population 12 years of age and older (28.6 million people) reported using illicit drugs (including addicting prescription drugs) in the prior month. In addition, the 2018 National Institute on Drug Abuse (2019) revealed that more than 130 Americans die each day from opioid overdose.
Nurses are often the first medical professional to assess a patient, making them ideal candidates to use SBIRT techniques to identify patients in need. Since a Gallup Poll from December 2017 rated nurses as the most honest and ethical profession for the 16th consecutive year by 82% of the respondents (Brenan, 2017), nurses are valuable partners, along with physicians and pharmacists in promoting SBIRT principles and implementing the model of universal SBIRT screening for every patient encountered.
Integrating SBIRT into a Community and Environmental Online Course
The course selected for implementation of the SBIRT modules within the Registered Nurse–Bachelor of Science of Nursing (RN-BSN) curriculum at the University was Community and Environmental Health, which first began in 2016. This was a three-credit hour, 7-week course. The students were RNs working in a variety of settings, with experience ranging from being recently licensed to many years. Class sizes ranged from six to 20 students. This report covers seven semesters from January 2016 through April 2018.
The SBIRT modules were developed by a grant partner and delivered using audio/visual online presentations. The six course-learning modules included the following core topics: (a) Introduction to SBIRT, (b) Screening, (c) Brief Intervention, (d) Referral to Treatment, (e) Medical and Psychiatric Complications of Commonly Misused Substances, and (f) Pharmacotherapy for Substance Use Disorders. Students received information directing them how to log into the SBIRT course introductory module and complete an informed consent agreement and an online survey to validate “pre-testing” knowledge. Two YouTube videos were viewed by students to provide a brief overview of the SBIRT concepts: “Alcohol & Drug Education for Prevention & Treatment (ADEPT)” (Boles & Boles, n.d.) along with how it has been used productively by Denver Health (SBIRT Program at Denver Health, 2010). Students then completed the six core-learning modules over the first 3 weeks of the course, which took approximately 6 hours. All materials were provided online including interactive modules with all instructions provided to facilitate self-study at the preferred pace of the student. Following the viewing of each module, a quiz was administered requiring a 100% pass rate, which they were able to re-take as many times as necessary. There was minimal intervention required by the instructor to assist students.
SBIRT modules were designed to be relevant to nurses and the nursing practice environment. This included insertion of practice exercises, case-studies, and YouTube videos that used examples modeled as actual nursing scenarios. In addition, a packet of information with local and national resources, along with a pocket information card that defines low-risk drinking limits, what is a standard drink, cues such as sample questions to facilitate the screening, and tips to help the nurse be more effective in working with patients was given to all students to help them achieve and maintain SBIRT proficiency.
As part of SBIRT training, an interprofessional discussion forum was initiated by course instructors in the university’s learning management system (e.g., Moodle), designed to facilitate discussion among the various professions and reinforce learning. Students were able to share differing viewpoints as their approach and delivery of patient care may be different based on their profession. During the discussion, course instructors monitored student comments and helped stimulate further conversations. This forum mirrored the clinical collaboration present in most practices today, helping multiple disciplines work more effectively as a team and enhancing patient care (Johnson & Johnson, 2016).
In this discussion forum, students were assigned to read an article from a local newspaper detailing a woman’s experience who lost her mother due to mental health issues, alcohol dependence, and prescription drug misuse (Jackson, 2016). They then viewed a video that included testimonials of several drug and alcohol users (SBIRT Oregon, 2014). Students were then expected to post their comments in the discussion forum, which were to include (a) their discipline and practice setting, (b) how the article and video informed and/or altered their patient/client approach, and (c) comments on any biases or assumptions about patients struggling with drug and/or alcohol misuse the student may have brought with them into the class. In addition, they were asked to respond to the posts of two students not in their discipline. The goal was to identify common perceptions about the case, discussing different approaches to care delivery and bridging professional differences in approaching a common health care scenario (Johnson & Johnson, 2016).
After completion of the SBIRT modules, the nursing students, who work in areas such as medical-surgical nursing, orthopedics, neurology, physical rehabilitation, and emergency, were required to practice their newly acquired skills for the next 30 days and then assess what they learned through a self-evaluation form.
Data Collection
To promote continuous quality improvement in the course, feedback was collected from the instructor and students by a grant partner who served as the evaluator. A pre-training survey collected student demographic information, levels of prior education about drug and alcohol use, past involvement in caring of patients with drug and alcohol misuse problems, and numbers of patients currently seen with drug and alcohol misuse problems. Other information ascertained included knowledge about standard drink sizes, perceived self-confidence of students when working with alcohol/drug impaired patients, and the frequency with which the nursing students engaged patients in discussions about their substance usage. Questions were asked before and after training to measure effectiveness of the modules and student learning.
