
Abstract
The purpose of this study was to explore occupational health nurses’ attitudes, beliefs, and practices regarding the delivery of smoking cessation services to workers. The study included 707 members of the American Association of Occupational Health Nurses (AAOHN) who completed a one-time survey during the fall of 2012. Results indicated that occupational health nurses believed that evidence-based treatments are at least somewhat effective and that they should provide smoking cessation services to their workers; however, a majority of occupational health nurses reported that they did not have appropriate smoking cessation training or guidelines in their workplaces. Occupational health nurses would benefit from training in the use of smoking cessation guidelines and evidence-based smoking cessation interventions, which could be used in their clinical practice. Employers should ensure that workplace policies, such as providing coverage for cessation services, facilitate smokers’ efforts to quit. Employers can benefit from many of these policies through cost savings via reduced health care costs and absenteeism.
Among the 41.2 million Americans who smoke, 70% have indicated a desire to quit, 52% have made a quit attempt, and yet only 6% have quit successfully (Agaku, King, & Dube, 2014; Centers for Disease Control and Prevention, 2011). The Clinical Practice Guidelines for Treating Tobacco Use and Dependence: 2008 Update recommended strategies that are effective in assisting smokers to quit, including a recommendation that health care providers and clinicians should intervene with their clients who use tobacco (Fiore et al., 2008). Research demonstrates that clinician-led treatment results in higher abstinence rates compared with interventions without a clinician (Fiore et al., 2008). These guidelines recommend that health care providers use the 5A’s framework for smoking cessation interventions (Fiore et al., 2008; see “5 A’s Framework”).
5 As Framework.
Nurses are among the health care providers shown to effectively assist smokers to quit. Research shows that nurse-led cessation interventions at the point-of-care increase the likelihood of quitting by 30% (Rice & Stead, 2008). In addition, because nurses care for a large number of clients every day (World Health Organization, 2005) and are held in high esteem by the public due to their perceived trustworthiness (Newport, 2012), their interventions are likely to positively affect a significant number of smokers. Nurses practice in a variety of clinical settings, including worksite clinics and wellness programs, at various professional levels. As the largest health care profession (Halcomb, 2005), nurses can significantly impact the health of their clients by using evidence-based smoking cessation interventions.
In spite of these positive characteristics, nurses underutilize evidence-based smoking cessation interventions, including those recommended in the 5As framework (Bastian, 2009; Hamlett-Berry et al., 2009; National Academy of Sciences, n.d.; Sarna et al., 2009; Tobacco Free Nurses, 2007; Tong, Strouse, Hall, Kovac, & Schroeder, 2010). One national study found that most nurses ask clients whether they smoke, and a majority advise smokers to quit; yet only about half of these nurses explore clients’ interests in quitting, and few provide assistance in setting a quit date or refer clients to smoking cessation programs as outlined in relevant evidence-based guidelines (Tong et al., 2010). Tong et al. (2010) found that possible barriers to nurses using evidence-based guidelines include lack of training, competing priorities, and nurses’ attitudes and beliefs regarding their role in delivering smoking cessation interventions. Another study cited lack of provider willingness or time, lack of standardized protocols, and lack of systematic processes using multiple members of the health care team as reasons for lack of adherence to evidence-based guidelines (Bastian, 2009).
As a subspecialty of community health nursing, occupational health nurses have unique opportunities to reach smokers through partnerships with workers in support of worker health and safety. Occupational health nurses are located at the worksite and interact frequently with workers over long periods of time to address both occupational and personal health and safety concerns and to promote healthy habits. Since a majority of the U.S. population is part of the workforce (U.S. Bureau of Labor Statistics, 2014) and spend about half of their non-sleeping time at work (U.S. Bureau of Labor Statistics, 2013), the workplace is an ideal setting for targeted health promotion and prevention programs (World Health Organization, n.d.). Despite occupational health nurses’ vital role in addressing tobacco use, no research was found on the extent to which occupational health nurses deliver smoking cessation interventions or their attitudes toward, beliefs about and challenges in delivering smoking cessation interventions.
This study addressed a gap in the literature by using cross-sectional data to examine (a) occupational health nurses’ training in the use of smoking cessation guidelines, resources, and practices; (b) occupational health nurses’ attitudes and beliefs about smoking cessation interventions and nurses’ roles in delivering smoking cessation in the workplace; and (c) barriers to implementing smoking cessation interventions in the workplace.
