
Abstract
Background:
Reusable elastomeric respirator use in health care may represent one solution to address N95 respirator shortages experienced during infectious disease outbreaks, but cleaning and disinfection requirements may limit their utility. Evidence of respirator cleaning and disinfection behaviors and practices by health care workers may inform guidance on reusable respirator use.
Methods:
Medical system elastomeric respirator users were surveyed about respirator cleaning and disinfection practices and perceptions via an electronic survey. Respondents were subsequently classified based on reported compliance with their assigned respirator use. To explore whether respirator cleaning and disinfection issues affected compliance with assigned device use, responses were compared between user groups and adjusted for covariates.
Results:
A total of 432 of 2,024 (21%) eligible elastomeric respirator users completed the survey. Most (>90%) reported that their respirator was clean, but only 52% reported that they always disinfect their respirators after use according to the hospital’s expected practice. Only 40 respondents (9%) reported regularly cleaning the respirator with soap and water, in accordance with manufacturer recommendations. Reporting of suboptimal decontamination practice was not associated with assigned device compliance, however, except among providers and respiratory therapists.
Conclusion/Application to Practice:
Although perceptions of cleanliness and adherence to expected decontamination practices during routine use did not appear to influence compliance with assigned respirator use overall, this did predict compliance among providers and respiratory therapists, both of whom have nonfixed workstations. Practical and effective strategies to assure easy access to and availability of clean reusable respiratory protective devices are needed to facilitate their use in health care respiratory protection programs.
Keywords
Background
Respiratory protection is often required to safeguard health care workers (HCWs) from airborne infectious agents such as tuberculosis (TB). Conventionally, disposable N95 filtering facepiece respirators (N95s) are used for this purpose (Siegel et al., 2007; Wizner et al., 2016). N95 shortages experienced in each of the last major infectious public health emergencies, including the 2002 severe acute respiratory syndrome (SARS), 2009 H1N1 influenza, and 2014 Ebola outbreaks (Beckman et al., 2013; Srinivasan et al., 2004), demonstrate the need to identify additional solutions to address the predictable demand for these devices in future pandemics. One solution to avert N95 shortages may be employing reusable respirators (Bach, 2017). These include elastomeric half-facepiece respirators (EHFRs) and powered air-purifying respirators (PAPRs; Figure 1). Many health care respiratory protection programs (RPPs) include the use of loose-fitting PAPRs, as they are often used as alternatives to tight-fitting devices when HCWs are unable to successfully complete a fit-test for various reasons, including presence of facial hair (Brown et al., 2018; Wizner et al., 2016). Elastomeric half-facepiece respirators however, while frequently used in general industry, are less familiar to hospital RPP staff (National Academies of Sciences Engineering and Medicine [NASEM], 2018; Wizner et al., 2016). Thus, the adoption and utility of EHFRs as a reasonable alternative to N95s in health care settings is unclear.
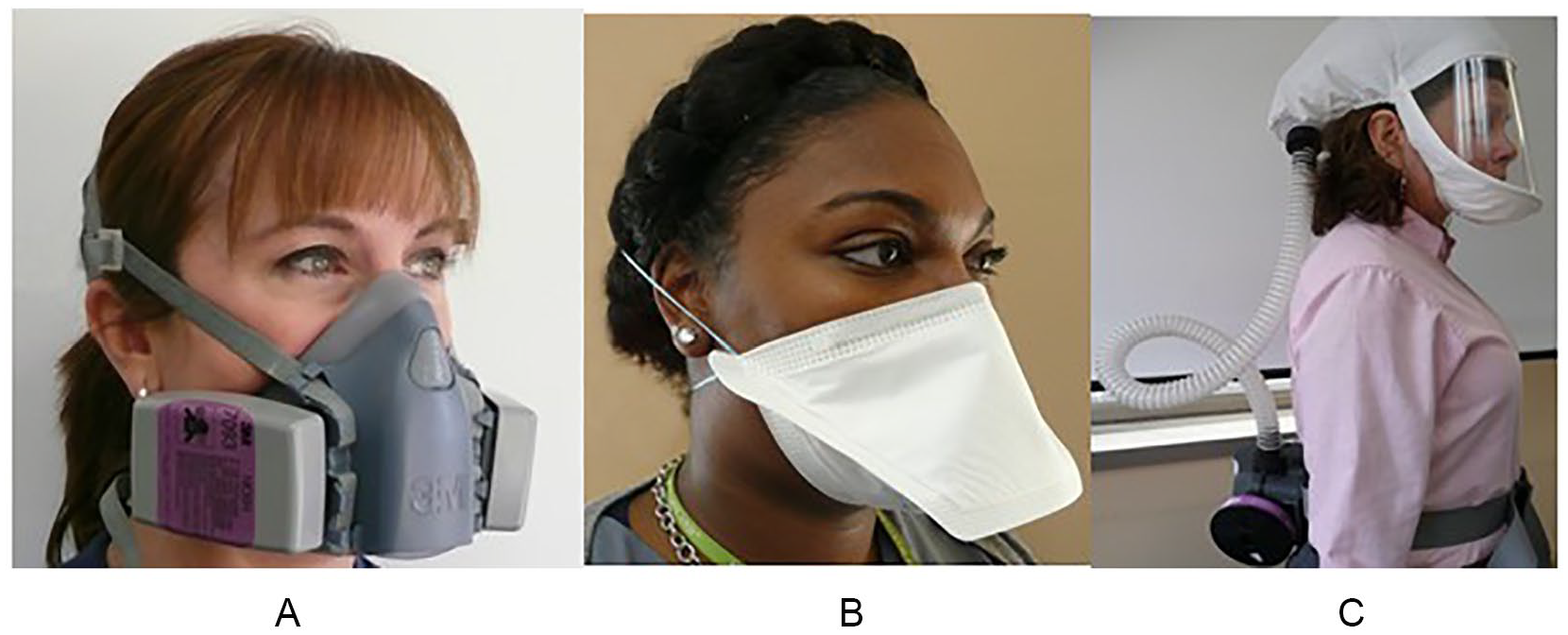
Examples of types of air-purifying respirators used in health care settings: (A) elastomeric half-facepiece respirator (EHFR), (B) N95 filtering facepiece respirator, and (C) powered air-purifying respirator (PAPR).