Upon completion of the modules, at least three students from each class were recruited to participate in a focus group to discuss the perceived effectiveness of the course modules, communications with faculty, and suggestions for improvement of the course. Similar questions were asked of the instructor with the goal of using these data to improve future sessions of the course. The course instruction team met after the completion of each course to consider the feedback from students and evaluate potential changes to improve the course. In the last week of the class, students were asked to comment on use of SBIRT in their practice and how helpful the curriculum had been to them in their practice. All comments were evaluated as a basis for making future course improvements by the course instruction team.
Findings
Data were compiled and analyzed by the grant partner from the pre- and post-training surveys over seven semesters from January 2016 to May 2018. A total of 128 students were enrolled and 119 (93%) completed the SBIRT training evaluation required of the grant. A total of 101 (91%) students completed the pre- and post-training evaluations. Results demonstrated that most students (83%) reported they felt the information received from the instructor during the SBIRT training was useful in their practice. Furthermore, survey results showed that only 14% of students demonstrated correct knowledge of a “standard drink” size before training, whereas 34% demonstrated this knowledge on post-training surveys. Similarly, 8% of students had a correct understanding of drinking limits in the pre-training survey, with an increase to 37% that answered correctly after training. In addition, in the pre-training period, the AUDIT (Alcohol Use Disorders Identification Test; World Health Organization, 1987) questionnaire was recognized by 34% of students as the most reliable screening tool to identify alcohol misuse, with an increase to 65% after training.
Student self-perceived competence in conducting aspects of SBIRT and patient care (including screenings, brief intervention, referral to treatment, and documentation of care) was assessed on a 4-point Likert-type scale, with 1 = competent and 4 = not at all competent. Lower Likert-type scores signified a higher level of perceived competence. Students’ mean self-perceived ability to screen for substance misuse was 2.01 pre-training and an improvement to 1.77 after training. When assessing the patient’s readiness to change behavior, the student mean score was 2.48 pre-training and improved to 1.95 post-training. Other areas of positive improvement included making the best treatment decisions based on gathered evidence (2.26 pre-training and 1.86 post-training) and the ability to refer the patient for appropriate care that best benefits the patient (2.42 pre-training and 1.94 post-training). Students already considered themselves adept at care documentation before starting the course (pre-training 1.97 and post-training 1.73) a moderate improvement in their self-perceived competence.
Student Comments About SBIRT
Most students found significant value of SBIRT training in their current practice setting. Among the comments received,
“The SBIRT Curriculum made me a better screener for substance abuse and other sensitive health history topics . . . It was a lot of work, but an important responsibility as a nurse, and an area where we could improve”;
“I found the SBIRT curriculum to be one of the greatest and most useful areas of learning from this class . . .”;
“I enjoyed the SBIRT curriculum, mostly because of how prevalent drug and alcohol use and abuse is in my current patient population. Adding screening tools to my assessment has been useful . . .”;
“I think the SBIRT training was really useful. I see a lot of people come into my unit who are withdrawing from alcohol and drug overdoses . . . I have been able to talk to people when they come out on the other end of withdrawal. Usually at that point they agree to quit drinking or stop doing drugs . . . The one thing I do not like, is that I do not know what happens to my patients after they leave my unit. I wish I did . . .”
“I can say that in my current position, the SBIRT training has been a lot of help. I now work in a primary care office and I assist the physicians in assessing patient’s perception of drug and alcohol misuse. So, for this reason, it really was a great asset.”
We also received some beneficial comments through the interprofessional discussion forum postings over the second year of the grant. Anecdotal remarks included the willingness of patients to talk about their substance use with nurses, that patients struggling with substance use are seeking support and hope, and to encourage nurses about their role in initiating conversations and offering resources to patients.
Plans for Sustaining SBIRT in the Nursing Program
The SBIRT modules were installed as an activity in all three online nursing programs at the university including the RN-BSN, MSN, and DNP programs. The selected RN-BSN course housing the SBIRT modules was the Global Cultural Diversity and Specialty Population Nursing course. For MSN students, the selected course is Health Assessment and Promotion Across the Lifespan. In the DNP program, the instructor introduces SBIRT to all students in the second half of the Developing Evidence-Based Practice course. As in the other programs, students will be given directions within the course, as well as be able to go to the Nursing Student site for self-enrollment and access to all course modules. Having all SBIRT modules readily accessible provides all students an opportunity to complete the modules and receive an SBIRT Completion Certificate. Students are strongly encouraged to complete all modules, supplementing their assessment skills, and earn the SBIRT Completion Certificate.