Method
This survey was conducted by the Legacy/AAOHN project team (Legacy & AAOHN, 2013), which is a collaborative partnership between Legacy, a national public health non-profit organization focused on tobacco control research and programs, and the American Association of Occupational Health Nurses, Inc. (AAOHN), an organization of nursing professionals who specialize in worker health and safety. AAOHN has a membership of over 5,000 licensed nursing professionals, predominantly in the United States, who are dedicated to advancing and maximizing the health, safety, and productivity of domestic and global workforces by providing education, research, public policy, and practice resources for occupational and environmental health nurses (AAOHN, 2012).
Survey and Sample
Members of AAOHN (n = 5,200), age 18 years or older, were invited to participate in this one-time survey. Data were collected using Survey Monkey (www.surveymonkey.com), a web-based survey tool. Members of AAOHN were contacted four times via an e-mail invitation with a link to the survey. AAOHN’s monthly newsletter, which is distributed to all members, also included a link to the survey. The e-mail invitation and newsletter announcement informed members that the purpose of the survey was to collect data on smoking cessation programs and practices. The survey was open to participants from October 25, 2012, to November 21, 2012, and took about 15 minutes to complete. Respondents could skip questions they did not wish to answer. The survey included the following topics: (a) personal, work environment, smoking behavior, and demographic characteristics; (b) smoking policies in respondents’ workplaces; (c) training, guidelines, and resources for implementing smoking cessation programs in respondents’ workplaces; (d) barriers to providing smoking cessation services; (e) smoking cessation practices, attitudes, and beliefs; and (f) knowledge of alternative tobacco products and use of tobacco products among workers. The study was approved by Chesapeake Institutional Review Board in 2012.
Measures
Personal, work environment, and demographic characteristics included age, gender, race/ethnicity, type of employment (e.g., nurse clinician, case manager), employment status (e.g., full-time, part-time), educational attainment, employment sector (e.g., hospital sector), and marital status. Smoking behavior was assessed with the question, “Have you smoked at least 100 cigarettes in your entire life?” Those who answered “no” were defined as never smokers. Those who answered “yes” were asked, “Do you currently smoke cigarettes every day, some days, or not at all?” Those who selected “every day” or “some days” were defined as current smokers, and those who selected “not at all” were defined as former smokers (U.S. Department of Health and Human Services & National Institutes of Health, 2014). Items about the work environment included the number of workers that nurse respondents cared for each day and the amount of time the nurse spent with each worker.
Previous smoking cessation training was assessed with questions about whether participants had received cessation training and, if not, whether they were interested in receiving such training. Questions about smoking cessation guidelines included whether each participant’s place of work had cessation guidelines, including questions about knowledge and use of the Clinical Practice Guidelines for Treating Tobacco Use and Dependence: 2008 Update (Fiore et al., 2008).
Smoking cessation resources and practices were assessed with questions about the availability and use of various smoking cessation medications and materials in the workplace as well as nurses’ knowledge of various tobacco use treatments, such as Internet interventions and smoking cessation medications.
To measure attitudes and beliefs about smoking cessation treatment effectiveness, questions on respondents’ perceived effectiveness of various smoking cessation treatments were included. Questions were also included on attitudes and beliefs about the role of occupational health nurses in delivering smoking cessation services and perceived barriers to delivering smoking cessation services to workers.
The majority of questions about smoking cessation guidelines, training, practices, and resources as well as questions about attitudes and beliefs toward smoking cessation treatment effectiveness were obtained from Surveys of Health Professionals Knowledge, Attitudes, Beliefs and Behavior Regarding Smoking Cessation Assistance and Counseling and National Sample Survey of Registered Nurses (Strouse, Hall, & Kovac, 2004; U.S. Department of Health and Human Services, 2010). Frequency distributions of survey items were examined using a report generated by Survey Monkey.
Results
Of the approximately 5,200 AAOHN members invited to participate in the survey, 707 responded (13.6%). Since respondents could skip questions, some data were missing on each item, ranging from approximately 9.2% to 16.3% for questions without skip patterns; numbers reported below indicate the percentages among the sample of respondents who answered the question. A summary of findings was disseminated to members of AAOHN in March 2013 (Legacy & AAOHN, 2013).