Previous research has shown that user acceptance features, like respirator comfort and communication, are rated less favorably among EHFR and PAPR users compared with N95 users; however, EHFRs are preferred to N95s in hypothetical higher risk scenarios such as during care of patients with active TB or pandemic influenza (Hines et al., 2019b). This suggests that user acceptance is not an insurmountable barrier to their use in health care, particularly when the exposure threat is perceived to be higher.
Logistical issues also impose potential challenges to EHFR use in health care settings. For example, both storage and availability of elastomeric respirators have been shown to be potential barriers to their optimal use in these settings (Hines et al., 2019a). Perhaps more imposing, however, are questions about whether a reusable respirator can be cleaned and disinfected acceptably. Given that respirators are typically worn in health care to protect the wearer from exposure to an infectious microbial pathogen, concern also arises because respirators may become fomites, capable of transferring infectious materials to a user’s hands or face (Casanova et al., 2008). Such fear of contaminated respirators contributing to disease transmission is fairly unique to health care and emergency response settings (Fisher et al., 2014). As most respiratory protection regulatory policies are not tailored to specific industry sectors, little health care–specific guidance exists for practical assurance that reusable respirators can be deployed in such settings without becoming contaminated and thus, a hazard to users.
The U.S. Occupational Safety and Health Administration’s (OSHA) Respiratory Protection Standard requires that employers “ensure that the respirator is properly cleaned and disinfected in a manner that prevents damage to the respirator and does not cause harm to the user” (OSHA 1910.134 Appendix B-2). This OSHA guidance is generic, which directs employers to use the cleaning recommendations provided by the respirator manufacturer, which typically is not tailored to the specific biohazard concerns of the health care setting. Thus, while specific protocols for cleaning and disinfecting elastomeric respirators are available from respirator manufacturers, minimal information is available to address a protocol’s efficacy for elimination of microbial contaminants (Heimbuch & Harnish, 2019). Importantly, the terms “cleaning” and “disinfection” refer to two distinct actions. Cleaning is the removal of visible soil from surfaces using water and a detergent or enzymatic product (Centers for Disease Control and Prevention [CDC], 2008), while disinfection eliminates all pathogenic microorganisms, except bacterial spores, using liquid chemicals or wet pasteurization (CDC, 2008; Lawrence et al., 2017). In general industry, where soiling of respirators due to heavy particulate loads is likely to occur, cleaning is important to assure optimal respirator performance. In health care, while removal of soiling agents such as facial oils or dusts is important, the role of disinfection is likely more critical.
The NASEM Committee on the Use of Elastomeric Respirators in Health Care has concluded that EHFRs can be a viable solution for health care respiratory protection when logistical issues, such as cleaning and decontamination, are addressed (NASEM, 2018). Currently, limited evidence from modeled and experimental studies of reusable respirator use exists to guide recommended cleaning and disinfection practices in health care (Bessesen et al., 2015; Ciconte & Danyluk, 2013; Lawrence et al., 2017; Subhash et al., 2014).
One large U.S. medical system, anchored by an urban teaching hospital, has utilized EHFRs as one of the several devices in use in its RPP cache since 2009, due to H1N1 pandemic-related N95 shortages (Hines et al., 2017). This medical system population presented an experienced user group to query and to assess actual and perceived logistical barriers to the hospital’s elastomeric respirator use.
This study aimed to determine the perceptions of HCWs toward cleanliness of these reusable devices and to quantify their reported frequency of cleaning and disinfection under routine use. A secondary objective was to understand whether cleaning and disinfection perceptions and use practices were associated with compliance with respirators that they are assigned by their employer.
Methods
A cross-sectional survey of HCWs enrolled in RPPs of the aforementioned U.S. medical system was performed between August and October 2016. This mixed population included users of EHFRs, N95s, and PAPRs. Health care workers were eligible to complete the survey if they were included in the RPP, were at least 18 years old, had used a respirator at least once outside of training within the last year, could read English, and had worked for their current employer for at least 3 months. Two clinical sites within the medical system participating in the survey used elastomeric respirators as part of their RPP inventory: a large, urban academic medical center and its associated ambulatory physician practices, including primary and specialty care practices. An estimated 2,024 EHFR users were eligible to participate at the time of survey based on employee health rosters.