Implications for Occupational Health Nursing Practice
As SBIRT is being introduced to more nurses, it is important for occupational health nurses to learn the necessary skills for assessing workers for alcohol misuse. Table 1 includes SBIRT resources for the occupational health nurse. Since it can often be difficult for nurses to learn these new skills, the occupational health nurse is encouraged to practice the principles at every patient encounter and to learn from mistakes made (Brobeck et al., 2011). SBIRT and Motivational Interviewing techniques can help workers recognize their individual lifestyle habits (drug usage, smoking, alcohol usage, poor eating habits, and physical inactivity) so they can make positive changes in their daily lives (Brobeck et al., 2011). Brobeck also indicated that occupational health nurses must make the effort to continually use the skills and avoid reverting to their former practice of merely giving advice—a technique that is not very effective in helping workers make positive changes in their lives. Another reason for occupational health nurses to embrace the SBIRT model is the documented concern employers have about employee alcohol misuse in the workplace. According to McPherson et al. (2009), an employer survey found that almost 90% (of 78 employers) reported their company was “very concerned” (50%) or “moderately concerned” (39%) about alcohol misuse. Most companies who were performing screening (n=76) reported it was done by someone other than a supervisor/manager, whereas 12% report that screening was conducted by supervisors/managers. Finnell (2012) and Rubenstein et al., (2010) noted that the communication and organizational skills of nurses and their ability to educate and help motivate workers through short interactions are key in caring for patients at risk for alcohol and other substance misuse. These skills are also in line with the 2010 American Nurses Association [ANA] standards of professional practice and performance (ANA, 2010).
SBIRT Resources for the Occupational Health Nurse
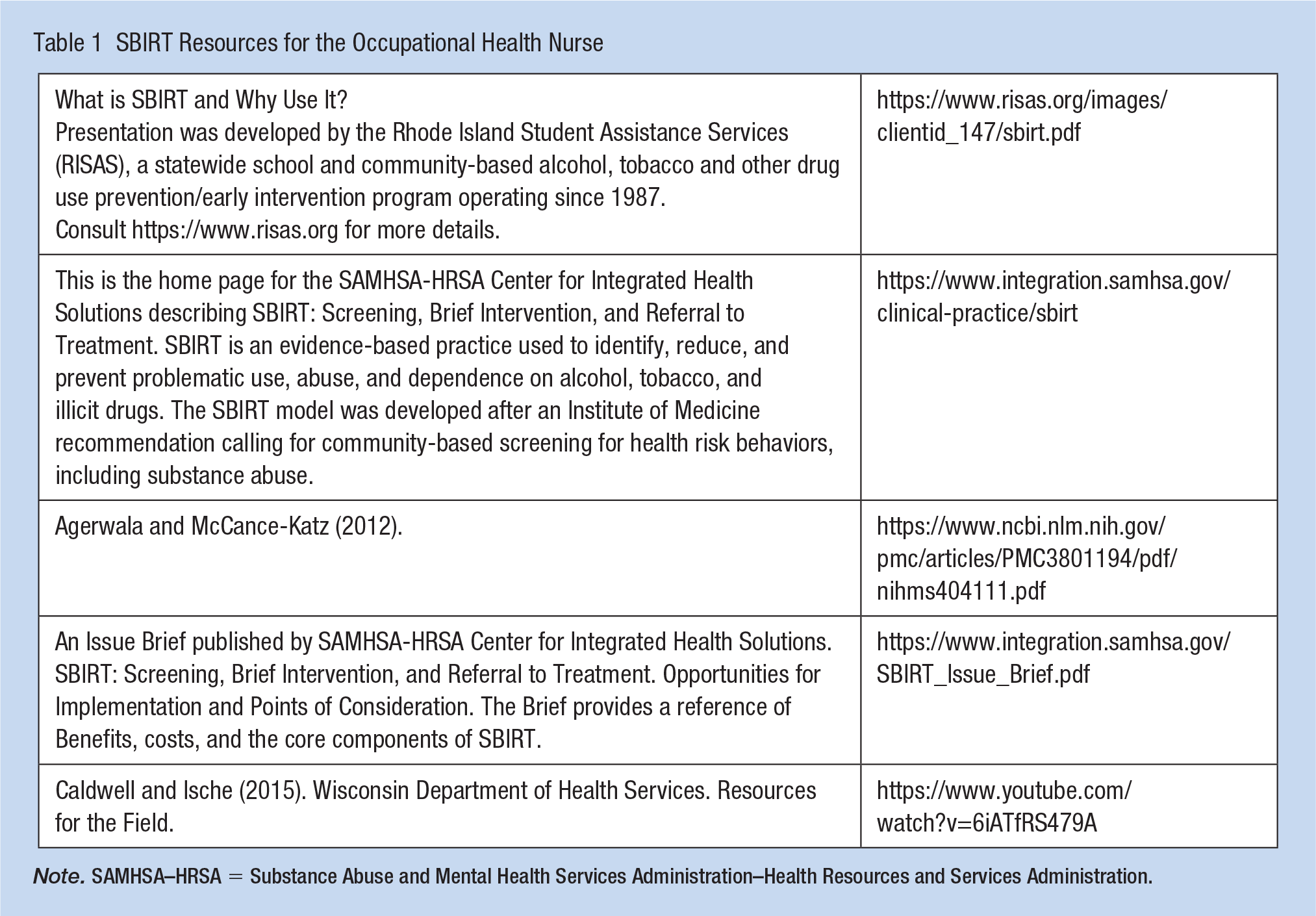
Note. SAMHSA–HRSA = Substance Abuse and Mental Health Services Administration–Health Resources and Services Administration.