Respondents’ Personal, Work, Demographic, and Smoking Characteristics
Table 1 details the demographic characteristics of the survey respondents. In summary, the majority of respondents were female (94.5%), White (94.2%), and 55 years or older (61.3%). The most common sectors that respondents worked in were the manufacturing (30.4%) or hospital sector (18.2%). The most common type of employment reported was nurse clinician (32.8%). Almost all respondents were licensed as registered nurses (RN; 90.6%); 9.4% were licensed as advanced practice nurses (APN), and 1.8% as practical or vocational nurses (licensed practical nurse [LPN]/licensed vocational nurse [LVN]). Respondents could select more than one licensure.
Demographic and Work Characteristics of Study Respondents a
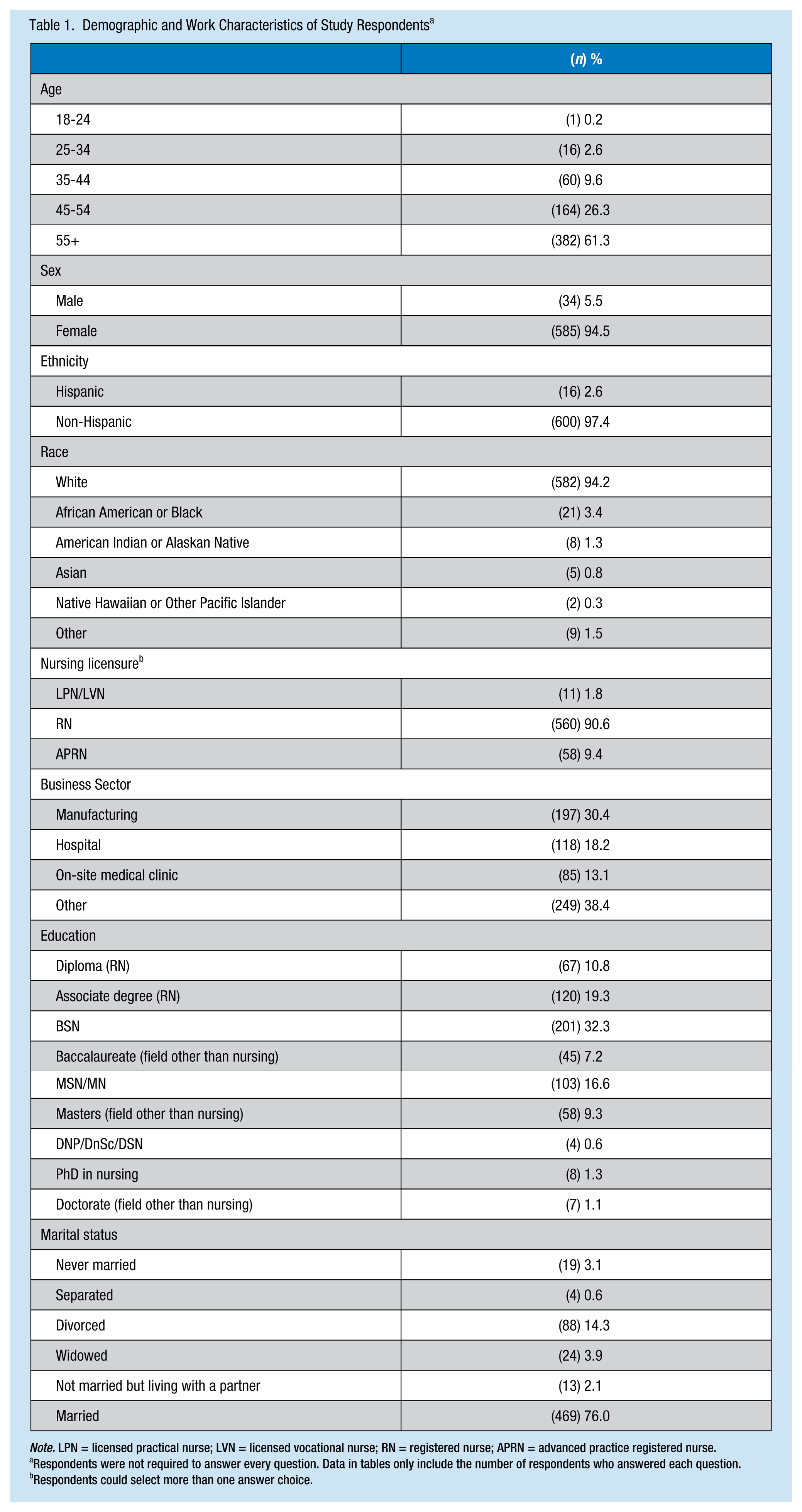
Note. LPN = licensed practical nurse; LVN = licensed vocational nurse; RN = registered nurse; APRN = advanced practice registered nurse.