At the time of survey, the expected practices according to the institutions’ RPP were that users should wipe down their respirators with an alcohol pad or disinfectant wipe after each use. Guidance dating back to original program implementation during 2009 H1N1 outbreak also recommended that HCWs remove the filter cartridges and clean the mask using detergent, such as dish soap and water. It was also recommended that the cartridge-covered filters be changed if they became wet, soiled, or damaged. Staff received reeducation about respirator use during their annual fit-testing. Faculty physicians and advanced practice providers, however, received biennial respirator fit-testing and training coupled with hospital recredentialing requirements.
Health care workers were recruited to participate via flyers displayed in approved common workspace areas, announcements at shift change meetings and huddles, as well as divisional leadership and nursing manager meetings. Health care workers who completed the survey received US$20 electronic gift cards as compensation for their participation. Due to budgetary constraints, recruitment was closed after reaching enrollment of the first 1,152 participants, regardless of the respirator type use.
Health care workers could complete the electronic survey via personalized links to the questionnaire embedded in email messages sent by the study team to addresses obtained from employee health rosters of RPP participants. To assure opportunities for all eligible HCWs to participate, the study team also scheduled times to be present on nursing units with laptop computers available for HCWs to complete the survey on-site through a general entry portal, entered via a single-use access code. All study activities were approved by the University of Maryland, Baltimore Institutional Review Board.
Survey Methods
Survey questions were developed based on feedback provided by HCWs who had participated in a focus group about respiratory protection in an earlier, qualitative phase of the study (Hines et al., 2017). These targeted questions were combined with questions modified from other relevant, existing questionnaires (Peterson et al., 2015; Sorra et al., 2016) to address topics related to respirator cleaning and disinfection. After conversion into an electronic format, the survey was pilot-tested by a group of critical care physician respirator users, followed by additional refinement based on tester feedback, before reaching its final version. The survey was designed to be completed within 20 minutes. Aside from questions about demographic factors, only questions about cleaning and disinfection of elastomeric respirators were analyzed for this article.
The survey included questions about a variety of demographic, occupational, and respirator use factors. Occupational questions asked about job type (e.g., nurse, nurse practitioner, physician assistant, resident or attending physician, patient care technician, medical assistant, laboratory or radiology technician, respiratory therapist [RT], or other), unit setting, clinical site, and years worked in health care. Questions oriented to respirator use asked about the type of assigned respirator (disposable N95, EHFR, PAPR), type of respirator usually used (disposable N95, reusable elastomeric, PAPR), percentage of time wearing a respirator as part of routine work (<1%, 1%–10%, 10%–25%, 25%–50%, >50%), and frequency of respirator training and fit-testing (once at hire, and then annually; once at hire, and then every 2 years; once at hire, then as required by a physician-based on medical necessity; no requirements; do not know; other). With regard to respirator cleaning and disinfection perceptions and practices, workers were asked how clean they perceived their respirator to be (very clean, clean, somewhat clean, not very clean, not at all clean), the frequency I wipe my reusable elastomeric respirator with an alcohol pad or disinfectant wipe after each use (never, sometimes, about half the time, usually, always), and frequency of removing the filters and washing inside the respirator with soap and water (after each shift, weekly, monthly, yearly, rarely/never).
Most question responses were in the form of three to five categorical response options. Additional details about setting and survey methods related to different research questions among the same population have been described previously (Hines et al., 2019a, 2019b). An earlier qualitative analysis of workers and RPP decision makers from this same medical system had determined that some elastomeric respirator users were “usually” using a different model of respirator, such as an N95, rather than their assigned EHFRs (Hines et al., 2017). Thus, they had unofficially (and autonomously) switched from wearing EHFRs to N95s. This practice suggested noncompliance with expected respirator use. Thus, the questionnaire asked participants to report what respirator they most recently had been assigned to use (e.g., N95, EHFR, PAPR), and then asked what respirator they usually use. These users were classified as “concordant EHFR users” when they indicated that they were assigned the EHFR and they wore the EHFR. Those assigned to use EHFRs but who reported usually using a different type of respirator were classified as “discordant users.”