Applications to Professional Practice
The purpose of this project was to describe the implementation of SBIRT and detail some of the successes focusing on the basic principles of the course. SBIRT was implemented via online self-study with the goal of training all nurses (including occupational health nurses) to address the negative effects substance misuse and addiction has on society. The belief that occupational health nurses and other health care professionals need to use these techniques to screen all patients at every encounter was consistently promoted during the class exercises. The continuing growth of drug, alcohol, and opioid usage and the associated medical costs shows that all medical professionals, including occupational health nurses, need to be trained in the valuable skills of SBIRT and Motivational Interviewing. Occupational health nurses need to master these new skills, providing a pathway toward better employee health, as well as reducing employer health care costs.
Footnotes
Acknowledgements
The author would like to thank the following for their efforts, assistance, and support in developing the SBIRT modules, implementation of these modules in BSN courses, and otherwise helping to fine-tune the teaching of these skills to BSN students. Without their efforts and support, this project would not have been successful: (a) the staff and management of PERU at the University of Pittsburgh, led by Jan Pringle, PhD; (b) Heather Santa, Research Specialist; (c) Nicholas Korach II, Data Manager for providing data used in this article; (d) Alexandra Falk, SBIRT Research Specialist; (e) the staff and management at Allegheny Health Network, led by William Johnjulio, MD; Chair—Department of Family Medicine; and Robert Sulkolsky, MA, Director of Training, Forbes Family Medicine Residency; (f) Gabrielle Strong, Bridget Burns and Fredricka Odelstierna; (g) Dr. Pat Downey, Dean, School of Health Sciences; (h) Dr. Diane Hunker, Professor, Director of Nursing; and (i) Dr. Michell Doas, Nursing Faculty.
Author’s Note
C.R. is the main author and teacher of the SBIRT learning modules throughout the period covered.
Author Contributions
H.S., research specialist, acquired the qualitative data and conducted the analysis; this included interviewing instructor and students via focus groups and served as an approver of interim and final versions submitted for publication. A.F., research specialist, managed the quantitative data and conducted analysis of pre- and postsurveys and training satisfaction survey. A.N., SBIRT program director, managed data reporting, data compliance, and overall program/training evaluation efforts and served as an approver of interim and final versions submitted for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Chad Rittle is an associate professor of nursing at Chatham University in Pittsburgh, PA. He teaches Community and Environmental Nursing and Cross-Cultural Nursing among other courses.
Heather Santa, MS, MA is a research specialist at the University of Pittsburgh, School of Pharmacy, Program Evaluation and Research Unit in Pittsburgh, PA. She leads implementation, evaluation, and reporting efforts as well as provides substance use education and training to healthcare professionals and students.
Alexandra Falk, BS, is a research specialist at the University of Pittsburgh, School of Pharmacy, Program Evaluation and Research Unit in Pittsburgh, PA. She performs quantitative and qualitative data analysis for several SBIRT initiatives, oversees data reporting, and maintains the digital backend for substance use training programs.
Alexandra Nowalk, MPH, CPH, CHES, is the SBIRT Program Director at the University of Pittsburgh, School of Pharmacy, Program Evaluation and Research Unit in Pittsburgh, PA. She supervises a current grant portfolio of $3 million in federal, state, and foundation SBIRT initiatives. She has trained hundreds of healthcare professionals in various healthcare settings, authored two SBIRT book chapters, and has spoken at multiple conferences and webinars as a technical expert.