Respondents were not required to answer every question. Data in tables only include the number of respondents who answered each question.
Respondents could select more than one answer choice.
Most respondents reported earning a bachelor of science in nursing (BSN; 32%), an associate degree in nursing (ASN; 19%), or a graduate degree (29%). A total of 85.9% of respondents reported working full-time. These findings are consistent with another study that examined AAOHN membership; the majority of members were over 45 years of age, held an RN license, and had earned at least a baccalaureate degree (Burgel & Kennerly, 2012). A total of 68% of respondents were never smokers, 28.4% were former smokers, and 3.7% were current smokers. Participants reported caring for an average of 58 workers per week and spending an average of 22 hours per week interacting directly with workers.
Smoking Cessation Training and Guidelines
About half of the respondents (51.9%) indicated that they had never received smoking cessation training. Of those who had never received training, most said they would be interested in receiving training (65.1%).
A total of 27.3% of the respondents indicated that their practice setting had guidelines or procedures prompting nurses to conduct smoking cessation counseling. Thirty-six percent of the respondents had heard of the U.S. Public Health Service (USPHS) Clinical Practice Guidelines: Treating Tobacco Use and Dependence: 2008 Update and among those who had heard of the guidelines, 34.2% had read the guidelines partially or in full, 29.3% had not read them, and 36.4% did not know whether they had read them. Furthermore, among those who had heard of the USPHS Clinical Practice Guidelines: Treating Tobacco Use and Dependence: 2008 Update, 47.4% said that they had been either partially or fully implemented in their workplaces, 26.3% said that they were not implemented, and 26.3% did not know whether the guidelines had been implemented. A total of 34.2% of the respondents indicated that their workplaces had implemented other smoking cessation guidelines either partially or in full, including the Freshstart Program from the American Cancer Society or the American Lung Association Guidelines.
Less than half (44%) of respondents indicated that they felt adequately trained to implement smoking cessation interventions, and 47% disagreed with the statement, “I am very confident in my ability to assess a worker’s nicotine dependence.”
Smoking Cessation Resources and Practices
Eighty-four percent of respondents reported having smoking cessation materials available to workers in their practice setting. Close to 94% of those respondents reported having materials such as cards or brochures with telephonic counseling services (i.e., quit lines) contact information available to assist workers quit smoking. A total of 37.6% of respondents had heard of an Internet service to assist individuals quit smoking, and most respondents who had heard of such a service reported referring workers to the service (76.1%). A majority of respondents indicated that recommended smoking cessation medications had been prescribed or recommended to workers in their workplaces; 76% had recommended or prescribed the nicotine patch, 68.8% nicotine gum, 50.5% Zyban (Bupropion SR), and 67.7% Chantix (varenicline). Very few respondents indicated that the nicotine inhaler had been recommended to workers (15.9%).
Attitudes and Beliefs About Smoking Cessation Treatment Effectiveness
Table 2 displays data depicting respondents’ beliefs about the effectiveness of various tobacco dependence treatments. Chantix (varenicline) was the most highly endorsed item, with 36.5% reporting they believed it to be very effective, followed by 34.6% and 28.3% of respondents who reported believing smoking cessation programs (including group counseling sessions) and face-to-face counseling or advice to be very effective, respectively. The least endorsed item was the nicotine inhaler, with only 4.8% of respondents reporting that they believed the inhaler to be very effective.