Analysis
For this analysis, responses only from HCWs who had been assigned to use an EHFR respirator were analyzed (n = 432). Among the sample of more than 1,152 total HCWs who completed the survey, 720 did not use EHFRs. Hence, they were not asked about cleaning and disinfection practices and not included in this analysis
Frequency distributions for the entire sample of EHFR users were calculated to address the primary study objective of understanding use practices and perceptions related to cleaning and disinfection. To address the secondary objective of understanding whether concordant and discordant EHFR users reported different cleaning and disinfection-related responses, frequency distributions of categorical and dichotomous demographic and other background characteristics between these two user groups were compared using chi-square analysis. The groups were also compared by the number of years worked in health care using a Wilcoxon rank-sum test. These comparisons were then reevaluated after adjustment for factors hypothesized to affect these outcomes that were significantly different between the two user groups using multinomial logistic regression. Physicians (both attending and resident), nurse practitioners, and physician assistants were classified as “providers.” Registered nurses and licensed practical nurses were classified as “nurses.” Medical assistants, patient care technicians, nurse’s aides, and laboratory or radiology technicians were classified as “patient support/other.” Inpatient settings including emergency department, medical intensive care unit, medical wards, and pediatric wards were classified as “higher-risk inpatient unit,” and all other inpatient unit responses were classified as “lower-risk inpatient units.” After adjustment for job category, site (urban academic hospital versus urban ambulatory practice), primary unit, frequency of respirator training/fit-testing, and years worked in health care, odds ratios (ORs) were calculated for reporting of specific practices or perceptions in discordant compared with current EHFR users. Noncritical categories of outcomes and independent variables were folded into larger or more meaningful categories to prevent regression model overfitting in the multivariable analyses. For example, to test the hypothesis workers who do not work in fixed unit settings such as RTs and physicians might report different practices compared with HCWs who work in “fixed” locations, responses of RTs and providers were combined for adjusted analysis and compared with nurses. To understand whether effect modification was occurring between the independent variable of user group status with potential confounders of job category and frequency of respirator training/fit-testing on the outcomes, a post hoc analysis was performed by adding interaction terms between user status and the above two independent variables. To determine whether job category or frequency of fit-testing or training were confounding the true relationship between user status and cleaning outcomes, differences in these associations between subgroups defined by job category and frequency of fit-testing or training were also examined. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Demographic and occupational characteristics of the 432 EHFR user survey respondents are shown in Table 1. Respondents were predominantly of female gender (85%), younger than 40 years (65%), nurses or patient support staff (76%), and worked at the urban academic hospital (84%); 65% were classified as concordant (n = 280) users, and 35% were classified as discordant (n = 152) users.
Demographic Characteristics of Concordant Compared With Discordant EHFR Users (n = 432)
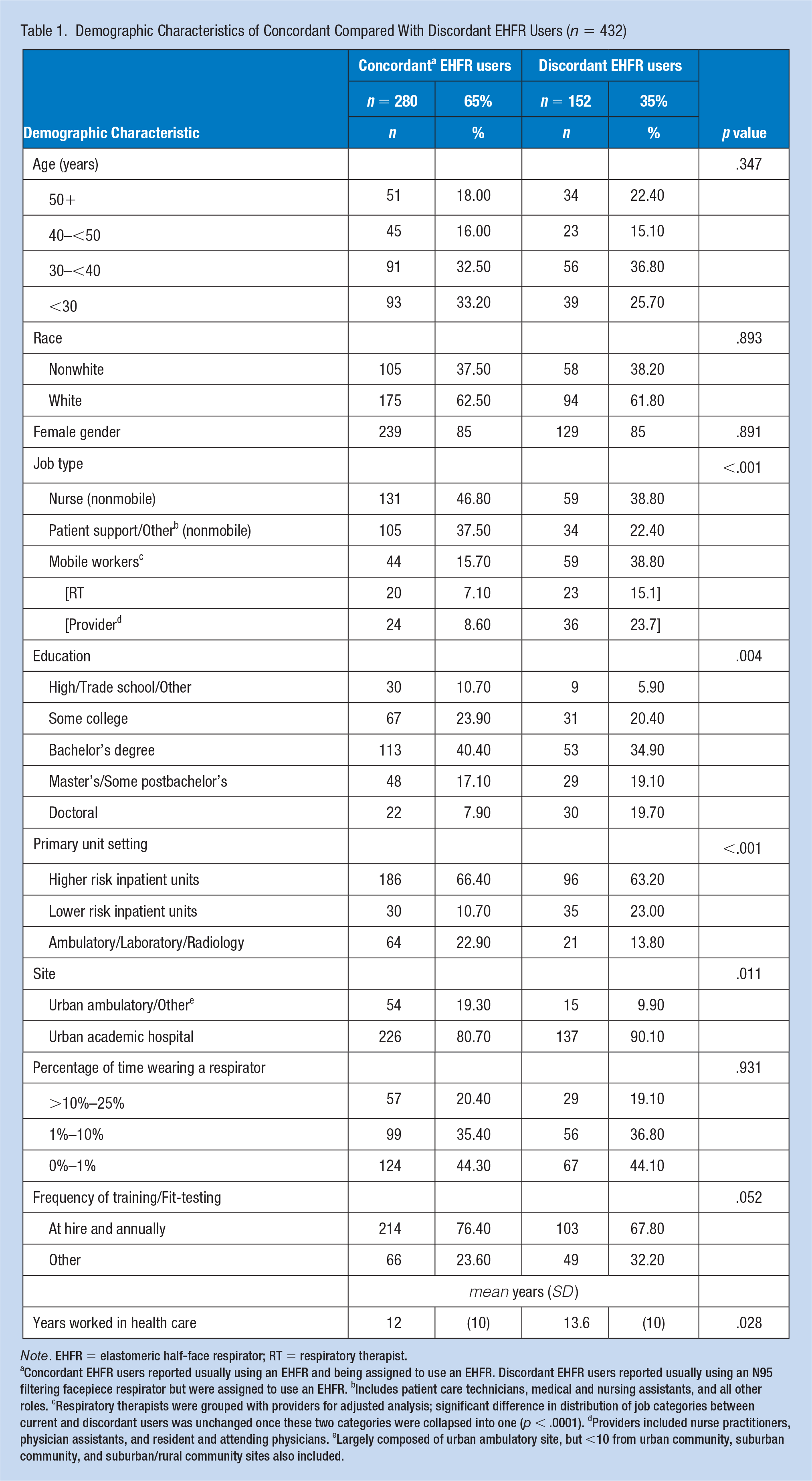
Note. EHFR = elastomeric half-face respirator; RT = respiratory therapist.
aConcordant EHFR users reported usually using an EHFR and being assigned to use an EHFR. Discordant EHFR users reported usually using an N95 filtering facepiece respirator but were assigned to use an EHFR. bIncludes patient care technicians, medical and nursing assistants, and all other roles. cRespiratory therapists were grouped with providers for adjusted analysis; significant difference in distribution of job categories between current and discordant users was unchanged once these two categories were collapsed into one (p < .0001). dProviders included nurse practitioners, physician assistants, and resident and attending physicians. eLargely composed of urban ambulatory site, but <10 from urban community, suburban community, and suburban/rural community sites also included.
Overall, 90% of respondents reported that their respirator was “clean” or “very clean.” Only 52% reported “always” and another 22% reported “usually” wiping the respirator with a disinfectant wipe after each use, the designated disinfection method according to the hospital’s RPP (Table 2). Only 9% reported removing the filters and washing the respirator with soap and water after each shift or at least weekly. Perception of cleanliness of the respirator did not differ between concordant and discordant EHFR users. Almost 58% of the concordant EHFR users reported “always” wiping down the respirator with a disinfectant wipe or alcohol pad after use, but the proportion of discordant users always performing this task was lower (42%). Both groups reported infrequent washing of the respirator, but more concordant users reported performing this task more regularly than did discordant users.
Perceived Cleanliness of Elastomeric Respirator, Disinfection and Cleaning Frequency Reported by Concordant Compared With Discordant EHFR Users (n = 432), Unadjusted.
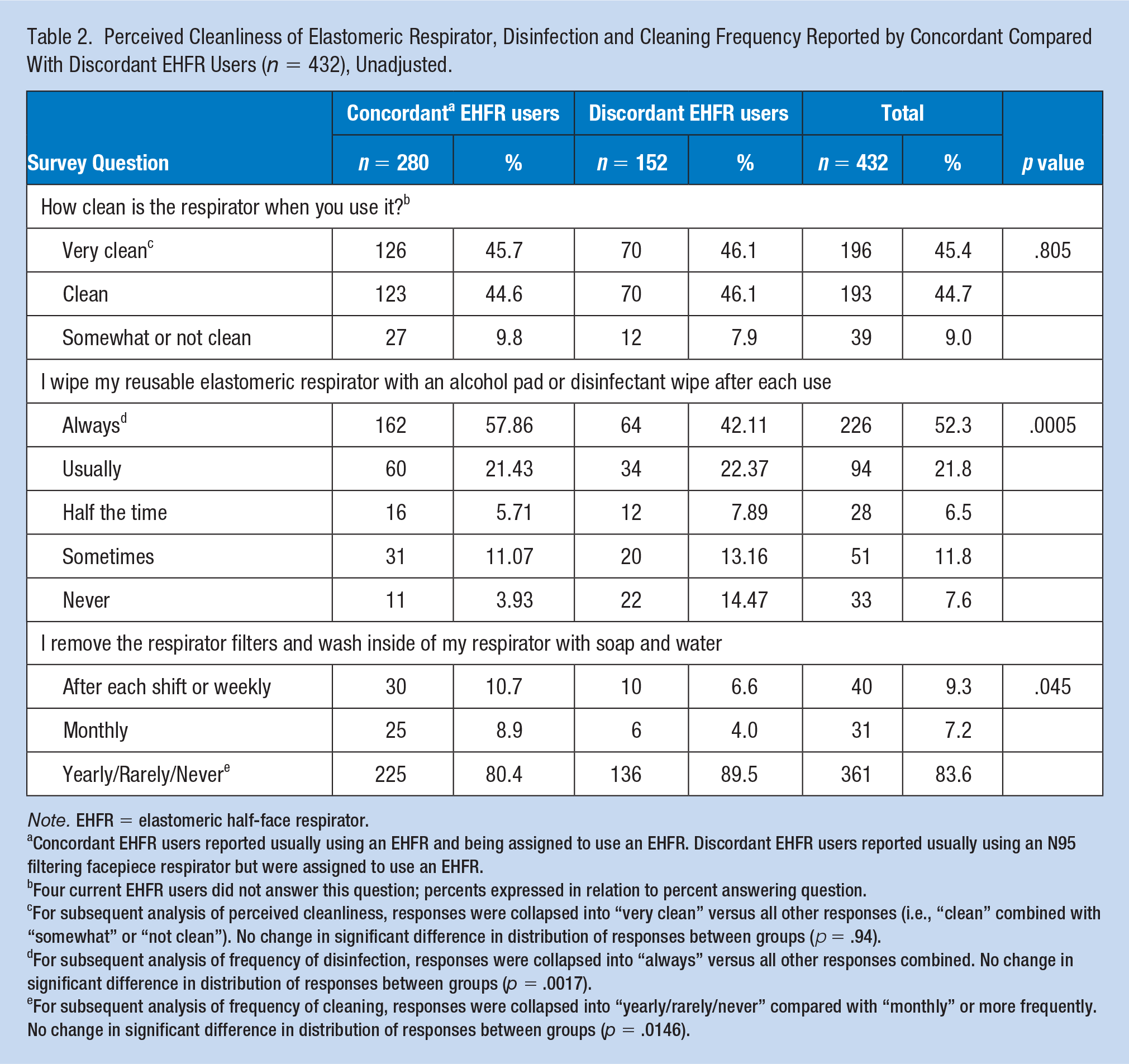
Note. EHFR = elastomeric half-face respirator.