Respondents’ Beliefs About the Effectiveness of Various Tobacco Dependence Treatments a
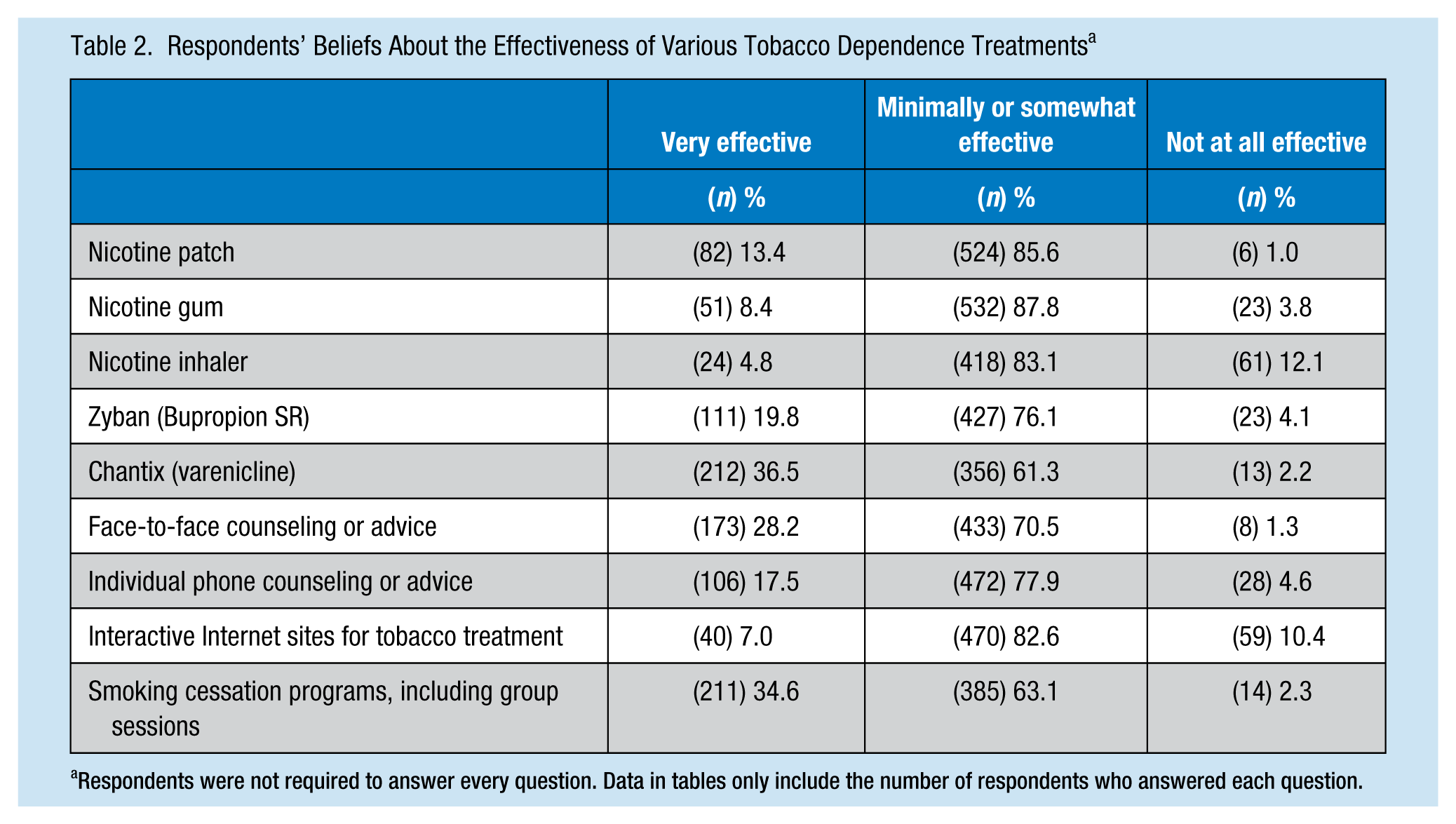
Respondents were not required to answer every question. Data in tables only include the number of respondents who answered each question.
Attitudes and Beliefs About Occupational Health Nurse’s Role in Delivering Smoking Cessation Services
Respondents’ attitudes and beliefs about the occupational health nurse’s role in delivering smoking cessation services in the workplace are described in Table 3. Overall, the majority of respondents agreed that nurses should refer smokers to quit lines or counseling services (96.5%), should provide written smoking cessation materials to smokers who want to quit (98.2%), and should assist workers in formulating quit plans (88.7%). In comparison, relatively fewer agreed that occupational health nurses should provide the most basic components of recommended smoking cessation guidelines: asking smokers to quit (65.2%), asking smokers if they were willing to quit in the next 30 days (77.6%), and providing cessation counseling (77.6%).
Attitudes and Beliefs About the Role of Occupational Health Nurses in Providing Smoking Cessation Services a
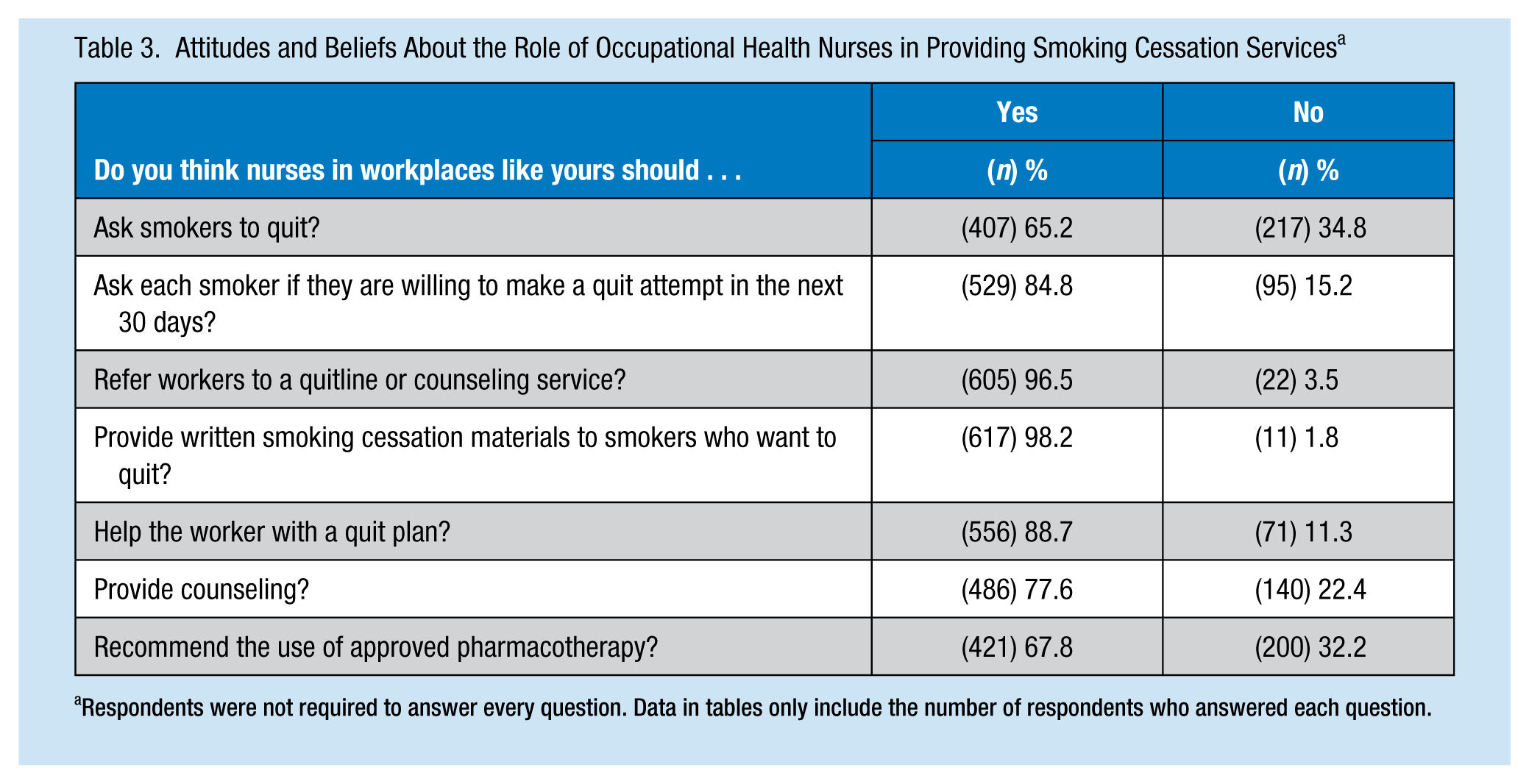
Respondents were not required to answer every question. Data in tables only include the number of respondents who answered each question.
Barriers to Providing Smoking Cessation Services
About half of respondents (51.5%) agreed that workers would resist their advice on smoking cessation, and 38% felt that occupational health nurses had competing priorities and time limitations, which kept them from assisting smokers to quit. Almost half of respondents (49.4%) agreed that little or no reimbursement for smoking cessation is available in their area, and 13.9% of respondents reported they were uncomfortable asking workers if they smoked.
Discussion
Study findings indicate that most occupational health nurses believe they should play a role in assisting smokers to quit and most have smoking cessation materials available for workers. In addition, most occupational health nurses believe that current, evidence-based interventions to assist smokers quit are at least somewhat effective, yet nearly half of respondents indicated they do not feel adequately trained or confident in their ability to provide smoking cessation interventions; just over a quarter of respondents reported that guidelines had been implemented at their place of employment.