Concordant EHFR users reported usually using an EHFR and being assigned to use an EHFR. Discordant EHFR users reported usually using an N95 filtering facepiece respirator but were assigned to use an EHFR.
Four current EHFR users did not answer this question; percents expressed in relation to percent answering question.
For subsequent analysis of perceived cleanliness, responses were collapsed into “very clean” versus all other responses (i.e., “clean” combined with “somewhat” or “not clean”). No change in significant difference in distribution of responses between groups (p = .94).
For subsequent analysis of frequency of disinfection, responses were collapsed into “always” versus all other responses combined. No change in significant difference in distribution of responses between groups (p = .0017).
For subsequent analysis of frequency of cleaning, responses were collapsed into “yearly/rarely/never” compared with “monthly” or more frequently. No change in significant difference in distribution of responses between groups (p = .0146).
For the multivariate analysis, concordant versus discordant user status was not associated with perceived cleanliness of the respirator (OR 0.82, 95% confidence interval [CI] = [0.53, 1.26]) or frequency of disinfection with a wipe (OR 1.50, 95% CI = [0.97, 2.34]). However, the frequency of cleaning the respirator with soap and water (OR 1.84, 95% CI = [0.95, 3.59]) was almost twofold higher for the concordant group, although statistical significance was not reached (Table 3). No significant interactions were observed for outcomes of perceived cleanliness or frequency of cleaning. A significant interaction was observed for frequency of disinfection between discordant respirator user status and job category: Among providers and RTs, discordant users were more likely to report suboptimal disinfection practices (OR 3.87, 95% CI = [1.65, 9.08]). Frequency of fit-testing/training did not significantly alter the association between discordant user status and frequency of disinfection.
Adjusted Odds of Perception or Elastomeric Respirator Use Practice Among Discordant (n = 152) Compared With Concordant EHFR Users (n = 280)
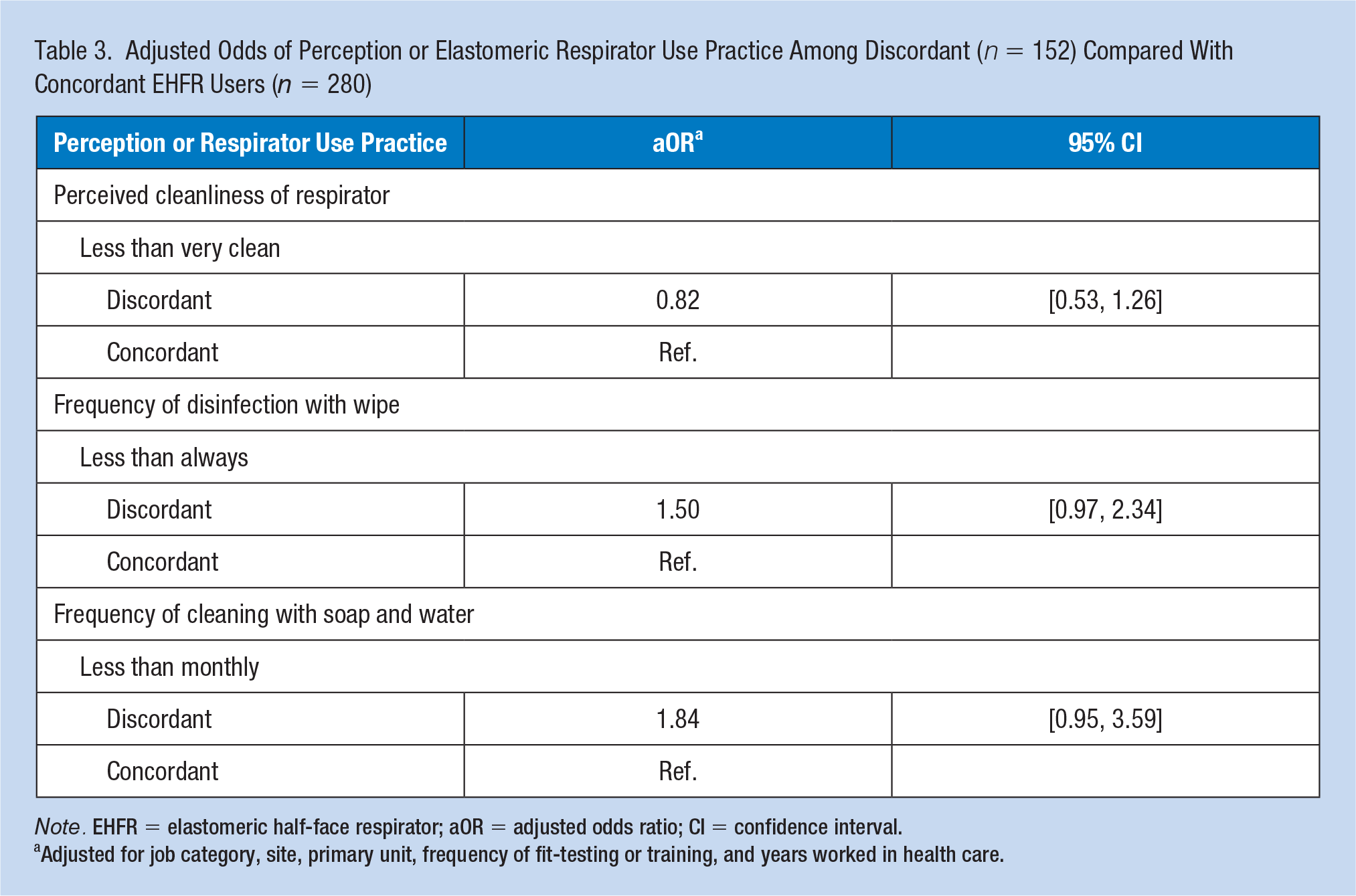
Note. EHFR = elastomeric half-face respirator; aOR = adjusted odds ratio; CI = confidence interval.
Adjusted for job category, site, primary unit, frequency of fit-testing or training, and years worked in health care.
Discussion
This study found that while most EHFR users report that their perception is that the respirator is clean, 74% report always or usually disinfecting the respirator after each use with a wipe, and most users have never reported cleaning the respirator with soap and water. Suboptimal use practices were more likely to be reported by the discordant users, but when adjusted for covariates, there were no significant differences in reporting of cleaning practices between concordant and discordant users. This suggests that behaviors required for optimal cleaning and disinfection of reusable respirators are not the primary reason for noncompliance with assigned elastomeric respirator use overall. The significant interaction, however, between care providers and RTs with discordant user status on the outcome of disinfection frequency suggests that occupational characteristics influence compliance with expected disinfection practice. Here, it is hypothesized that this may be related to nonfixed practice setting or mobile worker status, and not having a nearby, convenient storage location for an individual-maintained EHFR. This is the case for providers and RTs, but not for nurses. This pattern of occupation-associated discordant use was demonstrated in a previous analysis of self-reported respirator storage location and availability (Hines et al., 2019a). Overall, these results suggest that while cleaning and disinfection of reusable elastomeric respirators in health care must be improved, decontamination practices are not the reason for HCW noncompliance with assigned respirator use, except among job categories that require mobility throughout the hospital, such as providers and RTs.