These findings align with other research indicating that health care professionals underutilize evidence-based smoking cessation guidelines, and many do not have processes and procedures to prompt the delivery of smoking cessation interventions to clients (Bastian, 2009; Hamlett-Berry et al., 2009; Steinberg et al., 2003; Tong et al., 2010). Less than 40% of participants in this study had heard of the Clinical Practice Guidelines for Treating Tobacco Use and Dependence: 2008 Update despite being the current gold standard for tobacco treatment guidelines in the clinical setting; about half of respondents had never received training in the delivery of smoking cessation services. The importance of providing training and support to health care providers in implementing smoking cessation guidelines were demonstrated in a quasi-experimental study by Katz et al., which found that provision of a multi-component 5A’s training program for nurses at a U.S. Department of Veterans Affairs (VA) medical center significantly improved nurses’ attitudes toward the 5As and delivery of 5As services to VA patients over time (Katz et al., 2013).
Employers must educate occupational health nurses on these guidelines and provide training and professional development opportunities on the implementation of evidence-based guidelines in their daily practice. Specifically, the Clinical Practice Guidelines for Treating Tobacco Use and Dependence: 2008 Update guidelines recommend that education and training in tobacco dependence treatment be required for all clinical staff. The guidelines also recommend continuous professional development through tobacco cessation training and continuing education (Fiore et al., 2008). Furthermore, other stakeholders, such as clinical policymakers, APN, and clinic managers, may require guidance and access to tools to support the education and professional development of occupational health nurses in clinical settings.
The majority of respondents reported that workers would resist their advice regarding smoking cessation, and over one third reported that they have competing priorities and limited time to assist smokers to quit. These beliefs are consistent with challenges experienced by other health care providers (Blumenthal, 2007; Katz et al., 2014; Tong et al., 2010). Although occupational health nurses may have limited time with workers, a tobacco use screening and brief intervention is one of the three highest ranking preventive services based on preventable burden of disease and cost-effectiveness (Maciosek et al., 2006). Furthermore, occupational health nurses should be reminded that only minimal time is necessary for person-to-person contact between a smoker and a clinician to effectively support smoking cessation; minimal counseling (<3 minutes) results in an estimated abstinence rate of 13.4 compared with no contact at all, which has an abstinence rate of 10.9 (Fiore et al., 2008). The estimated abstinence rate increases as the level of contact increases beyond 3 min, but shorter interventions are still effective. Education and training are necessary to communicate that even screening for tobacco use or discussing smoking cessation for a short period of time can positively impact workers’ cessation outcomes and provide nurses with the knowledge and skills needed to provide these services.
Employers and clinic managers should also review their policies and procedures to ensure that no systematic barriers interfere with the delivery of smoking cessation services (Blumenthal, 2007). For example, employers should enact smoking bans in the workplace to decrease employee exposure to secondhand smoke, reduce tobacco use, and increase cessation rates among smokers (Task Force on Community Preventive Services, 2001). Also, workplaces should ensure that smoking cessation medications and counseling are covered by employer insurance policies. The Clinical Practice Guidelines for Treating Tobacco Use and Dependence: 2008 Update state that providing tobacco dependence treatment as a benefit to employees has been shown to increase the proportion of those who use treatment, make quit attempts, and quit successfully (Fiore et al., 2008). Furthermore, the National Institute for Health and Clinical Excellence recommends that employers implement policies that allow employees to use smoking cessation services during the workday without loss of pay (National Institute for Health and Clinical Excellence, 2007).
Providing workers with smoking cessation benefits and supporting smokers in their efforts to quit offers cost benefits to employers (Fiore et al., 2008; Fitch, Iwasaki, & Pyenson, 2006; Hojgaard, Olsen, Pisinger, Tonnesen, & Gyrd-Hansen, 2011; Warner, Smith, Smith, & Fries, 1996). Smoking cessation can prevent the onset of costly chronic illnesses, such as cancer and heart disease, and providing coverage for cessation services can produce significant financial savings for employers through lower health care costs, higher productivity, lower absenteeism, and lower life insurance payouts (Fiore et al., 2008).
This study has several limitations, including a low response rate (13.6%), missing survey data, and convenience sampling, which may have resulted in selection bias. Since all recruitment materials specified that the survey was about smoking cessation practices and programs, nurses who were non-smokers or former smokers, interested in smoking cessation, or familiar with smoking cessation interventions may have been more motivated to participate in the survey.