The hospital’s EHFR RPP structure may have influenced noncompliance with expected respirator use beyond factors of cleaning and disinfection. The standard practice in place at the study hospital during the survey period was for placement of an equipment cart immediately outside of the room of a patient on airborne precautions, for which respirator use is required by HCWs (Hines et al., 2017). The cart contains a variety of sizes and models of N95s to allow HCWs who have been assigned to use them to find the respirator they have been fit-tested to use. This practice may confuse HCWs not assigned to use N95s on what they should use: The N95s are available and signage states that airborne precautions are required. Thus, if an HCW assigned to use an EHFR presents to enter a patient room where airborne precautions are in place and does not have their EHFR with them, they may elect to use an N95 filtering facepiece respirator from the cart even though they have not been fit-tested to wear it. This alternative respirator choice may be viewed as more convenient for the provider, rather than retrieving their own EHFR, to comply with the PPE requirement for airborne precautions. This would not have influenced responses of EHFR users in the ambulatory practices, however, as N95s are not regularly used there.
This study has several limitations, the first being the small number of participants. The study was originally powered to detect differences in user acceptance outcomes between an estimated 400 versus 600 EHFR and N95 users (Hines et al., 2019b). The sample of 432 assigned EHFR users included in this analysis met the original enrollment goal. After learning that EHFR users were not always wearing their respirators as assigned, however, it was decided that it was important to analyze the EHFR group further to try and understand how cleaning and disinfection practices might be affecting compliance with expected use. This led to comparison of smaller numbers of respirator users. Thus, results are compared among smaller populations of concordant compared with discordant EHFR users to address the secondary objective of understanding impacts on compliance with assigned use. Despite the small samples, differences in reporting of disinfection and cleaning practices were still discernable. Also, research suggests that while low response rates may affect univariate analyses, it is less likely to bias multivariate analysis, which is presented in this study (Rindfuss et al., 2015). Second, these data are based on self-report only and not based on observed practices. It is possible that the frequency of cleaning and disinfection may be higher or lower than that reported here, as has been demonstrated in studies comparing self-report with observed handwashing in HCWs (Jenner et al., 2006; O’Boyle et al., 2001). Self-report of safety practices among HCWs, however, has been considered an important outcome in prior research (Chokephaibulkit et al., 2013). Finally, it is unclear how consistently cleaning and disinfection is emphasized during initial and interval respirator training. This has not been measured in the past and doing so would aid in understanding the impact of training on expected maintenance practices.