Despite these limitations, this research validates the need to implement smoking cessation guidelines, including evidence-based training, tools and resources, and continuing professional development and education, to support the delivery of smoking cessation interventions by occupational health nurses at the workplace. Collaborative development and implementation of evidence-based clinical guides, tools, and resources as well as policy and process improvements will address the documented issue of underutilization of evidence-based guidelines at the point of care. Future research should examine effective strategies for implementing and disseminating tobacco use treatment guidelines in the workplace.
Implications for Practice
In response to these survey findings, the Legacy/AAOHN Project Team developed a smoking cessation resources page on the practice section of the AAOHN website. Members of AAOHN can now easily access resources for their own professional development as well as materials for employee education. These professional development tools include information and materials from The Association of the Treatment of Tobacco Use and Dependence, The Cochrane Review, Legacy, and other smoking cessation organizations. Some of these resources provide members with continuing nursing education contact hours. Other resources to support the development of smoking cessation policies and programs for various workplaces, as well as links to instructions on the use of motivational interviewing as a strategy to support smoking cessation, are also available. A link to Legacy’s free BecomeAnEx smoking cessation program (www.BecomeAnEx.org) is also on the website. The BecomeAnEx site provides interactive tools and practical information for smokers as well as a robust online community to support workers as they quit using tobacco. This evidence-based program supports the assist portion of the evidence-based 5As framework for smoking cessation. In addition, a link to a series of Legacy fact sheets provides credible information on alternative tobacco products such as hookah, cigars, electronic cigarettes, and smokeless tobacco, so members of AAOHN can educate themselves on the variety of tobacco products currently available.
Applying Research to Practice
Employers and clinic managers must institute policies and practices that incorporate the use of smoking cessation guidelines (i.e., the 5As) and training for occupational health nurses on how to deliver evidence-based smoking cessation services to their workers. These interventions will ensure that smokers in the workplace receive the benefits of evidence-based smoking cessation treatment, which can result in more quit attempts among smokers, successful smoking cessation, and ultimately reduced morbidity and mortality from tobacco-related disease. Employers should also examine their current policies, including insurance coverage for cessation services, to ensure that these policies are conducive to supporting workers in their efforts to quit smoking and maintain long-term cessation. These policies will likely result in financial savings for employers through reduced health care costs and employee absenteeism.
Footnotes
Acknowledgements
We thank the Legacy/AAOHN Project Team for their contributions to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Ollie Ganz, MSPH, is a research associate in Evaluation Science and Research at Legacy. She works on the evaluation of the truth® campaign, Legacy’s national youth smoking prevention campaign, and on research examining tobacco industry advertising. She is also a doctoral student in the Department of Prevention and Community Health at the George Washington University Milken Institute School of Public Health.
Grace Fortuna is a nurse executive with 30 years of progressive management and leadership experience in the hospital environment, academia, and the health care staffing industry. As the corporate chief clinical officer for Kelly Healthcare Resources, a Fortune 500 company headquartered in Troy, Michigan, she is responsible for clinical oversight of nursing activities, quality and licensure issues, and educational programs. She also serves as a liaison between senior management and branch contracts/negotiations.
Stephanie Weinsier is a certified nurse practitioner and occupational health nurse specialist who currently works as nurse practitioner and manager of the American Express Healthy Living Wellness Center, Ft. Lauderdale, Florida. She is president of the Ft. Lauderdale Chapter of AAOHN, serves on the Florida State Chapter Board of Directors, and currently represents AAOHN on the Legacy Taskforce.
Kay Campbell, EdD, RN-C, COHN-S, FAAOHN, is currently executive director of the American Association of Occupational Health Nurses (AAOHN); president and CEO of Healthy DireXions, her health consulting company; and an adjunct professor in the School of Public Health at the University of North Carolina. Having worked for population health management her entire career, she has had many opportunities to develop strategies for health, well-being, and productivity as well as develop and implement programs and initiatives to improve the health of workers around the world.
Jennifer Cantrell, DrPH, MPA, is the director of Evaluation Science and Research at Legacy. She directs the evaluation of the truth® campaign, Legacy’s national youth smoking prevention campaign. Her other research focuses on examining the role of advertising, public policy, and geographic factors on tobacco use and tobacco-related disparities among vulnerable populations, including individuals in low-income and minority communities.
William L. Furmanski is senior vice president for Communications at Legacy. He has more than 20 years of experience at nonprofit organizations, including 15 years working in public health. He has implemented multiple national public education campaigns to prevent teen smoking and help adults quit, supported research and advocacy initiatives, managed more than a dozen grant projects, and fostered partnerships with for-profit, nonprofit, and government organizations.