This study also has notable strengths. First, it is the only study among active EHFR users in health care to report on actual individual use practices related to cleaning and disinfection, for which optimal protocols are still being designed and compared (NASEM, 2018). While experimental conditions have provided guidance on potential best practices for respirator reprocessing, this study gives a practical evaluation of real-world use of these devices (Bessesen et al., 2015; Ciconte & Danyluk, 2013; Heimbuch & Harnish, 2019; Lawrence et al., 2017; Subhash et al., 2014). In addition, by including respirator users who autonomously elected to use a different respirator though assigned to use an elastomeric respirator, the responses may give some insight to barriers which this subpopulation found inconvenient. While challenging, this reflects real-world experiences of HCW safety behavior. These finding also suggest that addressing these problems could improve hospitals’ RPPs and reduce or eliminate noncompliance.
Implications for Occupational Health Practice
N95 respirator shortages experienced during recent infectious disease outbreaks have exposed vulnerabilities to hospital RPP readiness. Use of reusable elastomeric respirators may be one solution to combat these predictable N95 shortages and has been recommended by the U.S. CDC during coronavirus disease 2019 (COVID-19) response (CDC, 2020). Practical and effective cleaning and disinfection strategies are needed to facilitate inclusion of reusable elastomeric respirators as part of hospital RPPs. An evidence base to support development of decontamination strategies exists (Bessesen et al., 2015; Heimbuch & Harnish, 2019; Lawrence et al., 2017). Occupational health professionals involved in their hospital’s RPP should be knowledgeable about the various types of respiratory protection devices, as well as the pros and cons to these devices during everyday use.
Conclusion
Although perception of cleanliness and adherence to recommended cleaning practices do not appear to influence compliance with use of assigned reusable respirators overall, this did predict lack of compliance among providers and RTs, both of which are mobile workers, possibly due to challenges and the inconvenience of a nonfixed work setting. Importantly, HCW respirator cleaning behavior can be optimized through innovative strategies in training, the organization of the RPP, and enhanced safety culture. The results of this study provide an evidence base to inform organizational practice and policy revisions. Practical and effective approaches to assure easy access to and availability of clean reusable respiratory protective devices will facilitate inclusion of elastomeric respirators in health care RPPs. That done, reusable elastomeric respirators can effectively serve as one solution to the predictable N95 filtering facepiece respirator shortages occurring during pandemics and as a dependable form of routine hospital respiratory protection.
Applying Research to Occupational Health Practice
Health care workers who use reusable elastomeric respirators under routine respiratory protection scenarios report that they perceive their respirators to be clean. Just more than half, however, report always disinfecting the respirator with a wipe after each use. Practical and effective decontamination strategies are needed to facilitate inclusion of these respirators as part of hospital respiratory protection programs. Use of reusable elastomeric respirators may be one solution to abate disposable N95 respirator shortages experienced during infectious disease outbreaks.
Footnotes
Author Contributions
S.E.H., M.O., P.G., M.F., R.H., T.R., J.C., and M.M. participated in conception or design of the work; S.E.H., C.H.B., M.O., M.F., and M.M. drafted or critically revised the work for important intellectual content; all authors participated in the acquisition, analysis, or interpretation of data for the work; and all authors provided the final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors received grant funding to their institution for completion of this research. S.E.H. currently receives grant funding to her institution from CleanSpace Technology to study reusable respirators, but not during the period in which this research occurred.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Centers for Disease Control and Prevention—National Institute for Occupational Safety and Health (NIOSH; 1R211OH010868-01).
Institution and Ethics Approval and Informed Consent
The study was approved by the University of Maryland, Baltimore Institutional Review Board. A waiver of written informed consent was granted for this electronic survey study.
Author Biographies
Stella E. Hines is an Occupational & Environmental Medicine (OEM) and pulmonary physician and directed the employee health services for the University of Maryland Faculty Physicians Inc. ambulatory practices.
Clayton H. Brown is a professor of biostatistics at the University of Maryland School of Medicine.
Marc Oliver is an occupational health nurse and research analyst.
Patricia Gucer is a sociologist and statistician.
Melissa Frisch is an OEM physician and Medical Director of Employee Health Services for the University of Maryland Medical Center (UMMC).
Regina Hogan is an occupational health nurse and the program manager for the UMMC Employee Health Services.
Tracy Roth is an occupational health nurse and the program manager for the Faculty Physicians Inc. Employee Health Services.
James Chang is a certified industrial hygienist and the Director of Safety for the UMMC.
Melissa McDiarmid is the Division Director of the University of Maryland School of Medicine Division of Occupational & Environmental Medicine.